SIMPLY. Fluids. Dr Will Dooley
|
|
|
- Myra Hill
- 6 years ago
- Views:
Transcription
1 SIMPLY. Fluids Dr Will Dooley

2 Plan Maintenance vs Resuscitation Prescribing Common Errors Calculations Drip rates
3 Case 54 yo presents with severe diarrhoea and vomiting. How would you proceed?
4 Assessment History Examination Investigation Management
5 Assessment History
6 Case 54 yo presents with severe diarrhoea and vomiting. HPC Vomiting for 3 days, 2 days of diarrhoea Unable to tolerate oral fluids for 24hrs Ate dodgy kebab on Saturday. No recent travel. Feeling unwell, thirsty, light-headed when standing Passing less urine than normal No feverish symptoms HISTORY Input vs Output?Limited intake?high Losses Symptoms Urine Co-morbidities Normally fit and well
7 Assessment Examination
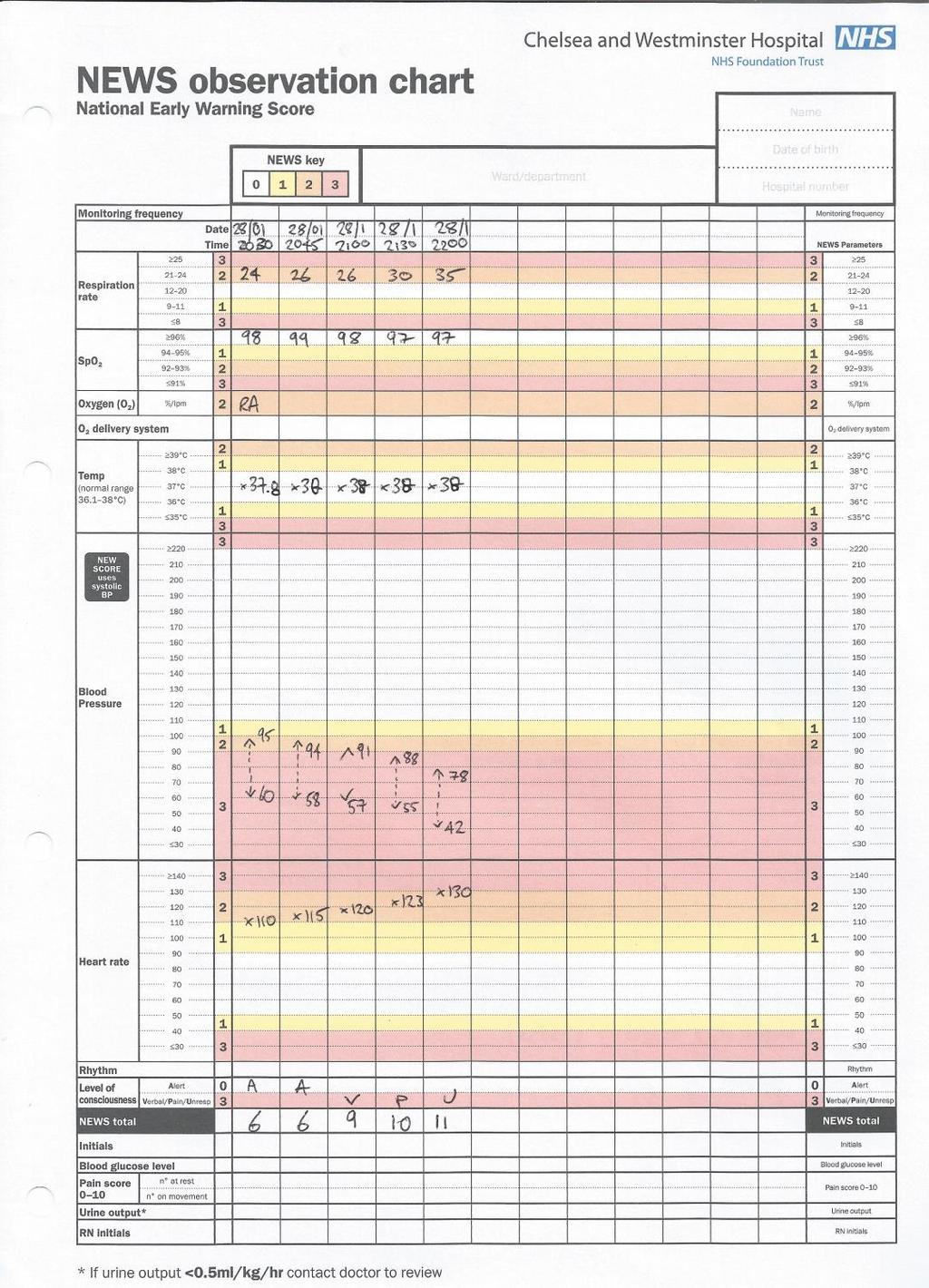
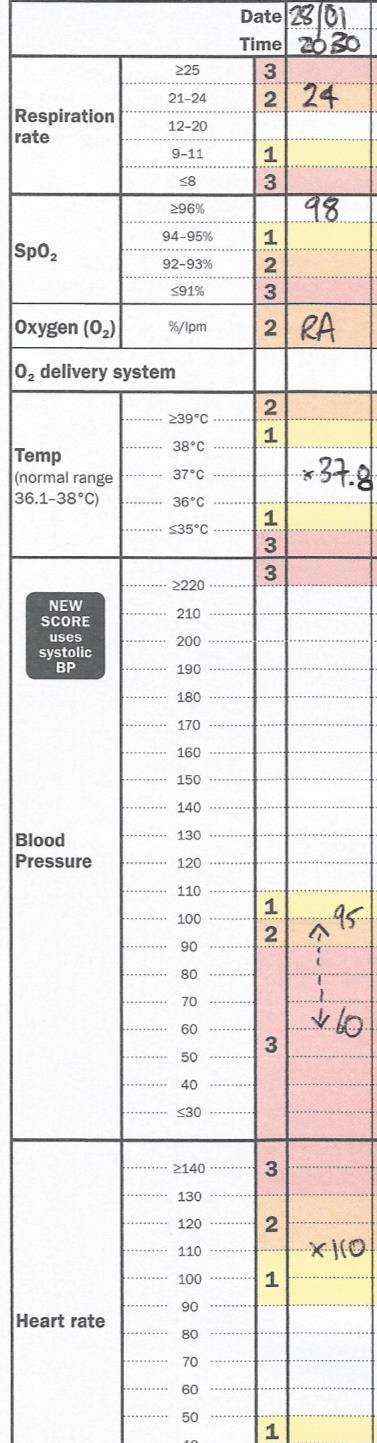
8 Case 54 yo presents with severe diarrhoea and vomiting. Examination Alert Accessory muscles of respiration Cool peripheries Dry mucus membranes Observations: See chart A B C D E EXAMINATION Respiratory Rate >20/min Systolic Blood Pressure <100mmHg Heart Rate >90 bpm Cold peripherally JVP Urine output < 0.5 ml/kg/hr Temperature AVPU Dry mucosae T37.0 BP 95/60 HR 110 RR 24 98% OA

9
10 Assessment Investigation Bedside: INVESTIGATIONS Weight Fluid Balance Chart Urine dipstick Weight: 100kg Urine : 4+ ketones, nil else What should his Urine Output be over 4 hours? Bloods: U&E FBC Bloods: Electrolytes Imaging:Chest X-Ray
11 Management IV Access: What size cannula? Fluid Challenge: What type of fluid? How much fluid?


12 Type of fluid and rate 0.9% Normal saline Hartmann / Plasmalyte 5% glucose Crystalloids Clear fluids- water+electrolytes 0.9% Normal Saline Dextrose Hartmann's Na 154 mmol 131 mmol 0 K 0 5 mmol 0 Cl 154 mmol 111 mmol 0 Osmol 303 mosm/l 279 mosm/l 253 Other nil Lactate 29 Calcium 2 mosm/l Glucose 50g/l Colloids Gelatinous- particles suspended in solution Volplex Gelofusion Blood
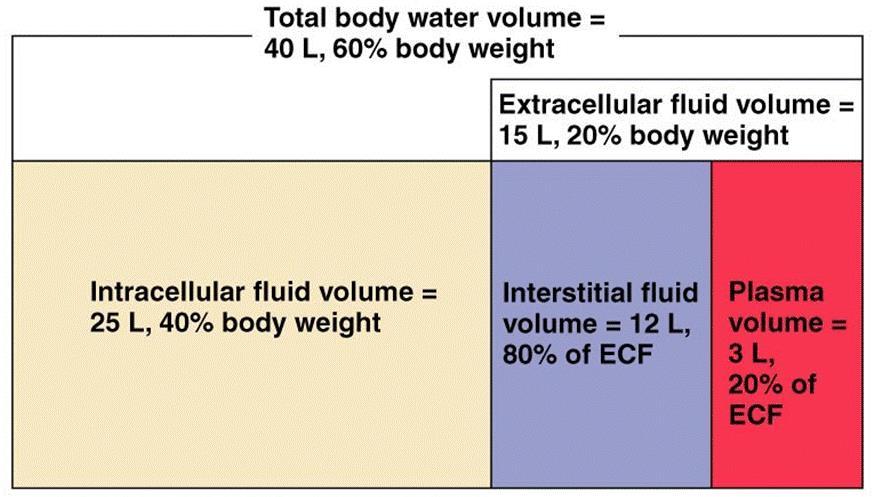


13 Fluid compartments COLLOIDS C STALLOIDS
14 How much fluid?
15 Resuscitation IF NO OVERLOAD SIGNS Assess- ABCDE * FLUID CHALLENGE * mls Crystalloid Re-assess Further mls bolus until 2L given RE-ASSESS
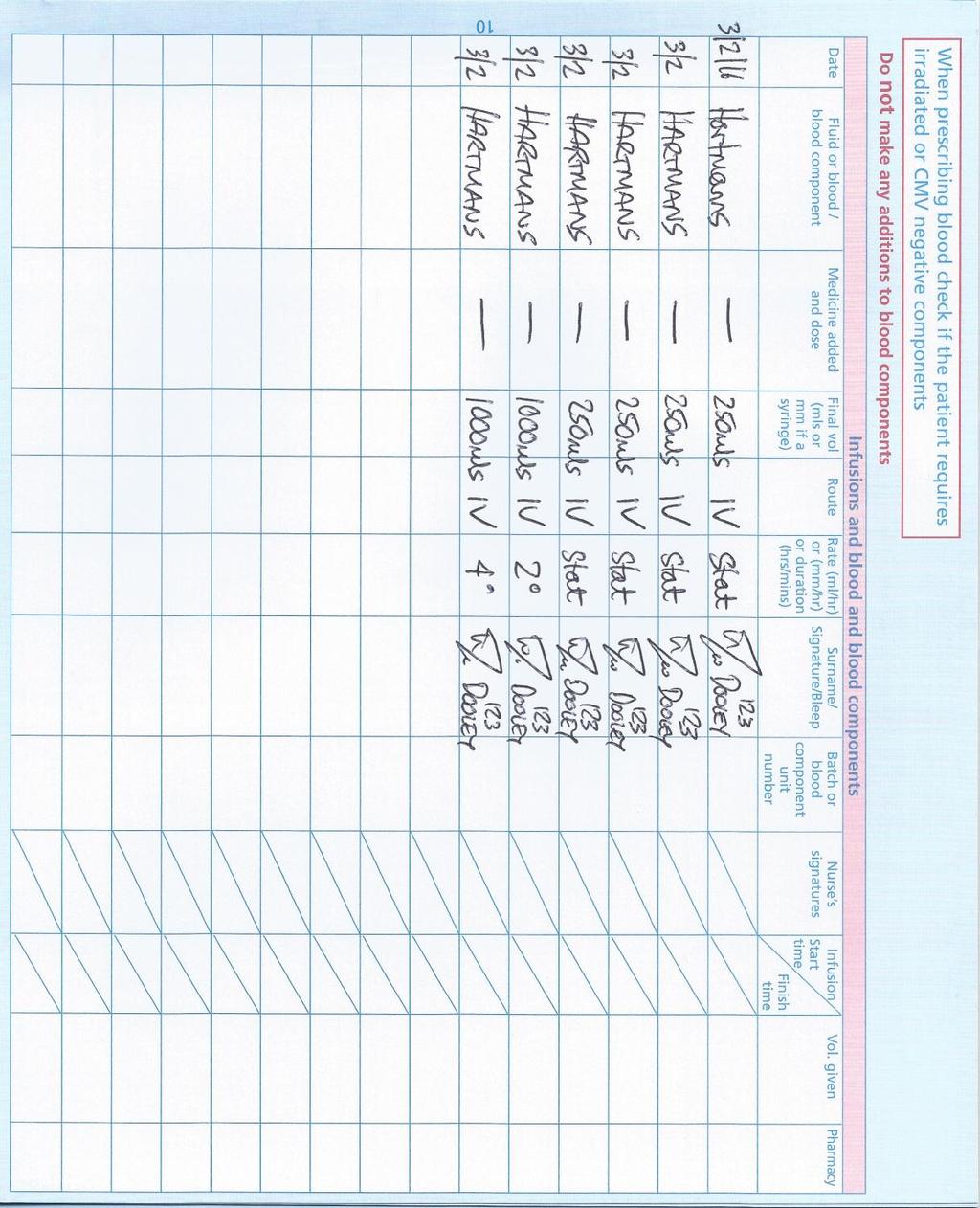
16 Fluid prescription

17 Fluid balance
18 Case 2 35yo Post emergency caesarean section (for sepsis and fetal distress) Blood loss 1300mls Obs T37.0 BP 95/60 HR 110 RR 24 98% OA Fluid challenge
19 Resuscitation Assess- ABCDE IF NO OVERLOAD SIGNS * FLUID CHALLENGE * mls Crystalloid Reassess Further mls bolus until 2L given REASSESS If improves likely hypovolaemia If does not improve... Likely something else
20 Maintenance Requirements Fluid: Sodium: K +: ml/kg/day 1-2mmol /kg/day 0.5-1mmol /kg/day (approx. max 10mmol/hr) + Replacements Example 70kg per day Fluid: ml Sodium: mmol Potassium: 35-70mmol DOES PATIENT NEED IV FLUID??? 0.9% Normal saline Hartmanns Na 154 mmol 131 mmol 0 K 0 5 mmol 0 Cl 154 mmol 111 mmol 0 Osmol 303 mosm/l 279 mosm/l Other nil Lactate 29 Calcium 2 5% glucose 253 mosm/l Glucose 50g/l
21 Prescribing maintenance fluids HISTORY Input vs Output A EXAMINATION INVESTIGATIONS Bedside: Weight?Limited intake?high Losses Symptoms Urine Co-morbidities B C D E Respiratory Rate >20/min Systolic Blood Pressure <100mmHg Heart Rate >90 bpm Cold peripherally JVP Urine output < 0.5 ml/kg/hr Temperature AVPU Dry mucosae balance dipstick Bloods: Imaging: Fluid Urine Electrolytes Chest X-Ray Depends on the case: e.g.?nbm

22 Calculations
23 Calculating Drip Rate What is the drip rate (drops/minute) required for a unit of blood to run over 4 hours using giving set with drop factor of 20 drops/ml? 1 unit of blood = approx 400mls
24 Calculating Drip Rate Drip rate (drops per minute) Volume (ml) Time (minute) Drop Factor (drops per ml) or (gtt per ml) Three different methods use the one you re most comfortable with
25 1. Know the Equation What is the drip rate (drops/minute) required for a unit of blood to run over 4 hours using giving set with drop factor of 20 drops/ml? Drip rate = Volume x Drop Factor Time Drip Rate = 400mls x 20 gtt/ml 240mins = 33 drops / min = 32 drops / min OR 8 drops / 15 sec
26 2. Think about the problem Drip rate is DROPS PER MINUTE This is TOTAL DROPS DIVIDED BY TIME TOTAL DROPS same as VOLUME x DROP FACTOR (as this is drops per ml) What is the drip rate (drops/minute) required for a unit of blood to run over 4 hours using giving set with drop factor of 20 drops/ml? TOTAL DROPS = VOLUME X DROP FACTOR = 400 X 20 = 8000 DRIP RATE = TOTAL DROPS / TIME = 8000 / 240 = 33 drops/min

27 3. Look at the units Drip rate (drops per minute) Volume Time Drop Factor (ml) (minute) (drops per ml) Drip rate Drops = Volume ml x Drop Factor min Time mins Drops ml Drip Rate = 400mls x 20 gtt/ml 240mins = 33 drops / min
28 Converting drip rate to ml/hour What is the transfusion rate in ml/hour of a blood transfusion being run at 40 drops/minute through a giving set with drop factor of 20 drops/ml? Transfusion Rate Drip rate Drop Factor (ml/hr) (Drops/minute) (Drops/ml)

29 1. Know the Equation Transfusion Rate = Drip Rate Drop Factor What is the transfusion rate in ml/hour of a blood transfusion being run at 40 drops/minute through a giving set with drop factor of 20gtt/ml? Transfusion Rate = 40 x = 120 ml/hr
30 2. Think about the problem What is the transfusion rate in ml/hour of a blood transfusion being run at 40 drops/minute through a giving set with drop factor of 20 drops/ml? 20 drops per ml Therefore 40 drops = 2ml Therefore 2ml per minute Therefore 2x60 = 120 ml per hour
31 3. Look at the units What is the transfusion rate in ml/hour of a blood transfusion being run at 40 drops/minute through a giving set with drop factor of 20 drops/ml? Transfusion Rate Drip rate Drop Factor (Ml/hr) (Drops/minute) (Drops/ml) Ml/hr = drops divided by drops hr ml = drops x ml hr drops = 40 x 60 divided by 20 = 120 ml per hour
32 Try these later What is the drip rate (drops/minute) required for a 1 litre bag of saline to run over 5 hours using giving set with drop factor of 10 drops/ml? Drip rate = Volume x Drop Factor Time Drip rate = 1000 x 10 60x5 = 33 gtt/min What is the transfusion rate in ml/hour of a blood transfusion being run at 20 drops/minute through a giving set with drop factor of 15 drops/ml? Transfusion Rate = Drip Rate Drop Factor = 20 x = 80 ml/hr

33 Summary IV only if not PO Calculations Take your time! Is your answer sensible? Practice! Any Questions?
34 Calculations % Adrenaline. How many grams of adrenaline are in 1 litre of saline? Same as 1:10,000 adrenaline So 1 unit adrenaline in 10,000 units saline Or 1g Adrenaline in 10,000ml saline So 0.1g in 1 litre (one decimal place to the right) 2. What should the urine output for a 80kg patient over 4 hours be? UO > 0.5 ml / kg / hr So at least 0.5 x 80 x 4 = 160ml
35 Burns A patient presents with burns from fire. The burns are affecting both his arms, his face and head. What percentage body area has been effected?

36 Herndon Rule of 9s Arm 9% Head 9% Neck 1% Leg 18% Anterior trunk 18% Posterior trunk 18%
SIMPLY. Fluids. Dr William Dooley
 SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
SIMPLY. Fluids Dr William Dooley Plan Fluid management Resuscitation Routine Maintenance Replacement Redistribution Reassessment Common Errors Calculations Assessment?ORAL vs. IVF History Limited intake
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline 1.1. This guideline contains recommendations about general principles for managing intravenous (IV)
CLINICAL GUIDELINE FOR INTRAVENOUS FLUID THERAPY FOR ADULTS IN HOSPITAL 1. Aim/Purpose of this Guideline 1.1. This guideline contains recommendations about general principles for managing intravenous (IV)
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
IV Fluids Do you know what you are doing?
 IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
LET - Maths, Stats & Numeracy
 Metric Conversions Here are some metric weights arranged in size order, starting with the biggest:- Kg (kilogram) g (gram) mg (milligram) mcg (microgram) Each one is a thousand (1000) times smaller than
Metric Conversions Here are some metric weights arranged in size order, starting with the biggest:- Kg (kilogram) g (gram) mg (milligram) mcg (microgram) Each one is a thousand (1000) times smaller than
HHS. Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours. Page 1 of 2 AFFIX PATIENT LABEL ! INFORM DIABETES TEAM OF ADMISSION!
 Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Country Health SA Local Health Network. Version control and change history
 Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Index No: MMG11/1. Version: 1. Date ratified: 12 th November 2013
 Index No: Intravenous fluid prescription in children For previously well children aged one month to 16 years (excluding renal, cardiac, diabetic ketoacidosis and acute burns patients) Version: 1 Date ratified:
Index No: Intravenous fluid prescription in children For previously well children aged one month to 16 years (excluding renal, cardiac, diabetic ketoacidosis and acute burns patients) Version: 1 Date ratified:
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Dengue Fever & Dengue Shock Syndrome. 07-May-18 PLES / SLCP 1
 Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Easy way to calculate drugs MONA ALHARBI
 Easy way to calculate drugs MONA ALHARBI Objective At the end of this lecture you should be able to : Calculate dosage drugs. Calculate drip rate (drops/min). Conversion of dosages to ml/hour Calculating
Easy way to calculate drugs MONA ALHARBI Objective At the end of this lecture you should be able to : Calculate dosage drugs. Calculate drip rate (drops/min). Conversion of dosages to ml/hour Calculating
INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE
 INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE WORKBOOK FOR THE CALCULATION OF FLOW RATES AND MEDICATION DOSAGES January 2014 WORKBOOK C O N T E N T S Page Professional Responsibilities 3 Methods for flowrate
INTRAVENOUS THERAPY INSTRUCTIONAL PACKAGE WORKBOOK FOR THE CALCULATION OF FLOW RATES AND MEDICATION DOSAGES January 2014 WORKBOOK C O N T E N T S Page Professional Responsibilities 3 Methods for flowrate
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Applicable to. Team Members Performing MD House Staff APRN/PA RN LPN
 Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Protocol: Adult Burn Fluid Resuscitation Category Clinical Practice Protocol Number Approval Date vember 1, 2016 Due for review vember 1, 2018 Applicable to VUH Children s DOT VMG Off-site locations VMG
Standard Operating Procedure (SOP) Management of intervention group patients SOP 001
 Management of intervention group patients SOP 001") ` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
SCENARIO. Maternal Medicine -DKA LEARNING OBJECTIVES
 SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Suboptimal hydration harms patients.
 Suboptimal hydration harms patients. NHS Fife is committed to improving hydration management. To achieve this we need your help! In 2014 new fluid balance charts were implemented in the Victoria Hospital,
Suboptimal hydration harms patients. NHS Fife is committed to improving hydration management. To achieve this we need your help! In 2014 new fluid balance charts were implemented in the Victoria Hospital,
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
THe Story of salty Sam
 THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
THe Story of salty Sam Understanding fluids, urea and electrolyte balance; a quantitative approach. A self-directed learning activity. Part One. meet salty sam Salty Sam is a pretty average 70 kg bloke,
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
Acute Kidney Injury shared guidance
 Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
September 2014 V0.17. Paediatric Daily Fluid Prescription & Balance Chart
 September 14 V0.17 Aims and outcomes of session. Aim: To provide guidance on correctly completing the paediatric daily fluid prescription & balance chart. Outcomes: Demonstrate the ability to: calculate
September 14 V0.17 Aims and outcomes of session. Aim: To provide guidance on correctly completing the paediatric daily fluid prescription & balance chart. Outcomes: Demonstrate the ability to: calculate
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
CLINICAL GUIDELINES ID TAG
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Guideline for the perioperative fluid management in children Kieran O Connor Anaesthetics ATICS Date Uploaded: 26/04/2016 Review
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Guideline for the perioperative fluid management in children Kieran O Connor Anaesthetics ATICS Date Uploaded: 26/04/2016 Review
PAEDIATRIC FLUIDS RCH DEHYDRATION
 PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Country Health SA Local Health Network
 Country Health SA Local Health Network Protocol (Clinical) Title: Hyperglycaemic Hyperosmolar State Management in Adults with Type 2 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor:
Country Health SA Local Health Network Protocol (Clinical) Title: Hyperglycaemic Hyperosmolar State Management in Adults with Type 2 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor:
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI. CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) HEPARIN ANTICOAGULATION Page 1 of 5
 HEPARIN ANTICOAGULATION Page 1 of 5") HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
TOTAL PARENTERAL NUTRITION
 TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
ADVANCED ASSESSMENT Medical Math
 ONTARIO BASE HOSPITAL GROUP ADVANCED ASSESSMENT Medical Math 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Medical Math AUTHOR Tim Dodd AEMCA, ACP Hamilton Base Hospital REVIEWERS/CONTRIBUTORS Rob
ONTARIO BASE HOSPITAL GROUP ADVANCED ASSESSMENT Medical Math 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Medical Math AUTHOR Tim Dodd AEMCA, ACP Hamilton Base Hospital REVIEWERS/CONTRIBUTORS Rob
The History & Practice of IV Fluid Therapy have we advanced in 185 years?
 The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
The History & Practice of IV Fluid Therapy have we advanced in 185 years? Liam Plant Clinical Professor of Renal Medicine University College Cork Consultant Renal Physician Cork University Hospital National
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
DIABETIC KETOACIDOSIS MANAGEMENT PLAN:
 DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
Tubes, Lines, and Drains for the MS3 Surgery Clerkship. Chris Freeman, MD University of Cincinnati Department of Surgery
 Tubes, Lines, and Drains for the MS3 Surgery Clerkship Chris Freeman, MD University of Cincinnati Department of Surgery A Patient s Volume Status Matters! A Patient s Volume Status Matters! Hypovolemia
Tubes, Lines, and Drains for the MS3 Surgery Clerkship Chris Freeman, MD University of Cincinnati Department of Surgery A Patient s Volume Status Matters! A Patient s Volume Status Matters! Hypovolemia
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline
 TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
TBSA Burn Estimation Chart Adult Major Burn Clinical Practice Guideline Patient Label Anatomical Subunit Percent Total Percent One Side Anterior Posterior Injury Subtotal 3.5% 2nd and 3rd degree burns
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank
 Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank Adam Sutherland Senior Clinical Pharmacist, RMCH Clinical Lecturer, University of Manchester NIHR MClinRes Trainee,
Using Balanced Fluids in Paediatrics: Implementing NICE Guidance without breaking the bank Adam Sutherland Senior Clinical Pharmacist, RMCH Clinical Lecturer, University of Manchester NIHR MClinRes Trainee,
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
LESSON 14 Medication Math
 LESSON 14 Medication Math What is Med Math? (Drug/Dosage Calculations) Nurses must perform dosage calculations when administering medications and intravenous fluids. Pharmacology math requires the nurse
LESSON 14 Medication Math What is Med Math? (Drug/Dosage Calculations) Nurses must perform dosage calculations when administering medications and intravenous fluids. Pharmacology math requires the nurse
Paediatric Directorate
 Paediatric Directorate Dehydration Guidelines Primary cause of dehydration diarrhoea +/- vomiting. Approximately 10%Children < 5yrs present with gastroenteritis each year Diagnosis History - sudden change
Paediatric Directorate Dehydration Guidelines Primary cause of dehydration diarrhoea +/- vomiting. Approximately 10%Children < 5yrs present with gastroenteritis each year Diagnosis History - sudden change
48 th Annual Meeting. A Review of Pharmacy Calculations for Pharmacy Technicians. Metric System of Measurement. Disclosure. Common Conversions
 48 th Annual Meeting A Review of Pharmacy Calculations for Pharmacy Technicians Nina Pavuluri, Ph.D. Navigating the Oceans of Opportunity Metric System of Measurement Base Unit Factor Name Symbol 1 (g,
48 th Annual Meeting A Review of Pharmacy Calculations for Pharmacy Technicians Nina Pavuluri, Ph.D. Navigating the Oceans of Opportunity Metric System of Measurement Base Unit Factor Name Symbol 1 (g,
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Review calculation procedures for the following:
 Review calculation procedures for the following: Convert in the Metric System 1000 mg = 1 gram 1000 ml = 1 liter To convert from grams to mg, move the decimal point 3 places to the right (add zeros to
Review calculation procedures for the following: Convert in the Metric System 1000 mg = 1 gram 1000 ml = 1 liter To convert from grams to mg, move the decimal point 3 places to the right (add zeros to
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC)
") Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
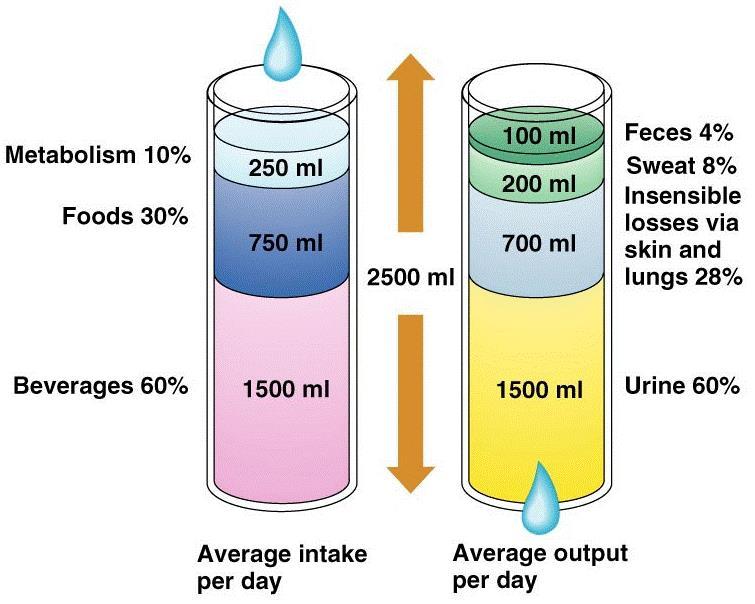
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group
 in Adults Inpatient Diabetes Steering Group") Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group 1. Introduction 1.1 This document sets out the University Hospitals of Leicester (UHL) guidelines
Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group 1. Introduction 1.1 This document sets out the University Hospitals of Leicester (UHL) guidelines
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
It s as easy as ABC. Dr Andrew Smith
 It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
Top tips for surviving your first on call Dr Maleeha Rizvi
 Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Diabetic Ketoacidosis (DKA)
") Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
AS - EXPERT
 AS - EXPERT 204-009-361 AS - EXPERT 204-009-362 AS - EXPERT 204-009-363 AS - EXPERT 204-009-364 AS - EXPERT 204-009-365 AS - EXPERT 204-009-366 AS - EXPERT 204-009-367 AS - EXPERT 204-009-368 AS - EXPERT
AS - EXPERT 204-009-361 AS - EXPERT 204-009-362 AS - EXPERT 204-009-363 AS - EXPERT 204-009-364 AS - EXPERT 204-009-365 AS - EXPERT 204-009-366 AS - EXPERT 204-009-367 AS - EXPERT 204-009-368 AS - EXPERT
Weekly Cisplatin + Radiotherapy - Interlace study -
 Weekly Cisplatin + Radiotherapy - Interlace study - A phase III multicentre trial of weekly induction chemotherapy followed by standard chemoradiation versus standard chemoradiation alone in patients with
Weekly Cisplatin + Radiotherapy - Interlace study - A phase III multicentre trial of weekly induction chemotherapy followed by standard chemoradiation versus standard chemoradiation alone in patients with
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
File No 99/ Circular No 2002/26. Issued 28 June Contact
 CIRCULAR File No 99/11383-4 Circular No 2002/26 Issued 28 June 2002 Contact Mary Crum (02) 9391 9100 Quality and Clinical Policy Branch MANAGING YOUNG CHILDREN AND INFANTS WITH GASTROENTERITIS IN HOSPITALS
CIRCULAR File No 99/11383-4 Circular No 2002/26 Issued 28 June 2002 Contact Mary Crum (02) 9391 9100 Quality and Clinical Policy Branch MANAGING YOUNG CHILDREN AND INFANTS WITH GASTROENTERITIS IN HOSPITALS
The assessment helps decide if the patient is an emergency, priority or non-urgent case.
 Emergency Triage Assessment and Treatment The World Health Organisation (WHO) has produced some useful guidelines about how to improve the care of our patients and their survival in hospital. This is a
Emergency Triage Assessment and Treatment The World Health Organisation (WHO) has produced some useful guidelines about how to improve the care of our patients and their survival in hospital. This is a
Dengue Case Discussion. When things can go wrong!
 Dengue Case Discussion When things can go wrong! What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but
Dengue Case Discussion When things can go wrong! What the local experts say! 99.99% of walked in patients who come to hospital with dengue should walk out from hospital! Even those who come in Shock but
Emergency Department Chest Pain, Suspected Cardiac Adult Order Set
 Form Title Form Number Chest Pain, Suspected Cardiac Adult Order Set 20746 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
Form Title Form Number Chest Pain, Suspected Cardiac Adult Order Set 20746 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sample. Affix patient label within this box.
 Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
Nonparenteral medications
 Nonparenteral medications Capsules and unscored tablets are rounded to the nearest whole tablet. Scored tablets are rounded to the nearest 1/2 tablet. Liquid medications are rounded to one decimal place
Nonparenteral medications Capsules and unscored tablets are rounded to the nearest whole tablet. Scored tablets are rounded to the nearest 1/2 tablet. Liquid medications are rounded to one decimal place
COBIS. Fluid Resuscitation in Adults ADULT GUIDELINE
 COBIS Fluid Resuscitation in Adults ADULT GUIDELINE Page 1 of 6 Fluid resuscitation in adults Summary Fluid resuscitation for adults with burns is indicated for patients with greater than 15% burns. Patients
COBIS Fluid Resuscitation in Adults ADULT GUIDELINE Page 1 of 6 Fluid resuscitation in adults Summary Fluid resuscitation for adults with burns is indicated for patients with greater than 15% burns. Patients
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
CONTROLLED DOCUMENT. Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) Controlled Document Number: CG259
 Controlled Document Number: CG259") Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
Guidelines for the use of subcutaneous hydration in palliative care (hypodermoclysis) CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor:
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS
 Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Infection. Risk factor for infection ACoRN alerting sign with * Clinical deterioration. Problem List. Respiratory. Cardiovascular
 The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
The ACoRN Process Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis Support Infection Risk factor for
Blood Transfusion. Dr Will Dooley
 Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck
 Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
CETEP PRE-TEST For questions 1 through 3, consider the following scenario:
 CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY