High Value Care of GI Bleeding
|
|
|
- Sarah Alexander
- 5 years ago
- Views:
Transcription

1 High Value Care of GI Bleeding Bennie R. Upchurch MD, FACP, FASGE, AGAF, FACG Medical Director, GI Bleeding Program, Division of Gastroenterology, Nutrition, and Hepatology Ohio State University Wexner Medical Center
2 Objectives Accurately assess, triage and resuscitate the GI bleeding patient. Recognize common causes of GI bleeding and the approach in management. Understand and facilitate a multidisciplinary approach to management of the GI bleeding patient.
3 Acute Gastrointestinal Bleeding Annually ~ 300,000 hospitalizations and ~ 20,000 deaths in US Common cause for ICU admission and potentially lethal medical emergency Overall incidence: /100,000 pts/yr Incidence of UGI : LGI bleeding ~ 5:1 More common in elderly esp. men > 70 yrs, who comprise ~ 30 % of all pts with UGI bleeding Mortality rates over past yrs have been stable at ~ 7-10%
4 Initial Assessment of Severe UGIB 1. Resuscitation and stabilization 2. Assessment of severity and location of bleeding 3. Preparation for emergent upper endoscopy 4. Role of endoscopist - Localization and identification of the bleeding site - Control of active bleeding or high risk lesions - Stratification of the risk for rebleeding - Minimization of treatment-related complications - Treatment of persistent or recurrent bleeding
5 Initial Evaluation - History - Age: Elderly ( ischemia, cancer, diverticula) Young ( ulcers, esophagitis, varices) - Prior GI Bleeding - Previous gastrointestinal disease - Previous GI surgery - Underlying Medical Disorders ( esp - liver disease, CKD) - Meds : NSAIDS - ASA/Anticoagulant use - Symptoms: Abdominal pain, fever, wt loss, anorexia, epistaxis, hematuria etc - Allergies
6 Physical examination - Hemodynamics with a thorough cardiopulmonary exam - Skin ( spider angiomata, purpura, cutaneous telangiectasias /pigmentation) - Abdomen ( ascites, tenderness, masses ) - Digital Rectal exam
7 Initial Patient Care/Management - Appropriate IV access: 2 large bore I.V catheters - IV fluids (NS/LR) and/or blood product resuscitation. ( Target HCT 30% in elderly/ 25-30% in young adults and pts with in Portal HTN ) - Continuous cardio-pulm monitoring for those with coronary risk factors with supplemental O2. - Frequent vital signs / urine output monitoring. - Consider intubation in those with altered mental status or brisk bleeding.
8 Labs and Studies Complete blood count ( check MCV) and electrolytes ( BUN >> Cr ), Iron studies. Coagulation Panel: PT/INR Type + screen or type + cross-match blood EKG for patients > 50 yrs or risk factors for heart disease. Abdominal radiographs usually not indicated
9 Naso Gastric Lavage - 79% sensitivity and 55% specificity for active bleeding - Positive NGL does not provide etiology - A non bloody aspirate in ~ 25% of UGIB - A bile aspirate does not R/O UGIB - NO evidence based data that NGL affects outcome
10 Increasing age - Age > 70 yrs Predictors of Mortality Concurrent active major organ disease Preexisting hospitalization ( mortality rate ~ 34% ) Passing frequent frank blood. Esp if - Shock or Orthostatic hypotension Variceal vs. Non variceal ( eg. Variceal bleed has mortality rate of 30% during initial hosp, with 1 yr mortality rate of ~ 60% ) Requiring emergency surgery for GIB Active bleeding / Transfusion requirement 4 or more red cell units in the first 24 hours 2 or more units for rebleeding event 6-8 units total
11 Forrest Classification System with Respective Prognosis Forrest Classification Type I: Active Bleed Ia: Spurting Bleed Ib: Oozing Bleed Rebleeding Incidence Surgical Requirement % 35% 11% Incidence of Death Type II: Recent Bleed Ila: Non-Bleeding Visible Vessel (NBVV) Ilb: Adherent Clot 40-50% 34% 11% 20-30% 10% 7% Type III: Lesion without Bleeding Flat Spot Clean Base 10% 6% 3% 5% 0.5% 2%



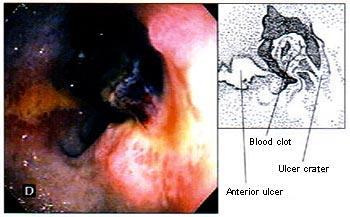
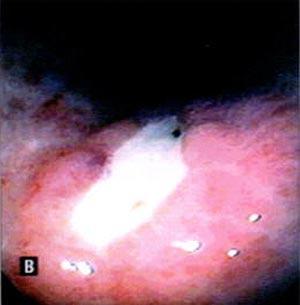

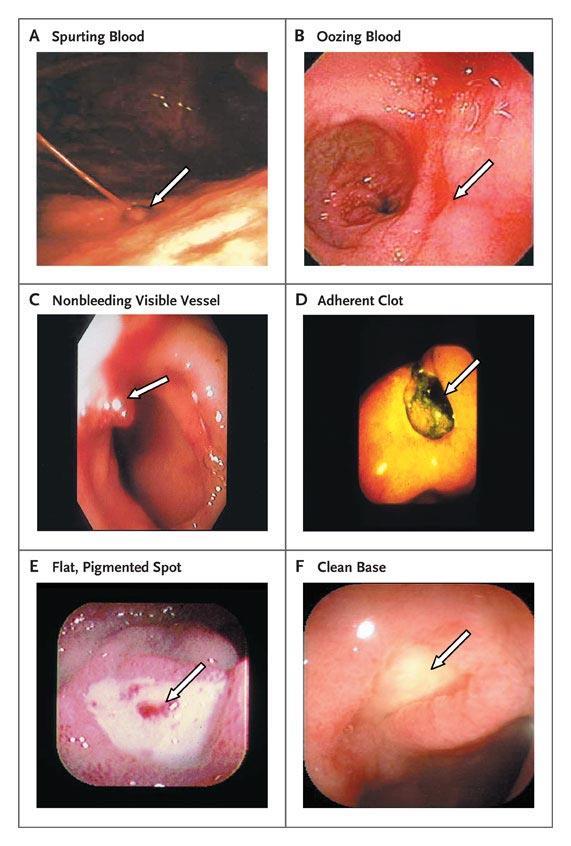
12 The Forrest Classification of Peptic Ulcers (Stigmata of recent hemorrhage)
13 Prognostic Features of GD Ulcers Ulcer size > 1 cm is associated with increased rebleeding and mortality Endoscopic hemostasis is less successful in ulcers > 2 cm in size Greatest re-bleeding risk from ulcers is within first 72 hours
14 H. pylori (H.P) and PUD Some studies suggest rebleeding less with H. pylori Rx than PPI TX. NSAID users infected with H.P has ~ two-fold risk of ulcer bleeding. ASGE guidelines suggest that all pts with PUD should be checked and treated for H.pylori. ( Class A rec ) Note rapid urease tests have reduced sensitivity in acute GIB. Use tests of active infection.to r/o infection.
15 PUD and NSAIDS / ASA Mechanism : Reduced production of cycloxygenase generated cytoprotective PG, platelet dysfunction Risk of Bleeding : gastric ulcers > duodenal ulcers RR of NSAIDS is 4-7 compared to ASA (2.5) and COX 2 inhibitors (1.5). Relative risk varies with individual NSAIDS ex : piroxicam > ibuprofen etc Risk of bleeding is dose dependant Multiple cofactors contribute to risk ( eg. age > 75 yrs, h/o CAD, prior GIB, H. pylori, steroids, bisphosphonates & ETOH etc )
16 Resumption of Low Dose ASA ( 81 mg ) After Bleeding Ulcer Sung et al. Gastro 2006;130 (suppl 2): A 44 8 week DB RCT after Endoscopic Therapy. i.v PPI X 3 days followed by oral PPI Rx. Rebleeding at 1 month; 11% of pts on placebo (N=55) rebled c/to 18% of pts on ASA (N=58). - P = 0.25 Mortality at 2 months: There was a 14% mortality in placebo group (n=55) c/to 2% in pts on ASA (N=58). - P =
17 Guidelines for Medical Tx for Non Variceal UGIB Somatostatin /Octreotide reduce portal venous blood flow and gastroduodenal arterial flow, while preserving renal blood flow. These are not routinely recommended for patients with acute ulcer bleeding. ( Class A rec), Dose mcg bolus f/by 25 mcg/hr x 3 days. In Meta-analyses of 14 studies, 1829 pts with Non variceal UGIB PPI reduced risk of continued bleeding and need for surgery. ( Khuroo et al -NEJM 1997;336: ) PPIs were better for bleeding from PUD than non PUD bleeding; eg.- hemorrhagic gastritis. I.V Erythromycin 250 mg i.v bolus or 3 mg/kg over 30 min, administered minutes before EGD significantly increases quality of mucosal visibility. ( Class A rec) PPI ( Pantoprazole ) 80 mg i.v bolus followed by an infusion of 8 mg/hr x 72 hrs. ( Class A rec)


18
19 Rebleeding after Endoscopic Therapy ~ 20% of pts with active UGIB rebled. A second-look endoscopy demonstrated benefit in only those cases with active re-bleeding patients with bleeding peptic ulcers Initial therapy 98.6% successful Rebleeding 8.2% Predictors of rebleeding: OR Hypotension 2.2 Anemia <10 gm/dl 1.9 Active bleeding / fresh blood 1.7 / cm ulcer 1.8 Wong et al Gut 2002
20 Early (2-24 hrs) vs. Delayed Endoscopy for UGIB Lower costs: - Early discharge of low risk patients. - Location of admission (ICU vs. ward) Significant benefit of endoscopic therapy in high risk pts suggests early endoscopy is beneficial, but has not been documented in RCTs. Major clinical outcome parameters such as rebleeding rate, mortality and the need for an emergency operation have no bearing with timing of endoscopy. There is insufficient evidence to support endoscopy within 12 hours of presentation leading to better clinical outcome. J Sung, AGA Perspectives Vol 5, Dec 2009
21 Indications for Angiography in UGIB Consensus statement from American College of Radiology: - Endoscopy is the best dx and therapeutic procedure. - Surgery and transcatheter arteriography /intervention (TAI) are equally effective following failed EGD. TAI is considered in cases with high operative risk. - TAI is less successful in pts with impaired coagulation - TAI is best technique for UGIB into the biliary tree or pancreatic duct.
22 Angiographic Therapy Bleeding should be > 0.5 ml/hr. Selective Intra-arterial vasopression not used now. Risks: Brady-arrhythmias, ischemia etc Selective occlusion of bleeding arteries with gelfoam, beads, tissues adhesives and coils etc are used. Rebleeding is common, and complications such as ischemia, infarction, perforation and abscess etc are prominent. CTA, MRA, CTe

23 Technetium Tagged RBC Scan
24 Surgical Therapy for UGIB- When? Role is controversial. Is usually considered in high risk cases when ; 1) HD instability even after > 3 units PRBC transfusions 2) TWO unsuccessful EGDs/attempts at hemostasis 3) Shock with recurrent hemorrhage 4) Continuous bleeding with transfusion requirements of > 3 units PRBC / day.
25 Surgical Therapy Typically pts are severely ill and mortality is ~ 25 % c/to ~ 10% in un-operated pts. Primary objective is not to cure ulcer disease but stop hemorrhage. Acid-reducing procedures may be added. A large RCT trial of 92 pts demonstrated that after initial failure of Endo Tx an endoscopic re-treatment reduced the need for surgery without increasing death and had fewer complications than surgery. At this time, no data from current endoscopic era supports early surgery except - A-E fistula, bleeding benign tumors and severe GAVE
26 Acute Lower GI Bleeding
27 LGIB Epidemiology Bleeding distal to ligament of Treitz Self-limited in over 80% More commonly from colon than SB (<15%) Annual incidence 20/ (1/5 of UGI bleeding) Mean age over 65 years Incidence increases with age Mortality 1-5% (23% if bleeding after hospitalization)
28 Outcomes Acute rebleeding 7-32 Delayed rebleeding Surgery 4-24 Mortality 1-5 PRBC (mean #units) Length of stay 4-11 *(%) Strate LL. Gastro Clin N Am 2005;34:
29 Predictors of Mortality Age > 60 Concurrent active major organ disease Renal, cardiopulmonary, hepatic, neurological Preexisting hospitalization Passing frequent frank blood Orthostatic hypotension Transfusion requirement 4 or more red cell units in the first 24 hours 2 or more units for rebleeding event 6-8 units total
30 LGIB Etiology Colonic sources (243/300) 81% Diverticulosis 29.6 Internal Hemorrhoids 14.0 Ischemic colitis 12.3 Rectal ulcers 9.1 UC, Crohn s, other colitis 8.2 Post-polypectomy ulcer 7.4 Colon polyp or cancer 6.2 Colon angiomas or radiation proctitis 5.7 Other LGI diagnoses 7.5 UGI source 15.3% SB source 1.3% No identified source 2.4% CURE hemostasis research group
31 Evaluation of LGIB Medical history Nature and duration of bleeding episode Symptoms: pain, fever, dyspepsia Relevant history: bleeding, trauma, GI surgery, comorbidity, risk factors for liver disease Medications: NSAIDs, ASA, anti-coagulants Physical examination Vital signs, orthostatics Cardiopulmonary exam Abdominal and rectal exam (repeat even if reported by ED)
32 Evaluation Laboratory Complete blood count and electrolytes PT/PTT Type blood / screen/cross-match EKG for patients > 50 yrs or risk factors for heart disease Abdominal radiographs not indicated Barium studies contraindicated Appropriate IV access Fluid and/or blood product resuscitation PRBC to HCT >30 FFP to INR <1.2 Platelets to > 50k Continuous cardiac monitoring for those with coronary risk factors Monitored bed/ frequent VS
33 Management Pass NGT to exclude UGIB 10-20% with hematochezia have UGI source of bleeding Consider EGD if NGT inconclusive (particularly w/ hemodynamic compromise, risk factors for UGI source) Helps to prep colon (Golytely) Early colonoscopy (within 12-24hr) After Golytely prep Identifies lesion in over 75% cases Therapy possible Associated with reduced length of stay Low complications 0.5-1% 10-20% undergoing urgent colonoscopy receive endoscopic therapy
34 ASGE 2001
35 Vascular Ectasia Multiple, mainly right colon Associated with advanced age, CRF, Valvular heart disease Intermittent hematochezia, massive bleeding rare Argon Plasma Coagulation effective, widely used All lesions should be treated
36 Cecal AVM
37 Radiation Proctopathy Intermittent hematochezia with tenesmus 9m to 4 yrs after XRT for prostate or gyn cancers Multiple telangiectasias on endoscopy APC most effective All visible lesions treated and repeated Q 4 weeks, full bowel prep advised, mean 2.9 sessions (1-8) Post procedure rectal pain and cramps possible Post procedure rectal ulcers Rx with 5 ASA suppositories

38 Radiation Proctitis
39 Internal Hemorrhoids Most common cause of LGI bleeding in ambulatory adults Second most common cause of severe LGIB High fiber diet, avoiding straining and sitz baths usually effective Emergency hemostasis and refractory cases treated with rubber band ligation and rarely surgery
40 Internal Hemorrhoids

41 External Hemorrhoids
42 Ischemic Colitis Results from sudden and often temporary reduction in mesenteric blood flow Sudden lower abdominal pain followed w/in 24 hrs by bloody diarrhea Segmental involvement of water shed areassplenic flexure and descending colon Endoscopy mainly diagnostic - mucosal erythema, friability, necrotic ulcerations Supportive management

43 Ischemic Colitis
44 Small Bowel Bleeding
45 Small Bowel Bleeding 5-7 % of obscure GI bleeding Proximal jejunum angioectasia Similar to right colon AVMs Capsule endoscopy Balloon assisted enteroscopy Double balloon endoscopy Single balloon enteroscopy Intraoperative enteroscopy


46 Capsule Endoscopy Bleeding consensus 2005 Should be part of initial evaluation of obscure bleeding Earlier use may be positive for QOL and alter management Lead to treatment success 86.9% when actively bleeding State of the art in small bowel imaging
 Advantages Steer/wash/therapeutic ½ to 2/3 of bowel seen avg.")

47 Double Balloon Enteroscopy Indications OGIB after Neg capsule Surveillance of FAP or Peutz Jaegers PEJ Roux-en Y endoscopy(ercp) Advantages Steer/wash/therapeutic ½ to 2/3 of bowel seen avg. Target lesion on CE or CTe helps determine route Learning curve Time/flouro/depth 1 st 10 cases 109 mins to ~90 after Retrograde 31% failure Outcomes Yield as high as capsule Mehdizadeh et al, GIE 2006 Courtesy of Fujinon Corp.
48 Conclusions: Medical stabilization Signs and symptoms help to localize Direct the investigation Alter risk factors Value = Benefits/Costs

49 Thank You
Nothing to disclose. Annually ~ 300,000 hospitalizations and ~ 20,000 deaths in US*
 Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding
 ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding
 ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
True obscure causes hemobilia, hemosuccus pancreaticus, vasculitis
 Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
The Usefulness of Capsule Endoscopy
 The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
But.. Capsule Endoscopy. Guidelines (OMED ECCO) Why is Enteroscopy so Important? 4/19/2017
 Why is Enteroscopy so Important? 4/19/2017") Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
Endoscopic Doppler in the Management of Upper and Lower GI Bleeding: Case Studies & Atlas
 Endoscopic Doppler in the Management of Upper and Lower GI Bleeding: Case Studies & Atlas Presented By: Dennis M. Jensen, MD Professor of Medicine David Geffen School of Medicine at UCLA Associate Director,
Endoscopic Doppler in the Management of Upper and Lower GI Bleeding: Case Studies & Atlas Presented By: Dennis M. Jensen, MD Professor of Medicine David Geffen School of Medicine at UCLA Associate Director,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Occult and Overt GI Bleeding: Small Bowel Imaging. Outline of Talk
 Occult and Overt GI Bleeding: Small Bowel Imaging Lauren B. Gerson MD, MSc Director of Clinical Research, GI Fellowship Program California Pacific Medical Center San Francisco, CA Outline of Talk Definition
Occult and Overt GI Bleeding: Small Bowel Imaging Lauren B. Gerson MD, MSc Director of Clinical Research, GI Fellowship Program California Pacific Medical Center San Francisco, CA Outline of Talk Definition
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Helicobacter pylori. Objectives. Upper Gastrointestinal Bleeding Peptic Ulcer Disease
 Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING
 Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Role of radiology in colo-rectal bleedings. Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE
 Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
Capsule Endoscopy and Deep Enteroscopy
 Capsule Endoscopy and Deep Enteroscopy Are they complementary? ACG Governors / ASGE 2012 Best Practices Course January 29, 2012 The Hyatt Regency Huntington Beach, California John A. Martin, MD Disclosure
Capsule Endoscopy and Deep Enteroscopy Are they complementary? ACG Governors / ASGE 2012 Best Practices Course January 29, 2012 The Hyatt Regency Huntington Beach, California John A. Martin, MD Disclosure
Update on Gastrointestinal Bleeding COPYRIGHT. Update in Internal Medicine 5 th December, 2016
 Update on Gastrointestinal Bleeding Update in Internal Medicine 5 th December, 2016 Simon C. Robson. MD, PhD, FRCP (UK). Charlotte F. and Irving W. Rabb Professor of Medicine Liver and Gastroenterology,
Update on Gastrointestinal Bleeding Update in Internal Medicine 5 th December, 2016 Simon C. Robson. MD, PhD, FRCP (UK). Charlotte F. and Irving W. Rabb Professor of Medicine Liver and Gastroenterology,
Occult small bowel bleeding - Video capsule first
 Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
10/1/2018. Case. History. Initial Assessment. Vital Signs. Factors predictive of UGI source. Gastrointestinal Hemorrhage
 Case 79 yo M transferred from OSH with blood per rectum Gastrointestinal Hemorrhage Piroska Kopar MD Assistant Professor of Surgery Section of Acute and Critical Care Surgery 4u prbc 2u FFP Mentating,
Case 79 yo M transferred from OSH with blood per rectum Gastrointestinal Hemorrhage Piroska Kopar MD Assistant Professor of Surgery Section of Acute and Critical Care Surgery 4u prbc 2u FFP Mentating,
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding
 PRACTICE GUIDELINES nature publishing group 459 CME ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG1 and Ian M. Gralnek, MD, MSHS2
PRACTICE GUIDELINES nature publishing group 459 CME ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG1 and Ian M. Gralnek, MD, MSHS2
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
CT Angiography g of Lower Intestinal Bleeding
 CT Angiography g of Lower Intestinal Bleeding Jorge A. Soto, MD General concepts: Learning Objectives Clinical Importance Presentation, Location Etiologies CT Ttchniques: CT Angiography CT Enterography
CT Angiography g of Lower Intestinal Bleeding Jorge A. Soto, MD General concepts: Learning Objectives Clinical Importance Presentation, Location Etiologies CT Ttchniques: CT Angiography CT Enterography
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Gastroenterology. 3. Which of the following clotting factors is dependent on Vitamin K? a) II b) VII c) IX d) X e) All of the above
 II b) VII c) IX d) X e) All of the above") Gastroenterology 1. Which one of the following is not a symptom of Vitamin A deficiency? a) Keratomalacia b) Poor wound healing c) Osteomalacia d) Night blindness 2. Which one of the following is not a
Gastroenterology 1. Which one of the following is not a symptom of Vitamin A deficiency? a) Keratomalacia b) Poor wound healing c) Osteomalacia d) Night blindness 2. Which one of the following is not a
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
GI Emergencies and the On-Call Call
 GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
GI Emergencies and the On-Call Call Julie Yang, MD, FASGE Director of Therapeutic Endoscopy Assistant Professor of Medicine Montefiore Medical Center Albert Einstein College of Medicine Objectives Scenarios
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
ACUTE UPPER GASTROINTESTINAL HEMORRHAGE: PHARMACOLOGIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Management of acute upper gastrointestinal bleeding
 1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding
 in high risk peptic ulcer bleeding") ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
ISSN: 2347-3215 Volume 2 Number 7 (July-2014) pp. 203-208 www.ijcrar.com Efficacy of dual therapy (APC & Adrenaline) in high risk peptic ulcer bleeding Saleh Azad Bakht*, Manouchehr Khoshbaten, Kamal Bostani,
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Gustavo Mariño, MD VA Medical Center Washington, DC
 Gustavo Mariño, MD VA Medical Center Washington, DC True emergency? Likelihood that an intervention is required to improve outcomes Optimal timing Other factors: VIPs?, demanding patient?, convenience?,
Gustavo Mariño, MD VA Medical Center Washington, DC True emergency? Likelihood that an intervention is required to improve outcomes Optimal timing Other factors: VIPs?, demanding patient?, convenience?,
Peri-Endoscopic Period. Neena S. Abraham MD, MSCE, FACG
 How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N
 Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Gastroenterology Fellowship Program
 Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Antiplatelets in cardiac patients with suspected GI bleeding
 Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants
 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
Upper and Lower GI Bleeding
 Upper and Lower GI Bleeding John Poneros MD, FASGE, NYSGEF Associate Professor Columbia University College of Physicians and Surgeons Acting Director, Endoscopy Unit New York Presbyterian/Columbia UGIB
Upper and Lower GI Bleeding John Poneros MD, FASGE, NYSGEF Associate Professor Columbia University College of Physicians and Surgeons Acting Director, Endoscopy Unit New York Presbyterian/Columbia UGIB
Antithrombotics and the Gut
 Antithrombotics and the Gut Panelists: AR Tagahvi MD, N Nozari MD Moderator: S Nasseri-Moghaddam MD, MPH IAGH monthly meeting Shahrivar 1395 (September 2016 ) IAGH Conference Hall Antithrombotic agents
Antithrombotics and the Gut Panelists: AR Tagahvi MD, N Nozari MD Moderator: S Nasseri-Moghaddam MD, MPH IAGH monthly meeting Shahrivar 1395 (September 2016 ) IAGH Conference Hall Antithrombotic agents
CHAPTER 30 Gastrointestinal Bleeding
 CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Upper Gastrointestinal Bleeding. December 4, 2018 & December 11, 2018 Sonia Lin
 Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
UPPER AND LOWER GASTROINTESTINAL BLEEDING. Prof. G. Zuliani
 UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
Colon ischemia. ACG Clinical Guideline; Am J Gastroenterol 2015
 Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
Colon ischemia ACG Clinical Guideline; Am J Gastroenterol 2015 Manifestations Acute, reversible Irreversible : gangrene, fulminant colitis/stricture formation, chronic ischemic colitis Recurrent sepsis
Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit
 Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit Authors Shahrad Hakimian 1, Salmaan Jawaid 2, Yurima Guilarte-Walker 3, Jomol Mathew
Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit Authors Shahrad Hakimian 1, Salmaan Jawaid 2, Yurima Guilarte-Walker 3, Jomol Mathew
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
The Usefulness of Capsule Endoscopy
 The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Associate Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut INDICATIONS FOR USE PillCam
The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Associate Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut INDICATIONS FOR USE PillCam
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010
 Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010 Background Angiodysplasia is an important cause of occult and acute
Epidemiology and Treatment of Colonic Angiodysplasia; a Population-Based Study. Naomi G. Diggs, MD Lisa L. Strate, MD MPH March 2, 2010 Background Angiodysplasia is an important cause of occult and acute
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often