Fluids and Lactate. A/Prof Peter Morley
|
|
|
- Nickolas Richards
- 5 years ago
- Views:
Transcription
1 Fluids and Lactate A/Prof Peter Morley

2
3

4 RCTs Other evidence
5 5
6 6
7 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
8 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
9 Fluids and fluids balance
10 Most of the body is water infants (75% of total body weight) young males (60%) young females (54%) elderly males (50%) elderly females (45%)
11 Where is the water? 2/3 in intracellular fluid (40% of body weight) 1/3 in extracellular fluid (20% of body weight) 1/4 of ECF is intravascular in plasma (5% of bw) Blood volume (including RBCs) approx 7-8% bw
12 Fluid requirements obligatory fluid requirement metabolism obligatory losses urine evaporation
13 Fluid requirements (2) amount required correlates with metabolic rate ml/100kcal (approx. 1ml/kcal) Children 0-10 kg ml/kg/day 10-20kg ml/kg[in excess of 10]/day >20kg ml/kg[in excess of 20]/day Adults ml/kg/day
14 Water balance per day input (2500 ml) oral fluids (1400 ml) food (700 ml) metabolic oxidation (400 ml) output (2500 ml) urine (1500 ml) lung (500 ml) skin (400 ml) faeces (100 ml)
15 Fluid requirements (3) additional fluid requirement inceased losses gastrointestinal urinary tissues/third space specific deficiencies carrier fluid for medications resuscitation
16 Indications for IV therapy and types of solutions used
17 Which route for fluid (and medication) administration gastrointestinal tract best route cheaper more physiological avoids risks of intravenous access
18 Risks of intravenous access infection site time in situ trauma site unwanted material air non-iv sustances restrictions mobility nursing time
19 When is the gastrointestinal tract inappropriate not allowed to/don t want to (nil orally) no point functional ileus mechanical obstruction anatomical resected diseased nutrients broken down red blood cells insulin etc. too slow resuscitation
20 N Engl J Med 2015;372:

21 N Engl J Med 2015;372:
22 Types of fluid crystalloid Colloid (including blood products)
23 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
24 Crystalloid normal saline (0.9%) Hartmanns (5% glucose)
25 What is in crystalloids? Normal Hartmanns 5% saline glucose Na K Ca Cl HCO * 0 Glucose mosm ph (components as mmol/l) *as lactate (d- & l-)
26 Crystalloid pharmacokinetics provides water and electrolytes intravascular half life 8 minutes Water/5% glucose distributes to TBW equilibrium 80mL/L NS/Hartmanns distributes to extracellular fluid volume at equilibrium mL/L intravascular
27 200 ml/hr N Saline means over 30 min: 100 mls given and mls added to intravascular volume (<1%)
28 200 ml/hr N Saline means over 5 hours: 1000 mls given and mls added to intravascular volume (10%)
29 Traditional indications for crystalloids simple replacement of losses losses crystalloid-like volume replacement not urgent
30 Problems with crystalloids? fluid overload inadequate resuscitation dilution oedema specific to fluid hyperglycaemia hyperchloraemia hyponatraemia
31 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
32 Nsaline vs Hartmanns

33
34
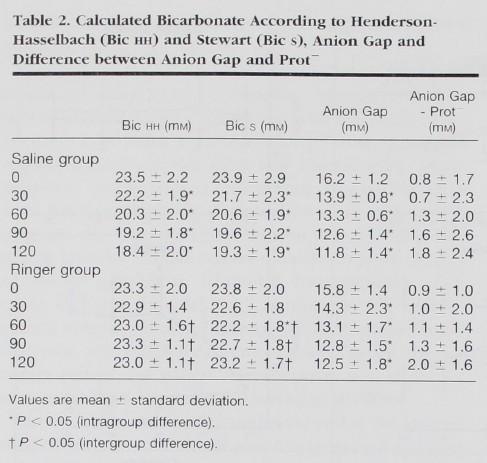
 was restricted to attending specialist approval only during the intervention period; patients instead received a lactated solution")
35 During the control period, patients received standard intravenous fluids. After a 6-month phase-out period (August 18, 2008, to February 17, 2009), any use of chloride-rich intravenous fluids (0.9% saline, 4% succinylated gelatin solution, or 4% albumin solution) was restricted to attending specialist approval only during the intervention period; patients instead received a lactated solution (Hartmann solution), a balanced solution (Plasma-Lyte 148), and chloride-poor 20% albumin. The implementation of a chloride-restrictive strategy in a tertiary ICU was associated with a significant decrease in the incidence of AKI and use of RRT.
36

37 Among critically ill adults with sepsis, resuscitation with balanced fluids was associated with a lower risk of in-hospital mortality. If confirmed in randomized trials, this finding could have significant public health implications, as crystalloid resuscitation is nearly universal in sepsis. (Crit Care Med 2014; 42: )
38
39
40
41
42 Other crystalloids? hypertonic saline hypotonic saline combinations (e.g. 4% and 1/5, plasmalyte)
43
44
45 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
46 Colloid Gelofusin Dextrans Hydroxyethyl starches Albumin
47 What is in colloids? Geofusin 4% solution of succinylated gelatin Mol. Weight 30,000 Na 154 Cl 120, ph Dextran polysaccharides fractionated into different molecular sizes 70 (M.W. 70,000), 40 (M.W. 40,000) Hydroxyethyl starches (HES) are produced by hydroxyethyl substitution of amylopectin, a D-glucose polymer, obtained from sorghum or maize
48 Albumin? Human albumin is a naturally occurring monodisperse colloid. Solutions (4% and 20%) are prepared from human plasma and heat treated to ensure that neither hepatitis nor HIV can be transmitted 4%: treatment of hypovolaemia 20% human albumin is used for the treatment of hypoalbuminaemia in the presence of salt and water overload (e.g. hepatic failure with ascites).
49 Colloid pharmacokinetics provides water and electrolytes plus additional components intravascular half life hours distributes mainly to intravascular space hypertonic solutions attract more fluid
50 OH S INTENSIVE CARE MANUAL
51 Traditional teaching about indications for colloids? volume replacement is urgent (?) specific blood products are not necessary anti-thrombotic properties desired (?) Keen to induce acute kidney injury
52 Problems with colloids? fluid overload inadequate resuscitation dilution allergy (oedema) renal impairment specific to fluid Hydroxyethyl starches and renal impairmet Dextrans and bleeding blood products (disease transmission, incompatible)
53 Blood products red blood cells plasma normal serum albumin specific components clotting factors immunoglobulins
 or when the level was 9 g per deciliter or less (higher threshold) during the")
54 In this multicenter, parallel-group trial, we randomly assigned patients in the intensive care unit (ICU) who had septic shock and a hemoglobin concentration of 9 g per deciliter or less to receive 1 unit of leukoreduced red cells when the hemoglobin level was 7 g per deciliter or less (lower threshold) or when the level was 9 g per deciliter or less (higher threshold) during the ICU stay.
55 N Engl J Med 2014;371:
56 N Engl J Med 2014;371:
57

58 A large trial of transfusion strategies in older mechanically ventilated patients is feasible. This pilot trial found a nonsignificant trend toward lower mortality with restrictive transfusion practice. (Crit Care Med 2013; 41: )
59 multicenter, parallel-group trial, patients older than 16 years, undergoing nonemergency cardiac surgery, 17 centers in the United Kingdom. Patients with a postoperative hemoglobin level of less than 9 g per deciliter were randomly assigned to a restrictive transfusion threshold (hemoglobin level <7.5 g per deciliter) or a liberal transfusion threshold (hemoglobin level <9 g per deciliter).
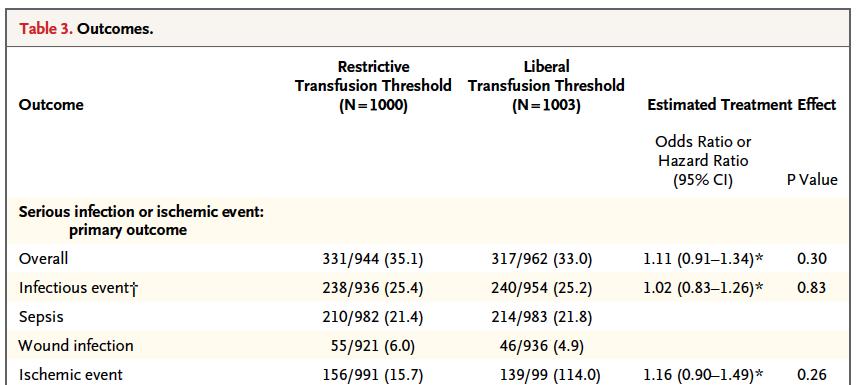

60 NNH = 60
61

62
63
64

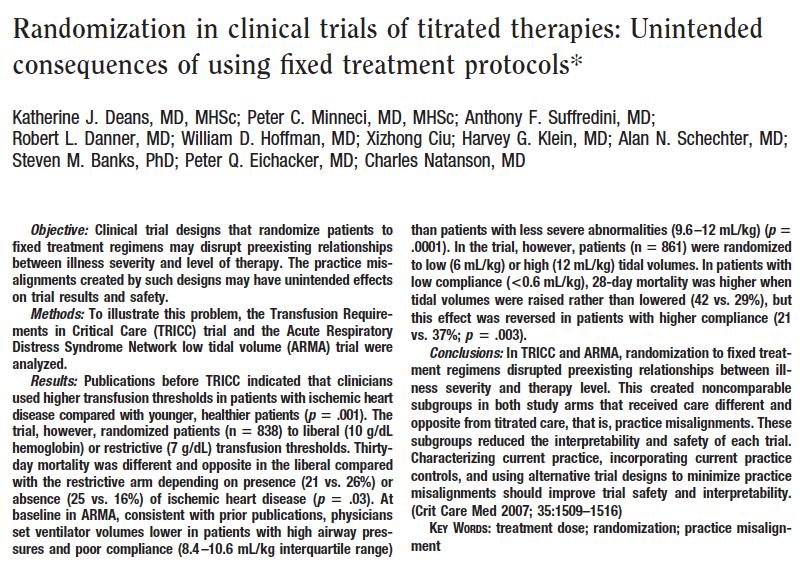
65 Unintended consequences of fixed treatment protocols
66 Unintended consequences of fixed treatment protocols

67 67

68 N Engl J Med 2015;372: Transfusion of fresh red cells, as compared with standard-issue red cells, did not decrease the 90-day mortality among critically ill adults.
69
70 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
71

72
73 Summary Our systematic review of randomised controlled trials showed that, for each of these patient categories, the risk of death in the albumin treated group was higher than in the comparison group The pooled relative risk of death with albumin was 1.68 (95% confidence interval 1.26 to 2.23) and the pooled difference in the risk of death was 6% (3% to 9%) or six additional deaths for every 100 patients treated We consider that use of human albumin solution in critically ill patients should be urgently reviewed

74 74
75
76 76
77 N Engl J Med 2004;350: In (>7000) patients in the ICU, use of either 4 percent albumin or normal saline for fluid resuscitation results in similar outcomes at 28 days. The ratios of the volume of albumin to the volume of saline administered during the first four days were as follows: 1:1.3 on day 1, 1:1.6 on day 2, 1:1.3 on day 3, and 1:1.2 on day 4.
78 78

79 15L:5L 3:1 OH S INTENSIVE CARE MANUAL
80 80
81 N Engl J Med 2013;369:
82 The structure and function of the endothelial glycocalyx layer, a web of membrane-bound glycoproteins and proteoglycans on endothelial cells, are key determinants of membrane permeability in various vascular organ systems. The integrity, or leakiness, of this layer, and thereby the potential for the development of interstitial edema, varies substantially among organ systems, particularly under inflammatory conditions, such as sepsis, and after surgery or trauma, when resuscitation fluids are commonly used. N Engl J Med 2013;369:
83 In this post hoc study of critically ill patients with traumatic brain injury, fluid resuscitation with albumin was associated with higher mortality rates than was resuscitation with saline.
84



85 The structure and function of the endothelial glycocalyx layer, a web of membrane-bound glycoproteins and proteoglycans on endothelial cells, are key determinants of membrane permeability in various vascular organ systems. The integrity, or leakiness, of this layer, and thereby the potential for the development of interstitial edema, varies substantially among organ systems, particularly under inflammatory conditions, such as sepsis, and after surgery or trauma, when resuscitation fluids are commonly used. N Engl J Med 2013;369:
86 N Engl J Med 2014;370: In patients with severe sepsis, albumin replacement in addition to crystalloids, as compared with crystalloids alone, did not improve the rate of survival at 28 and 90 days.

87 Administration of albumin compared to saline did not impair renal or other organ function and may have decreased the risk of death.
88 There is no evidence from randomised controlled trials that resuscitation with colloids reduces the risk of death, compared to resuscitation with crystalloids, in patients with trauma, burns or following surgery. Furthermore, the use of hydroxyethyl starch might increase mortality. As colloids are not associated with an improvement in survival and are considerably more expensive than crystalloids, it is hard to see how their continued use in clinical practice can be justified.
89 In (7000) patients in the ICU, there was no significant difference in 90-day mortality between patients resuscitated with 6% HES (130/0.4) or saline. However, more patients who received resuscitation with HES were treated with renal-replacement therapy.
90 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
91 200 ml/hr N Saline means over 30 min: 100 mls given and mls added to intravascular volume (<1%)
92 200 ml/hr N Saline means over 5 hours: 1000 mls given and mls added to intravascular volume (10%)
93 Fluid administration Bolus 0 to 30 ml/kg Maintenance ml/hr Time till review response minutes to hours
94 Inadequate response to fluids? tap not on full? plug not in consider pharmacology inotrope infusion dopamine dobutamine adrenaline titrated boluses of vasoconstrictors adrenaline metaraminol
95 What endpoints? blood (perfusion) pressure heart rate (and rhythm) urine output but beware vasoconstrictors decreasing oxygen delivery diuretics (including renal dose dopamine)
96 Peri-operative fluids?
97
98

99 Perioperative intravenous fluid should replace the minor physiological losses (0.5 1 ml/kg/h) and the blood loss. Fluid loss to a third space is negligible. Avoid postoperative weight gain which is a reliable marker of fluid overload. Fluid overload results in alterations in the endothelial glycocalyx resulting in fluid shift toward the interstitium, causing increased postoperative morbidity. Decreased urinary output is physiological during major surgery and not a surrogate parameter for hypovolemia alone or renal dysfunction.
100 Perioperative fluid management of the colorectal surgical patient has evolved significantly over the last five decades. Older notions espousing aggressive hydration have been shown to be associated with increased complications. In the preoperative phase, data suggests that avoidance of preoperative bowel preparation and avoidance of undue preoperative dehydration can improve outcomes. Although the type of intraoperative fluid given does not have a significant effect on outcome, data do suggest that a restrictive fluid regimen results in improved outcomes. Finally, in the postoperative phase of fluid management, a fluid-restrictive regimen, coupled with early enteral feeding also seems to result in improved outcomes.

101 We recommend that both perioperative fluid choice and therapy be individualized. Patients should receive fluid therapy guided by predefined physiologic targets. Specifically, fluids should be administered when patients require augmentation of their perfusion and are also volume responsive.
102 Trauma?
103
104 NEJM 1994; 331:

105 Aggressive volume resuscitation of patients with raaas before proximal aortic control predicted an increased perioperative risk of death, which was independent of systolic blood pressure. Therefore, volume resuscitation should be delayed until surgical control of bleeding is achieved. J Vasc Surg 2013;57:
106
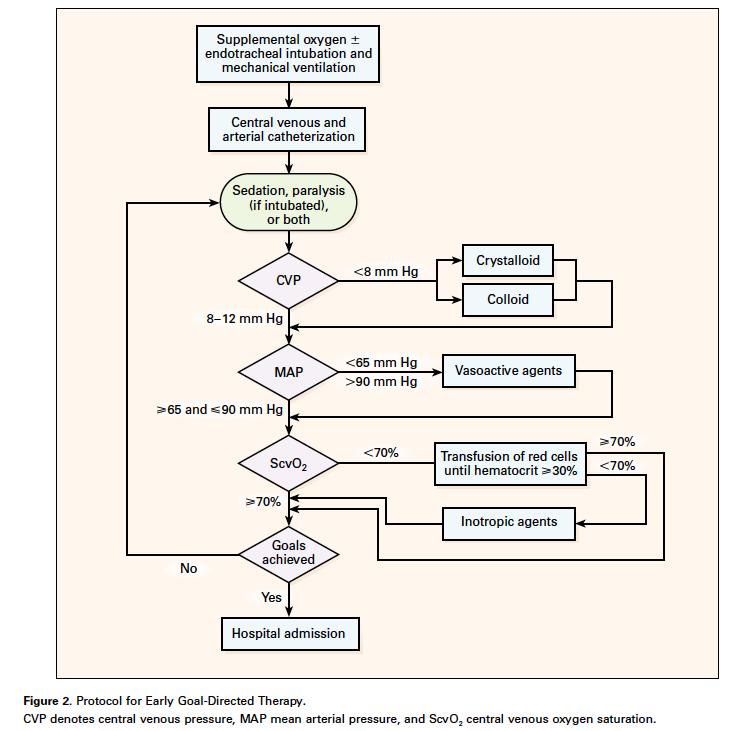
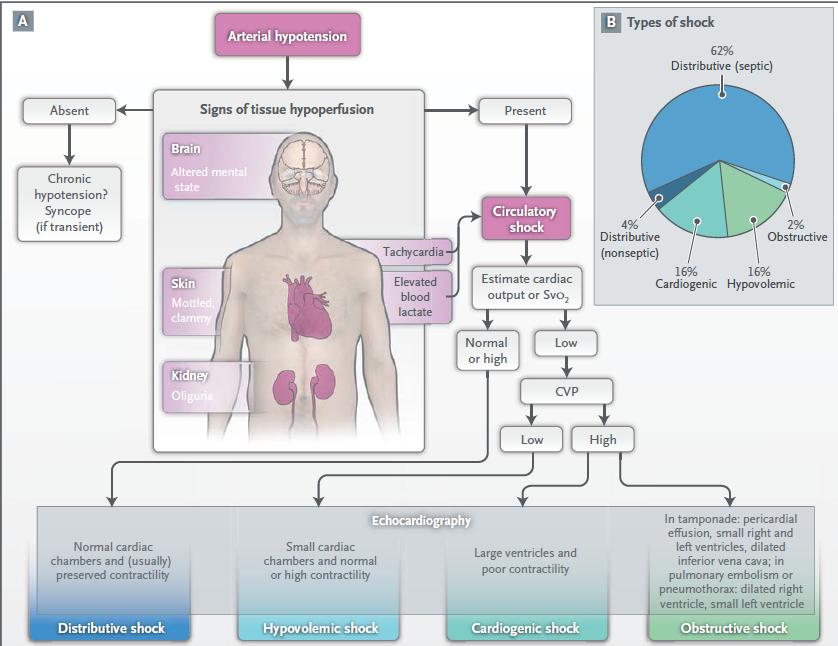
107 What about sepsis? What is Early Goal Directed Therapy
108 N Engl J Med 2001;345:
109
110
111 N Engl J Med 2014;371:
112 N Engl J Med 2015;372:
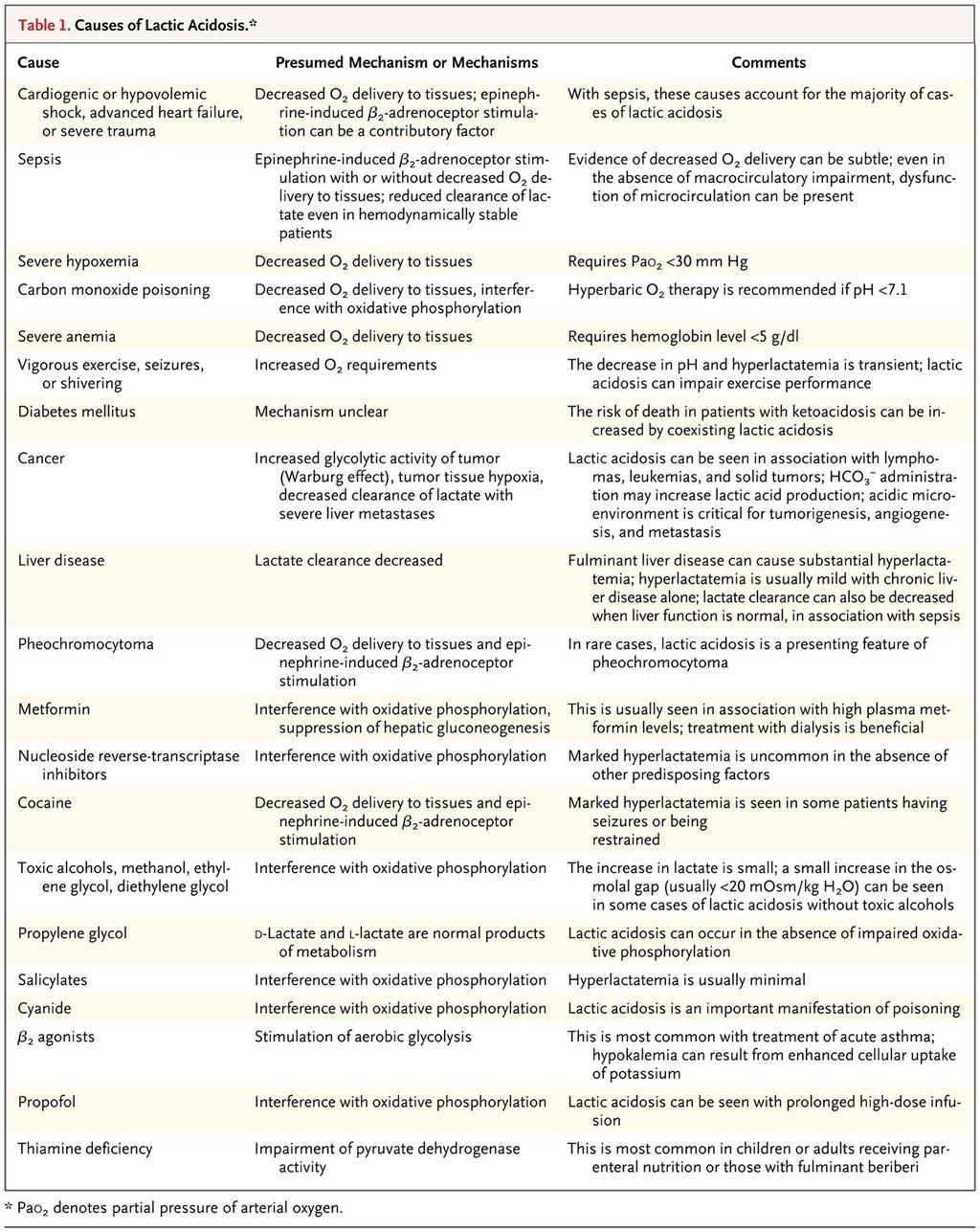
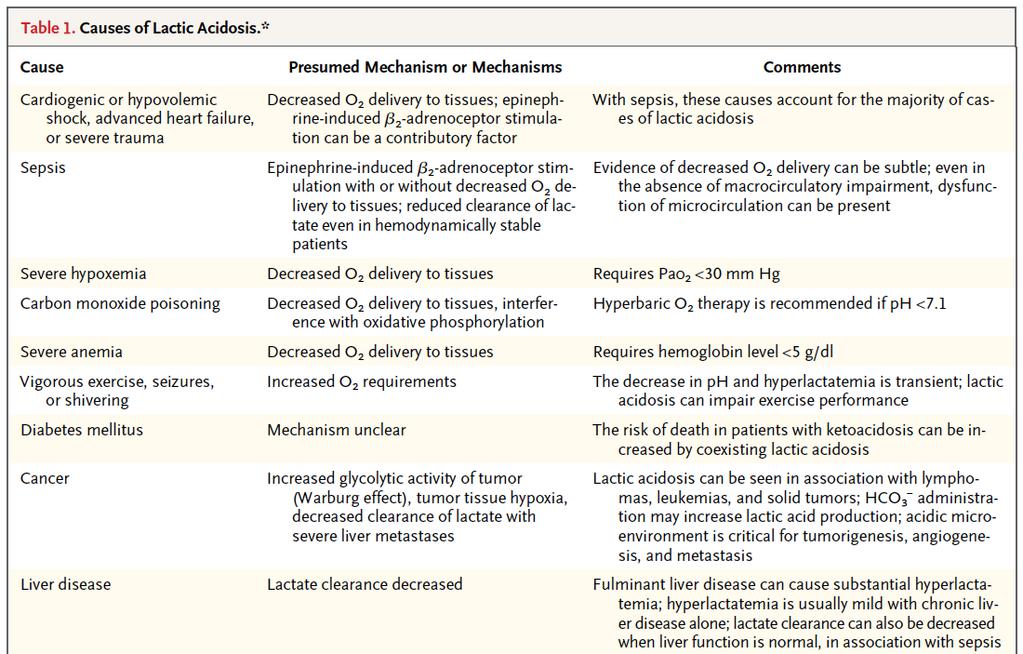
 per kilogram of body weight or no bolus (control group) at the time of admission to a hospital in Uganda, Kenya, or Tanzania (stratum A); children with severe")
113 We randomly assigned children with severe febrile illness and impaired perfusion to receive boluses of 20 to 40 ml of 5% albumin solution (albumin-bolus group) or 0.9% saline solution (saline-bolus group) per kilogram of body weight or no bolus (control group) at the time of admission to a hospital in Uganda, Kenya, or Tanzania (stratum A); children with severe hypotension were randomly assigned to one of the bolus groups only (stratum B). Fluid boluses significantly increased 48-hour mortality in critically ill children with impaired perfusion in these resource-limited settings in Africa.
114

115 Theoretically, colloids, containing suspensions of molecules with a molecular weight that makes them relatively impermeable to an intact capillary membrane, are retained within the intravascular compartment. Most of the evidence for the potential adverse effects of saline comes from observational studies comparing the effects of chloride-rich and chloride restricted solutions, such as buffered or balanced salt solutions, in cohorts of acutely ill patients. Saline is associated with a significant increase in mortality and use of renal replacement therapy in patients in ICU [45] and in those with sepsis [46], as well as a significant increase in major complications in patients undergoing surgery [47].
116
117
118
119
120 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
121 Lactate It s all about the clearance
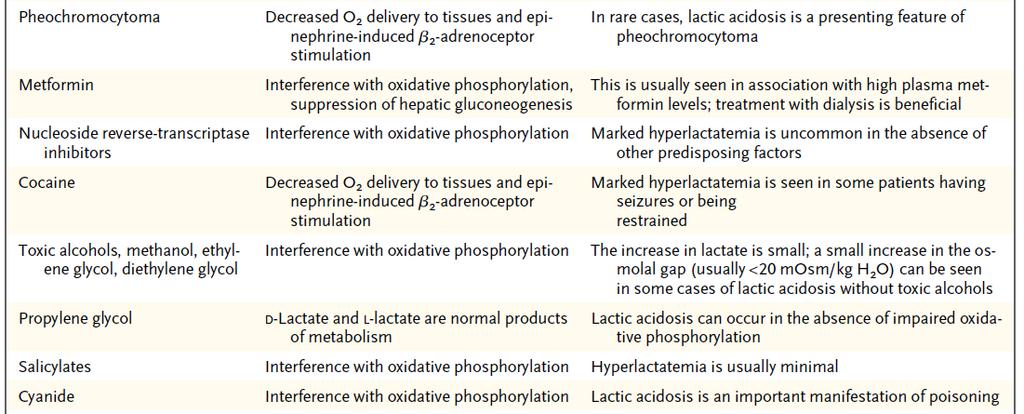
122 Lactic acidosis normal production is 20 mmols/kg/day, 70 kg:1400/day, 60/hr hepatic and renal metabolism Cohen & Woods classification type A = inadequate delivery of oxygen to meet requirements eg. seizures, cardiac arrest, hypoxia type B = no obvious defect in oxygen delivery eg. thiamine deficiency, biguanides, adrenergic
123 N Engl J Med 2014;371:
124
125 N Engl J Med 2014;371:
126 N Engl J Med 2014;371:
127 N Engl J Med 2014;371:
128 N Engl J Med 2014;371:

129 N Engl J Med 2014;371:
130 Normal N Engl J Med 2014;371:
131 Tissue hypoxia N Engl J Med 2014;371:
132 (Stimulated) Aerobic glycolysis
133 Albuterol induced lactic acidosis. Beta-2 effect Dodda, V. R., and Spiro, P. Respir Care 2012;57: (c) 2012 by Daedalus Enterprises, Inc.
134 Aerobic glycolysis = stimulated glycolysis that depends on factors other than tissue hypoxia Activated in response to stress, an effective, albeit inefficient, mechanism for rapid generation of ATP. Epinephrine, β2 -adrenergic agonists, extensive trauma, cardiogenic or hemorrhagic shock, and pheochromocytoma, can cause hyperlactatemia through this mechanism Inflammatory states, can also drive aerobic glycolysis by cytokine-dependent stimulation of cellular glucose uptake Note: Aerobic glycolysis and tissue hypoxia are not mutually exclusive
135
136
137
138 In severe sepsis patients with hemodynamic stability, reflected by optimized baseline CVP and ScvO2, the bundle items of fluid bolus administration, achieving MAP >65 mmhg, and lactate clearance were independent predictors of outcome.

139 The addition of BD and lactate to triage vital signs increases the ability to distinguish major from minor injury.
 with survival to hospital discharge after resuscitation from CA and TH")
140 Lower serum lactate levels at 12 h and 24 h, but not initially following cardiac arrest, are associated (on multivariate analysis) with survival to hospital discharge after resuscitation from CA and TH treatment.
141

142 Electrolytes: Lactate A guide to diagnostic Clinical Biochemistry Walmsley & White 1988
143 Electrolytes: Lactate 28 year old male admitted in status epilepticus second sample 3 hours after last convulsion A guide to diagnostic Clinical Biochemistry Walmsley & White 1988
144

145
146 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid
147 Lactate It s all about the clearance
148 148
149
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
Fluid Resuscitation in Sepsis. A Literature Review
 Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
Fluid Therapy and Outcome: Balance Is Best
 The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
THe Story of salty Sam
 THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Getting smart with fluids in the critically ill. NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia
 Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Proceeding of the LAVECCS
 Close this window to return to IVIS Proceeding of the LAVECCS Congreso Latinoamericano de Emergencia y Cuidados Intensivos Ju1. 28-30, 2011 Santiago de Chile, Chile www.laveccs.org Reprinted in IVIS with
Close this window to return to IVIS Proceeding of the LAVECCS Congreso Latinoamericano de Emergencia y Cuidados Intensivos Ju1. 28-30, 2011 Santiago de Chile, Chile www.laveccs.org Reprinted in IVIS with
Principles of Fluid Balance
 Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Septic AKI in ICU patients
 Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Septic AKI in ICU patients Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany achim.joerres@charite.de Agenda Epidemiology
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC Sept
 Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Fluid balance in the critically ill child with dengue Too much too little? Professor Lucy Lum Universiti Malaya ASMIC 2018 21-23 Sept CFR 0.22 in 2017 0.15 in 2018 2 Lecture Contents: Dynamic disease Self-limiting
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Les solutés de remplissage. Philippe Van der Linden MD, PhD
 Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Hell or High Lactate. Charles Bruen, MD. resusreview.com/regionsmar17
 Hell or High Lactate Charles Bruen, MD resusreview.com/regionsmar17 No Disclosures No Off-label Use 3 Positive troponin? Inpatient or Observation? Lactate elevated? Goals What causes lactate production?
Hell or High Lactate Charles Bruen, MD resusreview.com/regionsmar17 No Disclosures No Off-label Use 3 Positive troponin? Inpatient or Observation? Lactate elevated? Goals What causes lactate production?
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
PERANAN LAKTAT PADA PASIEN KRITIS DI ICU. Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO
 PERANAN LAKTAT PADA PASIEN KRITIS DI ICU Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO History of Lactate Karl Scheele, 1780 found in sour milk Joseph Scherer the German physician-chemist after 70 years demonstrate
PERANAN LAKTAT PADA PASIEN KRITIS DI ICU Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO History of Lactate Karl Scheele, 1780 found in sour milk Joseph Scherer the German physician-chemist after 70 years demonstrate
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Salt of the earth or a drop in the ocean An overview of the properties of iv fluids
 Bapen Conference 2009 13 th October 2009 Cardiff International Arena Salt of the earth or a drop in the ocean An overview of the properties of iv fluids Peter Gosling BSc MSc PhD FRCPath Consultant Clinical
Bapen Conference 2009 13 th October 2009 Cardiff International Arena Salt of the earth or a drop in the ocean An overview of the properties of iv fluids Peter Gosling BSc MSc PhD FRCPath Consultant Clinical
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Fluid Balance in an Enhanced Recovery Pathway. Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017
 Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
Fluid Balance in an Enhanced Recovery Pathway Edwin Itenberg, DO, FACS, FASCRS St. Joseph Mercy Oakland MSQC/ASPIRE Meeting April 28, 2017 No Disclosures 2 Introduction The optimal intravenous fluid regimen
SIMPLY. Fluids. Dr Will Dooley
 SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
SIMPLY. Fluids Dr Will Dooley Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed? Assessment
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
FLUID RESUSCITATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Failure of the circulation to maintain Tissue cellular. Tissue hypoperfusion Cellular hypoxia SHOCK. Perfusion
 Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Bicarbonate in the NICU
 OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
Neonatal Fluid Therapy Not my mother s physiology!!
 Neonatal Fluid Therapy Not my mother s physiology!! Physiologic Approach to Neonatal Fluid Therapy General principles of fluid balance Fetal physiology of fluid balance Neonatal physiology of fluid balance
Neonatal Fluid Therapy Not my mother s physiology!! Physiologic Approach to Neonatal Fluid Therapy General principles of fluid balance Fetal physiology of fluid balance Neonatal physiology of fluid balance