Paediatric Advanced Life Support
|
|
|
- Catherine Flowers
- 5 years ago
- Views:
Transcription
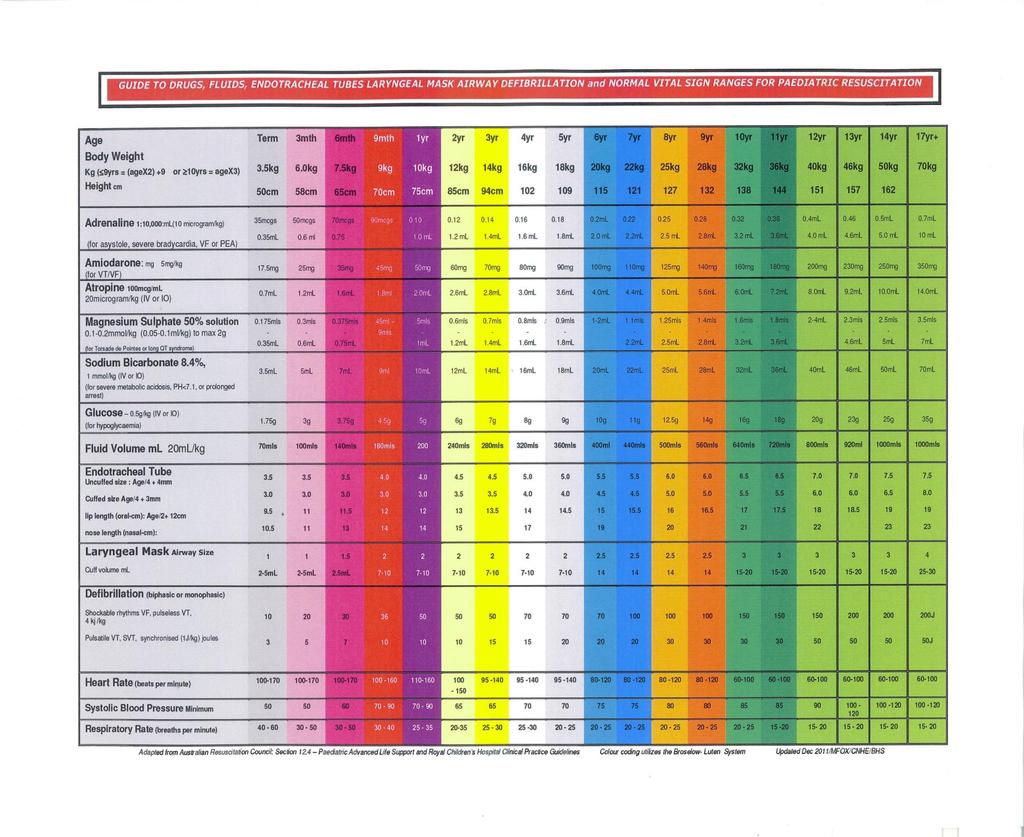
1 Paediatric Advanced Life Support CNHE- Ballarat Health Services Valid from 1 st March 2016 to 31 st June
2 Pathways leading to cardiac arrest in childhood 2
3 Age Groups Neonate: Newborn - 28days Infant: 29 days - 1 year Child: 1-8 years Older children: >9yrs (over 12 can be treated as per adults) 3
4 Rapid Estimation of Body Weight in Paeds NEWBORN 3.5 KG 6 MONTHS 7KG 1 YEAR 10KG 9 YEARS & LESS 2 x age in years YEARS & OVER Age x 3.3 = KG Weight (in kg) = 2 x age in years + 8 4
5 5
6 Anatomical differences - Airway Large head, short neck, large tongue, soft palate < 6months nasal breathers, narrow nasal passages 3-8yrs adenotonsillar hypertrophy Young children epiglottis is horseshoe shaped & projects posteriorly (intubation difficult) Larynx high & anterior Trachea short and soft Cricoid ring is the narrowest point of the paed airway 6
7 Anatomical differences-breathing Upper & lower airways are relatively small Infants rely on diaphragmatic breathing, supported by abdominal muscles Ribs are more horizontal in infants The chest wall is highly compliant therefore rib # s must be the result of great force this will result in severe pulmonary injury flail chest is more common and poorly tolerated in comparison to adults 7
8 Anatomical differences- Breathing Upper and lower airways are small & more easily obstructed. They have an increased work of breathing Muscles are more likely to fatigue as they have fewer type I fibres Horizontal ribs contribute less to chest expansion Compliant chest wall can equal serious pulmonary injury without rib # s 8
9 Anatomical differences - Circulation Circulating blood volume per kg of body weight is 70-80ml/kg Even small amounts of blood loss are critical Body surface area (BSA) Small children have a greater BSA in relation to their physical size The child will lose heat more rapidly & consequently be more prone to hypothermia 9
10 Physiological differences - Respiratory The increased respiratory rate results in a higher metabolic rate and higher 0 2 consumption With an increase in work of breathing the compliant chest wall allows sternal recession & rib space indrawing resulting in less negative intrathoracic pressure Paediatric Normal Respiratory Values <1yrs breaths/min >
11 Physiological differences - Respiratory Harder to generate negative pressures & Less negative pressure results in decreased lung volumes and small airway closure Respiratory insufficiency will lead to hypoxia, acidosis and eventually resp arrest 11
12 Physiological differences - Cardiovascular Infants have a small and relatively fixed stroke volume; cardiac output is directly related to heart rate Age Heart rate Systolic bp <1yr bpm 70-90sys > BP ~ 80 + ( age in yrs x 2) 12
13 Physiological differences - Cardiovascular Infants respond to fluids in a blunted manner Because stroke volume cannot increase greatly to improve CO By age 2 myocardial response to fluid are similar to adults 13
14 Circulation- insufficiency By the time a child has a cardiac arrest from circulatory insufficiency, they have had a substantial period of hypoxia & acidosis resulting in myocardial depression and finally causing cardiac arrest Hypotension is a late & preterminal sign 14
15 Circulation- insufficiency Compensated shock tachycardia cool extremities prolonged capillary refill >2-3 secs weak peripheral pulses compared with central normal BP As compensation fails depressed mental status urine output < 1ml/kg child & < 2ml/kg infants metabolic acidosis tachypnoea weak central pulses Decompensated the above plus hypotension 15
16 Psychological Fear, distress and anxiety in a child will result in an increase HR & respiratory rate Parents should be kept closely informed of events Parents should given the opportunity to be present during the resuscitation of their child in consultation with staff (ARC 2016) 16
17 Important Points Smaller functional respiratory reserve = hypoxia develops earlier than in adults Higher metabolic rate = higher O 2 demand Smaller airways = increased WOB Compliant thoracic cage = the generation of negative intrathoracic pressure is more difficult Respiratory arrest is the most common cause of arrest in children 17
18 Airway Assessment The aim is to establish a clear and open airway CLEARING the airway Visualise the nose and mouth Clear oral and nasal secretions with suction No blind finger sweeps in infants <1yr Magill s forceps may be used to extract foreign body OPEN the airway Head tilt-chin lift (no pressure on soft tissue) or Jaw thrust Position Infant: neutral position avoid hyperextension Children: head tilt increases with age 18

19 Airway Management - Infant Clear and open the airway If airway not open tilt head back very slightly Sniffing position 19

20 Airway Position - Child 20
21 Airway adjuncts Oropharyngeal: May be necessary to maintain an open airway when using bag-valve-mask ventilation in the unconscious patient with no cough or gag. Avoid due to potential oropharyngeal trauma only use if no cough or gag reflex is present measure centre of the lips to the angle of mandible In infants insert using a laryngoscope or tongue depressor and with the guedels airway the right side up 21
22 Breathing Assessment Once the airway has been cleared and opened If NO or inadequate respiratory effort commence rescue breathing (BVM) 2 breaths Then commence CPR 22
23 Breathing - Ventilation Use bag with volume at least 500ml infant & small children older children (9-14yrs) adult bag attach oxygen flow at 15L use only the force & tidal volume to make chest rise Observe bilateral rise and fall Minimise gastric inflation avoid high inspiratory pressures insert nasal/orogastric tube as soon as possible 23
24 Advanced Airway-ETT secures a patent airway reduces risk of aspiration facilitates adequate ventilation with 100% O 2 facilitates tracheal suctioning more practicable in prolonged resuscitation provides an alternative route for selected drugs de-emphasied by the ARC Do not delay CPR to put in an ETT 24
25 Advanced Airway-ETT If intubation cannot be accomplished easily continue to ventilate with 100% oxygen via bagvalve mask Endo tracheal intubation should not be attempted at the expense of prolonging hypoxaemia 25
26 ETT Uncuffed are preferred up until 8-10years During resus cuffed may be used (short term) Allow for a small air leak with cuffed & uncuffed ETT Uncuffed Internal diameter (mm)= (Age/4) + 4 Cuffed Internal diameter (mm)= (Age/4) + 3 Length (cm) = (Age/2) + 12 for an oral tube Length (cm) = (Age/2) + 15 for nasal tube Formula is suitable for ages over 1 year 26
27 ETT Larynx circular in cross section & narrowest part at cricoid ring rather than vocal cords ETT should give a relatively gas-tight fit in the larynx but should not be so tight in the larynx that no leak is audible or it may cause damage to the mucosa at the level of the cricoid ring and subsequent oedema on extubation Post resus allow a small leak Cuffed may be preferred with poor lung compliance 27
28 ETT Oral intubation during resuscitation is preferred quicker less likely to cause trauma, haemorrhage easier to replace than nasal tube Laryngoscopes straight blade is easier to use for intubation as it lifts the epiglottis straight blade may cause vagal stimulation curved blade moves the epiglottis forward - this is a more difficult technique 28
29 Advanced Airway Adjunct Laryngeal Mask Airway (LMA): generally not used in paed resuscitation can be life saving in the setting of can t intubate and can t ventilate does not provide definitive airway protection easily dislodged Can NOT be used as a route of drug administration 5kg size kg size kg size 2 > 20kg size
30 Circulation - Assessment absent signs of life, pallor and or cyanosis are suggestive of inadequate circulation if a pulse is not palpable or cannot be identified within 10secs or is < 60 bpm in an infant < 40 bpm in children Start immediate chest compressions at a minimal speed of 100 chest compressions per minute 30
31 Advanced Paediatric CPR ratio In the hospital setting BHS Acute site Two Health Care Providers 100% Oxygen with a Bag-Valve-Mask 2:15 2 ventilations /15compressions Aiming for a minimum speed of 100 chest compressions per minute Compressions pause for 2 ventilations 31
32 Advanced Paed CPR When an advanced airway is insitu (ETT) CPR is no longer delivered in cycles Compressions are continuous at a minimal speed of 100 chest compressions per minute with no pauses for ventilation Deliver about 10 breaths per min Avoid hyperventilation Minimise interruptions to compressions 32
33 Circulation - management Continue to assess circulation & attach cardiac monitor Gain IV/IO (intraosseous) access, attempt to obtain 2 sites - If IV access is not obtained within 60 seconds an IO route should be used for drug administration collect blood while getting IV/IO access 33
34 Circulation - management Fluid Management If hypovolaemia is suspected as the cause of the arrest; administer 20mls/kg bolus crystalloid Additional boluses should be titrated against response Fluid bolus-if more than 40mls/kg needed significant haemodilution may result equal to half the circulating volume 34
35 35
36 Paediatric Cardiac Arrest Algorithm Management Non-Shockable 36
37 Asystole/Symptomatic Bradycardia Heart rate <60 infant,<40 children If unresponsive to ventilation with O 2 CPR up to 2 mins, Adrenaline 10mcg/kg IV / IO initial & repeat dose every 4 mins ETT adrenaline100mcg/kg (as a last resort) IV Adrenaline infusion mcg/kg/min or higher Seek causes & correct 37
38 Asystole / Symptomatic Bradycardia continued Continue with adrenaline every 4mins Minimal interruptions to chest compressions Maintain adequate oxygenation Consider external pacing Correct reversible causes (as per adult) 38
39 Pulseless Electrical Activity (PEA) CPR - uninterrupted Adrenaline every 4 mins seek causes consider all H s & T s esp hypovolaemia, acidosis, dynamic hyperinflation & if trauma related:- tension pneumothorax & pericardial tamponade IV or IO bolus of crystalloid or colloid solution Consider external pacing 39
40 Paediatric Cardiac Arrest Algorithm Management Shockable 40
41 VF/Pulseless VT Unwitnessed / non-monitored arrest - Single shock 4j/kg Immediately followed by 2 mins CPR shock 4j/kg 2mins CPR & adrenaline 10mcg/kg every 4 mins shock 4j/kg & all subsequent shocks after each sequence of 2 mins of CPR Witnessed/ monitored arrest No stacked shocks. All shocks 4 j/kg all subsequent shocks 4j/kg after each sequence of 2 mins of CPR and adrenaline 41
42 VF/Pulseless VT continued Persistent or refractory VF Continue with uninterrupted CPR, with one DC shock every 2mins (if indicated by rhythm) and repeated adrenaline every 4mins Consider Amiodarone - 5mg/kg IV/IO after 3 rd shock MgSO mmol/kg IV/IO KCl mmol/kg IV/IO Consider Reversible Causes Establish advanced airway management 42
43 Supraventricular Tachycardia If severe hypotension immediate synchronised DC shock J/kg If circulation adequate vagal stimulation; infant & young child; ice water in plastic bag to face or carotid sinus massage older children perform valsalva eg blowing through a narrow straw/ into a 10ml syringe or carotid sinus massage Adenosine 0.1mg/kg (max 6mg) + 0.2mg/kg (max 12mg) IV/IO Amiodarone 5mg/kg over one hour followed by 5mcg/kg/min for the next 4 hours 43
44 SVT Most common non-arrest arrhythmia in children typically occurs in infancy or in children with congenital heart disease infant rate >= children rate >=180 SVT may be undetected in infants for a long period of time until they develop a low cardiac output Procainamide 15mg/kg may cause hypotension by vasodilation Ca channel blockers should not be used to treat SVT in infants & avoid in children as it may induce hypotension & cardiac depression 44
45 Pulsatile Ventricular Tachycardia Haemodynamically stable VT antiarrhythmic: amiodarone 5mg/kg IV over 20-60mins Pulse present, hypotensive & poor circulation synchronised DC shock 0.5-1j/kg sedate if conscious 45
46 ETT administration of Drugs Only if IV/IO not available Adrenaline / Atropine / Lignocaine only ALS drugs suitable for ETT administration Infant - make up to 1-2ml Child - make up to 2-5ml Large child - make up to 5-10ml Dilute with water for injection to increase the drug absorption Administration as per adult 46
47 Intraosseous injection of drugs and infusion of fluids Bone marrow has a rich blood supply & forms part of the peripheral circulation Drugs administered fast & at same concentrations as those administered IV IV fluids need to be administered under pressure (gravity sets are ineffective) Inject via a syringe 47
48 Intraosseous injection continued The antero-medial surface of the proximal or distal tibia are suitable puncture sites Iliac crest is suitable in older children, but rarely used Can be left insitu for up to 72 hours 48


49 EZI-IO 49

50 50
51 ALS drug therapy - Summary Adrenaline asystole, severe bradycardia, VF, pulseless VT & PEA 10mcg/kg IV/IO intervals 4 mins ETT 100mcg/kg infusion mcg/kg/min or higher Atropine Bradycardia 20mcg/kg IV/IO or 30mcg/kg ETT 51
52 ALS drug therapy - Summary Amiodarone shock resistant VF & pulseless VT 5mg/kg IV which may be repeated Can be used in the management of atrial tachycardias, SVT, stable VT 52
53 ALS drug therapy - Summary NaHCO 3 limited and unproven may be useful in severe metabolic acidosis ph< 7.1 or prolonged arrest 1mmol/kg IV/IO after adequate ventilation and chest compressions have been established Some evidence that it causes intracellular acidosis level of evidence for use in an arrest is very low 53
54 ALS drug therapy Bolus Dosages Magnesium mmol/kg IV/IO 10% Calcium Gluconate 0.7 ml/kg IV/IO 10% Calcium Chloride 0.2ml/kg IV/IO Glucose 0.5 g/kg IV/IO (5ml/kg of 10% glucose) Potassium 0.05 mmols/kg slow injection IV /IO FLUIDS crystalloid / colloid 20ml/kg IV/IO 54
55 Post Resuscitation Aims Preserve brain function, avoid secondary injury, diagnose & treat cause of arrest avoid hyperventilation (aim for normocarbia) Hypothermia (32-34c) 12-24hrs within 6hrs in children after cardiac arrest normoglycaemia treat seizures 55
56 56
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
Paediatric Resuscitation. EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009
 Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
Paediatric Resuscitation EMS Rounds Gurinder Sangha MD Paediatric Emergency Fellow June 18, 2009 Essentials of Resuscitation Airway Breathing Circulation AIRWAY Differences in Paediatric Airway Shorter
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PALS PRETEST. PALS Pretest
 PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Adult Advanced Cardiovascular Life Support. Emergency Procedures in PT
 Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Chapter 5 PEDIATRIC RESUSCITATION
 Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
PALS PROVIDER Course Study Guide/Pre-Test
 PALS PROVIDER Course Study Guide/Pre-Test *PLEASE COMPLETE AND BRING THIS DOCUMENT WITH YOU TO CLASS* Heartland CPR, llc 8101 NW 10 th St, Suite #C3 Oklahoma City, OK 73127 405-603-6666 contact@heartlandcpr.com
PALS PROVIDER Course Study Guide/Pre-Test *PLEASE COMPLETE AND BRING THIS DOCUMENT WITH YOU TO CLASS* Heartland CPR, llc 8101 NW 10 th St, Suite #C3 Oklahoma City, OK 73127 405-603-6666 contact@heartlandcpr.com
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Resuscitation in infants and children
 Resuscitation in infants and children The importance of respiratory support Dr. Simon Erickson Paediatric Intensive Care Princess Margaret Hospital for Children Paediatric cardiac arrests uncommon (~20/100,000)
Resuscitation in infants and children The importance of respiratory support Dr. Simon Erickson Paediatric Intensive Care Princess Margaret Hospital for Children Paediatric cardiac arrests uncommon (~20/100,000)
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
SAFE approach. Unresponsive? Shout or call for help. Open Airway. Not Breathing normally? 30 chest compressions. 2 rescue breaths
 Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
San Benito County EMS Agency Section 700: Patient Care Procedures
 Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005
 RESUSCITATION GUIDELINES 2005") THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010
 ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Advanced Life Support
 Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
PALS Study Guide 2016
 Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016
 HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016 CAPABILITIES Airway Management Finger sweep Head-tilt-chin lift Jaw-thrust
HEALTH PROFESSIONS COUNCIL OF SOUTH AFRICA PROFESSIONAL BOARD FOR EMERGENCY CARE CAPABILITIES OF EMERGENCY CARE PROVIDERS: JUNE 2016 CAPABILITIES Airway Management Finger sweep Head-tilt-chin lift Jaw-thrust
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Basic Airway Management
 Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Basic Airway Management Dr. Madhurita Singh, Assoc. Professor, Dept. of Critical Care, CMC Vellore. This is the first module in a series on management of airway and ventilation in critically ill patients.
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD
 ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
ABCDE HOW TO RECOGNISE AND TREAT THE SERIOUSLY ILL CHILD A B C D E Possible Problems Airway obstruction Partial or complete Foreign body Secretions/blood/vomit Infection Swelling e.g. anaphylaxis trauma
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Ventilating the paediatric patient. Lizzie Barrett Nurse Educator November 2016
 Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Outline of the 2005 European Resuscitation Council Guidelines
 Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Overview. Chapter 37. Advanced Airway Techniques. Sellick Maneuver 9/11/2012
 Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Chapter 37 Advanced Airway Techniques Slide 1 Sellick Maneuver Purpose Anatomic Location Technique Special Considerations Overview Advanced Airway Management of Adults Esophageal Tracheal Combitubes Tracheal
Paediatric Advanced Life Support SUPERSEDED
 Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
Pediatric Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Pediatric Emergencies Lesson Goal Explain special characteristics of infants and children to become both comfortable & efficient in treating pediatric emergencies Lesson Objectives Identify physical &
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Airway management. Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department
 Airway management Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department Airway management Airway management is the medical process of ensuring there is an open pathway between a patient
Airway management Dr. Dóra Ujvárosy Medical Unversity of Debrecen Emergency Department Airway management Airway management is the medical process of ensuring there is an open pathway between a patient
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9
 CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
ADVANCED LIFE SUPPORT
 ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
cardiopulmonary resuscitation by Centre CPR OLomouc
 cardiopulmonary resuscitation by Centre CPR OLomouc Epidemiology of cardiac arrest Europe- 40% from total death up to 75 y incidence out of hospital 38/100 000 inh. survival out of hospital 5 13 % survival
cardiopulmonary resuscitation by Centre CPR OLomouc Epidemiology of cardiac arrest Europe- 40% from total death up to 75 y incidence out of hospital 38/100 000 inh. survival out of hospital 5 13 % survival