Disclosures. Funding: CIHR, HSF, AIHS, UHF. Research: Novo Nordisk, CVRx, Valencia. Consulting: Valeant
|
|
|
- Vanessa Cunningham
- 5 years ago
- Views:
Transcription

1 Hypertension Update Raj Padwal Associate Professor General Internal Medicine and Clinical Pharmacology Director, Hypertension Clinic University of Alberta
2 Disclosures Funding: CIHR, HSF, AIHS, UHF Research: Novo Nordisk, CVRx, Valencia Consulting: Valeant Speaking and other Honoraria: Mylan, Servier, Merck
3 Objectives 1. Discuss the new CHEP diagnostic algorithm for hypertension. 2. Other updates: a. Smoking cessation b. Atherosclerotic renal artery stenosis c. Thresholds and targets in stage I uncomplicated HTN, diabetes, and the very elderly
4 European Society of Hypertension Classification of Blood Pressure Category Systolic Diastolic Optimal <120 and / or <80 Normal <130 and / or <85 High-Normal and / or Grade 1 (mild hypertension ) and / or Grade 2 (moderate hypertension) and / or Grade 3 (severe hypertension) 180 and / or 110 Isolated Systolic Hypertension (ISH) 140 and <90 The category pertains to the highest risk blood pressure *ISH=Isolated Systolic Hypertension. J Hypertens 2007;25:

5 Burden of disease attributable to 20 leading risk factors in 2010, expressed as a percentage of global disability-adjusted life-years
:1099 1105.")
:37 46. Statistics Canada.")
6 Hypertension In Canada Hypertension awareness, treatment, and control changes over time Joffres MR, Hamet P, MacLean DR, L italien GJ, Fodor G. Distribution of blood pressure and hypertension in Canada and the United States. Am J Hypertens. 2001;14(11): Leenen FHH, Dumais J, McInnis NH, Turton P, Stratychuk L, Nemeth K, Lum Kwong MM, Fodor G. Results of the Ontario Survey on the Prevalence and Control of Hypertension. CMAJ. 2008;178(11): Wilkins K, Campbell NRC, Joffres MR, McAlister FA, Nichol M, Quach S, Johansen HL, Tremblay MS. Blood pressure in Canadian adults. Health Reports. 2010;21(1): Statistics Canada. Blood pressure of Canadian adults, 2009 to Ottawa, ON: Statistics Canada, x/ /article/11714 eng.pdf.

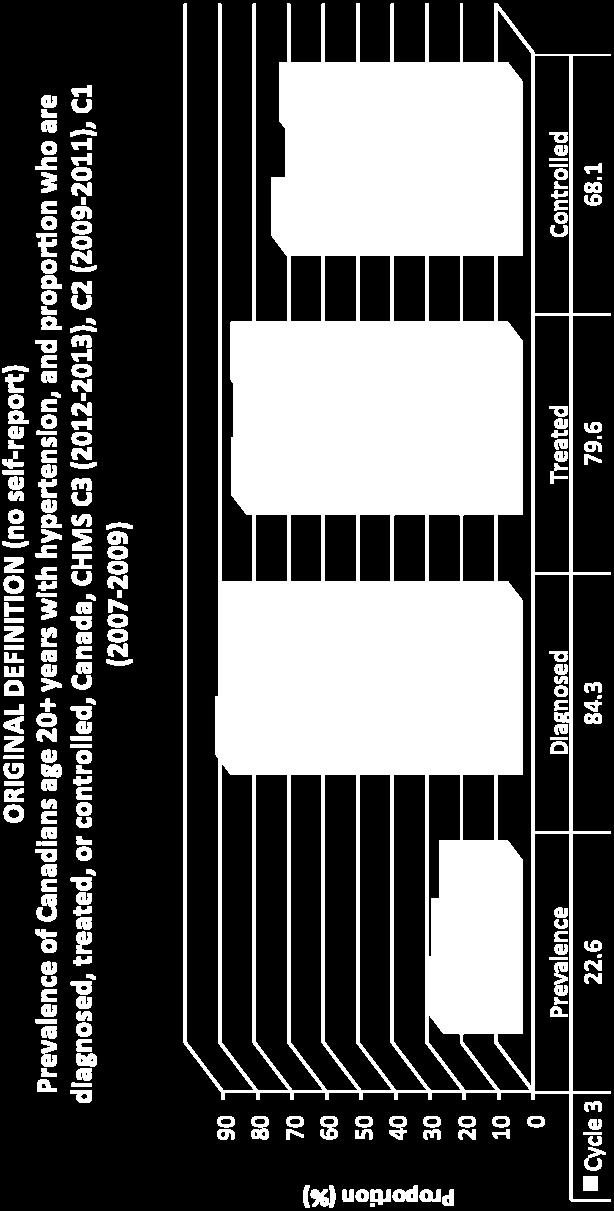
7 Hypertension In Canada: Latest Update
8 Question 55 y.o. female with hypertension and diabetes on three drugs. BP in the office is 165/95 mmhg. BP at home 120/72. Feels well. Next action: 1.Increase drug doses or add another agent 2.Trust home BP no changes 3.Get ABPM 4.2 or 3
9 What s new? CHEP 2015 Recommendations Clinic blood pressures should be using electronic (oscillometric) monitors The diagnosis of hypertension should be based on out ofoffice measurements The management of hypertension is all about global cardiovascular risk management and vascular protection including advice and treatment supporting smoking cessation Treatment of atherosclerotic renal artery stenosis is primarily medical 2015
10 BP measurement methods Office (attended, OBPM) Auscultatory (mercury, aneroid) Oscillometric (electronic) Office Automated (unattended, AOBP) Oscillometric (electronic) Ambulatory (ABPM) Home (HBPM) For information on blood pressure measurement devices: monitors/bp monitors/ 2015
 Oscillometric")

11 BP measurement methods Office (attended, OBPM) Auscultatory (mercury, aneroid) Oscillometric (electronic) monitors/bp monitors/ 2015



12 Recommended automated blood pressure monitors for home blood pressure measurement Please refer to for a complete list of devices endorsed by Hypertension Canada.
13 New 2015 Recommendation: BP Measurement Office BP measurement (OBPM): Measurement using electronic (oscillometric) upper arm devices is preferred to auscultatory devices (Grade C). 2015

. 4.")
14 Blood Pressure Assessment: Patient preparation and posture Standardized Preparation: Patient 1. No acute anxiety, stress or pain. 2. No caffeine, smoking or nicotine in the preceding 30 minutes. 3. No use of substances containing adrenergic stimulants such as phenylephrine or pseudoephedrine (may be present in nasal decongestants or ophthalmic drops). 4. Bladder and bowel comfortable. 5. No tight clothing on arm or forearm. 6. Quiet room with comfortable temperature 7. Rest for at least 5 minutes before measurement 8. Patient should stay silent prior and during the procedure Canadian Hypertension Education Program Recommendations 14
15 Manual OBPM is inaccurate Up to 20 studies in the past 4 decades have studied the errors observed in routine office auscultatory measurement, both in nurses and physicians, due to issues concerning the observer the preparation of the patient the technique and the device used Leads to misclassification of BP Armstrong RS, et al. Int J Nursing Practice 2002;8: Gillespie A and Curzio J. Nursing Standard 1998;12:35-7 Gleichmann SI, et al. J Hypertens 1989;7(S3):S99-S102 Villegas I, et al. Hypertension 1995;26: Dreveniiorn E, et al. J Clinical Nursing 2001;10: McKay DW, et al. Medical Education 1992;26: McKay DW, et al. J Hum Hypertens 1990;4: Kemp F, et al. Professional Nurse 1994;9:521-4 Campbell NC, et al. AJH 2005;18:1522-7
16 Auscultatory OBPM is inaccurate In the real world, the accuracy of auscultatory OBPM can be adversely affected by provider, patient and device factors such as: too rapid deflation of the cuff digit preference with rounding off of readings to 0 or 5 also, mercury sphygmomanometers are being phased out and aneroid devices are less likely to remain calibrated Consequence: Routine auscultatory OBPMs are 9/6 mm Hg higher than standardized research BPs (primarily using oscillometric devices) Myers MG, et al. Can Fam Physician 2014;60:
17 Keys to accurate OBPM Use standardized measurement techniques and validated equipment Measurement using electronic (oscillometric) upper arm devices is preferred over auscultation The first reading should be discarded and the latter two averaged. 2015
")

")

18 Out-of-office Assessment is the Preferred Means of Diagnosing Hypertension Elevated BP Reading(s) office, home or pharmacy Hypertension Visit 1 History, Physical Examination and Diagnostic Tests BP 180/110 Hypertension AOBP 135/85 OBPM 140/90 Yes No No Hypertension (Annual BP Measurement Recommended) Out-of-Office Assessment ABPM (preferred) HBPM Diagnostic Series Clinic BP as alternate method (If ABPM or HBPM is not available)
19 Normal Values ABPM 130/80 overall 135/85 daytime 120/70 nighttime HBPM 135/
20 Out of office BP measurements are more highly correlated with BP related risk SBP DBP Mule et al. J Cardiovasc Risk 2002;9:
21 ABPM predicts CV risk better than OBPM For every 10-mmHg increase in 24h ABPM SBP, adjusted HR for daytime 1.12 ( ) and 1.21 ( ) for night-time For every 5-mmHg increase in 24h ABPM DBP, adjusted HR for daytime 1.02 ( ) and 1.09 ( ) for night-time Dolan E, et al. Hypertension 2005;46: Adjusted for clinic BP
 Eur Heart J 2005;26:2026 31 Ohkubo T, et al. (Ohasama) J Hypertens 1998;16:971-5 Bobrie G, et al.")
22 HBPM predicts CV risk better than OBPM Niiranen T J et al. Hypertension. 2010;55: Asayama K, et al. (Ohasama) Eur Heart J 2005;26: Ohkubo T, et al. (Ohasama) J Hypertens 1998;16:971-5 Bobrie G, et al. Arch Intern Med 2001;161:
23 Only relying on office pressures misses out on white coat and masked hypertension 200 Ambulatory BP mmhg Masked Hypertension Normotension True Hypertension White Coat Hypertension Manual Office BP mmhg From Pickering et al. Hypertension 2002;40:
24 The prognosis of white coat and masked hypertension CV events per 1000 patient year CV Events 0 Normal 23/685 White coat 24/656 Uncontrolled 41/462 Masked 236/3125 Okhubo et al. J. Am. Coll. Cardiol. 2005;46;
25 Characteristics of ABPM and HBPM ABPM HBPM Cost Relatively high Relative low Reporting bias + Patient training Minimal + Wide availability + Diagnostic ability + + White coat phenomena and + + Masked HTN BP variability Short term Day to day Nocturnal BP + Prognostic ability + + Repeatability/long term follow up Low High (treatment adjustment and f/u) Improves long term adherence to drug therapy and hypertension control rates
26 Summary of evidence Out of office is needed to identify white coat hypertension (and to rule out masked hypertension) ABPM has better predictive ability than OBPM HBPM has better predictive ability than OBPM 2015
27 A standardised approach should be used for ABPM (Grade D) The appropriate sized cuff should be applied to the non dominant arm unless the SBP difference between arms is >10 mm Hg, in which case the arm with the highest value obtained should be used The device should be set to record for a duration of at least 24 hours with the measurement frequency set at a minimum of 20 minute intervals during the day and 30 minutes at night A patient reported diary to define daytime (awake), night time (sleep), activities, symptoms and medication administration is useful for study interpretation. Daytime and night time should preferentially be defined using the patient s diary. Alternatively, pre defined thresholds can be used (e.g. 08:00 to 22:00 for daytime and 22:00 to 8:00 for night time). The ABPM report should include all of the individual BP readings (both numerically and graphically), the percentage of successful readings, the averages for each time frame (daytime, night time, 24 hours) and the dipping percentage (the percentage the average BP changed from daytime to night time). Criteria for a successful ABPM study are: At least 70% of the readings are successful AND At least 20 daytime readings and 7 night time readings are successful
28 VII. Suggested Protocol for Home Measurement of Blood Pressure for the diagnosis of hypertension Home blood pressure values should be based on: Duplicate measures, Morning and evening, For an initial 7-day period. First day home BP values should not be considered. The following six days blood pressure readings should be averaged Average BP equal to or over 135/85 mmhg should be considered elevated (for those patients whose clinic BP target is less than 140/90 mmhg).


29 Home BP Telemonitoring Omboni and Ferrari. Curr Hypertens Rep 2015
30 CHEP 2015 Recommendations What s new? Assess clinic blood pressures using electronic (oscillometric) monitors The diagnosis of hypertension should be based on out ofoffice measurements The management of hypertension is all about global cardiovascular risk management and vascular protection including advice and treatment for smoking cessation Treatment of atherosclerotic renal artery stenosis is primarily medical. 2015
31 New 2015 Recommendation: Vascular Protection Tobacco use status of all patients should be updated on a regular basis and health care providers should clearly advise patients to quit smoking. 2015
32 Effect of advice on smoking cessation rates Cochrane Database Syst Rev May 31;5:CD doi: / CD pub
33 New 2015 Recommendation: Vascular Protection Advice in combination with pharmacotherapy (e.g., varenicline, bupropion, nicotine replacement therapy) should be offered to all smokers with a goal of smoking cessation. 2015
34 Cochrane network meta analysis 2014 Kate Cahill et al Nicotine replacement therapy (NRT), antidepressant bupropion, and nicotine receptor partial agonist varenicline Impact on long term abstinence 6 months or longer Synthesis of 12 Cochrane reviews 267 studies Over 10,000 participants 2015
35 Network meta analysis of smoking cessation pharmacotherapies studies Cochrane Database Syst Rev May 31;5:CD doi: / CD pub4 2015

36 Smoking Cessation
37 What s new? CHEP 2015 Recommendations Clinic blood pressures should be using electronic (oscillometric) monitors The diagnosis of hypertension should be based on out ofoffice measurements The management of hypertension is all about global cardiovascular risk management and vascular protection including advice and treatment supporting smoking cessation Treatment of atherosclerotic renal artery stenosis is primarily medical 2015
38 CHEP Recommendations 2015: Therapy Patients with hypertension attributable to atherosclerotic renal artery stenosis (RAS) should be primarily medically managed because renal angioplasty and stenting offer no benefits over optimal medical therapy alone. 2015
39 Whats Old but Still Important? Treatment Thresholds and Targets
40 Question 83 y.o. female with hypertension,diabetes and CKD. Which is the best answer: 1.SBP target is <130 2.SBP target is <140 3.SBP target is <150 4.It depends.
41 Question 33 y.o. female elevated BP average is 150/93. Otherwise well. Which is the best answer: 1.Drugs should be started now 2.Drugs should be started if BP >160/100 3.Drugs should be started in 6 months if BP still at this level

42 Treat the Patient not Just the Number It is much more important to know what sort of a patient has a disease than what sort of a disease a patient has. Sir William Osler ( )
43 Usual blood pressure threshold values for initiation of pharmacological treatment Population SBP > DBP > Diabetes High risk (TOD or CV risk factors) Low risk (no TOD or CV risk factors) Very elderly* ( 80 yrs.) 160 NA TOD=target organ damage *This higher treatment target for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk benefit analysis. 2015
44 Recommended Treatment Targets Treatment consists of health behaviour ±pharmacological management Population SBP < DBP < Diabetes All others < 80 yrs. (including CKD) Very elderly ( 80 yrs.) 150 NA In patients with coronary artery disease be cautious when lowering blood pressure if diastolic blood pressures are < 60mmHg 2015
45 BP is a continuous risk factor Stroke IHD Prospective Studies Collaboration. Lancet 2002

46 BP Lowering Benefits and Baseline Risk 11 trials; 51,917 patients Blood Pressure Treatment Trialists Collaboration. Lancet 2014.
47 BP Lowering Benefits and Baseline Risk 11 trials; 51,917 patients NNT varies from 70 (<11%) to 26 (>21%) Blood Pressure Treatment Trialists Collaboration. Lancet 2014.
48 Canadian Hypertension Education Program Thresholds For Initiating Drug Therapy in Non Very Elderly, Non DM Patients 1. Prescribe for DBP 100 or SBP 160 if no TOD or risk factors (Grade A). 2. Strongly consider for DBP 90 and TOD or other CV risk factors (Grade A). 3. Strongly consider for SBP and TOD (Grade C).
49 II. Indications for Pharmacotherapy Usual blood pressure threshold values for initiation of pharmacological treatment Population SBP DBP Diabetes High risk (TOD or CV risk factors) Low risk (no TOD or CV risk factors) Very elderly 160 NA TOD=target organ damage *This higher treatment target for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk-benefit analysis. 2014

50 Treatment of Grade 1 HTN 10 studies; subjects Sundstrom et al. Ann Intern Med 2015
51 II. Indications for Pharmacotherapy after diagnosis of hypertension (1) Patients at low risk with stage 1 hypertension ( /90-99 mmhg) lifestyle modification can be the sole therapy. Patients with target organ damage (e.g. left ventricular hypertrophy) ( /90-99 mmhg) Treat with pharmacotherapy Patients with chronic kidney disease should be considered for pharmacotherapy if the blood pressure is equal or over 140/90 mmhg Patients with diabetes should be considered for pharmacotherapy if the blood pressure is equal or over 130/80 mmhg
52 II. Indications for Pharmacotherapy Usual blood pressure threshold values for initiation of pharmacological treatment Population SBP DBP Diabetes High risk (TOD or CV risk factors) Low risk (no TOD or CV risk factors) Very elderly 160 NA TOD=target organ damage *This higher treatment target for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk-benefit analysis. 2014
53 II. Indications for Pharmacotherapy Recommended Treatment Targets Treatment consists of health behaviour ±pharmacological management Population SBP DBP Diabetes <130 <80 All others < 80 y.a. (including CKD) <140 <90 Very elderly ( 80 years) <150* NA *This higher treatment target for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk benefit analysis. 2014

54 HYVET Trial Beckett et al. NEJM 2007
55 HYVET Trial Beckett et al. NEJM 2007

56 HYVET Trial Beckett et al. NEJM 2007
57 Diabetes
58 II. Indications for Pharmacotherapy Recommended Treatment Targets Treatment consists of non pharmacological ± pharmacological management Population SBP DBP Diabetes Grade C <130 <80 Very elderly ( 80 years) <150* <90 All others (including CKD) <140 <90 Grade A *This higher treatment threshold for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk benefit analysis.

59 HOT: Study Design and Treatment Arms Hansson. Lancet 1998

60 HOT: Results in DM2 Subgroup NNT 80 Hansson. Lancet 1998
61 ACCORD. NEJM. 2010
62 ACCORD 4733 patients with DM2 Standard BP (140 systolic) versus intensive (120) Factorial design also testing the efficacy of fibrates 4.7 years mean follow-up
63 ACCORD: BP Through Follow-up ACCORD. NEJM 2010

64 ACCORD: Results ACCORD. NEJM 2010


65 More Intensive Control in DM 13 trials; 37,736 patients Bangalore et al. Circulation 2011 NNT approx 185 over about 4y


66 More Intensive Control in DM 13 trials; 37,736 patients Bangalore et al. Circulation 2011 NNT approx 185 over about 4y
67 II. Indications for Pharmacotherapy Recommended Treatment Targets Treatment consists of non pharmacological ± pharmacological management Population SBP DBP Diabetes Grade C <130 <80 Very elderly ( 80 years) <150* <90 All others (including CKD) <140 <90 Grade A *This higher treatment threshold for the very elderly reflects current evidence and heightened concerns of precipitating adverse effects, particularly in frail patients. Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based upon an individualized risk benefit analysis.
68 Bottom Line: Thresholds and Targets These are our best guess in terms of thresholds and targets for most patients You should exercise your clinical judgment and tailor to individual patients 2015

69 hypertension.ca For patients: free access to the latest information and resources For professionals: Access an accredited 15.5 hour interdisciplinary training program Sign up for free monthly news updates, featured research and educational resources Become a member for special privileges and savings 2015
Update on HTN and ABPM. Raj Padwal Division of General Internal Medicine University of Alberta
 Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
A CASE-BASED AND PEDAGOGICAL APPROACH TO TEACHING NEW PRACTICE GUIDELINES
 A CASE-BASED AND PEDAGOGICAL APPROACH TO TEACHING NEW PRACTICE GUIDELINES Presented By: Tara Baldisera, Sheldon Tobe and Jennifer Zymantas April 8, 2016 Conflict of Interest Declaration: Dr. Sheldon Tobe:
A CASE-BASED AND PEDAGOGICAL APPROACH TO TEACHING NEW PRACTICE GUIDELINES Presented By: Tara Baldisera, Sheldon Tobe and Jennifer Zymantas April 8, 2016 Conflict of Interest Declaration: Dr. Sheldon Tobe:
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
& Wilkins. a Division of Cardiology, Schulich Heart Centre, b Institute for Clinical and
 Original article 333 Optimum frequency of office blood pressure measurement using an automated sphygmomanometer Martin G. Myers a, Miguel Valdivieso a and Alexander Kiss b,c Objective To determine the
Original article 333 Optimum frequency of office blood pressure measurement using an automated sphygmomanometer Martin G. Myers a, Miguel Valdivieso a and Alexander Kiss b,c Objective To determine the
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls
 Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right. Anthony J. Viera, MD, MPH, FAHA Professor and Chair
 Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Is Traditional Clinic Blood Pressure Dead?
 Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN?
 BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
STATE OF THE ART BP ASSESSMENT
 STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
가정혈압의활용 CARDIOVASCULAR CENTER. Wook Bum Pyun M.D., Ph.D. HOME BLOOD PRESSURE MONITORING. Ewha Womans University, school of Medicine
 가정혈압의활용 HOME BLOOD PRESSURE MONITORING CARDIOVASCULAR CENTER Wook Bum Pyun M.D., Ph.D. pwb423@ewha.ac.kr Ewha Womans University, school of Medicine Non-Invasive Blood Pressure Measurement 5-20% Resistant
가정혈압의활용 HOME BLOOD PRESSURE MONITORING CARDIOVASCULAR CENTER Wook Bum Pyun M.D., Ph.D. pwb423@ewha.ac.kr Ewha Womans University, school of Medicine Non-Invasive Blood Pressure Measurement 5-20% Resistant
Hypertension and Atrial Fibrillation
 Hypertension and Atrial Fibrillation Sheldon Tobe MD, MScCH (HPTE), FRCPC, FACP, FASH Hypertension and Nephrology HSF/NOSM Chair in Aboriginal and Rural Health Research Professor in Medicine, University
Hypertension and Atrial Fibrillation Sheldon Tobe MD, MScCH (HPTE), FRCPC, FACP, FASH Hypertension and Nephrology HSF/NOSM Chair in Aboriginal and Rural Health Research Professor in Medicine, University
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
2020 HYPERTENSION HIGHLIGHTS
 2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
White coat and masked hypertension
 White coat and masked hypertension Conflict of interest Support from Spacelabs, Microlife. Honoraria from Novartis, Elpen, Boeringer-Ingelheim, CANA, Lilly, MSD, Sanofi, Menarini, Ciezi, Astra-Zeneca.
White coat and masked hypertension Conflict of interest Support from Spacelabs, Microlife. Honoraria from Novartis, Elpen, Boeringer-Ingelheim, CANA, Lilly, MSD, Sanofi, Menarini, Ciezi, Astra-Zeneca.
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK. Michael Smolensky, Ph.D. The University of Texas Austin & Houston
 AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
Use and Interpretation of Home Blood Pressure Monitoring
 Use and Interpretation of Home Blood Pressure Monitoring BLOOD PRESSURE in year 2015 PARAMETERS TODAY Gianfranco Parati University of Milano-Bicocca & Ospedale S.Luca, IRCCS, Istituto Auxologico Italiano
Use and Interpretation of Home Blood Pressure Monitoring BLOOD PRESSURE in year 2015 PARAMETERS TODAY Gianfranco Parati University of Milano-Bicocca & Ospedale S.Luca, IRCCS, Istituto Auxologico Italiano
Hipertensión enmascarada. Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona
 Hipertensión enmascarada Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona HTA enmascarada Definición Prevalencia Características clínicas Riesgo derivado Asociación con LOD Progresión
Hipertensión enmascarada Alejandro de la Sierra Hospital Mútua Terrassa Universitat de Barcelona HTA enmascarada Definición Prevalencia Características clínicas Riesgo derivado Asociación con LOD Progresión
ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION*
 Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Please do not hesitate to contact our dedicated service unit for more details regarding this program at
 The Blue Cross and Blue Shield Federal Employee Program (FEP) and the American Medical Association (AMA) have come together in a collaborative effort to provide physicians with resources designed to improve
The Blue Cross and Blue Shield Federal Employee Program (FEP) and the American Medical Association (AMA) have come together in a collaborative effort to provide physicians with resources designed to improve
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE
 GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Professor Medicine and Cardiovascular Diseases Director, Seinsheimer Cardiovascular Health
GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Professor Medicine and Cardiovascular Diseases Director, Seinsheimer Cardiovascular Health
KDIGO Controversies Conference on Blood Pressure in CKD
 KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Hypertension Putting the Guidelines into Practice
 Hypertension 2018 Putting the Guidelines into Practice Ally P.H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Faculty: Metabolism, Faculty Disclosure
Hypertension 2018 Putting the Guidelines into Practice Ally P.H. Prebtani Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University Canada Faculty: Metabolism, Faculty Disclosure
Current strategies for managing hypertension
 Eπίκαιρο Άρθρο Ambulatory blood pressure monitoring: the gold standard for the diagnosis and management of hypertension in general practice Eoin O Brien ABSTRACT Although ambulatory blood pressure measurement
Eπίκαιρο Άρθρο Ambulatory blood pressure monitoring: the gold standard for the diagnosis and management of hypertension in general practice Eoin O Brien ABSTRACT Although ambulatory blood pressure measurement
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Summary of recommendations
 Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
High blood pressure (BP) or
 or") Janusz Kaczorowski, PhD, Martin Dawes, MBBS, MD, FRCGP, Mark Gelfer, MD, FRCPC Measurement of blood pressure: New developments and challenges Automated blood and out-of-office BP measurement can both play
Janusz Kaczorowski, PhD, Martin Dawes, MBBS, MD, FRCGP, Mark Gelfer, MD, FRCPC Measurement of blood pressure: New developments and challenges Automated blood and out-of-office BP measurement can both play
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Blood Pressure Measurement Does it matter where you do it or how often?
 Blood Pressure Measurement Does it matter where you do it or how often? James (Jim) M. Wright Coordinating Editor Cochrane Hypertension Group Conflict of Interest First half evidence based, no conflicts.
Blood Pressure Measurement Does it matter where you do it or how often? James (Jim) M. Wright Coordinating Editor Cochrane Hypertension Group Conflict of Interest First half evidence based, no conflicts.
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
IMET 2000 PAL International Medical Education Trust Palestine What the GP Should Know about Hypertension
 What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
Hypertension Canada CHEP Guidelines for the Management of Hypertension. What s new in the treatment of hypertension? What s still really important?
 Hypertension Canada CHEP Guidelines for the Management of Hypertension What s new in the treatment of hypertension? What s still really important? 1 Presenter Disclosure Relationships with commercial interests:
Hypertension Canada CHEP Guidelines for the Management of Hypertension What s new in the treatment of hypertension? What s still really important? 1 Presenter Disclosure Relationships with commercial interests:
Home blood pressure measurement with oscillometric upper-arm devices
 REVIEW Home blood pressure measurement with oscillometric upper-arm devices R.L. Braam, Th. Thien *# Department of Internal Medicine, University Medical Centre St Radboud, PO Box 9101, 6500 HB Nijmegen,
REVIEW Home blood pressure measurement with oscillometric upper-arm devices R.L. Braam, Th. Thien *# Department of Internal Medicine, University Medical Centre St Radboud, PO Box 9101, 6500 HB Nijmegen,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice
 Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY. Introduction. Patients and Methods
 Vol. 2, Issue 1, pages 31-36 ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY By Alejandro de la Sierra, MD Luis M. Ruilope, MD Hypertension Units, Hospital Clinico, Barcelona & Hospital 12 de Octubre,
Vol. 2, Issue 1, pages 31-36 ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY By Alejandro de la Sierra, MD Luis M. Ruilope, MD Hypertension Units, Hospital Clinico, Barcelona & Hospital 12 de Octubre,
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Home Blood Pressure Log
 Home Blood Pressure Log 2 You or your health care professional may want to monitor your blood pressure at home twice a day for a week or more before appointments to accurately confirm your average blood
Home Blood Pressure Log 2 You or your health care professional may want to monitor your blood pressure at home twice a day for a week or more before appointments to accurately confirm your average blood
Prognostic significance of blood pressure measured in the office, at home and during ambulatory monitoring in older patients in general practice
 (2005) 19, 801 807 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Prognostic significance of blood pressure measured in the office, at home and
(2005) 19, 801 807 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Prognostic significance of blood pressure measured in the office, at home and
AFFORDABLE TECHNOLOGY
 World Health Organization AFFORDABLE TECHNOLOGY BLOOD PRESSURE MEASURING DEVICES FOR LOW RESOURCE SETTINGS CARDIOVASCULAR DISEASES Blood Pressure Measurement in Low Resource Settings Annex 1: Blood Pressure
World Health Organization AFFORDABLE TECHNOLOGY BLOOD PRESSURE MEASURING DEVICES FOR LOW RESOURCE SETTINGS CARDIOVASCULAR DISEASES Blood Pressure Measurement in Low Resource Settings Annex 1: Blood Pressure
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
THE NEW ARMENIAN MEDICAL JOURNAL DISTRIBUTION, AWARENESS, TREATMENT, AND CONTROL OF ARTERIAL HYPERTENSION IN YEREVAN (ARMENIA)
") THE NEW ARMENIAN MEDICAL JOURNAL Vol.5 (2011), Nо 2, p.29-34 DISTRIBUTION, AWARENESS, TREATMENT, AND CONTROL OF ARTERIAL HYPERTENSION IN YEREVAN (ARMENIA) Zelveian P.H. 1, 2, Podosyan G.A. 2 1 Institute
THE NEW ARMENIAN MEDICAL JOURNAL Vol.5 (2011), Nо 2, p.29-34 DISTRIBUTION, AWARENESS, TREATMENT, AND CONTROL OF ARTERIAL HYPERTENSION IN YEREVAN (ARMENIA) Zelveian P.H. 1, 2, Podosyan G.A. 2 1 Institute
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Copyright Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
 Devices and technology 261 Validation of the ROSSMAX blood pressure measuring monitor according to the European Society of Hypertension International Protocol for Validation of Blood Pressure Measuring
Devices and technology 261 Validation of the ROSSMAX blood pressure measuring monitor according to the European Society of Hypertension International Protocol for Validation of Blood Pressure Measuring
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations
 Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Chapter 2 Home (Self) Monitoring of Blood Pressure
 Monitoring of Blood Pressure") Chapter 2 Home (Self) Monitoring of Blood Pressure Gianfranco Parati and Juan Eugenio Ochoa Introduction Elevated blood pressure (BP) levels represent the most important modifiable risk factor for cardiovascular
Chapter 2 Home (Self) Monitoring of Blood Pressure Gianfranco Parati and Juan Eugenio Ochoa Introduction Elevated blood pressure (BP) levels represent the most important modifiable risk factor for cardiovascular
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Blood Pressure Competency Training
 Blood Pressure Competency Training WORKBOOK Table of Contents 3..... Introduction 4..... Background 6..... Equipment Accurate blood pressure What impacts a patient s blood pressure Strategies for proper
Blood Pressure Competency Training WORKBOOK Table of Contents 3..... Introduction 4..... Background 6..... Equipment Accurate blood pressure What impacts a patient s blood pressure Strategies for proper
, 13TH EUGMS CONGRESS NICE GOALS OF ANTIHYPERTENSIVE TREATMENT IN THE FRAIL IS SPRINT APPLICABLE? CONTRA
 21.09.2017, 13TH EUGMS CONGRESS NICE GOALS OF ANTIHYPERTENSIVE TREATMENT IN THE FRAIL IS SPRINT APPLICABLE? CONTRA Prof. Dr. Ute Hoffmann Klinik für Allgemeine Innere Medizin und Geriatrie Nephrologie/Angiologie/Diabetologie/Endokrinologie
21.09.2017, 13TH EUGMS CONGRESS NICE GOALS OF ANTIHYPERTENSIVE TREATMENT IN THE FRAIL IS SPRINT APPLICABLE? CONTRA Prof. Dr. Ute Hoffmann Klinik für Allgemeine Innere Medizin und Geriatrie Nephrologie/Angiologie/Diabetologie/Endokrinologie