RENAL SYMPATHETIC DENERVATION PAST, PRESENT AND FUTURE
|
|
|
- Job O’Brien’
- 5 years ago
- Views:
Transcription

1 RENAL SYMPATHETIC DENERVATION THE ROLE OF THE SYMPATHETIC NERVOUS SYSTEM PAST, PRESENT AND FUTURE Dr RS DAWOOD DEPARTMENT OF CARDIOLOGY CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL SATURDAY 02/08/2014
2 FACT OR ILLUSION
3 PHENOMENON OR NOUMENON
4
5 Systemic HPT is a major global public health burden and represents a major cardiovascular (CV) epidemic in the developed and developing world It is the leading attributable cause of mortality worldwide, causing 7,5 million deaths annually Projections by 2025 suggest that up to 50% of the adult populations of Western countries will meet standard guideline definitions of HPT
6 Every 20/10 mm Hg increase in blood pressure is associated with the doubling of 10 year CV mortality A recent meta-analysis by Law et al (BMJ 2009) showed that irrespective of the type of medication used, the incidence of coronary heart disease events was reduced by 22%, after a systolic BP reduction of 10 mm Hg or diastolic BP reduction of 5 mm Hg. Even more, the incidence of stroke was reduced by 41% Despite the plethora of anti-hpt drugs, HPT remains resistant in a considerable no. of patients (5-30%), thus creating the need for an alternative strategy including interventional approaches. Treated hypertensive patients 12,8%
, starting at BP 115/75 mm Hg. Lewington S, et al. Lancet.")
7 CV Mortality Risk 8 8x x 3 2 2x /75 135/85 155/95 175/105 SBP/DBP, mm Hg CV = cardiovascular. SBP = systolic blood pressure. DBP = diastolic blood pressure. *In individuals aged 40 to 69 years (10-year study period), starting at BP 115/75 mm Hg. Lewington S, et al. Lancet. 2002;360:


8 s Thoracolumbar splanchni -cectomy s Refined animal models of RDN 2013-beyond Many new RDN technologies New applications beyond HTN s Medical treatments improved Early physiology sympatheti c tone s Sophisticated measurement of sympathetic tone Clinical studies of HTN treatment (HTN 1 & HTN 2)
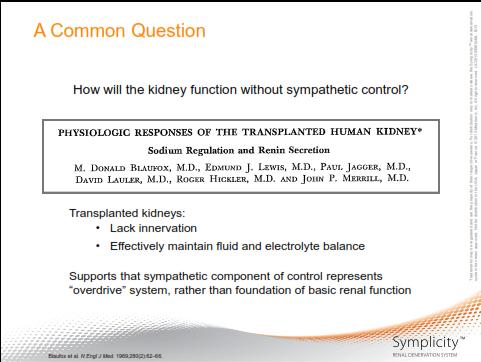
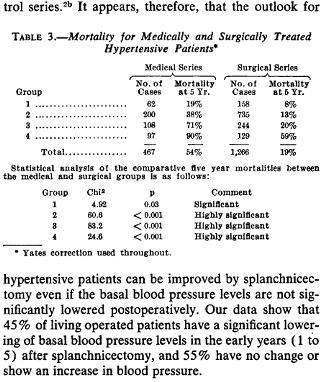
9 There is ample evidence that sympathetic nervous system (SNS) hyperactivity contributes to the initiation, maintenance and progression of HPT, with the renal SNS playing a crucial role. It is customary to acknowledge that amongst the earliest insights into the influence of the renal nerves on renal function was that of Claude Bernard in He observed cutting the greater splanchnic nerve (i.e. renal denervation) produced diuresis, whereas electrical stimulation of its peripheral cut end produced antidiuresis. Before the advent of pharmacological therapy, radical sympathectomy (or variations thereof e.g. splanchnicectomy) were performed for malignant HPT (100% 5 yr mortality) pioneering work done by Smithwick et al in the 1940 s.

10 Papademetriou V et al. International Journal of Hypertension. Volume Article ID





11 Nerves arise from T10 - L2 The nerves arborize around the artery and primarily lie within the adventitia Vessel Lumen Media Adventitia Renal Nerves




12 N S S N=schwann cells associated with multiple axons F=endoneurial fibroblasts, S=Schwann cells, P = pericyte Nonmyelinated Efferent Nerve Bundle Longitudinal Cross-section

![5] Neurofilament protein [NFP] Efferent nerve fibers Afferent nerve fibers UnMyelinated 96%](/docs-images/86/94125354/images/13-3.jpg "Myelinated 4% Sensory Aδ [pain fibers] Sensory C Adrenergic Nerve growth Factor [NGF] NGF")
![receptor p75 [NGFRp75] Tyrosine kinase receptor-a [Trk-A] Substance P [SP] Nerve development](/docs-images/86/94125354/images/13-4.jpg "and survival Substance P Calcitonin gene-related peptide [CGRP] Neuropeptide Y [NFY]")
13 Neural Recognition Markers Sympathetic nerves around the renal artery NEURAL MARKERS Protein Gene Product 9.5 [PGP9.5] Neurofilament protein [NFP] Efferent nerve fibers Afferent nerve fibers UnMyelinated 96% Myelinated 4% Sensory Aδ [pain fibers] Sensory C Adrenergic Nerve growth Factor [NGF] NGF receptor p75 [NGFRp75] Tyrosine kinase receptor-a [Trk-A] Substance P [SP] Nerve development and survival Substance P Calcitonin gene-related peptide [CGRP] Neuropeptide Y [NFY] Neuropeptide Y Dopamine b-hydroxylase (DBH) Tyrosine Hydroxylase [TH] adapted from Tokushige, 2007







![Substance P [SP] RED:](/docs-images/86/94125354/images/14-12.jpg "Tyrosine Calcitonin")
14 Immuno-Localization of Select Neuronal Markers in Human Renal Arteries V A N N N N V V V N Hematoxylin & Eosin PGP 9.5 NFP Dual Staining: Efferent and Afferent Sensory Neurons V A N V V Tyrosine Hydroxylase IF PGP9.5 = Protein Gene Product NFP = Neuro Fibrillary Protein RED: Tyrosine Hydroxylase Green: Substance P [SP] RED: Tyrosine Hydroxylase Green: Calcitonin Gene Related Peptide [CGRP]
15





16 Dr. Reginald H. Smithwick 1952 Photo of Dr. Smithwick reproduced with permission from JAMA.
17
18 % SURVIVALS Group 4 Group 1 Group 1 Group 2 Group 3 Group 4 SURVIVAL RATE OF NORMAL POPULATION Age 43 Group 2 Group 3 SURGICAL MEDICAL TIME IN YEARS Redrawn From Smithwick and Thompson; JAMA.1953;152:
19
20
21
22
23 Although improvement in BP and survival benefit, issues arose: skilled surgeon with specialised expertise required prolonged hospital stay (2 4 weeks) long recovery period (1 2 months) only few centres in the U.S and Europe As procedure was non-selective (affected abdominal, pelvic, lower extremity innervation), systemic side effects experienced: orthostatic hypotension and tachycardia bowel and bladder dysfunction sexual dysfunction thoracic duct injury
24 Advent of effective pharmacological therapy made surgical sympathectomy unattractive and undesirable in most patients which drove surgical sympathectomy into obscurity Building on the concept of surgical sympathectomy to control HPT, a novel catheter based endovascular renal artery sympathetic denervation (RASD) has been developed which offers more selective sympathetic denervation with: no systemic side effects (as selective and specific) localised procedure, minimally invasive short procedure and recovery times can be assumed to be widely adaptable




25 Lifestyle Medication Devices
26 Lifestyle Influence on blood pressure Weight BMI kg/m2 5 20mmHg/ 10kg Food Fruit, vegetable 6 14 mmhg Salt Salt intake < mg/day 3 8 mmhg Exercise 30 min/day, min 5 days/week 4 9 mmhg Alcohol Total Men: <2E alcohol/day Women: <1E alcohol/day 2 4 mmhg 20 mmhg!

27 After a 2 year loan to the United States, David returns to Italy



28 Proud Sponsors



29 Centrally acting antihypertensives Baroreceptor discharge Vascular smooth muscle Calcium-channel blockers α 1 -blockers α 1 Ca 2+ AT ARBs Vasodilation β -blockers β-blockers reset peripheral resistance β -blockers Renin Angiotensinogen Angiotensin I Na + Thiazide diuretics Angiotensin II ACEIs Aldosterone Peripheral resistance 1. Izzo JL, Black HR, Sica DA, eds. Hypertension Primer. 4th ed Schlaich MP, et al. Hypertension. 2009;54:


30 Uncontrolled Hypertension Includes all patients who lack BP control on treatment, including those on inadequate treatment regimens, those with poor adherence, white coat hypertension those with undetected secondary hypertension, as well as those with true treatment resistance 1 Resistant Hypertension Resistant Hypertension BP that remains above goal in spite of compliance with full doses of 3 antihypertensive medications of different classes; ideally, 1 of the 3 agents should be a diuretic 1 The treatment plan must include attention to lifestyle measures 2 Includes those patients who achieve BP control but require 4 antihypertensive agents to do so 1 1. Calhoun DA, et al. Circulation. 2008;117:e510-e Mancia G, et al. Eur Heart J. 2007;28:
 (+) (+) (+) Afferent feedback Differential")
 Rostral ventrolateral medulla (RVLM) Pariaqueductal gray")

31 Peripheral chemoreceptors (+) CNS-MAP set point PAG NTS Baroreceptors (-) elec. stim carotid body carotid sinus PVN RVLM (+) (+) (+) (+) Afferent feedback Differential patterning Sympathetic Set Point Nucleus tractus solitarus (NTS) Hypothalamic paraventricular nucleus (PVN) Rostral ventrolateral medulla (RVLM) Pariaqueductal gray (PAG) Contractility Capacitance RAAS Resistance Heart Rate Resistance Na + Reabsorpt n Re-modelling Immune Resistance Bone marrow MAP Perfusion Pressure Organ Blood Flow Sobotka, Osborn, Paton. Euro Intervention 2013
32 DiBona GF et al, Am J Physiol Regul Integr Comp Physiol 298:R246, 2010
 Reduce renal blood flow via renal arterial constriction (α1a - AR)")

33 Renal sympathetic efferent nerves Promote renin release (β1 - AR) Increase tubular sodium reabsorption (α1b - AR) Reduce renal blood flow via renal arterial constriction (α1a - AR) Renal sympathetic afferent nerves Modulate CNS outflow Mechanoreceptors & chemoreceptors signal renal injury Feedback to hypothalamus and contralateral kidney Bunte MC et al. JACC Interv. 2013; 6(1)1-9


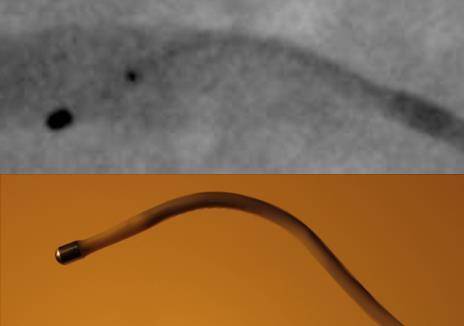
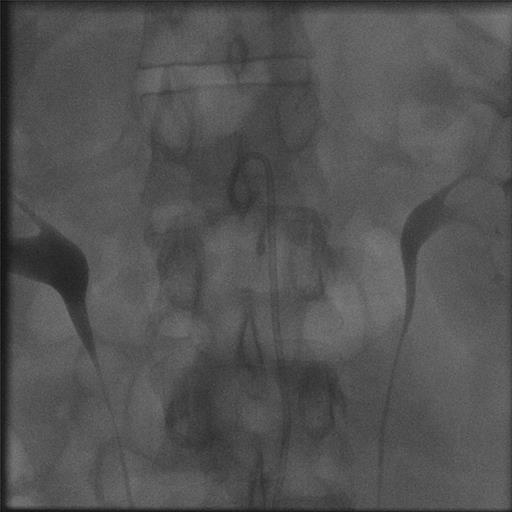
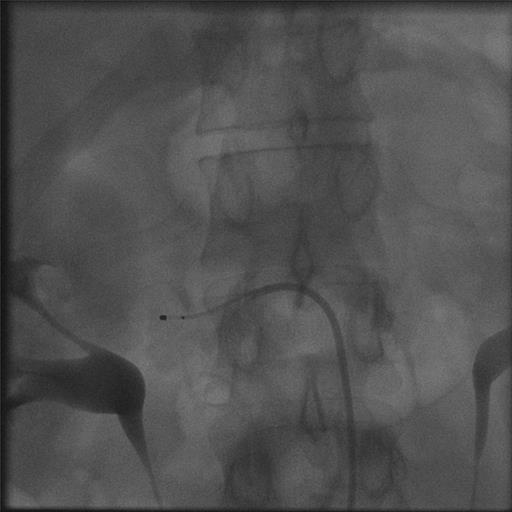
34 5 mm 12 mm Flexible Tip (selforienting) Deflectable Shaft





35 Spacing of e.g. 5 mm. Renal artery access via standard interventional technique 4-6 two-minute treatments per artery Proprietary RF generator Automated Low power Built-in safety algorithms 35
36
37

38
 Presentation; Ormiston et al. EuroIntv. 2013. The ReCor Device, Weil, TRENDS Frankfurt 2013; Sievert, Live Case, TRENDS, Frankfort 2013; LINC 2013, Live Case ReCor; J&J Thermocool Bertog, TRENDS Frankfurt 2013.")
39 (Some) RF Based RDN Technologies Medtronic Website, March 2013; The New Medtronic Device, Weil, TRENDS Frankfurt 2013; St. Jude Website, May 2013; Papademetriou, TRENDS Frankfort 2013; Covidien (Maya) Presentation; Ormiston et al. EuroIntv The ReCor Device, Weil, TRENDS Frankfurt 2013; Sievert, Live Case, TRENDS, Frankfort 2013; LINC 2013, Live Case ReCor; J&J Thermocool Bertog, TRENDS Frankfurt 2013.
 Series of Pilot Studies (EU, US & AU) Symplicity HTN-1 Symplicity HTN-2")
 Expand HTN Indication (Approved Regions) Pilot Studies in New Indications (Approved Regions)")
40 Comprehensive SYMPLICITY Clinical Trial Program will follow over 5000 patients across multiple indications First-in-Man (AU) Series of Pilot Studies (EU, US & AU) Symplicity HTN-1 Symplicity HTN-2 Initial RCT (EU & AU) SYMPLICITY HTN- 3 US Pivotal Trial (US) Global SYMPLICITY Registry (Approved Regions) Expand HTN Indication (Approved Regions) Pilot Studies in New Indications (Approved Regions) Trials under way

 - 12-month")
 -24-month follow-up Symplicity HTN-1 Investigators.")
41 Lancet. 2009;373: Hypertension. 2011;57: Initial Cohort Reported in the Lancet, 2009: -First-in-man, non-randomized -Cohort of 45 patients with resistant HTN (SBP 160 mmhg on 3 anti-htn drugs, including a diuretic; egfr 45 ml/min) - 12-month data \ Expanded Cohort This Report (Symplicity HTN-1): -Expanded cohort of patients (n=153) -24-month follow-up Symplicity HTN-1 Investigators. Hypertension. 2011;57:
42 Demographics Age (years) 57 ± 11 Gender (% female) 39% Race (% non-caucasian) 5% Co-morbidities Diabetes Mellitus II (%) 31% CAD (%) 22% Hyperlipidemia (%) 68% egfr (ml/min/1.73m 2 ) 83 ± 20 Blood Pressure Baseline BP (mmhg) 176/98 ± 17/15 Number of anti-htn meds (mean) 5.1 ± 1.4 Diuretic (%) 95% Aldosterone blocker(%) 22% ACE/ARB (%) 91% Direct Renin Inhibitor 14% Beta-blocker (%) 82% Calcium channel blocker (%) 75% Centrally acting sympatholytic (%) 33% Vasodilator (%) 19% Alpha-1 blocker 19% Symplicity HTN-1 Investigators. Hypertension. 2011;57:
43 38 minute median procedure time Average of 4 ablations per artery Intravenous narcotics & sedatives used to manage pain during delivery of RF energy No catheter or generator malfunctions No major complications Minor complications 4/153: 1 renal artery dissection during catheter delivery (prior to RF energy), no sequelae 3 access site complications, treated without further sequelae Symplicity HTN-1 Investigators. Hypertension. 2011;57:
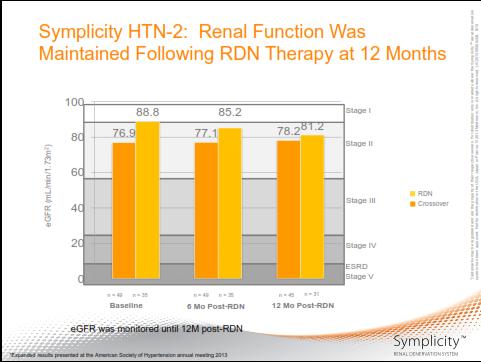
44 81 patients with 6-month renal CTA, MRA, or Duplex No vascular abnormalities at any site of RF delivery One progression of a pre-existing stenosis unrelated to RF treatment (stented without further sequelae) Two deaths within the follow-up period; both unrelated to the device or therapy No orthostatic or electrolyte disturbances No change in renal function at one year ( egfr) 12 Months: -2.9 ml/min/1.73m 2 (n.s.) (n=64) Symplicity HTN-1 Investigators. Hypertension. 2011;57:
45
46
47

48 Lancet. 2010;376: Purpose: To demonstrate the effectiveness of catheter-based renal denervation for reducing blood pressure in patients with uncontrolled hypertension in a prospective, randomized, controlled, clinical trial Patients: 106 patients randomized 1:1 to treatment with renal denervation vs. control Clinical Sites: 24 centers in Europe, Australia, & New Zealand (67% were designated hypertension centers of excellence) Symplicity HTN-2 Investigators. Lancet. 2010;376:
49 Inclusion Criteria: Office SBP 160 mmhg ( 150 mmhg with type II diabetes mellitus) Stable drug regimen of 3+ more anti-htn medications Age years Exclusion Criteria: Hemodynamically or anatomically significant renal artery abnormalities or prior renal artery intervention egfr < 45 ml/min/1.73m 2 (MDRD formula) Type 1 diabetes mellitus Contraindication to MRI Stenotic valvular heart disease for which reduction of BP would be hazardous MI, unstable angina, or CVA in the prior 6 months Symplicity HTN-2 Investigators. Lancet. 2010;376:
50 Assessed for Eligibility (n=190) Screening Excluded Prior to Randomization (n=84) BP<160 after 2-weeks of compliance confirmation (n=36; 19%) Ineligible anatomy (n=30; 16%) Declined participation (n=10; 5%) Other exclusion criteria discovered after consent (n=8; 4%) Randomized (n=106) Allocation Allocated to RDN (n=52) Allocated to Control (n = 54) Follow-up No Six-Month Primary Endpoint Visit (n = 3) Reasons: Withdrew consent (n=1) Missed visit (n=2) No Six-Month Primary Endpoint Visit (n = 3) Reasons: Withdrew consent (n=2) Lost to follow-up (n=1) Analysis Analyzed (n = 49) Analyzed (n = 51) Symplicity HTN-2 Investigators. Lancet. 2010;376:
51 RDN (n=52) Control (n=54) p-value Baseline Systolic BP (mmhg) 178 ± ± Baseline Diastolic BP (mmhg) 97 ± ± Age 58 ± ± Gender (% female) 35% 50% 0.12 Race (% Caucasian) 98% 96% >0.99 BMI (kg/m 2 ) 31 ± 5 31 ± Type 2 diabetes 40% 28% 0.22 Coronary Artery Disease 19% 7% 0.09 Hypercholesterolemia 52% 52% >0.99 egfr (MDRD, ml/min/1.73m 2 ) 77 ± ± egfr (% patients) 21% 11% 0.19 Serum Creatinine (mg/dl) 1.0 ± ± Urine Alb/Creat Ratio (mg/g) 128 ± ± Cystatin C (mg/l) 0.9 ± ± Heart rate (bpm) 75 ± ± n=42 for RDN and n=43 for Control, Wilcoxon rank-sum test for two independent samples used for between-group comparisons of UACR n=39 for RDN and n=42 for Control Symplicity HTN-2 Investigators. Lancet. 2010;376:
52 RDN (n=52) Control (n=54) p-value Number Anti-HTN medications 5.2 ± ± % patients on HTN meds >5 years 71% 78% 0.51 % percent patients on 5 medications 67% 57% 0.32 % patients on drug class: ACEi/ARB 96% 94% >0.99 Direct renin inhibitor 15% 19% 0.80 Beta-adrenergic blocker 83% 69% 0.12 Calcium channel blocker 79% 83% 0.62 Diuretic 89% 91% 0.76 Aldosterone antagonist 17% 17% >0.99 Vasodilator 15% 17% >0.99 Alpha-1 adrenergic blocker 33% 19% 0.12 Centrally acting sympatholytic 52% 52% >0.99 Symplicity HTN-2 Investigators. Lancet. 2010;376:
53 from Baseline to 6 Months (mmhg) RDN (n=49) Systolic Diastolic Control (n=51) 1 0 Systolic Diastolic 33/11 mmhg difference between RDN and Control (p<0.0001) 84% of RDN patients had 10 mmhg reduction in SBP 10% of RDN patients had no reduction in SBP Symplicity HTN-2 Investigators. Lancet. 2010;376:
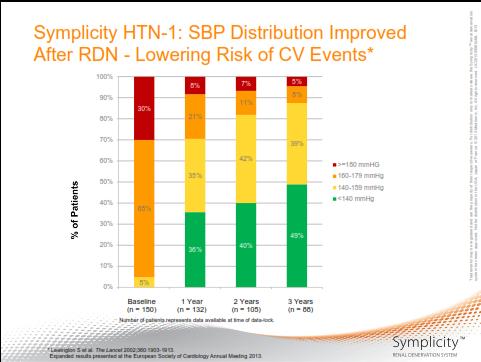
54 39% 6% 12% 35% 45% 180 mmhg mmhg mmhg 43% < 140 mmhg 51% 61% 31% 39% 18% 10% 4% 6% RDN Baseline RDN 6 Months Control Baseline Control 6 Months Symplicity HTN-2 Investigators. Lancet. 2010;376:
55 Home BP BP Change Change (mmhg) (mmhg) RDN (n=32) -20 Systolic 24-h ABPM: Analysis on technically sufficient (>70% of readings) paired baseline and 6-month RDN (n=20): -11/-7 mmhg (SD 15/11; p=0.006 SBP change, p=0.014 for DBP change) Control (n=25): -3/ -1 mmhg (SD 19/12; p=0.51 for systolic, p=0.75 for diastolic) -12 Diastolic Control (n=40) 2 0 Systolic Diastolic Symplicity HTN-2 Investigators. Lancet. 2010;376:
56 No serious device or procedure related adverse events (n=52) Minor adverse events 1 femoral artery pseudoaneurysm treated with manual compression 1 post-procedural drop in BP resulting in a reduction in medication 1 urinary tract infection 1 prolonged hospitalization for evaluation of paraesthesias 1 back pain treated with pain medications & resolved after one month 6-month renal imaging (n=43) No vascular abnormality at any RF treatment site 1 MRA indicates possible progression of a pre-existing stenosis unrelated to RF treatment (no further therapy warranted) Symplicity HTN-2 Investigators. Lancet. 2010;376:
57 Catheter-based renal denervation, done in a multicentre, randomised trial in patients with treatment-resistant essential hypertension, resulted in significant reductions in BP. The magnitude of BP reduction can be predicted to affect the development of hypertension-related diseases and mortality The technique was applied without major complications. This therapeutic innovation, based on the described neural pathophysiology of essential hypertension, affirms the crucial relevance of renal nerves in the maintenance of BP in patients with hypertension. Catheter-based renal denervation is beneficial for patients with treatment-resistant essential hypertension. Symplicity HTN-2 Investigators. Lancet. 2010;376:
58
59

60
61
62





63 EnligHTN OneShot Vessix Symplicity Symplicity Krum, H. ESC, 2013; Esler, M. ASH, 2013; Worthley, SG. EuroPCR, Ormiston, J. EuroPCR, 2013; Schofer, J. PCR, 2013;
64 Study Design Multi-center, prospective, blinded, randomized controlled trial Study Objective To demonstrate that catheter-based renal denervation is a safe and effective treatment for uncontrolled hypertension Study Population Uncontrolled hypertension population SBP 160 mmhg despite maximally tolerated doses of 3 antihypertensive medication classes Without significant renal impairment (egfr > 45mL/min) 530 randomized subjects at 60 sites Randomization (2:1) All patients maintained on baseline meds for 6 months
65 2:1 randomization Sham procedure in control patients that included renal angiogram 535 subjects randomized Rigorous screening process Initial Screening Office SBP 160 mmhg Full tolerated doses of 3 meds No HTN med changes in past 2 weeks No plan to change meds for 6 M Medical Hx 2 weeks Home BP & Med Confirmation Confirmatory Screening Office SBP 160 mmhg Documented compliance on meds Lab work 24 hr ABPM SBP 135 Control Renal Angiogram If eligible anatomy, randomize on the table 1M 3M 2 weeks Home BP & Med Confirmation 2 weeks 6M Primary Endpoint 30 days or maximum 6 weeks in exceptional circumstances Treatment 1M 3M Home BP & Med Confirmation 6M 12-60M Primary Efficacy Endpoint: Change in Office Systolic Blood Pressure Primary Safety Endpoint: MAE through 1 month, including Renal Artery Stenosis within 6m Patient and Research staff performing 1, 3 & 6 month follow-ups are blinded to treatment status No changes in medications for 6M
66 Patient Disposition 1441 subjects assessed for eligibility 535 subjects randomized Excluded: 880 not eligible for randomization 26 eligible but not randomized because randomization cap was reached 364 subjects randomly allocated to renal denervation 2:1 171 subjects randomly allocated to sham control 2 subjects died 1 subject withdrew 11 missed 6-month visit 1 subject died 1 missed 6-month visit 350 (96.2%) subjects with 6 month follow-up 169 (98.8%) subjects with 6 month follow-up
67 Safety analysis Composite endpoint of death, renal injury, vascular complications, and embolic tissue injury to 1 month and renal artery stenosis to 6 months. <7% MAE rate required to meet the primary safety endpoint. Primary safety analysis A performance goal established from renal artery stenting required the major adverse event rate for safety be <9.8%. This requires the observed MAE rate to be <7%, given the expected confidence interval for this endpoint.
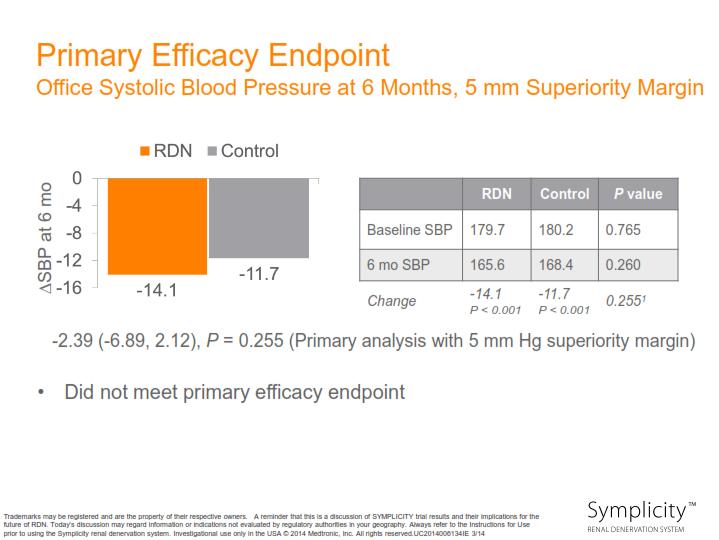
68 Efficacy analysis Comparison of SBP change from baseline to 6 mo in RDN arm compared with change from baseline to 6 mo in control arm Endpoint = (SBP RDN 6 mo SBP RDN baseline ) (SBP CTL: 6 mo SBP CTL baseline ) Primary efficacy (OBP) endpoint assumptions Superiority analysis Superiority margin of 5 mm Hg, per FDA recommendation Assuming a standard deviation of 25 mm Hg for both arms, 10 mm Hg is the minimum treatment difference required to meet the efficacy endpoint (95% CI) Secondary efficacy (ABPM) endpoint assumptions Superiority analysis Superiority margin of 2 mm Hg, per FDA recommendation Assuming a standard deviation of 18 for both arms, 5.5 mm Hg is the minimum difference required to meet the efficacy endpoint (95% CI)

69 Illustrative examples of endpoint scenarios, either meeting or not meeting the set assumptions for the primary endpoint hypothetical example-not actual trial data Meets Endpoint Does Not Meet Endpoint Relative Drop in Office Systolic Blood Pressure Between Treatment and Control Does Not Meet Endpoint Does Not Meet Endpoint 0 mm Hg

70 January 9 th, 2014 Primary efficacy endpoint was not met Primary safety endpoint was met
71 Major Adverse Event (MAE) Rate 10% Performance Goal = 9.8% 8% 6% P < % 2% 0% 1.4% Safety Measures Renal Denervation (N = 364) Sham Procedure (N = 171) Difference (95% CI) P MAE 1.4% (5/361) 0.6% (1/171) 0.8% (-0.9%, 2.5%) 0.67
72
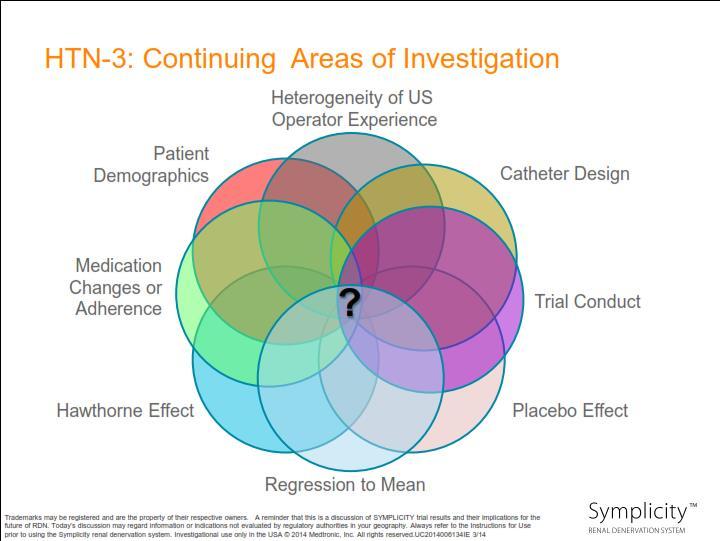
73 Patient behavior Due to being enrolled and closely monitored in a clinical trial, as well as blinded to treatment, the patients in SYMPLICITY HTN-3 may have improved or modified their lifestyle and drug adherence. Study population The population studied and the requirement for maximum tolerated medication dosage were different from other SYMPLICITY studies. Procedural experience and variability SYMPLICITY HTN-3 included a greater number of trial sites and proceduralists compared to SYMPLICITY HTN-1 and HTN-2, which may have led to greater procedural variability. Case proctoring was different and not comparable

74 Procedural Variability Correlation with # of ablations Correlation with 4-quadrant ablation pattern Cross-section of artery Inferior Anterior Superior Posterio r Lesion 4 quadrant ablation pattern

75 Impact of Number of Ablations on Change in Office SBP: Matched Cohort Analysis N= P value for trend= 0.01 Denervation Sham Baseline SBP % CI P* -1.7(-7.1, 3.7) (-8.6, 2.4) (-11.3, 0.5) (-13.9,-0.3) (-17.4, 0.7) (-21.8,-1.2) (-28.8, 0.7) (-30.0, 5.9) (-44.6, 19.8) 0.43 Propensity scores using baseline characteristics as covariates were used to match sham control and denervation patients *P value change in SBP for RDN compared with sham Data presented are mean (SD)
76 Impact of Number of Ablations on Change in Ambulatory SBP: Matched Cohort Analysis N= P value for trend= Denervation Sham Baseline SBP % CI P* -1.4(-5.1, 2.3) (-5.7, 1.9) (-8.0, 0.2) (-9.6,-0.04) < (-13.7, -3.1) (-14.6, -1.5) (-16.4, 2.7) (-20.6, 5.1) (-37.1, 7.0) 0.17 *P value change in SBP for RDN compared with sham Data presented are mean (SD)
77
78 SYMPLICITY HTN-3 did not reach the primary or powered secondary efficacy endpoints in this trial. There may be many factors that contributed to the outcome, which we continue to investigate. SYMPLICITY HTN-3 did meet its safety endpoint, which is consistent with all other Symplicity trials, including the Global SYMPLICITY Registry. Based upon our detailed analysis of HTN-3, we believe further clinical investigation is warranted and Medtronic will, in consultation with FDA, pursue a new IDE trial An unmet need in this uncontrolled hypertension population still exists. Medtronic will continue to provide access to the Symplicity system in countries where it has regulatory approval and will continue to support a global hypertension clinical program
79 PLEIOTROPIC EFFECTS
80 Aggravation of hypertension Progression of renal disease Trophic effects (LVH) Heart failure HIGH CARDIOVASCULAR MORTALITY Cardiac arrhythmias (SCD) Adverse metabolic effects

81
82 Conclusions: Renal denervation improves glucose metabolism and insulin sensitivity in addition to a significantly reducing blood pressure. However, this improvement appeared to be unrelated to changes in drug treatment. This novel procedure may therefore provide protection in patients with resistant hypertension and metabolic disorders at high cardiovascular risk. Mahfoud F et al. Circulation. 2011; 123:
83 SNS activity in multiple diseases Kidney Failure 1,2 Sleep Apnea 2,3 Heart Failure 1,2 Diabetes 2,3 Obesity 2,3 1. Schlaich MP, et al. Hypertension. 2009;54: Izzo JL, Black HR, Sica DA, eds. Hypertension Primer. 4th ed Tsioufis C, et al. Int J Hypertens. 2011:
84
85 Is BP a sensitive marker of RDN technical success? Are there patient subtypes where BP response is unlikely? Are there patient subtypes where BP response is delayed (e.g. is the time course of some benefit different amongst patient types)? Is the only benefit of reduction of renal neurologic signaling BP reduction If there are other exploitable clinical benefits, then using BP as the sole identifier of technical success is inappropriate
86 Efferent Denervation Renal Specific Metrics Activity of the RAA system Renal Salt Renal Vascular Resistance Markers of Renal Neuro Activity Renal NA Spillover Afferent Denervation Systemic Sympathetic State Total Body NA Spillover Change of Sympathetic state of down stream organs Peripheral Microneurography HRV HR (?) Euglycemic insulin Clamp; HOMA index Renal Afferent Nerve or systemic response to infusion of renal chemosensitive agents
87 ECG Repolarization Improvements ECG Voltage Regression LV Mass Regression MRI LVH Renal Metrics Improvment of egfr Reduction of population progressing to ESRD Vascular Metrics Analogous to the lipid intervention trials
88 Relatively small numbers of patients in trials Small trials tend to overestimate treatment effects Small trials tend to underestimate side effects Rare side effects (?renal artery stenosis) missed? No systematic imaging for renal artery stenosis Generalizeable to broader patient populations? Applicable to African patients with HTN? Generalizeable to other operators? Limited number of patients with long-term follow-up Durability of effect
89 Methodological limitations Not all patients on a diuretic. Low utilization of aldosterone blockade No ABPM to screen out white coat hypertension No rigorous assurance of compliance

90 10 year old boy Severe resistant hypertension despite numerous agents Autosomal Recessive Polycystic Kidney Disease Creat 130mcmol/L Multiple renal arteries Small caliber aorta / renal vessels Risk of Contrast-induced Nephropathy Paediatric case Complex consent / ethical / legal issues
91 Felodipine 10mg mane Nifedipine 10 mg BD Atenolol 75mg mane, 50mg nocte Prazosin 5mg tds Hydralazine 25 mg BD Furosemide 40 mg daily Aspirin 100 mg alternate days Phenytoin 75 mg BD, 50mg midday Zonisamide 100 mg bd Neulactil 2.5 mg nocte Lamotrigine 200 mg bd Clobazam 10 mg bd Modafinil 200 mg BD Strattera 35 mg mane Amitriptyline 50mg nocte Ferro liquid 7 mls BD Aranesp 40 ug twice weekly NaHCO3 i BD Ostelin 1 tablet midday


92 Vessix Renal Denervation Balloon-based technology (4-7 mm diameters) Helical pattern of bipolar radiofrequency electrodes for uniform treatment 30 second treatment time All electrodes activated simultaneously System Technology Overview Bipolar energy delivery, ~1 Watt Temperature-controlled algorithm ensures energy delivery at 68 C One button operation CE-marked and TGA-approved Vessix is an investigational device and not available for sale in the US. RF=Radiofrequency; TGA=Therapeutic Goods Administration, AU Regulatory Authority
93 At Baseline: Home BP >200/100 mmhg not uncommon 24hr ABPM = average daytime BP 154/89 mmhg At 3-months no home SBP > 180 mmhg At 6-months no home SBP > 160 mmhg At 12-months no home SBP > 140 mmhg 24hr ABPM = average daytime BP 129/69 mmhg No seizures since 6-months Dramatic reduction in poly-pharmacy Markedly improved academic performance / behaviour
94 Transcatheter renal denervation offers a safe and effective therapeutic option in the treatment of resistant hypertension However, many questions remain to be answered long-term safety data absolute benefits on cardiovascular mortality cost-effectiveness de-escalation of antihypertensive drugs efferent sympathetic regrowth
95 Although renal denervation might prove to be revolutionary in the treatment of hypertension, the complexity of its pathophysiology discourages the simplistic notion that inhibition of one factor will be effective in all patients, over-optimism should be avoided. SIMPLICITY 3 TRIAL has resulted in a reality check and shifted focus into identifying predictors that will determine which patients will respond to this therapy. However, the exciting results of the recent renal denervation studies have generated great expectation, the investigators have paved the way for interventional management of patients with resistant HPT
96 Thank you for your attention
97
98
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Disclosures for Dr. Bhatt
 Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
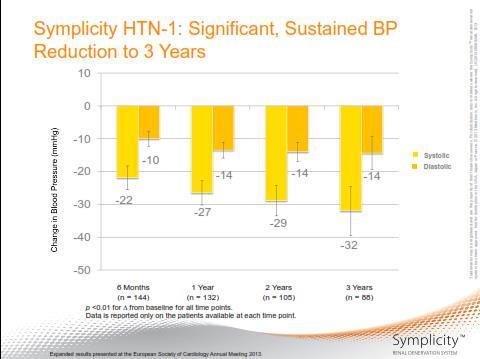
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1
 Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Renal denervation for treatment of resistant hypertension
 Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Autumn Meeting Birmingham. Renal Denervation
 Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Autumn Meeting Birmingham Renal Denervation Andreas Baumbach, MD, FRCP, FESC Consultant Cardiologist, hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol Renal Denervation BACKGROUND
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Renal sympathetic denervation as a potential treatment for hypertension
 Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Renal Denervation. Henry Krum MBBS PhD FRACP. Centre of Cardiovascular Research & Monash University/Alfred Hospital;
 Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Renal Denervation Henry Krum MBBS PhD FRACP Centre of Cardiovascular Research & Education in Therapeutics, Monash University/Alfred Hospital; Alfred Heart Centre, The Alfred Hospital, Melbourne Australia
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial
 Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
Renal Sympathetic Denervation for Treatment of Resistant Hypertension: 18-Month Results from the Symplicity HTN-2 Randomized Controlled Trial Prof Murray Esler Baker IDI Heart and Diabetes Institute, Melbourne
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Transcatheter Renal Denervation and Hong Kong Experience
 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction?
 Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Evidence of Baroreflex Activation Therapy s Mechanism of Action
 Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Transcatheter Perivascular Alcohol- Mediated Renal Denervation
 Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Phase 3 investigation of aprocitentan for resistant hypertension management. Investor Webcast June 2018
 Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Nurse-sensitive factors in hypertension management
 Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Ambulatory Blood Pressure Measurement. Objectives of the Presentation. Methods of Measuring BP: Pros and Cons
 Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Renal Sympathetic Denervation in the Treatment of Resistant Hypertension: Current Clinical Evidence, Patient Selection, Tips and Tricks
 Renal Sympathetic Denervation in the Treatment of Resistant Hypertension: Current Clinical Evidence, Patient Selection, Tips and Tricks Kostadin Kichukov, MD, PhD, Iskren Garvanski MD, Department cardiology,
Renal Sympathetic Denervation in the Treatment of Resistant Hypertension: Current Clinical Evidence, Patient Selection, Tips and Tricks Kostadin Kichukov, MD, PhD, Iskren Garvanski MD, Department cardiology,
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been