Drug-Induced cardiovascular disease. Parastoo Mirzabeigi, Clinical Pharmacist
|
|
|
- Esmond Long
- 5 years ago
- Views:
Transcription

1 نام خدا به فارماكوويژيلانس و عوارض ناخواسته داروها دي ماه 1393
2 Drug-Induced cardiovascular disease Parastoo Mirzabeigi, Clinical Pharmacist
3 Hypertension Hypertension is a chronic medical condition that is characterized by persistent increases in systolic or diastolic blood pressure, or both. Prehypertension is a term used to identify patients with elevated blood pressures that are not high enough to be classified as hypertension, but are higher than normal. Most patients (90 95%) with hypertension have primary (also called essential ) hypertension. The remainder have secondary hypertension, which includes patients with drug-induced causes.
4 CAUSATIVE AGENTS Drug-induced hypertension is defined as high blood pressure caused by using or discontinuing the use of a chemical substance, drug, or medication. These medications may cause hypertension, exacerbate previously well-controlled hypertension, or antagonize the effects of antihypertensive pharmacotherapy






5
6 MECHANISMS Arterial blood pressure is regulated by several factors: the adrenergic nervous system, The renin angiotensin aldosterone system, kidney function and blood flow, hormonal regulatory systems (adrenal cortical hormones, vasopressin, thyroid, insulin), the vascular endothelium (nitric oxide, bradykinin, prostacyclin, endothelin). The various mechanisms by which drugs may induce hypertension are broadly categorized as: fluid-volume expansion, stimulation of sympathetic nervous system activity, interference with the action of antihypertensive drugs, paradoxical responses to antihypertensive agents, and unknown mechanisms.




7
8 CLINICAL PRESENTATION/ Elevated blood pressure and the development of hypertension are nearly always asymptomatic. The clinical significance of elevated blood pressure associated with the use of a drug is variable, depending on an individual s baseline blood pressure. It is important to note that the threshold blood pressure for the diagnosis of hypertension varies. Drug-induced blood pressure elevations, if persistent, may be clinically significant even if the blood pressure is not increased to above an individual s goal value.
9 Risk Factors for Drug-Induced Hypertension
10
11 Hypotension Drug-induced hypotension is a clinically important and potentially disabling problem that may lead to syncope, falls and injury, or sustained lack of organ perfusion resulting in ischemia, infarction, or both. The majority of episodes of drug-induced hypotension involve a drop in blood pressure after a patient assumes an upright position. This is known as orthostatic hypotension and has also been referred to as postural hypotension. Orthostatic hypotension is defined as a reduction in systolic blood pressure of at least 20 mm Hg or diastolic pressure of at least 10 mm Hg within 3 minutes of standing
12 Orthostatic hypotension may result from two different disorders in autonomic cardiovascular control: autonomic failure and neurally mediated syncope. Autonomic failure involves chronic debilitation of sympathetic efferent activity such that vasoconstriction is impeded. Drug-induced orthostatic hypotension is primarily due to autonomic failure in which the causative agent affects central or peripheral autonomic pathways.
13 ANTIHYPERTENSIVES ACE Inhibitors Captopril, Enalapril Angiotensin-Receptor Blockers Losartan, Olmesartan, Telmisartan, Valsartan Peripheral -ɑ blockers β-adrenergic Blockers (particularly with IV) Atenolol, Esmolol, Propranolol, Metoprolol Carvedilol, Labetalol Calcium-Channel Blockers Centrally acting α- adrenergic agonists Clonidine Methyldopa Peripheral-acting arterial vasodilators Duretics Amiloride,Chlorothiazide, Chlorthalidone, Furosemide, Hydrochlorothiazide Mannitol Inhibition of angiotensin II with increase in bradykinin concentrations Inhibition of angiotensin II at the receptor level Blockade of -adrenoreceptors Blockade of β-and α1-adrenoreceptors Blockade of L-type calcium channel Direct stimulation of -receptors in the vasomotor center of the medulla leading to: Reduction in peripheral vascular resistance Decreased heart rate (secondary to increased vagal tone). Direct arteriolar vasodilatation Inhibition of renal sodium reabsorption thereby leading to intravascular volume depletion Intravascular volume depletion
14 NON-ANTIHYPERTENSIVES Alzheimer s Agents Galantamine, Donepezil Anesthetic Agents Propofol Antiarrhythmic Agents Antidepressant Agents Amitriptyline, Clomipramine, Desipramine, Doxepin, Imipramine Trazodone Aripiprazole, Chlorpromazine Clozapine, Doxazosin, Haloperidol Olanzapine, Pimozide, Prazosin Quetiapine, Risperidone, Tamulosin Terazosin, Thioridazine, Thiothixene Trifluoperazine, Ziprasidone Chemotherapy Agents Dacarbazine, Carmustine, Vincristine Vinblastine, Magnesium Overactivation of muscarinic and nicotinic sites of autonomic and somatic nerves Direct vasodilatation of venous smooth muscle Reduced systemic vascular resistance due to α- adrenoreceptor blockade Blockade of central and/or peripheral - adrenoreceptors Calcium chelation by citric acid in the preparation, Vasodilation due to alcohol content of the diluent, Neurotoxicity- Inhibition of norepinephrine secretion, Neurotoxicity, Opposition of calciumdependent arterial constriction Atracurium, Codeine, Fentanyl, Mivacurium, Morphine, Succinylcholine, Vancomycin Release of histamine
15 Signs and Symptoms Associated with Drug-Induced Hypotension

16 Risk Factors for Drug-Induced Hypotension

17 Approaches to Help Prevent Drug- Induced Hypotension
18 Myocardial Ischemia and Acute Coronary Syndromes Myocardial ischemia occurs as a result of increased myocardial demand, decreased myocardial oxygen supply, or both, and most commonly occurs in patients with atherosclerotic coronary artery disease. Acute myocardial infarction is a clinical syndrome associated with the development of a prolonged occlusion of a coronary artery leading to decreased oxygen supply, myocardial ischemia, and irreversible damage to myocardial tissue
19 MYOCARDIAL OXYGEN SUPPLY AND DEMAND The oxygen demand of the heart is determined by its workload. The major determinants of myocardial oxygen consumption are heart rate, contractility, and intramyocardial wall tension during systole. Of the many factors that affect oxygen supply to the heart, coronary blood flow and oxygen extraction are most important. Complex factors that determine coronary blood flow include duration of diastole and coronary vascular resistance. A drug may cause myocardial ischemia i simply by modifying i any one of these factors.
20
21 CLINICAL PRESENTATION AND DIFFERENTIAL DIAGNOSIS Drug-Induced Myocardial Ischemia The clinical presentation of a patient with drug induced ischemia is similar to that of any ypatient with angina or ischemia associated with atherosclerotic coronary artery disease. The most apparent difference is that drug-induced ischemia The most apparent difference is that drug-induced ischemia may occur in individuals who do not have, or who are not at risk for, coronary artery disease.
22 Drug-Induced Acute Coronary Syndrome In most situations, the clinical presentation of a patient with drug-induced acute coronary syndrome is similar to that of any patient with non drug-induced acute coronary syndrome. However, there are several exceptions to this generalization. like myocardial ischemia, acute coronary syndromes are relatively unusual in young populations (<45 years of age). Approximately 25% of all acute myocardial infarctions in individuals 18 to 45 years of age have been associated with frequent cocaine use
23 Drug-Induced Heart Failure Heart failure is a major cause of morbidity and mortality Drug-induced heart failure in patients without preexisting left ventricular dysfunction is quite rare; however, drug induced exacerbation of symptoms of heart failure occur more frequently in those with established heart failure.
24 Drug-induced HF is mediated by three basic mechanisms: - inhibition of myocardial contractility (negative inotropic agents and direct toxins), - proarrhythmic effects, - expansion of plasma volume
25 The most recognized negative inotropic agents are the β- blockers,calcium-channel blockers (CCB), most notably verapamil and diltiazem, antiarrhythmic agents, especially disopyramide, quinidine, flecainide The anthracyclines (daunorubicin and doxorubicin) have a direct, dose-related cardiotoxicity that can be minimized by limiting total cumulative doses to 500 to 600 mg/m Drugs that increase the QT interval induce proarrhythmic effects in some patients. Worsening of HF occurs if the disturbed rhythm compromises cardiac functioning.
26 Drugs that induce sodium and water retention are NSAIDs (via prostaglandin inhibition), certain antihypertensive drugs, glucocorticoids, androgens, estrogens Thiazolidinedione antidiabetic drugs pioglitazone and rosiglitazone. Worsening of HF appears to be dose-dependent dependent and is presumed to be at least partly caused by fluid retention. they not be administered to patients with NYHA class III or IV HF and that they be used cautiously in earlier stages of HF.
27
28 CLINICAL PRESENTATION The clinical presentation of patients with drug induced heart failure is not different from that from other causes. Symptoms may occur gradually following initiation of a culprit drug. For most drugs that induce heart failure, worsening symptoms of heart failure begin shortly (within days) after initiation of therapy with the drug or increasing the dose. For those drugs causing fluid retention, ti plasma volume expansion may take several days to manifest in symptoms of dyspnea. The onset of anthracycline-induced heart failure has been well characterized. Von Hoff et al. reported an average time of onset of symptoms of heart failure of 33 days
29 Risk Factors for Drug-Induced Heart Failure Antiarrhythmic Agents Preexisting left ventricular dysfunction Glitazones Preexisting left ventricular dysfunction History of myocardial infarction History of symptomatic coronary artery disease Hypertension Left ventricular hypertrophy Significant aortic or mitral valve disease Advanced d age (>70 yr) Long-standing diabetes (>10 yr) Preexisting edema Current treatment with loop diuretics Development of edema or weight gain Insulin coadministration Chronic kidney disease Anthracyclines Cumulative doxorubicin dose (550 mg/m2) Three-week schedule of administration Advancing age (adults) Concomitant cardiac irradiation Concomitant use of cyclophosphamide, fluorouracil, dactinomycin, mithramycin, mitomycin, or vincristine Trastuzumab Older age Higher body-mass index Antihypertensive therapy Lower pre-trastuzumab left ventricular ejection fraction Concurrent anthracycline use Cumulative anthracycline dose




30 Arrhythmias
31 SINUS BRADYCARDIA Sinus bradycardia is defined as a sinus rate <60 bpm. Drugs that inhibit sinus node function resulting in sinus pauses or sinus arrest will also be included d in this section.
32
33 ATRIOVENTRICULAR (AV) NODAL BLOCKADE AV nodal blockade occurs when conduction of impulses from the atria to the ventricles through the AV node is inhibited AV nodal blockade is classified as first, second, or third degree. First degree AV nodal blockade is defined as prolongation of the PR interval to >0.2 seconds on an electrocardiogram (ECG). Second degree AV block is a progression of AV nodal dysfunction to the point at which some impulses are not conducted from the atria to the ventricles. Thi d d AV d l bl k d f f d l Third degree AV nodal blockade, often referred to as complete heart block or AV dissociation, is defined by the absence of a relationship between atrial and ventricular depolarization
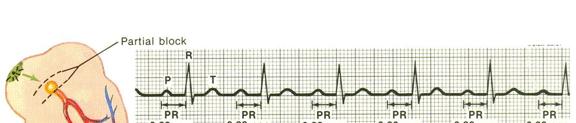
34



35 Mobitz type I second degree AV nodal blockade associated ated with phenylpropanolamine. p o a e.



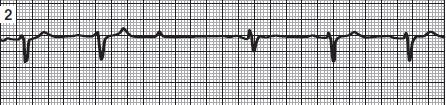
36 Mobitz type II second degree AV nodal blockade associated with amiodarone




37 Third degree AV nodal g blockade associated with carbamazepine.
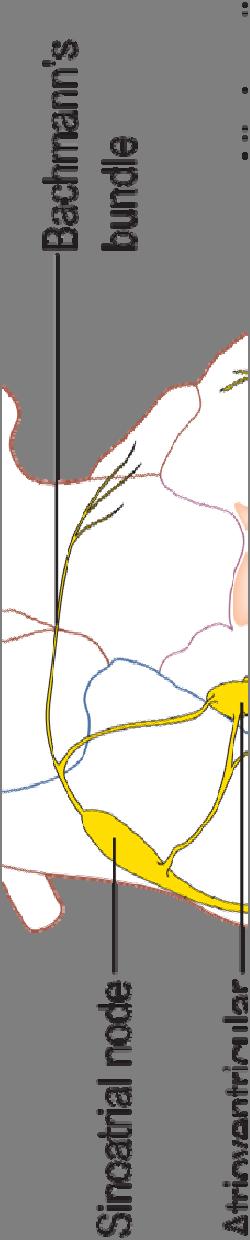
38 MECHANISMS Drug-induced sinus bradycardia may be caused by inhibition of automaticity of the node, slowing of sinus node conduction, or prolongation of sinus node repolarization AV nodal blockade may be caused by agents that inhibit AV node conduction or prolong AV node repolarization Both the sinus node and the AV node are heavily influenced by sympathetic and parasympathetic nervous system activity. The action potentials of both the sinus node and the AV node depend primarily on calcium and sodium flux, and calcium or sodium channel inhibitors may cause sinus bradycardia, AV nodal blockade, or both







39
40





41
42 CLINICAL PRESENTATION First degree AV nodal block is a common electrocardiographic phenomenon that is almost always asymptomatic. Second or third degree AV nodal blockade may result in bradycardia, with heart rates in the range of bpm. Symptoms of second or third degree AV nodal blockade are the same as those associated with sinus bradycardia Dizziness Light-headedness Fatigue Weakness Syncope Chest pain Symptoms of heart failure
43 Risk Factors for Drug-Induced Sinus Bradycardia or Atrioventricular (AV) Nodal Blockade Sinus bradycardia Pretreatment heart rate <60 bpm Underlying sinus-node dysfunction (may occur with advancing age) Concomitant use of >1 sinus-node node inhibiting drug Elevated plasma drug concentrations due to organ dysfunction or drug interactions Atrioventricular nodal blockade Concomitant use of >1 AV nodal blocking drug Pretreatment PR interval >0.2 sec Underlying AV nodal disease (may occur with advancing age) Elevated plasma drug concentrations due to organ dysfunction or drug interactions Hypothyroidism y (may be a risk factor for amiodarone-induced AV block)
44 Approaches to Help Prevent Drug- Induced Sinus Bradycardia and Atrioventricular (AV) Nodal Blockade For all drugs that may cause sinus bradycardia, AV block, or both Patient should take pulse daily, report if <50 bpm. Do not exceed maximum daily doses. Use combinations of drugs that may cause sinus bradycardia or AV block only when necessary and when the benefits likely outweigh the risks. Avoid sinus or AV node inhibiting drugs in patients with underlying sinus node dysfunction, unless a functioning pacemaker is present (in the case of AV node inhibiting drugs, there must be a functioning ventricular pacemaker).
45 For digoxin Measure serum digoxin concentrations: If kidney function is changing. If a drug that interacts with digoxin is added to therapy. Every 6 mo if there is no organ dysfunction or concomitant use of interacting drugs.
46 Torsades de point
47 Torsades de pointes is a potentially life-threatening ventricular tachyarrhythmia associated with prolongation of the QT interval QT interval prolongation and torsades de pointes may be congenital or acquired. Acquired torsades de pointes is most often caused by drugs Torsades de pointes associated with intravenous haloperidol
48 Drug induced Tdp Antiarrhythmic drugs associated with torsade include the following: Class IA - Quinidine, disopyramide, procainamide Class III - Sotalol, amiodarone (rare), ibutilide, dofetilide Nonantiarrhythmic agents can also exhibit potassiumchannel inhibitory properties and can prolong the QTc interval. Most of these drugs, including erythromycin, clarithromycin, fluoroquinolones, azole antifungals, methadone, tricyclic antidepressants, and antipsychotics, cause QTc interval prolongation by inhibiting the inwardly rectifying potassium ion channel, just like quinidine and sotalol
49 Guidelines suggest that the risk ofqtc prolongation is greater with certain antipsychotic agents, such as thioridazine, ziprasidone, and risperidone, haloperidol (when given parenterally or in high doses) QTc prolongation with perphenazine, clozapine, olanzapine, Q p g p p, p, p, quetiapine, aripiprazole appears to be minimal





50 Symptoms associated with torsades de pointes are similar to those of other tachyarrhythmias y and are related to heart rate and resulting effects on blood pressure and cardiac output. Although torsades de pointes is sometimes transient, self-limiting, and spontaneously terminating, it can degenerate into ventricular fibrillation and cause sudden cardiac death.
51 Diagnosis The diagnosis of torsades de pointes is dependent on the ECG. Torsades de pointes is a specific polymorphic ventricular tachycardia associated with prolongation of the QTc interval in the sinus beats that precede the arrhythmia Torsades de pointes, or twisting of the points, is characterized by the apparent twisting of the wide QRS complexes around the isoelectric baseline. A characteristic feature of torsades de pointes is a long short initiating sequence
52
53
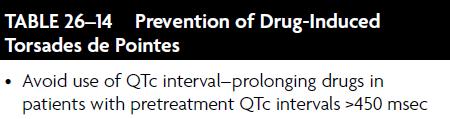
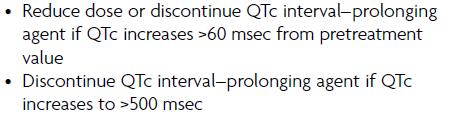
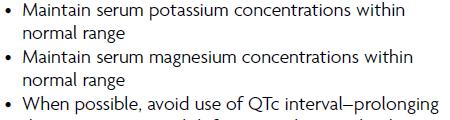
54 Prevention of Drug-Induced Torsades de Pointes Avoid use of QTc interval prolonging drugs in patients with pretreatment QTc intervals >450 msec Reduce dose or discontinue QTc interval prolonging agent if QTc increases >60 msec from pretreatment value Discontinue QTc interval prolonging agent if QTc increases to >500 msec Maintain i serum potassium concentrations ti within normal range Maintain serum magnesium concentrations within normal range When possible, avoid use of QTc interval prolonging drugs in patients with left ventricular systolic dysfunction, especially in patients with LVEF <20% who have been diagnosed with one of the
55 Adjust doses of renally eliminated QTc interval prolonging drugs in patients with kidney disease Avoid use of hepatically metabolized QTc interval prolonging drugs in patients with advanced liver disease Avoid drug interactions involving QTc interval prolonging drugs that are substrates of the cytochrome P-450 enzyme system and cytochrome P-450 enzyme inhibitors Avoid concomitant administration of QTc interval prolonging drugs Avoid use of QTc interval prolonging drugs in patients with a history of drug-induced torsades de pointes Avoid use of QTc interval prolonging drugs in patients
56 Intravenous erythromycin doses of 1g every 6 hours should be avoided, unless Legionella pneumophila infection is documented. The maximum daily dose of intravenous haloperidol should not exceed 35 mg all patients on methadone therapy should undergo a pretreatment ECG for determination of the QTc interval, a follow-up 12-lead ECG for determination of the QTc interval within 30 days of the initiation of methadone treatment, and a 12-lead ECG for QTc interval determination annually. More intensive QTc interval monitoring is recommended for patients who require daily methadone doses greater than 100 mg, and for those that experience unexplained syncope or seizures
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
PHARMACOLOGY OF ARRHYTHMIAS
 PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
(D) (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased
 (E) (F) 6. The extrasystolic beat would produce (A) increased pulse pressure because contractility. is increased. increased") Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Review Test 1. A 53-year-old woman is found, by arteriography, to have 5% narrowing of her left renal artery. What is the expected change in blood flow through the stenotic artery? Decrease to 1 2 Decrease
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Antiarrhythmic Drugs 1/31/2018 1
 Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Mr. Eknath Kole M.S. Pharm (NIPER Mohali)
") M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
12/19/16. Disclosures
 @atriumrx Don t Miss a Beat! Practical Tips on Managing Drug-Induced QTc Prolongation Sandeep Devabhakthuni, PharmD, BCPS- AQ Cardiology Assistant Professor University of Maryland School of Pharmacy Disclosures
@atriumrx Don t Miss a Beat! Practical Tips on Managing Drug-Induced QTc Prolongation Sandeep Devabhakthuni, PharmD, BCPS- AQ Cardiology Assistant Professor University of Maryland School of Pharmacy Disclosures
CVD: Cardiac Arrhythmias. 1. Final Cardiac Arrhythmias_BMP. 1.1 Cardiovascular Disease. Notes:
 CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Antiarrhythmic Drugs Öner Süzer
 Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 09.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 09.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Structure and organization of blood vessels
 The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
REGULATION OF CARDIOVASCULAR SYSTEM
 REGULATION OF CARDIOVASCULAR SYSTEM Jonas Addae Medical Sciences, UWI REGULATION OF CARDIOVASCULAR SYSTEM Intrinsic Coupling of cardiac and vascular functions - Autoregulation of vessel diameter Extrinsic
REGULATION OF CARDIOVASCULAR SYSTEM Jonas Addae Medical Sciences, UWI REGULATION OF CARDIOVASCULAR SYSTEM Intrinsic Coupling of cardiac and vascular functions - Autoregulation of vessel diameter Extrinsic
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Chapter 14. Agents used in Cardiac Arrhythmias
 Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
During exercise the heart rate is 190 bpm and the stroke volume is 115 ml/beat. What is the cardiac output?
 The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
Pharmacology. Drugs affecting the Cardiovascular system (Antianginal Drugs)
") Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Electrical Conduction
 Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
Collin County Community College
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Where are the normal pacemaker and the backup pacemakers of the heart located?
 CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification
 Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Fundamentals of Pharmacology for Veterinary Technicians Chapter 8
 Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Physiology Chapter 14 Key Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Physiology Chapter 14 Key Blood Flow and Blood Pressure, Plus Fun Review Study Guide 1 Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical Application
Physiology Chapter 14 Key Blood Flow and Blood Pressure, Plus Fun Review Study Guide 1 Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical Application
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Antiarrhythmic Drugs Öner Süzer
 Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.01.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.01.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Chapter 20 (2) The Heart
 The Heart") Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
BUSINESS. Articles? Grades Midterm Review session
 BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
BUSINESS Articles? Grades Midterm Review session REVIEW Cardiac cells Myogenic cells Properties of contractile cells CONDUCTION SYSTEM OF THE HEART Conduction pathway SA node (pacemaker) atrial depolarization
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets
 METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ. ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C
 ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
The Cardiovascular System
 The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
The Cardiovascular System The Cardiovascular System A closed system of the heart and blood vessels The heart pumps blood Blood vessels allow blood to circulate to all parts of the body The function of
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Drug Therapy of Heart Failure. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1
 Lecture 14 Cardiovascular control mechanisms p. 1") BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
CARDIOVASCULAR SYSTEM
 CARDIOVASCULAR SYSTEM 1. Resting membrane potential of the ventricular myocardium is: A. -55 to-65mv B. --65 to-75mv C. -75 to-85mv D. -85 to-95 mv E. -95 to-105mv 2. Regarding myocardial contraction:
CARDIOVASCULAR SYSTEM 1. Resting membrane potential of the ventricular myocardium is: A. -55 to-65mv B. --65 to-75mv C. -75 to-85mv D. -85 to-95 mv E. -95 to-105mv 2. Regarding myocardial contraction:
Is There a Genomic Basis to Acquired Channelopathic disease
 Is There a Genomic Basis to Acquired Channelopathic disease Yaniv Bar-Cohen, M.D. Associate Professor of Pediatrics Division of Cardiology / Electrophysiology Children s Hospital Los Angeles Keck School
Is There a Genomic Basis to Acquired Channelopathic disease Yaniv Bar-Cohen, M.D. Associate Professor of Pediatrics Division of Cardiology / Electrophysiology Children s Hospital Los Angeles Keck School
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Antiarrhythmics & QT Prolongation: Avoiding Drug Interactions
 Antiarrhythmics & QT Prolongation: Avoiding Drug Interactions M E L I N D A D E U B N E R, P H A R M D, B C C C P A w e b i n a r f o r H e a l t h T r u s t m e m b e r s A u g u s t 2 4, 2 0 1 8 Disclosures
Antiarrhythmics & QT Prolongation: Avoiding Drug Interactions M E L I N D A D E U B N E R, P H A R M D, B C C C P A w e b i n a r f o r H e a l t h T r u s t m e m b e r s A u g u s t 2 4, 2 0 1 8 Disclosures
Vasospasm and cardiac ischemia (Type 3 ) Hypertension Hypotension Arrhythmias Miscellaneous ( pericardial inflammation, valvular abnormalities )
 Hypertension Hypotension Arrhythmias Miscellaneous ( pericardial inflammation, valvular abnormalities )") Management of Cardiotoxicity due to Systemic Cancer Therapy Left Ventricular Dysfunction Type 1 cardiac dysfunction Type 2 cardiac dysfunction Vasospasm and cardiac ischemia (Type 3 ) Hypertension Hypotension
Management of Cardiotoxicity due to Systemic Cancer Therapy Left Ventricular Dysfunction Type 1 cardiac dysfunction Type 2 cardiac dysfunction Vasospasm and cardiac ischemia (Type 3 ) Hypertension Hypotension
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia