Lipids management and prevention of Stroke
|
|
|
- Cynthia Reynolds
- 5 years ago
- Views:
Transcription
1 Lipids management and prevention of Stroke Dr.Vamshi Mallavarapu MD, FACC,RPVI Director CCU, Abington Hospital-Jefferson Health Diplomat of American Board of Clinical Lipidology
2 None Disclosures
3 Objectives Discuss preventative therapy for stroke- Primary and secondary Focus on lipid lowering therapy Discuss new agents for low lipid lowering therapy
4 Epidemiology An estimated 6.6 million Americans 20 years of age Prevalence of stroke is 2.6% and for silent stroke is 6-8% By 2030, an additional 3.4 million people aged 18 years will have had a stroke, a 20.5% increase in prevalence from Each year, people experience a new or recurrent stroke Medicare beneficiaries showed that the rate of first stroke among patients aged >65 years decreased by 40% over the past 2 decades ( ), a decline driven primarily by marked reductions in the incidence of ischemic stroke. The decline in stroke rates occurred over a period of significant uptake in the use of medications that attenuate stroke risk: Statin use in the general population increased from4% in 1992 to 41% in 2008, and antihypertensive drug use increased from 53% in 1992 to 74% in Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
5 TIA Prevalence 2.3%- estimated ~5 million 15% all strokes are heralded by TIA 10-year stroke risk of roughly 19% and a combined 10-year stroke, MI, or vascular death risk of 43%(4% per year). 1-year mortality rate after a TIA ~12%. Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
6 Stroke Recurrence Recurrent stroke rates -1.8% at 1 month, 5% at 6 months, 8% at 1 year, and 18.1% at 4 years 987 ARIC participants with first-ever strokes, there were 183 recurrent strokes among 147 participants. Approximately 70% of recurrent strokes were of the same subtype; however, 28% were the same when the index stroke was lacunar. One-year stroke recurrence rates by index subtype were 7.9% for thrombotic, 6.5% for cardioembolic, and 6.5% for lacunar events Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
7 Mortality 1 person dies every 4 minutes Stroke accounted for 1 of every 20 deaths in the United States. When considered separately from other CVDs, stroke ranks No. 5 among all causes of death, behind diseases of the heart, cancer, CLRD, and unintentional injuries/accidents. Approximately 59% of stroke deaths occurred outside of an acute care hospital. More women than men die of stroke each year because of the larger number of elderly women. Women accounted for 58% of US stroke deaths in From 2003 to 2013, the age-adjusted stroke death rate decreased 33.7%, and the actual number of stroke deaths declined 18.2%. Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.

8 Percentage population attributable risk of main modifiable risk factors for acute myocardial infarction and stroke (ischemic and haemorrhagic stroke combined) based on the estimates from the INTERHEART study and the INTERSTROKE study. Population attributable risk (PAR) is estimating the proportion of a disease that can theoretically be attributed to a specific risk factor; estimates derived from the INTERHEART study and the INTERSTROKE study. Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
9 Hypertension- Risks - BP<120/80, 50% reduction in risk -10 mm Hg increase in levels of SBP, the increased stroke risk in whites is 8%; however, a similar 10 mm Hg increase in SBP in African Americans is associated with a 24% increase in stroke risk. Diabetes: Risk ratios In patients with TIA, impaired glucose tolerance doubles risk of recurrent stroke Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
10 Atrial fibrillation: Increases risk upto 5 fold Smoking: increases risk 2-4 fold Physical activity: decreases risk about 20-50% Family history CKD- Hazard ratio of 1.7 Sleep apnea Nutrition: Mediterranean diet: Hazard ratio of 0.54 Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.

11 Exercise capacity and muscle strength and risk of vascular disease and arrhythmia in 1.1 million young Swedish men: cohort study Kasper Andersen,1 Finn Rasmussen,2 Claes Held,1 Martin Neovius,3 Per Tynelius,2 Johan Sundström1 BMJ 2015;351:h4543
:1299-1306. doi:10.1016/j.jacc.2014.06.1190 Figure Legend:")
12 From: Low-Risk Diet and Lifestyle Habits in the Primary Prevention of Myocardial Infarction in Men: A Population-Based Prospective Cohort Study J Am Coll Cardiol. 2014;64(13): doi: /j.jacc Figure Legend:

13
14 Lipids and cerebrovascular disease The relationship between lipids and stroke is complex. Direct relationship between cholesterol levels and ischemic stroke, varies by stroke subtype, with associations strongest for atherosclerotic subtypes. Increased risk of intracerebral hemorrhage at low cholesterol levels Data strongest for total cholesterol (TC) and low-density lipoprotein-cholesterol Lipids and Cerebrovascular Disease: Research and Practice.Yaghi, Shadi MD; Elkind, Mitchell S.V. MD, MS. Issue: Volume 46(11), November 2015, p
15 HDL Decreased risk of ischemic stroke ranging from 11% to 15% for each 10-mg/dL increase in HDL-C HDL2- increased atherosclerosis HDL3- decreased atherosclerosis Lipids and Cerebrovascular Disease: Research and Practice.Yaghi, Shadi MD; Elkind, Mitchell S.V. MD, MS. Issue: Volume 46(11), November 2015, p
16 Triglycerides Association between higher triglyceride levels and relative risk (RR) of stroke (adjusted RR, 1.05; 95% CI, 1.03 to 1.07) for each 10-mg/dL increase in baseline triglycerides. Studies have also shown that triglycerides levels are inversely associated with hemorrhagic stroke risk Lipids and Cerebrovascular Disease: Research and Practice.Yaghi, Shadi MD; Elkind, Mitchell S.V. MD, MS. Issue: Volume 46(11), November 2015, p
17 Cholesterol and stroke subtype stratified for the history of prior myocardial infarction (MI) based on estimates from the MRFIT study
18 INTERSTROKE: Population-attributable risk for common risk factors Risk factor Population-attributable risk, % (99% CI) Hypertension 34.6 ( ) Smoking 18.9 ( ) Waist-to-hip ratio (tertile 2 vs tertile 1) 26.5 ( ) Dietary risk score (tertile 2 vs tertile 1) 18.8 ( ) Regular physical activity 28.5 ( ) Diabetes 5.0 ( ) Alcohol intake 3.8 ( ) Cardiac causes 6.7 ( ) Ratio of apolipoprotein B to A ( ) (tertile 2 vs tertile 1) Psychological factors Stress 4.6 ( ) Depression 5.2 ( ) *For the protective factor of physical activity, the population-attributable risks are provided for individuals who do not participate in regular physical activity. O'Donnell MJ et al. Lancet 2010; available at:
19 Meta-analysis : Statin and Stroke N total= Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
20 Meta-Analysis Stroke Death Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
21 Meta-analysis Hemorrhagic stroke Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
22 Stroke Risk and LDL Lowering Each 1 mmol (39 mg) LDL-C reduction reduced the risk of stroke by 21% (95% CI 6.3 to 33.5%, p<0.001) Total n=165,732 Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
23 N=17,802 LDL-c<130 mg/dl hscrp >2 mg/dl F/U 1.9 yrs JUPITER Men >50 yrs Women >60 yrs Event Rosuva * Placebo * Hazard Ratio Risk Reduction (CI) Primary endpoint 142 (1.6%) 251 (2.8%) 44% (31-54) p= Any MI 31 (0.35%) 68 (0.76%) 54% (30-70) Stroke 33 (0.37%) 64 (0.72%) 48% (21-66) p=0.002 Revascularisation or Unstable angina 76 (0.85%) 143 (1.6%) 47% (30-60) MI, Stroke, CVdeath 83 (0.93%) 157 (1.8%) 47% (30-61) * N (% randomised) Favours Rosuvastatin Favours Placebo
 27% reduction p=0.0236 0 0,0 0,5 1,0 1,5 2,0 2,5 3,0 3,5 Years Sever PS, Dahlöf B, Poulter N, Wedel H, et al, for the ASCOT Investigators. Lancet. 2003;361:1149-58")
24 Secondary End Point: Fatal and Nonfatal Stroke 3 Atorvastatin 10 mg Number of events 89 (1.7%) Placebo Number of events 121 (2.4%) Cumulative Incidence (%) 2 1 HR = 0.73 ( ) 27% reduction p= ,0 0,5 1,0 1,5 2,0 2,5 3,0 3,5 Years Sever PS, Dahlöf B, Poulter N, Wedel H, et al, for the ASCOT Investigators. Lancet. 2003;361:
25 CARDS: Cumulative Hazard for Stroke Cumulative Hazard (%) Atorvastatin10 mg Placebo Placebo n=39 [31% of all first CVD events] Atorvastatin n=21 48% Risk Reduction In Stroke (P=0.016) [25% of all first CVD events] Years from Randomization Hitman GA, et al. EASD Diabetologia. 2005; Abstract 120 Data on file, Pfizer Inc.
26 Pleiotropic Effects Studied Parameter Within the Plaque Control Group n=13 Pravastatin Group n=11 P Value Lipid contain (Oil Red O) 23.9% 8.2% <0.001 Ox-LDL (NA59) 22% 13.3% <0.001 Macrophage contain 25.3% 15.3% <0.05 T-Cell count 23.4% 11.2% <0.05 SMC 16.9% 24.3% <0.05 Apoptotic Cells (TUNEL) 32% 17.7% <0.05 Crisby et al. Circulation 2001
27 Between-Group LDL Reduction and Carotid- IMT Reduction Per Year r=0.70, p= For Each 10% LDL-cholesterol IMT reduction per year = 0.76% (95%CI, ) Amarenco et al. Stroke 2004;35:2902-9



28 Stroke: Potential Mechanisms of Benefit LDL Reduction Statin 35 to 80% of the benefit Plaque stabilization: macrophages smooth muscle cells immunologic response lipid core oxidized LDL Neuroprotection. Up-regulation NO. Improves CBF. Reduces infarct size Blood pressure reduction Decrease incidence of MI and of left ventricular mural thrombus Improved endothelial function Reduced hemorheologic stress Reduced platelet aggregation Reduced thrombotic and Enhanced fibrinolytic state

29 HPS: No Reduction in Risk of Recurrent Stroke in Patients With Prior Cerebrovascular Disease Patient with Event (5) n=406 n=488 Major Vascular Events n=169 n=170 Stroke *29% RR, P=.001 Heart Protection Study Collaborative Group. Lancet. 2004;363:
30 Clinical Trial data Treat stroke to target Trial-Expected results Dec 2018
31 SPARCL: Study Design Patient Population 205 sites worldwide Double-Blind Period Atorvastatin 80 mg/day Previously documented stroke or TIA within 6 months 4,731 Patients No history of CHD LDL-C levels 100 mg/dl and 190 mg/dl Placebo 540 Primary Endpoints Primary End Point Time to the First Occurrence of a Fatal or Nonfatal Stroke Source: The SPARCL Investigators. Cerebrovasc Dis. 2003;16:
32 140 LCL-C During Follow-up Baseline LDL-C: 133 mg/dl +1% 120-7% 100 Mean (mg/d % Mean on-treatment LDL-C: Placebo = 129 mg/dl -38% 20 Atorvastatin = 73 mg/dl 0 Baseline Month 3 Year 1 Year 3 Year 5 Last Timepoint Amarenco P, Bogousslavsky J, Callahan A III, et al. N Engl J Med. 2006;355:549-59
33 Primary Endpoint: Time to Fatal or Non-Fatal Stroke Fatal or Non-Fatal Stroke (%) 16% 12% 8% 4% Placebo Atorvastatin Adjusted HR (95% CI)* = 0.84 (0.71, 0.99), p = % RR 0% Years Since Randomization * Treatment effect from Cox proportional hazards models with pre-specified adjustment for geographical region, entry event, time since entry event, gender, and baseline age. Amarenco P, Bogousslavsky J, Callahan A III, et al. N Engl J Med. 2006;355:549-59
34 Secondary Endpoint: Time to Major Coronary Event 8% Major Coronary Event (%) 6% 4% Placebo Atorvastatin 35% RR 2% 0% Adjusted HR (95% CI)* = 0.65 (0.49, 0.87), p = Years Since Randomization * Treatment effect from Cox proportional hazards models with pre-specified adjustment for geographical region, entry event, time since entry event, gender, and baseline age. Amarenco P, Bogousslavsky J, Callahan A III, et al. N Engl J Med. 2006;355:549-59
35 Gender: Stroke Outcomes Gender X Treatment Interaction p-value All Stroke Women Men Non-fatal Stroke Women Men Fatal Stroke Women Men Treatment Better Placebo Better Adjusted Hazard Ratio Pre-specified adjustment for region, entry event, time since entry event and age Goldstein LB, Amarenco P, Callahan A III, al.. Stroke. 2008;39:
36 Ischemic and Hemorrhagic Stroke Post hoc analysis Ischemic or Hemorrhagic Stroke (%) Fatal and Non-fatal Stroke Placebo: Ischemic Atorvastatin: Ischemic Placebo: Hemorrhagic Atorvastatin: Hemorrhagic Ischemic: HR (95% CI) = 0.79 (0.66, 0.95) Hemorrhagic: HR (95% CI) = 1.68 (1.09, 2.59) Years Since Randomization Unadjusted HR Goldstein LB, Amarenco P, Szarek M, al. Neurology ;70:
37 Impact of Atorvastatin on Hemorrhagic stroke by Entry Event Goldstein LB, Amarenco P et al. Neurology. 2008;70: Entry Event HR (95% CI) P-value Large Vessel 1.23 (0.44, 3.39) TIA 0.97 (0.44, 2.17) Hemorrhagic 4.67 (0.96, 22.6) Small Vessel 5.07 (1.73, 14.9) Unknown 0.80 (0.30, 2.13) *Adjusted for time since entry event, gender, and age Hazard ratio* Atorvastatin better Placebo better

38 Benefit/Risk P=0.002 P= % Incidence (%) 11.2% 13.1% 14.1% Major Coronary Event Ischemic Stroke Hemorrhagic Stroke Unclassified Stroke Atorvastatin n = 2365 Placebo n = 2366 Atorvastatin n = 2365 Placebo n = 2366 Stroke Stroke and Major Coronary Events Amarenco P, et al. Exp Op Pharmacotherapy. 2007
39 Effect of Atorvastatin on Stroke In SPARCL Patients with Diabetes Percentage of Patients Free of End Points RR: 30% HR=0.70 (95% CI 0.50, 0.98), P=0.0387* Log-rank P= Atorvastatin 80 mg Placebo *Adjusted for entry event, time since entry event, gender, age, and geographic region Years since randomization Callahan A, Welch KMA, Amarenco P, et al. 6
40 Effect of Atorvastatin on CV Events In SPARCL Patients with Diabetes Percentage of Patients Free of End Points Any CHD Event RR: 51% Atorvastatin 80 mg Placebo HR=0.49 (95% CI 0.31, 0.79), P=0.0033* Log-rank P= Percentage of Patients Free of End Points Any Revascularization RR: 64% Atorvastatin 80 mg Placebo HR=0.36 (95% CI 0.21, 0.61), P=0.0001* Log-rank P= Years since randomization Years since randomization *Adjusted for entry event, time since entry event, gender, age, and geographic region Callahan A, Welch KMA, Amarenco P, et al.
41 Stroke in Patients With Carotid Stenosis Patients free of fatal or non-fatal stroke (%) RR: 33% Atorvastatin Placebo HR=0.67 (95% CI 0.47, 0.94), P=.02* Years since randomization *: adjusted for entry event, time since entry event, gender, age, and geographical region Sillesen H, Amarenco P, Hennerici MG, et al. Stroke. 2009;40:E-pub
42 Any Cardiovascular Event in patients With Carotid Stenosis 100 Atorvastatin Patients free of any cardiovascular event (%) RR: 42% Placebo 60 HR=0.58 (95% CI 0.46, 0.73), P< Years since randomization *: adjusted for entry event, time since entry event, gender, age, and geographical region Sillesen H, Amarenco P, Hennerici MG, et al. Stroke. 2009;40:E-pub
43 Stroke Risk and LDL Lowering Each 1 mmol (39 mg) LDL-C reduction reduced the risk of stroke by 21% (95% CI 6.3 to 33.5%, p<0.001) N total= Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
 0.67 (0.52, 0.86) 0.84 (0.50, 1.40) 1.04 (0.61, 1.78) 0.3394 0.0018 0.4716 0.8864 0.4 0.7 1.")
44 Time Varying LDL-C and Stroke Risk All Stroke HR (95% CI) p-value 0% Increase 1.00 <50% Decrease 50% Decrease 0.89 (0.73, 1.08) 0.69 (0.55, 0.87) Ischemic Stroke 0% Increase 1.00 <50% Decrease 50% Decrease Hemorrhagic Stroke 0% Increase 1.00 <50% Decrease 50% Decrease 0.90 (0.73, 1.12) 0.67 (0.52, 0.86) 0.84 (0.50, 1.40) 1.04 (0.61, 1.78) Note: Percent change effects from Cox proportional hazards Hazard Ratio (95% CI) models with adjustment for gender and baseline age with reference group = no change or increase Amarenco P, Goldstein LB, Szarek M, et al. Stroke. 2007;38:
45 Meta-analysis: Intensive LDL-C Lowering vs. Standard Statin Therapy Fatal and Nonfatal STROKE Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63
46 Meta-analysis: Intensive Lipid-Lowering vs. Standard Statin Therapy MAJOR CARDIOVASCULAR EVENTS Amarenco P, Labreuche J. Lancet Neurol. 2009; 8:453-63

47
48 A. More statin vs less statin (5 trials: 0.51 mmol/l LDL difference) Any major coronary event Any coronary revascularization Any stroke 5 trials: any major vascular event B. Statin vs control (21 trials: 1.07 mmol/l LDL difference) Any major coronary event Any coronary revascularization Any stroke 21 trials: any major vascular event C. More statin vs less statin vs control (26 trials) Vascular events Major vascular event Patients with type 1 diabetes Patients with type 2 diabetes Patients without diabetes Any vascular event Mortality Cause-specific mortality All cardiac Stroke Any vascular Any non-vascular All-cause mortality (any death) Effect of Statins on CV Event Rates Related to 1 mmol/l LDL Reduction 1725 (1.9) 2250 (2.6) 572 (0.6) 3837 (4.5) 3380 (1.3) 3103 (1.2) 1730 (0.7) 7136 (2.8) 145 (4.5) 2494 (4.2) 8272 (3.2) 10,973 (3.2) 3333 (0.9) 483 (0.1) 4220 (1.2) 2943 (0.8) 7642 (2.1) 1973 (2.2) 2741 (3.2) 663 (0.7) 4416 (5.3) 4539 (1.7) 4066 (1.6) 2017 (0.8) 8934 (3.6) 192 (6.0) 2920 (5.1) 10,163 (4.0) 13,350 (4.0) 3384 (1.1) 501 (0.1) 4220 (1.2) 2994 (0.8) 8327 (2.3) Relative risk per 1 mmol/l (39 mg/dl) reduction in LDL-C (95% CI) More statin better Statin better 0.74 ( ) 0.66 ( ) 0.74 ( ) 0.72 ( ) 0.76 ( ) 0.76 ( ) 0.85 ( ) 0.79 ( ) 0.77 ( ) 0.80 ( ) 0.78 ( ) 0.78 ( ) 0.84 ( ) 0.96 ( ) 0.86 ( ) 0.92 ( ) 0.90 ( ) Statin or more statin better Less statin better Control better Control or less statin better CCT Trialists. Lancet 2010;376:1670
49 Reported Adverse Effects of Statins Muscle-related symptoms Elevated hepato-cellular enzymes Cancer New diabetes Hemorrhagic stroke Fatigue Neuro-psychiatric effects and insomnia Proteinuria / hematuria Erectile dysfunction Alopecia
50 Mancini GB et al. CJC 2011; 27: Muscle Adverse Effects of Statin Clinical features include Muscle aches, myalgia, weakness Stiffness, and cramps CK not increased in most patients Compromises quality of life Reduces medication adherence Major symptom limiting the use of statins
51 Risk Factors for Statin Induced Myopathy Patient Characteristics Demographics Older Age, Female gender Asian race Genetic Predisposition Transporters SLCO1B1 CYP isoenzymes Comorbidities Hypothyroidism Systemic disease Alcoholism / drugs Major surgery Myopathy Hereditary (PYGM, CTP II, AMPD) Acquired FH of statin intolerance
52 Therapeutic Options for Management of Statin Intolerant Patient Dietary and health behaviour measures Statin based strategies Alternative statin Alternative dosing Non-statin alternatives and adjuncts Ezetimibe Bile acid sequestrants Fibrates Niacin
53 Other Lipid-Lowering Drugs Niacin: A meta-analysis of 11 studies (n=9959 subjects) showed no association between the use of niacin and the risk of stroke (OR, 0.88; 95% CI, 0.50 to 1.54). Fibric acid derivatives: Veterans Affairs-HDL Intervention Trial (VA-HIT) among men with coronary artery disease and low HDL-C, benzofibrate provided a 31% reduction in stroke risk(p=0.036). A recent meta-analysis, however, included 18 trials, and > patients provided no evidence that fibrates reduce stroke risk (RR reduction, -3%; 95% CI, -16 to 9). Lipids and Cerebrovascular Disease: Research and Practice.Yaghi, Shadi MD; Elkind, Mitchell S.V. MD, MS. Issue: Volume 46(11), November 2015, p

54 Ezetimibe: Background Ezetimibe inhibits Niemann-Pick C1- like 1 (NPC1L1) protein, located primarily on the epithelial brush border of the GI tract resulting in reduced cholesterol absorption When added to statin, produces ~20% further reduction in LDL-C Two recent human genetic analyses have correlated polymorphisms in NPC1L1 with lower levels of LDL-C and lower risk of CV events* *MI Genetics Consortium Investigators NEJM 2014; online Nov 12; Ference BA et al AHA 2014

55 LDL-C and Lipid Changes 1 Yr Mean LDL-C TC TG HDL hscrp Simva EZ/Simva Δ in mg/dl Median Time avg 69.5 vs mg/dl

56 CV Death, Non-fatal MI, or Non-fatal Stroke HR 0.90 CI (0.84, 0.97) p=0.003 NNT= 56 Simva 22.2% 1704 events EZ/Simva 20.4% 1544 events 7-year event rates
57 Individual Cardiovascular Endpoints and CVD/MI/Stroke HR Simva* EZ/Simva* p-value All-cause death CVD CHD MI Stroke Ischemic stroke Cor revasc 30d UA CVD/MI/stroke Ezetimibe/Simva Better Simva Better *7-year event rates (%)
58 Dyslipidemia Recommendations 1. Statin therapy with intensive lipid-lowering effects is recommended to reduce risk of stroke and cardiovascular events among patients with ischemic stroke or TIA presumed to be of atherosclerotic origin and an LDL-C level 100 mg/dl with or without evidence for other clinical ASCVD (Class I; Level of Evidence B). (Revised recommendation) 2. Statin therapy with intensive lipid-lowering effects is recommended to reduce risk of stroke and cardiovascular events among patients with ischemic stroke or TIA presumed to be of atherosclerotic origin, an LDL-C level <100 mg/dl, and no evidence for other clinical ASCVD (Class I; Level of Evidence C). (New recommendation) 3. Patients with ischemic stroke or TIA and other comorbid ASCVD should be otherwise managed according to the 2013 ACC/AHA cholesterol guidelines, which include lifestyle modification, dietary recommendations, and medication recommendations (Class I;Level of Evidence A). (Revised recommendation) Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
59 Clinical ASCVD* LDL-C 190 mg/dl, Age 21 years Primary prevention Diabetes: Age years, LDL-C mg/dl Primary prevention - No Diabetes : 7.5% 10-year ASCVD risk, Age years, LDL-C mg/dl Circulation 2016 Jan 26;133(4): Executive Summary: Heart Disease and Stroke Statistics Update: A Report From the American Heart Association.
60 Cryptogenic stroke Retrospective study of 1008 patients with crypotgenic stroke Patients on statins, less likely to have recurrent cardiovascular events, (hazard ratio 0.23, 95% confidence interval ; p = 0.006) Statins after ischemic stroke of undetermined etiology in young adults. Putaala et.al., 2011 Aug 2;77(5):426-30
61 PCSK9 inhibitors Pharmacology: Human monoclonal antibody that inhibits PCSK9 PCSK9 is a protease that degrades LDL receptors on hepatocytes. LDL receptors clear circulating LDL
62 LDL Receptor Function and Life Cycle 62
63 The Role of PCSK9 in the Regulation of LDL Receptor Expression 63 63

64 Impact of an Anti-PCSK9 mab on LDL Receptor Expression 64 64

65

66

67 OSLER study- Evolocumab
68
69
70
71

72 CETP inhibitors
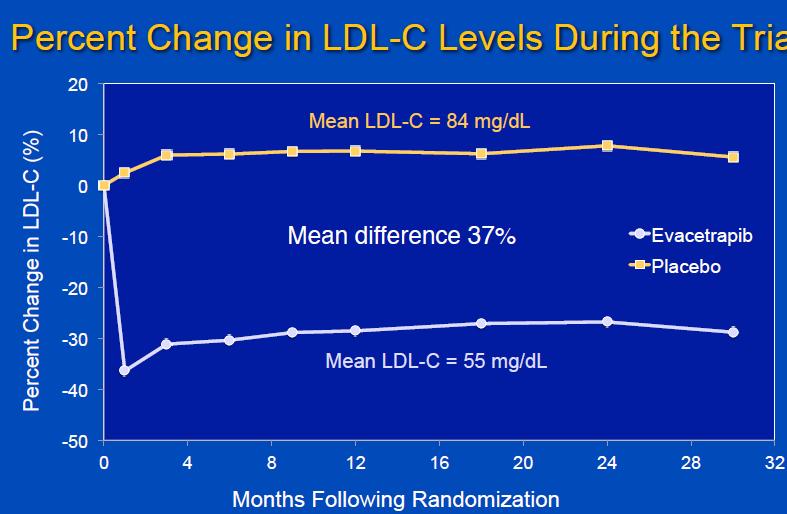
73 ACCELERATE ACC 2016

74

75

76
77 Mipomersen Inhibits protein synthesis of apob Reduces LDL ~30% Injected weekly No outcomes trials
78 Conclusions Statins are highly effective in primary and secondary stroke prevention Lifestyle modifications are equally important in reducing stroke risk Promise for newer therapies for lipid modification
79 Questions?
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Game Strategy: High Intensity Statin in Stroke. K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018
 Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
Game Strategy: High Intensity Statin in Stroke K.M. Osei MD, MSc Cardiovascular Conference PARMC Feb 24, 2018 No Disclosures Are you Mind Full or Mindful? Objectives 1. Discuss the correlation between
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP
 STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
STATIN THERAPY IN THE ELDERLY: THERE ARE MILES TO GO BEFORE WE SLEEP Peter P. Toth, MD, PhD, FAAFP, FICA, FNLA, FCCP, FAHA, FACC Director of Preventative Cardiology CGH Medical Center, Sterling, Illinois
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Zürcher Herzkurs, New drugs and interactions. LDL - what else?
 Zürcher Herzkurs, 29.09.2017 New drugs and interactions LDL - what else? Heinz Drexel, MD, FESC, FAHA, FRCP (Ed.) VIVIT Institut am Akademischen Lehrkrankenhaus Feldkirch, A Private Universität im Fürstentum
Zürcher Herzkurs, 29.09.2017 New drugs and interactions LDL - what else? Heinz Drexel, MD, FESC, FAHA, FRCP (Ed.) VIVIT Institut am Akademischen Lehrkrankenhaus Feldkirch, A Private Universität im Fürstentum
Statin intolerance. Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France
 Statin intolerance Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France Disclosure Statement of Financial Interest I currently have, or have had over the last two
Statin intolerance Pr Franck Boccara, MD, PhD Cardiologie, INSERM UMRS938 CHU St Antoine, UPMC, Paris, France Disclosure Statement of Financial Interest I currently have, or have had over the last two
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice
 Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Epidemiology and Prevention of Stroke
 Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Copyright Information Copyright protected material has been deleted from this presentation. References to the deleted material are provided for each slide. Epidemiology and Prevention of Stroke Larry B.
Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation
 TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and