The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
|
|
|
- Doreen Neal
- 5 years ago
- Views:
Transcription
1 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
2 Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing and managing blue baby
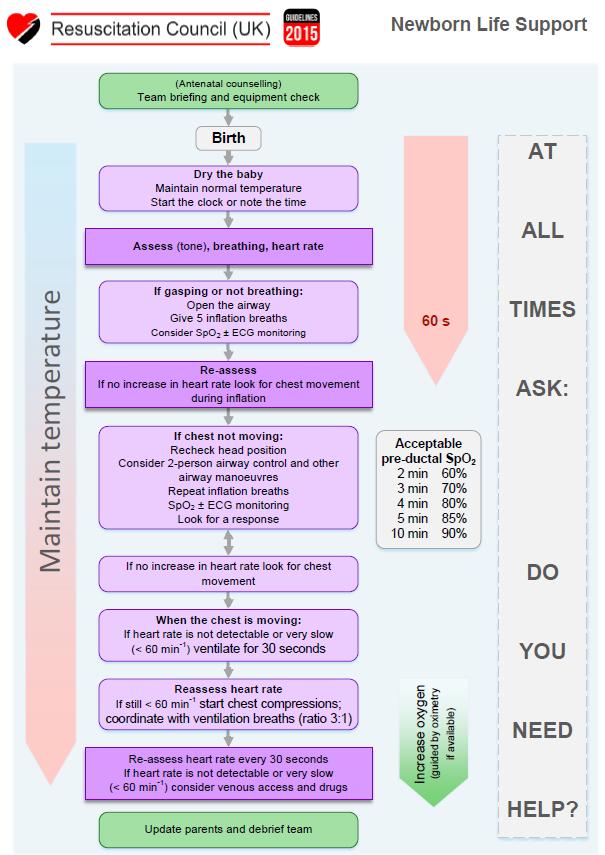

3
4 Cyanosis Cyanosis is visible when there is an excess of deoxygenated haemoglobin in the blood It may be less visible if the infant is anaemic Central - mucous membranes inside mouth Peripheral extremities Result of inadequate functioning of either the heart or lungs Primary pathology Secondary to other problems such as sepsis
5 Early Effective Intervention Recognising the sick infant and need for intervention Timely and effective stabilisation and referral for definitive care Slowing the progression of any illness Avoiding iatrogenic harm
6 Delay in intervention may lead to further clinical compromise and increased morbidity or mortality Death
 Pneumonia Meconium Aspiration Syndrome Persistent Pulmonary Hypertension of the Newborn Pneumothorax Conge")
7 CNS diseases Intra / periventricular haemorrhage Meningitis Seizures causing hypoventilation Other: Polycythaemia Sepsis Shock Methaemoglobinaemia Respiratory: Respiratory distress syndrome (rare in term babies) Pneumonia Meconium Aspiration Syndrome Persistent Pulmonary Hypertension of the Newborn Pneumothorax Congenital Anomalies (e.g. Congenital diaphragmatic hernia or cystic adenomatous malformation) Potential causes of cyanosis Cardiac: Cyanotic heart disease Transposition of the great arteries Total anomalous pulmonary venous drainage Tricuspid atresia Tetralogy of fallot Truncus arteriosus Critical pulmonary stenosis Critical obstruction to the systemic circulation will cause pallor / greyness aortic stenosis hypoplastic left heart
8 Assessing the infant with Cyanosis Structured approach is key ABCD Identify life-threatening features requiring urgent intervention Make a diagnosis & definitive management plan
9 Airway and Breathing Assess the infants airway and breathing Signs of airway obstruction Effort of breathing Apnoeas Equal air entry Added sounds Administer oxygen ECG, saturation monitoring (pre & post ductal) Check for pneumothorax and if present clinically, consider the need for cold light examination, needle aspiration or chest drain insertion Blood gas
10
11
12 Management of pneumothorax Needle Thoracocentesis -Butterfly needle attached to three way tap and syringe -2 nd intercostal space -Mid clavicular line -Aspirate air until BP / saturations improve -Follow up with a definitive chest drain Chest Drain - See workshops
13 Recognition of respiratory distress in term babies Decide whether infant requires respiratory support and initiate Order a CXR early (don t wait until 4 hours of age) If PPHN is suspected special measures
14 Respiratory support in term babies Options: Supplemental oxygen (headbox, incubator, nasal cannulae NCPAP HHFNC oxygen Mechanical Ventilation Maintaining oxygenation, avoiding excessive work of breathing, strategies to avoid lung trauma Term babies are at risk of pneumothorax and PPHN
15 Circulation Is there a murmur? Are the pulses normal? Cyanosis associated with a murmur or abnormal pulses make a cardiac leasion more likely If pulses are diminished consider: Critically obstructed systemic circulation Severe sepsis Consider a formal cardiac assessment including cardiac ECHO, liaise with cardiology team Measure pre and post ductal saturations and perform a blood gas if not already done Consider starting prostaglandin
16 Prostaglandin There should be a low threshold for starting prostaglandin in an unwell infant. Consider starting if: There is a murmur and cyanosis If the infant has reduced pulses If the patient is in extremis
17 Disability Are there signs of neurological compromise? What is the blood sugar? Is the baby having seizures?
18 Factors to help discriminate between respiratory and cardiac pathology History Respiratory Prolonged ruptured membranes, maternal sepsis, meconium, difficult delivery Cardiac Antenatal scans, family history of congenital heart disease Examination Respiratory distress Cardiac signs (murmur, parasternal heaves) Relative lack of respiratory distress and signs on auscultation CXR Evidence of lung pathology: RDS, meconium aspiration, infection, CDH ECG Normal Abnormal Blood gases and response to increased FiO 2 High PaCO 2 Increasing oxygen improves saturations Decreased pulmonary vascular markings, cardiomegaly, abnormal cardiac shadow Low or normal PaCO 2 Increasing oxygen has little effect on saturations
19 Persistent Pulmonary Hypotension Failure of adaptation to ex-utero life Persistence of high pulmonary vascular resistance after birth leading to cyanosis from right to left shunting at ductal and atrial levels The heart is structurally normal
20 Causes Mechanisms Pulmonary vasoconstriction secondary to factors secondary to hypoxia and acidosis Decreased size of pulmonary vascular bed associated with pulmonary hypoplasia Chronic hypertrophy of pulmonary vascular smooth muscle inutero PPHN is associated with a number of conditions Meconium Aspiration Sepsis (Especially GBS) Birth asphyxia Respiratory distress syndrome Pulmonary hypoplasia Congenital diaphragmatic hernia
21 Clinical presentation Respiratory distress Difficulty in achieving oxygenation may be out of proportion to relative ease of maintaining normal PaCO2 Difference of >5% between pre and post ductal saturation measurements (pre=higher) Significantly higher pre ductal PaO2 (right radial artery) compared with post ductal PaO2 Chest X-ray may demonstrate a primary respiratory pathology

22
23 Goals of management Strategies aimed to reduce pulmonary vascular resistance: Optimise oxygenation FiO2 Ventilatory strategies Sedation and muscle relaxation Avoid and correct acidosis Systemic BP > pulmonary BP Inotropes Aim for a BP 5-10 greater than estimated pulmonary pressures Normal glucose, calcium and magnesium Correct polycythaemia Thermoregulation (refractory PPHN indication to rewarm in HIE) Consider inhaled nitric oxide
24 ECMO Criteria Neonates requiring ECMO treatment need to meet the following criteria: Inclusion Criteria: Exclusion Criteria: Oxygenation Index * (OI) >40 Gestational age >35 weeks Weight >2kgs Reversible lung disease Significant coagulopathy or uncontrollable bleeding Major (>grade 1) intracranial haemorrhage Irreversible lung injury Major congenital / chromosomal anomalies or severe encephalopathy Major cardiac malformation Mechanical ventilation days Cardiac arrest other than immediately at birth * OI = (Mean Airway Pressure [cmh20] x FiO2 [in percentage]) divided by (post ductal PaO2 [mmhg])

25
26 Duct dependent congenital heart Antenatal diagnosis Clinical signs disease Common presenting features Difficulty feeding secondary to increased breathlessness Cyanosis unresponsive to supplemental oxygen Acute cardiorespiratory collapse with shock




27 Diagnostic algorithm Blue Femoral pulses Y Murmur Y Fallot AVSD Tricuspid atresia Pulmonary atresia Critical Pulmonary stenosis N Transposition of the great arteries PPHN Total anomalous pulmonary venous circulation Pink Femoral pulses N Co-arctation of the aorta Hypoplastic left heart Critical aortic stenosis Y VSD / ASD/ Aortic stenosis / pulmonary stenosis
28 Management Airway and Breathing Intubate if indicated Pre-post ductal saturations Administer supplemental oxygen target saturations 75-85% Indications for intubation Apnoea Shock Respiratory failure
29 Management Circulation IV access consider UVC Treat hypotension (volume & dopamine) Prostin to maintain ductal patency 5ng/kg/min can be increased 4 limb BP ECHO ECG Side effects of prostin: Hypotension hypoglycaemia Apnoea (more common >10ng/kg/min) Fever Higher doses may be needed to open a closed duct following cardiology advice
30 Summary Structured approach is key - the initial goal should be to Identify life-threatening features requiring urgent intervention followed by diagnosis and definitive management Low threshold for mechanical ventilation rather than ncpap or NCHHFO 2 if respiratory support needed Term infants with respiratory disorders are at risk of PPHN which has a specific management strategy Think could the cause of cyanosis be cardiac
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease Document Control Information Author CATS/NTS Author Position CC Transport Services Document Owner E. Polke
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Pediatrics. Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test. Definition. See online here
 and Hyperoxia Test. Definition. See online here") Pediatrics Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test See online here Blue babies lack sufficient hemoglobin, resulting in the bluish discoloration of tissues, a term referred to as cyanosis.
Pediatrics Blue Baby Syndrome (Cyanotic Newborn) and Hyperoxia Test See online here Blue babies lack sufficient hemoglobin, resulting in the bluish discoloration of tissues, a term referred to as cyanosis.
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical
 Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Karen Corlett, RN, MSN, CPNP-AC/PC Pediatric Nurse Practitioner Congenital Heart Surgery Unit Pediatric Cardiac Intensivists of North Texas Medical City Children s Hospital, Dallas Hypoxia Shortage of
Extracorporeal Membrane Oxygenation (ECMO) Referrals
 Referrals") Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
CCHD Screening with Pulse Oximetry: A Success Story!
 CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
PAEDIATRIC EMQs. Andrew A Mallick Paediatrics.info.
 PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
PAEDIATRIC EMQs Andrew A Mallick Paediatrics.info www.paediatrics.info Paediatric EMQs Paediatrics.info First published in the United Kingdom in 2012. While the advice and information in this book is believed
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
1st Annual Clinical Simulation Conference
 1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Ummeenatrbilaoiasetptiwmsaiiri
 atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
atrial This This atrial CIRCULATORY CHANGES My My pressure In the foetus the left atrial is low as relatively Ummeenatrbilaoiasetptiwmsaiiri ze@fgffmftheyubsidtritupyeiirieminfyifjjtajefjjieiminylntentiiiarmmnitnteimiiiinc1udingfromthepl9centaj
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
PULMONARY VENOLOBAR SYNDROME. Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital.
 PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
Management of a child with cyanosis
 German Society of Paediatric Cardiology Guidelines Management of a child with cyanosis L. Kändler (Wittenberg), N. Haas (München), M. Gorenflo (Heidelberg) Acknowledged by the executive board of the German
German Society of Paediatric Cardiology Guidelines Management of a child with cyanosis L. Kändler (Wittenberg), N. Haas (München), M. Gorenflo (Heidelberg) Acknowledged by the executive board of the German
PPHN (see also ECMO guideline)
") Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Congenital Heart Disease. CCCHD In WI. Critical Congenital Heart Disease. Why Screen? 4/20/2018. Early Detection = Better Outcomes
 Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
Congenital Heart Disease A Positive Screen? What Does it Mean? A Review of Pulse Oximetry Screening for Critical Congenital Heart Disease Elizabeth Goetz MD MPH 8-10/1000 livebirths 3% of all infant mortality
CYANOSIS. İ.U. Cerrahpaşa Medical School Department of Pediatric Cardiology. İ. Levent SALTIK, MD
 CYANOSIS İ.U. Cerrahpaşa Medical School Department of Pediatric Cardiology İ. Levent SALTIK, MD CYANOSIS Cyanosis is a blue-purple discoloration of the skin and mucous membranes Cyanosis is not a disease
CYANOSIS İ.U. Cerrahpaşa Medical School Department of Pediatric Cardiology İ. Levent SALTIK, MD CYANOSIS Cyanosis is a blue-purple discoloration of the skin and mucous membranes Cyanosis is not a disease
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Scope: This guideline is aimed at all Health Care Professionals involved in the care of infants within the Neonatal Service.
 Persistent Pulmonary Hypertension of the Newborn (PPHN) University Hospitals of Leicester NHS NHS Trust June 2018 June 2021 Scope: This guideline is aimed at all Health Care Professionals involved in the
Persistent Pulmonary Hypertension of the Newborn (PPHN) University Hospitals of Leicester NHS NHS Trust June 2018 June 2021 Scope: This guideline is aimed at all Health Care Professionals involved in the
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care
 Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
Cardiology Competency Based Goals and Objectives
 Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Cardiology Competency Based Goals and Objectives COMPETENCY 1. Patient Care. Provide family centered patient care that is developmentally and age appropriate, compassionate, and effective for the treatment
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Ductal-dependent cardiac anomalies. Donna Cheung Pediatric Emergency Rotation January 31, 2014
 Ductal-dependent cardiac anomalies Donna Cheung Pediatric Emergency Rotation January 31, 2014 Case 1 A 6 day old Caucasian male presents to the ER with poor feeding and SOB. He was born FT via VD with
Ductal-dependent cardiac anomalies Donna Cheung Pediatric Emergency Rotation January 31, 2014 Case 1 A 6 day old Caucasian male presents to the ER with poor feeding and SOB. He was born FT via VD with
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Spectrum and age of presentation of significant congenital heart disease in KwaZulu Natal, South Africa
 Spectrum and age of presentation of significant congenital heart disease in KwaZulu Natal, South Africa EGM Hoosen, K Sprenger, H Dama, A Nzimela, M Adhikari KwaZulu Natal Population 10.3 million 3.3 million
Spectrum and age of presentation of significant congenital heart disease in KwaZulu Natal, South Africa EGM Hoosen, K Sprenger, H Dama, A Nzimela, M Adhikari KwaZulu Natal Population 10.3 million 3.3 million
Admission/Discharge Form for Infants Born in Please DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
Selection Criteria Admission/Discharge Form for Infants Born in 2016 To be eligible, you MUST answer YES to at least one of the possible criteria (A-C) A. 401 1500 grams o Yes B. GA range 22 0/7 31 6/7
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen
 Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Shock is defined as a state of cellular and tissue hypoxia due to : reduced oxygen delivery and/or increased oxygen consumption or inadequate oxygen utilization The effects of shock are initially reversible
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline.
 Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
Pediatric Learning Solutions course alignment with the Neonatal/Pediatric Specialty Examination Detailed Content Outline. The following Pediatric Learning Solutions courses align to focus areas of the
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
HFOV IN THE NON-RECRUITABLE LUNG
 HFOV IN THE NON-RECRUITABLE LUNG HFOV IN THE NON-RECRUITABLE LUNG PPHN Pulmonary hypoplasia after PPROM Congenital diaphragmatic hernia Pulmonary interstitial emphysema / cystic lung disease 1 30 Mean
HFOV IN THE NON-RECRUITABLE LUNG HFOV IN THE NON-RECRUITABLE LUNG PPHN Pulmonary hypoplasia after PPROM Congenital diaphragmatic hernia Pulmonary interstitial emphysema / cystic lung disease 1 30 Mean
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
: Provide cardiovascular preventive counseling to parents and patients with specific cardiac diseases about:
 Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Children s Hospital & Research Center Oakland Cardiology Primary Goals for this Rotation 5.13 GOAL: Prevention, Counseling and Screening (Cardiovascular). Understand the role of the pediatrician in preventing
Experience. Initials Medical Staffing Network Rev. 06/15 F01201 NNICU 2 of 5
 Neonatal Intensive Care Unit Self Assessment Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
Neonatal Intensive Care Unit Self Assessment Directions Please circle a value for each question to provide us and the interested facilities with an assessment of your clinical experience. These values
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Blue Babies, Twitchy Toddlers, and Kool Kids. By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN
 Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Objectives. Prenatal Diagnosis of Critical Congenital Heart Disease. The Law. Disclosure. Dylan s Story
 Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
It is important to distinguish the
 Diagnostic Considerations in Infants and Children with Cyanosis Gurumurthy Hiremath, MD; and Deepak Kamat, MD, PhD Abstract Cyanosis is defined by bluish discoloration of the skin and mucosa. It is a clinical
Diagnostic Considerations in Infants and Children with Cyanosis Gurumurthy Hiremath, MD; and Deepak Kamat, MD, PhD Abstract Cyanosis is defined by bluish discoloration of the skin and mucosa. It is a clinical
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
PUMANI bcpap GUIDELINES FOR CLINICIANS. An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use
 An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
Standard of Newborn Care in the Age of Birth Plans. Stephanie Deal, MD Tiffany McKee-Garrett, MD
 Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Standard of Newborn Care in the Age of Birth Plans Stephanie Deal, MD Tiffany McKee-Garrett, MD Disclosure We have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
T wo dimensional and Doppler echocardiography is being
 F287 ORIGINAL ARTICLE Evaluation of echocardiography on the neonatal unit S Moss, D J Kitchiner, C W Yoxall, N V Subhedar... See end of article for authors affiliations... Correspondence to: Dr Subhedar,
F287 ORIGINAL ARTICLE Evaluation of echocardiography on the neonatal unit S Moss, D J Kitchiner, C W Yoxall, N V Subhedar... See end of article for authors affiliations... Correspondence to: Dr Subhedar,
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Scope This guideline is aimed at all Health care professionals involved in the care of infants within the Neonatal Service.
 Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Management of Newborn Infants born through Meconium-stained liquor University Hospitals of Leicester NHS NHS Trust March 2018 March 2021 Scope This guideline is aimed at all Health care professionals involved
Hypoxic Respiratory Failure in the Newborn. Question and Answer
 Hypoxic Respiratory Failure in the Newborn Question and Answer Question: When administering nitric oxide to premature babies what is considered safe or common practice in terms of length of treatment?
Hypoxic Respiratory Failure in the Newborn Question and Answer Question: When administering nitric oxide to premature babies what is considered safe or common practice in terms of length of treatment?
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
PROSTIN VR STERILE SOLUTION
 PROSTIN VR STERILE SOLUTION PRODUCT INFORMATION PROSTIN VR STERILE SOLUTION (alprostadil; prostaglandin E 1 ) DESCRIPTION PROSTIN VR Sterile Solution contains 500 micrograms alprostadil in 1.0 ml of dehydrated
PROSTIN VR STERILE SOLUTION PRODUCT INFORMATION PROSTIN VR STERILE SOLUTION (alprostadil; prostaglandin E 1 ) DESCRIPTION PROSTIN VR Sterile Solution contains 500 micrograms alprostadil in 1.0 ml of dehydrated
PAEDIATRIC ACUTE CARE GUIDELINE. Resuscitation Coma
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
APPROACH TO CARDIAC HISTORY TAKING. Index
 Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Christopher Cheung APPROACH TO CARDIAC HISTORY TAKING Index General Presentation...1 2 Table 1 Congenital Heart Conditions...2 Questions to Ask...2 Table 2 PQRSTAAA Mnemonic Approach to Chest Pain...3
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
MANAGEMENT OF THORACIC TRAUMA. Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA
 MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease. Frequently Asked Questions
 Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Pulse Oximetry Screening in Newborns to Enhance the Detection Of Critical Congenital Heart Disease Frequently Asked Questions Current Recommendation: The current recommendation from the Canadian Cardiovascular
Three Decades of Managing Congenital Diaphragmatic Hernia
 Three Decades of Managing Congenital Diaphragmatic Hernia Desmond Bohn The Department of Critical Care Medicine The Hospital for Sick Children, Toronto Robert E Gross Congenital Diaphragmatic Hernia 1960-80
Three Decades of Managing Congenital Diaphragmatic Hernia Desmond Bohn The Department of Critical Care Medicine The Hospital for Sick Children, Toronto Robert E Gross Congenital Diaphragmatic Hernia 1960-80
Neonatal/Pediatric Cardiopulmonary Care
 Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Neonatal/Pediatric Cardiopulmonary Care Resuscitation 2 When To Resuscitate Need usually related Combination of Can occur in 3 Causes of Fetal Asphyxia 1 4 Apnea Hypoxia Stimulates chemoreceptors & baroreceptors
Oh SCH It s a neonatal emergency
 trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
trekk.ca 1 1 Oh SCH It s a neonatal emergency Emma Burns, MD, FRCPC IWK Health Centre 2 1 Objectives Critically ill neonate approach and tips Stay on time! Thanks to: Shannon MacPhee, Mike Young, Jon Cherry,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator