Renal Sympathetic Denervation in the Treatment of Resistant Hypertension: Current Clinical Evidence, Patient Selection, Tips and Tricks
|
|
|
- Anthony Price
- 6 years ago
- Views:
Transcription

1 Renal Sympathetic Denervation in the Treatment of Resistant Hypertension: Current Clinical Evidence, Patient Selection, Tips and Tricks Kostadin Kichukov, MD, PhD, Iskren Garvanski MD, Department cardiology, angiology and electrophysiology City Clinic - Sofia

2 In 2014 everyone knows what renal denervation is Symplicity HTN 2
3 Uncontrolled Hypertension is not equal to Resistant Hypertension! What we have to look for? White coat hypertension Secondary hypertension Inaccurate measurement Inappropriate drug combinations Interfering substances Non compliance with drug regimen or lifestyle modification Sleep apnoea

4 Real life data Utrecht registry. Referral for RDN 66% dropouts. Why? Blankestijn, P. J. RHC 2013
5 From theory to practice Symplicity (Medtronic Ardian)




6 Renal Denervation Technologies BSC Vessix MDT Symplicity MDT Spyral STJ EnligHTN COV OneShot ReCor Gen 2 Paradise JNJ ThermoCo ol CE Mark Catheter Design Balloon catheter 4 8 electrodes Catheter with single electrode Pigtail Catheter 4 electrodes Basket with four electrodes Balloon catheter helical electrode and cooling Balloon catheter; internal cooling; Circumferential treatment Pigtail catheter with 5 electrodes and cooling Balloon No No No No Guidewire No No No Energy Bipolar RF Monopolar RF Monopolar RF Monopolar RF Monopolar RF Ultrasound Monopolar RF Power ~1W 8W 8W 6W 25W ~12W 15W Energy Delivery Time Total Treatment Time 30 sec. 2 min. 1 min. 90 sec 2 min. 30 sec. Unknown 2 min min. 2 min. 24 min. 4 min. 3 min. Unknown None of these devices are available for sale in the US. Medtronic Website, March 2013; The New Medtronic Device, Weil, TRENDS Frankfurt 2013; St. Jude Website, May 2013; Papademetriou, TRENDS Frankfort 2013; Covidien (Maya) Presentation; Ormiston et al. EuroIntv The ReCor Device, Weil, TRENDS Frankfurt 2013; Sievert, Live Case, TRENDS, Frankfort 2013; LINC 2013, Live Case ReCor; J&J Thermocool Bertog, TRENDS Frankfurt RF=Radiofrequency; W=Watt

 3 Month (n=44) OneShot 6 Month (n=47)")



7 RF Energy Devices Consistent Data EnligHTN Change in Office Blood Pressure Month (n=47) 3 Month (n=44) OneShot 6 Month (n=47) SBP DBP Vessix Symplicity HTN 2 RCT p < p = /7 mm Hg n=49 n=47 n=43 n=40 Symplicity Symplicity Symplicity Spyral Krum, H. ESC, 2013; Esler, M. ASH, 2013; Worthley, SG. PCR, Whitbourn R. PCR 2013; Ormiston, J. PCR, 2013; Schofer, J. PCR, 2013 Verheye S, TCT 2013
 Kona: External Ultrasound Wave 1 study -10 mm Hg 0,0-20 mm")

 0 5 10 15 20 25 30 35 6 9 9 12 16 22 22 29 External ultrasound energy delivered to renal")

8 Ultrasound Energy Devices Just the same 0 mm Hg Recor Study: Office Blood Pressure Cardiosonic TIVUS ABPM 3 Month Follow up (n=10) Kona: External Ultrasound Wave 1 study -10 mm Hg 0,0-20 mm Hg -30 mm Hg -40 mm Hg -50 mm Hg Systolic Diastolic BP Mm Hg 5,0 10,0 15,0 20,0 25,0 Systolic Diastolic 11,9 11,8 11,2 23,1 22,2 22,6 24 Hr ABPM Day ABPM Night ABPM Non Focused, High Intensity Ultrasonic Catheter Change from Baseline (mm Hg) External ultrasound energy delivered to renal nerves Ultrasound tranducer inside 6 F balloon Ultrasound creates heat Cooled water in the balloon to protect None of these devices are available for sale in the US. Whitbourn R, WAVE 1; PCR 2013

9 SYMPLICITY HTN 3 Complicated the future of renal denervation. All onging similar trials were stopped. WHY?
10 Still we have only assumptions But look at Eurointervention Vol.9 Num.9! we need to wait until the peer-reviewed publication of clinical data, most likely around the end of March 2014, to have further information rather than speculating on a technical level, the cannulation of the catheter is relatively straightforward, however, the renal nerves are widely distributed and perhaps catheter orientation issues appeared. As in all new therapies, a learning curve exists, perhaps this was a contributing factor. The majority of the first studies, and the Symplicity HTN-1 and 2, were performed at selected sites in Europe and Australia, whereas the Symplicity HTN-3 trial was performed at selected sites in the United States and Australia. Patrick W. Serruys, Editor in Chief EuroIntervention
11 Still we have only assumptions, but look at Eurointervention Vol.9 Num.9! Despite the strict inclusion/exclusion criteria in HTN-3, did the patients truly have resistant hypertension? How did the investigators confirm medication adherence when a recent publication recently reported that 43 to 65.5% of patients with presumed resistant hypertension are nonadherent? Was the HTN-3 primary efficacy endpoint of a 10 mmhg systolic pressure difference between the two groups overly ambitious? Some experts explain that a long-term sustainable 5 mmhg decrease in systolic pressure is still beneficial for the patient group, suggesting that this decrease is the equivalent of adding one additional tablet. Is the outcome of Symplicity HTN-3 related to the first generation device that has been used? What about the other investigational devices with different design and energy sources? Patrick W. Serruys, Editor in Chief EuroIntervention
12 Renal denervation success is not in the believing, but in doing it right The non-responder hypotheses emerged nearly an year ago
13 A Non responding patient Hypothesis 1 for Non Response The Patient You did a good technical but clinically ineffective job because in some patients: Overactivation of sympathetic system trough the kidneys is not involved in the pathophysiology of resistant hypertension Anatomical variations of the splanchnic sympathetic fibers are able to bypass the renal plexus through other circuits (independently of vascularization) Masked presence of multiple renal arteries is able to maintain some sympathetic connections despite main renal artery denervation
14 A Non responding patient Hypothesis 2 for Non Response The Technique You did an ineffective job because you don t know the temperature at the adventitia/nerves level and in some patients : Atheromatous disease and renal artery thickness are limiting temperature rise/transduction A significant proportion of nerves are at more than 4 mm from the intima which distance may be out of the efficacy perimeter of the electrode Some surrounding anatomical structures (renal veins, IVC) may limit temperature rise / transduction
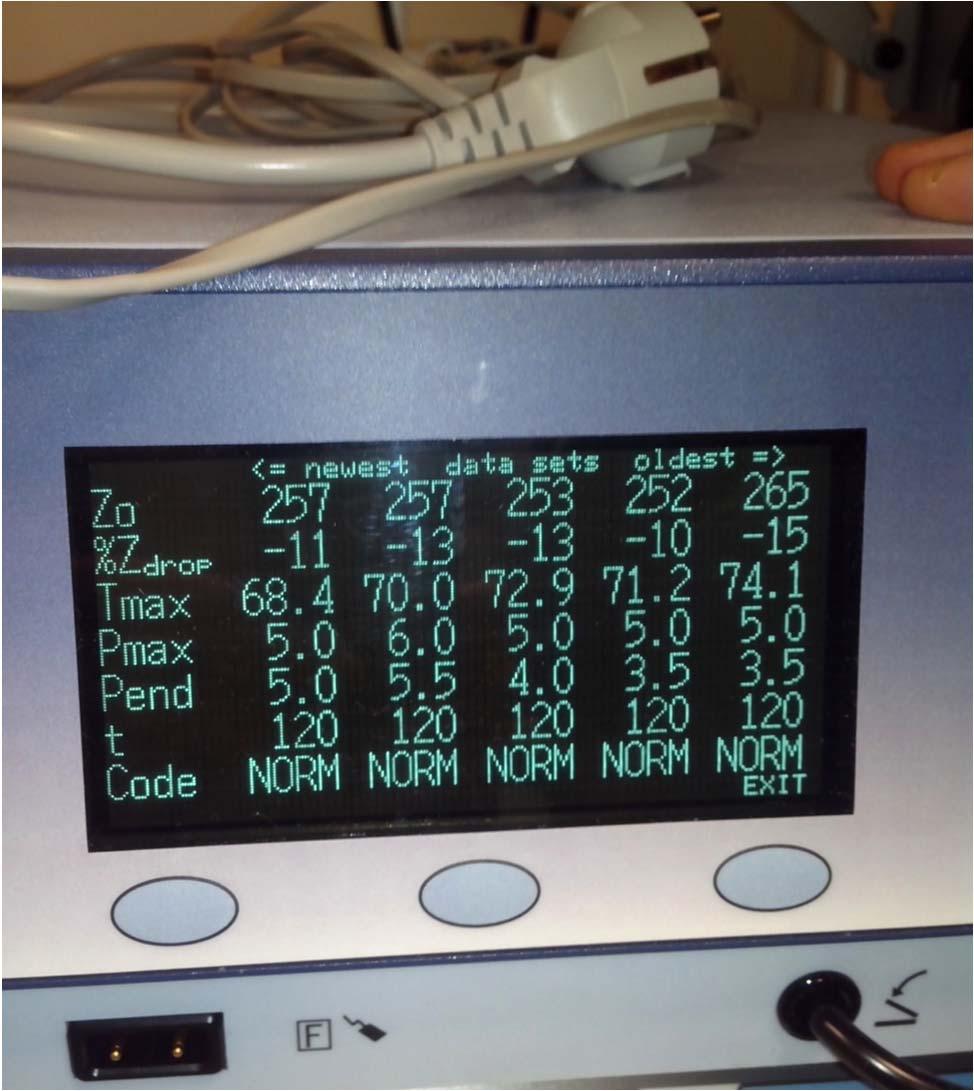
15 A Non responding patient Hypothesis 3 for Non Response The Doctor You did an ineffective job because you don t follow current recommendations of use of the device : Diameter/lenght of the target vessels Inappropriate value of impedance (tissue contact) To limited number of ablations (only 4) per artery or unilateral procedure Inappropriate duration of ablation (repeated automatic interruption from generator for technical reasons) Inappropriate anticoagulation (fibrin deposit) Other mistakes
")
16 Vascular Safety? Prospective observational study, 32 renal arteries of patients with treatment-resistant hypertension underwent OCT pre & post RDN Vasospasm in 10 renal arteries (42%) after RDN (no vasospasm before the procedure) (P < 0.001) Await Similar studies with other RF & balloon based technologies Templin C et al, Eur Heart J 2013

 Templin C et al, Eur")
17 Intraluminal thrombus formation from 18% to 67% EnligHTN multi-electrode induces a different tissue response (with a higher amount of thrombus formation measured by OCT per renal artery than the Simplicity catheter) Templin C et al, Eur Heart J 2013
18 Pioneers in Bulgaria Ivo Petrov MD, PhD and team: Kostadin Kichukov MD, PhD Christo Dimitrov, MD Lora Nikolova, MD Currently three active RDN centres in Bulgaria City Clinic, Lozenetz, Sv. Anna (Pat. N>100) All treated with Symplicity system
19 Patient Selection o Office SBP 160 mmhg ( 150 mmhg with type II diabetes mellitus) o ABPM above thresholds for day/night; 24H BP o Stable drug regimen of 3+ more anti-htn medications o Age >18 years o Suitable renal vessels - Length>20mm, Diameter>4mm. o Without hemodynamically or anatomically significant renal artery abnormalities or prior renal artery intervention o egfr > 45 ml/min/1.73m 2 (MDRD formula)
20 Renal denervation is not a procedure it is a program Started on March 15, 2012 (FIB) patients urdergone the procedure patients up to All procedures performed with the Medtronic Symplicity system A dedicated team for patient management
21 PRE PROCEDURE AND IN HOSPITAL ASSESSMENT All patients are well KNOWN with initial ABPM readings 100%. Clinical physical exam ECG EchoCG Doppler ultrasound of renal arteries Baseline laboratory panel Careful observation (BP) after procedure Control doppler and creatinine before discharge
22 Follow up scheme? You need a team! Tailored for individual patient s needs, e.g. associated morbidities treated Control physical exams at M1, M3, M6, M12 Control ABPM M1, M3, M6, M12 Control Lab screa, suric Acid, sk, sna, Control cardiac Echo M12 Control Doppler of the renal arteries M1, M3.
23 PRE PROCEDURE ANTIHYPERTENSIVE TREATMENT Average number of drug classes 4,7 (3 7) % usage ACE I 34% ARB 66% CCB 71% Duiretic 100% Aldosterone antagonist 27% Centrally acting sympatholytics 57% DRI 11% Beta blockers 92% Alfa blockers 43%

24 Results over office BP City clinic data 180 P<0, SBP 80 DBP MO M1 M3 M6 P<0,05
25 Other variables during FU egfr Without significant change between BL, M01, M03, M06. o With 2 exclusions. 1 Pt with early CIN (72h), successfully treated. 1 patient with CKD had dialysis on the day of procedure and the day after. After that case all patients with ESRD have planned dialysis the same manner. o 2 patients had gradual deterioration of kindey function at M06 Consulted with nephrologist+biopsy (Both with DM type 2>15years). Dg: Diabetic Nephropathy. Heart Rate Without significant change between BL, M01, M03, M06 o Explanation: First type of medication withdrawn are usually centrally acting sympaticolytics Responder rate by the Symplicity HTN criteria: o At M03 67%, at M06 82%
26 Other variables during FU Antihypertensive Medication o Average No. of antihypertensive classes dropped from 4,7 (3-7) to 3,8 (2-6) at M03. There were exclusions. Exclusions o Three patients (6,81%) were non-responders ( 2 without any change in BP; 1 with insignificant elevation of BP. Two retreated after M06 one with good result. Off-Label Use o RDN in 4 patients with CKD on dialysis with malignant hypertension with perfect outcome during FU More than 25mm drop in SBP, 14mmDrop in DBP. Safe and sound! Responder vs non-responder o Up to now we do not have predictors of success. Optimal response in unilateral RDN vs poor response in bilateral x6-7.

27 We cautiously change therapy at Mo 3 following this advice Plouin, RHC 2013
28 The Renal Denervation Procedure Itself Data and tips from our Experience
29 INVASIVE PROCEDURE (1) Femoral / Brachial artery access 6/5 Fr Up to 08/02/14 5 patients had RDN via Brachial Renal angiogram o Absence of flow limiting stenoses o Diameter >4mm in target vessel o Length >20mm o Guide catheter selection RDC, IMA, MP o Areas to avoid Atherosclerosis, calcification, FMD
30 INVASIVE PROCEDURE (2) Remember Treat all suitable vessels! Never rely on 4 ablations per artery! Conscious sedation and analgesia o Midazolam uptitration to 5mg; Fentanyl up to 6ml o Tip: Lidocaine mg ia in the renal artery before/during ablation session Careful monitoring of pulse oxymetry Anticoagulation Heparine IU All patients pretreated with mg ASA
31 Procedure specific details City Clinic data (up to sep/2013) Renal ablation procedural details Procedural success 100% Procedure time 69±35 min X ray time 16 min Number of ablations per artery 5.8 Bilateral ablation 94,5% Combined with coronary intervention Combined with renal intervention Contrast volume 23% 6,8% 145 ± 67 ml GC used IMA RDC 2 Guiding sheath 5/6Fr Double GW use Telescopic technique 38% 58% 4% 18% 12%
32 Procedural safety City Clinic Data 73 patients treated Minor bleeding at puncture site - 2 pt 1 pt transient haematuria with on D1 with full resolution 3 pt with hypotension within hospital period 1 case of renal artery dissection, successfully stented No cases of renal artery blood flow compromise (assessed by doppler)during FU
33 Some brief clinical cases (If we still have time)


34 The Easy renal arteries Telescopic technique for accessory vessel/ FMD


35 The Easy Renal arteries Brachial approach could help (Guiding sheath 5F, MP Curve)
36 Case 1 KTK History (FIB) 53 YO Male History of severe uncontrolled hypertension since 2005 Dyslipidemia on statin therapy Hyperurikaemia Evidence of Target organ Damage: o LV Hypertrophy - ECG and Echo criteria o No evidence of angina at effort Drug regimen o Lercanidipine - 2x10mg o HCTZ - 25mg o Candesartan - 32mg o Metoprolol Succinate - 150mg o Doxazosine - 4mg o Moxonidine - 0,4mg

37 Case 1 KTK ABPM readings 09 10/03/2012
38 Case 1 KTK Clinical and lab findings 13/03/12 Physical exam - unremarkable; BP - 180/100 ECG - sinus rhythm, criteria for LVH Cardiac Echo: Preserved LV systolic function - EF-65% LVH - IVS/LVPW - 14/14mm; LVd Mass A-L 191g Impaired LV relaxation; E/e - 10,660 Peripheral Echo Doppler: No evidence of carotid, mesenteric or renal stenoses. Renal arteries - solitary bilaterally, with diameter 6mm, lenght >30mm. Lab - CrCl - 112,77ml/min

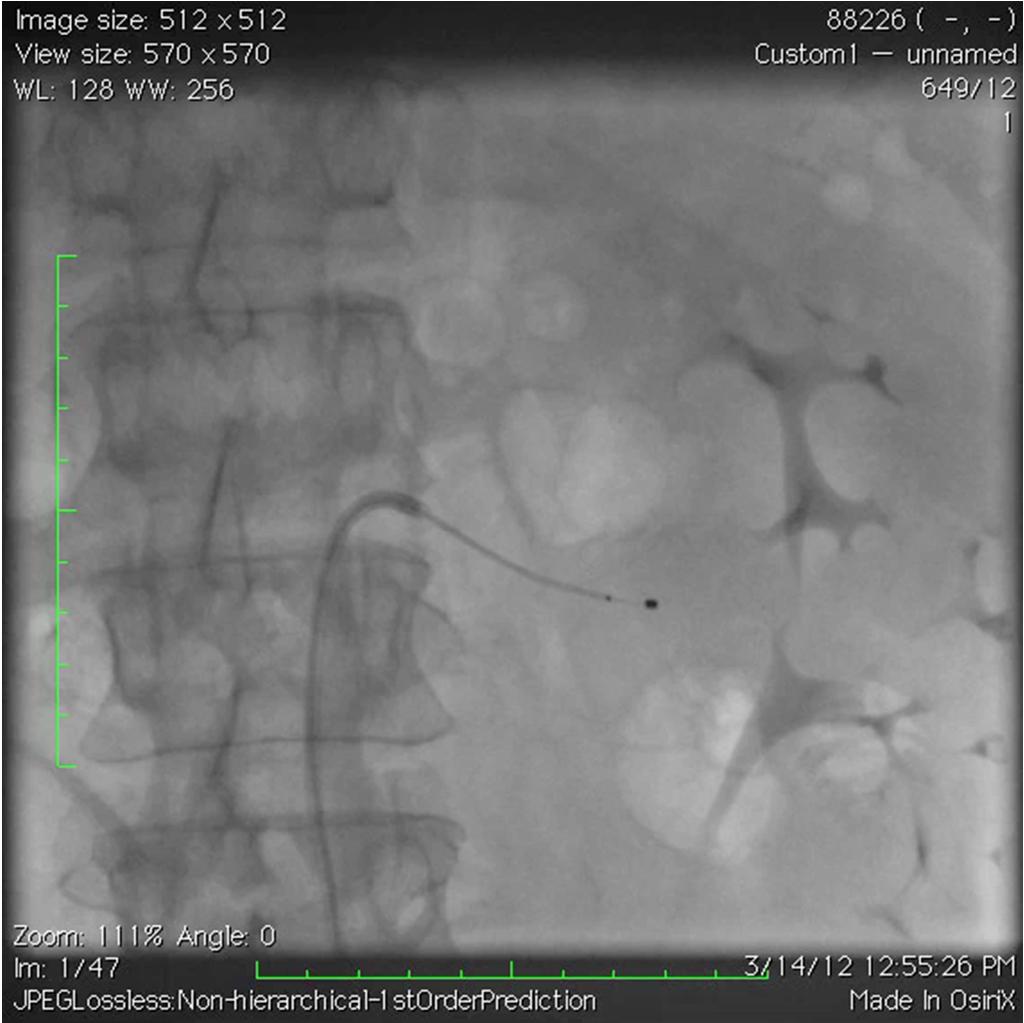
39 KTK Procedure

40 KTK 18M FU Lercanidipine - 2x10mg HCTZ - 25mg Candesartan - 32mg Metoprolol Succinate - 150mg Doxazosine - 4mg Moxonidine - 0,4mg
41 Expanding indications Heart failure LV Hypertrophy Sleep apnoea Insulin resistance Chronic kidney disease/esrd Atrial fibrillation
42 Case VPS History 62 YO Male History of severe uncontrolled hypertension since ESRD: on dialysis since SBP at home 260 systematically; during dialysis. Type 2 Diabetes since Hard evidence of Target organ Damage Drug regimen o o o o o Nifedipine - 6x10mg Zofenopril - 15mg Prazosine 4x2mg Moxonidine 2x0,4mg Clonidine up to 6x0,150mg
43 Case VPS Clinical and lab findings Physical exam HR - 53; BP 210/80 ECG - sinus rhythm, criteria for LVH Cardiac Echo: Preserved LV systolic function EF-73% LVH - IVS/LVPW - 17/15mm; Impaired LV relaxation; E/e 16,2 Peripheral Echo Doppler: No evidence of carotid, mesenteric or renal stenoses. Renal arteries - solitary bilaterally, with diameter 6mm, lenght >30mm. Lab Hb 114; Cr 457; NT-pro BNP > 35000

44 Case VPS Challenging, state of the art procedure
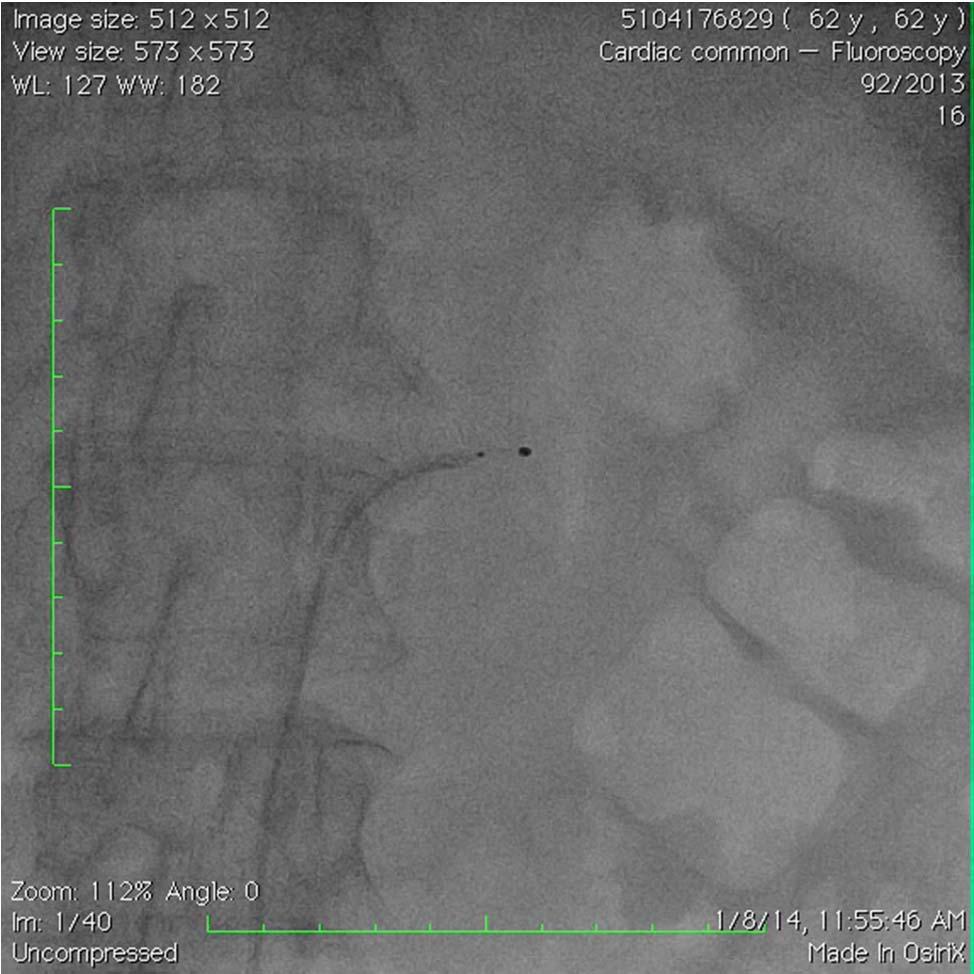
45 Case VPS Challenging, state of the art procedure

 Home BP Drop of SAP")
46 Case VPS Compelling evidence of effect on M01 Mean 24h SAP 196,4 178 (Drop 18,4) Mean 24h DAP 88,6 79 (Drop 9,6) Home BP Drop of SAP 40-50mm!
47 Take home messages Careful selection of candidates for RDN is essential Inform patients not to expect immediate results and be patient up to M06. But be prepared for immediate drops in BP! Expect results in most of the cases around M03 Never miss to control s Creatinine, e.g. GFR soon after procedure and during FU Try to keep BP-lowering therapy unchanged until M03, except in cases of hypotension. You never know who will be responder of the procedure, because we do not have reliable predictors of success. That s why do your best!
48 Thank you for your attention!
Devices and Long-Term Outcomes of Renal Denervation for Hypertension
 18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
18th ANGIOPLASTY SUMMIT-TCTAP 2013 Seoul, Korea, April 23-26, 2013 Devices and Long-Term Outcomes of Renal Denervation for Hypertension Horst Sievert, Ilona Hofmann, Laura Vaskelyte, Stefan Bertog, Simon
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Percutaneous Renal Denervation: A New Promise in the Treatment of RHT?
 BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
BAD KROZINGEN Prof. T. Zeller, MD Bad Krozingen, Germany Percutaneous Renal Denervation: A New Promise in the Treatment of RHT? Potential conflicts of interest Speaker s name: Thomas Zeller X I have the
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension
 EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
EnligHTN I, First-in-Human Multicenter Study of a Multi-Electrode Renal Denervation Catheter in Patients with Drug-Resistant Hypertension Vasilios Papademetriou, MD 1 Prof. Stephen Worthley, MD 2 Costas
Preliminary Results of RETREAT
 LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
LINC 2015 Leipzig, Germany, Jan 27-30, 2015 Preliminary Results of RETREAT (Renal Denervation with Ultrasound After Failed Radiofrequency Denervation) Horst Sievert, Jan Philipp Kulow, Stefan Bertog, Predrag
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Renal Denervation For Hypertension: Status Update
 Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
Samuel N. Steerman, Presenter MD, FACS, name RPVI EVMS Assistant Professor of Surgery Sentara Vascular Specialists Renal Denervation For Hypertension: Status Update Disclosures Disclosures Speaker s Panel
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Disclosures for Dr. Bhatt
 Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Renal Denervation Deepak L. Bhatt, MD, MPH, FACC, FAHA, FSCAI, FESC Executive Director of Interventional Cardiovascular Programs, BWH Heart & Vascular Center Professor of Medicine, Harvard Medical School
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
With an unrestricted educational grant from. The Interventional Treatment of Resistant Hypertension
 With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
With an unrestricted educational grant from The Interventional Treatment of Resistant Hypertension Felix Mahfoud Interventional Cardiology University Hospital Homburg/Saar Germany Dr. Mahfoud graduated
Renal Sympathetic Denervation for HTN
 Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Renal Sympathetic Denervation for HTN Se-Young Yim Department of CardioVascular Center Samsung Medical Center Worldwide Prevalence of Hypertension Is Increasing In 2000, 972 million (26%), of the adult
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction?
 Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
Renal Sympathetic Denervation Beyond Hypertension: Therapy for Arrhythmias and for Autonomic Nervous System Dysfunction? Vivek Y. Reddy, MD Helmsley Trust Professor of Medicine Director, Cardiac Arrhythmia
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Transcatheter Perivascular Alcohol- Mediated Renal Denervation
 Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Transcatheter Perivascular Alcohol- Mediated Renal Denervation Wojtek Wojakowski, MD, PhD Medical University of Silesia American Heart of Poland Katowice, Poland I, Wojciech Wojakowski DO NOT have a financial
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION
 CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
CATHETER-BASED RENAL DENERVATION INCREASES INSULIN SENSITIVITY AND IMPROVES GLUCOSE METABOLISM IN PATIENTS WITH RESISTANT HYPERTENSION F. Mahfoud, Ch. Ukena, B. Cremers, I. Kindermann, M. Kindermann, P.
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Management of Resistant Hypertension in Diabetes
 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University,
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
WPCCS May2013. Mr Ian Williams Consultant Vascular Surgeon UHW. Consultant Cardiologist UHW
 Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Peripheral Vascular Disease WPCCS May2013 Mr Ian Williams Consultant Vascular Surgeon UHW Prof Julian Halcox Prof Julian Halcox Consultant Cardiologist UHW Case 1? Ischaemic Legs History 85 years lady?varicose
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Neuromodulation Device Therapy for Treatment of Hypertensive Heart Disease
 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp REVIEW Neuromodulation Device Therapy for Treatment of Hypertensive Heart Disease Thomas M. Todoran, MD;
Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp REVIEW Neuromodulation Device Therapy for Treatment of Hypertensive Heart Disease Thomas M. Todoran, MD;
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1
 Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Radiofrequency Energy Provides Safe & Durable Blood Pressure Reduction: Complete 3 Year Results from Symplicity HTN-1 Henry Krum MBBS PhD FRACP FESC for the Symplicity I Investigators CCRE Therapeutics,
Christian Daugaard Peters, MD, PhD Department of Renal Medicine Aarhus University Hospital, Denmark Disclosures: None
 The effect of renal denervation on central blood pressure and arterial stiffness in treatment resistant essential hypertension: a substudy of a randomized sham-controlled double-blinded trial (the ReSET
The effect of renal denervation on central blood pressure and arterial stiffness in treatment resistant essential hypertension: a substudy of a randomized sham-controlled double-blinded trial (the ReSET
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Renal Denervation Catheters - Medical Devices Pipeline Assessment, 2017
 Renal Denervation Catheters - Medical Devices Pipeline Assessment, 2017 Renal Denervation Catheters - Medical Devices Pipeline Assessment, 2017 The Business Research Store is run by Sector Publishing Intelligence
Renal Denervation Catheters - Medical Devices Pipeline Assessment, 2017 Renal Denervation Catheters - Medical Devices Pipeline Assessment, 2017 The Business Research Store is run by Sector Publishing Intelligence
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich,
 The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The effect of renal denervation in patients with advanced heart failure: OLOMOUC I Study M. Táborský, M. Lazárová, J. Václavík, D. Richter ESC 2012, Munich, 27.08.2012 Disclosures MT: honoraria Bayer,
The Future of Renal Denervation
 The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
The Future of Renal Denervation Ron Waksman, MD, FACC, FSCAI Professor of Medicine, (Cardiology) Georgetown University Director, Cardiovascular Research Advanced Education MedStar Heart Institute, Washington
Renal Artery FFR. Woo-Young Chung. Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center
 Renal Artery FFR Woo-Young Chung Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center Why renal FFR? Renal artery angioplasty (PTRA) Indication of Renal artery angioplasty
Renal Artery FFR Woo-Young Chung Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center Why renal FFR? Renal artery angioplasty (PTRA) Indication of Renal artery angioplasty
SPYRAL HTN ON MED. Disclosure
 Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Renal Denervation in the Presence of Antihypertensive Medications: Six-month Results from the Randomized, Blinded, Sham-controlled SPYRAL HTN-ON MED Trial Dr. David E. Kandzari Piedmont Heart Institute,
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension
 The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
The Global SYMPLICITY Registry: Safety and Effectiveness of Renal Artery Denervation In Real World Patients With Uncontrolled Hypertension Michael Böhm, MD on behalf of the GSR Investigators March 30,
RENAL SYMPATHETIC DENERVATION PAST, PRESENT AND FUTURE
 RENAL SYMPATHETIC DENERVATION THE ROLE OF THE SYMPATHETIC NERVOUS SYSTEM PAST, PRESENT AND FUTURE Dr RS DAWOOD DEPARTMENT OF CARDIOLOGY CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL SATURDAY 02/08/2014 FACT
RENAL SYMPATHETIC DENERVATION THE ROLE OF THE SYMPATHETIC NERVOUS SYSTEM PAST, PRESENT AND FUTURE Dr RS DAWOOD DEPARTMENT OF CARDIOLOGY CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL SATURDAY 02/08/2014 FACT
Creative blood pressure management: whys and the tricks
 Creative blood pressure management: whys and the tricks Cynthia D. Caraballo-Hunt, MD Kaiser/OHSU Family Medicine Faculty Beaverton Medical Office NW Permanente, Portland, OR Objectives 1. Describe current
Creative blood pressure management: whys and the tricks Cynthia D. Caraballo-Hunt, MD Kaiser/OHSU Family Medicine Faculty Beaverton Medical Office NW Permanente, Portland, OR Objectives 1. Describe current
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Transcatheter Renal Denervation and Hong Kong Experience
 Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Transcatheter Renal Denervation and Hong Kong Experience Dr. Steven Li Siu-lung FACC, FESC, FRCP, FACP Director, Heart Centre, Union Hospital President, Hong Kong Society of Congenital and Structural Heart
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications
 Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Relevance of sympathetic overactivity in hypertension and heart failure Therapeutic Implications Uta C. Hoppe, MD, FESC Dep. of Internal Medicine II Paracelsus University Salzburg Austria Disclosures Within
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Prof. Andrzej Wiecek Department of Nephrology, Endocrinology and Metabolic Diseases Medical University of Silesia Katowice, Poland.
 What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
What could be the role of renal denervation in chronic kidney disease? Andrzej Wiecek, Katowice, Poland Chairs: Peter J. Blankestijn, Utrecht, The Netherlands Jonathan Moss, Glasgow, UK Prof. Andrzej Wiecek
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Renal denervation for treatment of resistant hypertension
 Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Renal denervation for treatment of resistant hypertension Dr U. Nqebelele Division of Nephrology Department of Internal Medicine Charlotte Maxeke Johannesburg Academic Hospital Thomas Willis: 1621-1675
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Ambulatory Blood Pressure Measurement. Objectives of the Presentation. Methods of Measuring BP: Pros and Cons
 Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
Ambulatory Blood Pressure Measurement William B. White, MD Professor of Medicine and Chief, Hypertension and Clinical Pharmacology Calhoun Cardiology Center University of Connecticut School of Medicine
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Renal sympathetic denervation as a potential treatment for hypertension
 Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Renal sympathetic denervation as a potential treatment for hypertension (Why we must keep going) Dr Andrew SP Sharp Consultant Cardiologist and Honorary Senior Lecturer Royal Devon and Exeter Hospital
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
NEWLY DETECTED ATRIAL FIBRILLATION. Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology
 NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Implanting a baroreceptor stimulation device for resistant hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Implanting a baroreceptor stimulation device for resistant hypertension Hypertension (or high blood pressure)
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Implanting a baroreceptor stimulation device for resistant hypertension Hypertension (or high blood pressure)
Renal Denervation: The Case for Cardiology
 Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Renal Denervation: The Case for Cardiology John C. Gurley, MD University of Kentucky Presenter Disclosure Information John C Gurley, MD Renal Denervation: The Case for Cardiology FINANCIAL DISCLOSURE:
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal