Post-infectious (bacterial) Glomerulonephritis
|
|
|
- Alexia Manning
- 5 years ago
- Views:
Transcription

 Glomerulonephritis (An")

1 Far East Regional Conference Russia Dialysis Society Khabarovsk, Russia October 30, 2015 Post-infectious (bacterial) Glomerulonephritis (An Update) William Couser, MD Affiliate Professor of Medicine University of Washington Seattle, WA USA


2 Post-streptococcal GN (PSGN) LM IF-IgG IF-C3 EM

3 PSGN diffuse proliferative and exudative GN From Rennke ASN BRC 2011



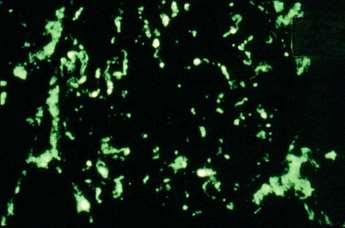
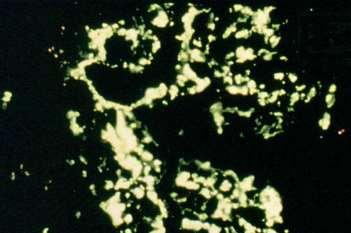
4 PSGN IF: 1+ IgG, 3+ C3 A C3 nephropathy IgG Modified from Nephpath.com C3

5 Subepithelial humps in PSGN PMN Subendothelial deposits in PSGN

 Strep")
6 ETIOLOGY OF PSGN Strep pharyngitis (40%) Strep pyoderma (60%)

7 Perio Peri-orbital edema in 10 yo boy with acute, poststreptoccocal GN
8 Typical time course of symptoms and lab values in PSGN C3 ASOT Hematuria HTN, edema

9 Post-strep GN in adults today (109 cases) Changing epidemiology and outcomes Incidence About 12% of exposed people get clinical GN 25% of exposed people or family members get subclinical GN Clinical features Bottom line: Mean peak creatinine 5.1 mg/dl As the population ages and epidemic cases decrease 46% required dialysis with improved Longest time hygiene, on dialysis PSGN with full in recovery adults is 38 is days. becoming a disease of greater severity, worse prognosis and often Low complement 72% Indications affecting older, for biopsy mostly immunocompromised men. Anuria > 24 hrs Oliguria > 7 days Atypical laboratory results or clinical picture. Recovery (3 months) Complete: 22% Partial-CKD 44% ESRD 33% Kanjanabuch, Nat Rev Nephrol 5:259, 2009; Nasr et al, JASN 22: 187, 2011
10 Post-streptococcal nephritis Can you make the diagnosis serologically? Test Sensitivity Specificity Duration Increased ASO Titer Increased Streptozyme Low complement (alternate or MBL pathway) 75% Only for infection 6-8 weeks >90% Only for infection 6-8 weeks >90% (First 2 weeks) Cryoglobulins 20% Rheumatoid factor 20% No (C3 nephropathies) Any chronic inflammation Several collagen vascular diseases 4-8 weeks 4 weeks 4 weeks
11 Differential diagnosis of renal diseases with fluid phase C activation ( low serum complement levels) Disease Pathway Serum C levels Other SLE Classical Low C1,C4,C2,C3, CH 50 ANA, anti-dsdna MPGN I Classical Low C1,C4,C3, CH 50 Anti-HCV, cryos, rheumatoid factor Chronic infection (SBE, shunt nephritis, IgA dominant PIGN Classical Low C1,C4,C3, CH 50 Bacterial infection Cryoglobulins Rheumatoid factors Post-strep GN Alternative Normal C1,C4,C2 Very low C3, CH 50 ASOT, streptozyme C3 GN Alternative Normal C1,C4,C2 Low C3, CH 50 C3-nephritic factors, Abnormal C regulatory proteins

")
12 Post-streptococcal GN: Typical clinical course derived mostly from pediatric studies Sign Resolution Diuresis 1 week Hypertension 2 weeks Cr to normal longest on 3-4 weeks HD=38 days Low C3 6-8 weeks, longest 9 mos EM humps 6-7 weeks Hematuria 3-6 weeks Proteinuria 3 years: 15%, 10 years: 2% Acute renal failure 5% CKD: up to 20% (Sinha et al NDT ) ESRD: 2.5%
13 Outcomes of PSGN with >50% crescents and AKI in children Patients: Although it is a reasonable clinical 27 option, kids, mean there age 8.7 is yrs, no mean data Scr to 3.9 mg/dl. demonstrate that steroid pulse Treatment therapy given to patients with acute, 18 pulsed, 6 pulse steroids/ctx, 8 required dialysis. crescentic PSGN accelerates Outcomes: recovery, improves recovery rate or 22 alters recovered long to normal term GFR, outcome. 2 CKD, 3 ESRD Only outcome predictor: Need for dialysis Jellouli et al. Nephrol Ther (Epub )
")
14 Long term prognosis in PSGN (4021 patients, 5-18 yr FU) ESRD is an uncommon outcome Any abnormality 17% Proteinuria 14% Hypertension 14-45% Reduced GFR 1.3% From Rodriguez-Iturbe et al JASN 19:1855, 2008; Pinto et al. PLOS 1 (Epub )
: Males: 4.1 Females: 3.1 + PSGN history Hoy W et al. NDT (Epub 7-24-14); Hoy et al Kidney int 81:1026, 2012")
15 History of PSGN > 5 yrs ago increases CKD later in life Hazard ratios of a history of PSGN from impetigo for developing ACR >34 (overt albuminuria): Males: 4.1 Females: PSGN history Hoy W et al. NDT (Epub ); Hoy et al Kidney int 81:1026, 2012
16 What are the major risk factors for CKD and ESRD due to PSGN? Epidemic (low) vs sporadic (higher) Children (low, 1%) vs adults (10-35%) Age (>60, 75% have CKD) Severity (Crescents, AKI) (50%) Proteinuria after 12 mos Persistent low C3 beyond 6 weeks
17 Atypical post-infectious GN Acute onset of nephritic syndrome with persistent proteinuria, hematuria Bottom line: Persistent low C3 with normal C4 beyond 3 mos. Some (? many) cases of GN following infectious Proliferative episodes GN with have subepithelial C3 nephropathies humps on rather biopsy than immune complex GN. These IF staining patients for C3 do > not IgG fully recover. Examples 11/11 patients of complement tested had regulatory abnormalities protein abnormalities regulation of associated the complement with more AP severe disease C3 Nephritic have now factor been positive reported 7/11 in SLE and IgA nephropathy as well. CFH mutations 4/11 Sethi et al. Kidney Int 83:293, 2013
18 Treatment of PSGN There is no KDIGO guideline for treating acute PSGN because most patients recover spontaneously and need only supportive care. Steroid pulse therapy can be considered in patients with persistent AKI and a crescentic lesion on biopsy. There is one case report of a dramatic and immeadiate response to Eculizumab in a 10 yo girl with classical acute PSGN, elevated ASOT, oliguric ARF (Scr 6.4) and crescents who did not respond to pulse steroids. (Sharma et al. ASN abstract 2014)

19 Non-streptococcal post-infectious GN is now called Infection-related GN (IRGN) Clinical features Now 34% age >65 35% have a co-morbid condition: Diabetes (15%), cancer, alcoholism, cirrhosis, immunosuppression, HIV, IVDA, malnutrition 50% of cases are subclinical 20-40% nephrotic at the outset Increasing incidence of IgA-dominant PIGN Older males Diabetic or other co-morbid conditions Acute renal failure Only 30-70% low C % CKD (60% if sporadic) Overall ESRD 10-20%, 50% if diabetic Nasr et al: Medicine 87:21, 2008; Nast: Am J CKD 12:68, 2012
 Upper respiratory 23% Skin 18% Lung 18% Endocarditis 12% Organisms (Mostly Staph) Staph 46% Strep 16% Gram negatives % 10% Nasr S et al: JASN")
20 Infection-related GN in adults (109 cases) Changing demographics Risk factors (61% immunocompromised) Age >64 64% Diabetes 29% Cancer 5% HIV 2% IVDU 1% Sites of infection (Diverse) Upper respiratory 23% Skin 18% Lung 18% Endocarditis 12% Organisms (Mostly Staph) Staph 46% Strep 16% Gram negatives % 10% Nasr S et al: JASN 22:187, 2011

21 Site of Infection % Upper respiratory 23 Pneumonia 17 Skin Endocarditis Infection-related GN Sites of infection Osteomyelitis 5 Urinary Tract 5 Abscess 2 Vertriculo-peritoneal shunt 1 Phlebitis Unknown 16 Nasr et al. Medicine 87: 21, 2008
22 Clinical features Serum Cr at biopsy Mg/dl Mean Proteinuria G/day Nephrotic Syndrome (%) Infection-related GN Clinical features Without diabetes (N=70) With diabetes (N=16) Hematuria Low C3 or C Nasr et al. Medicine 87:21, 2008

23 Infection-related GN Outcomes (52 pts, mean FU 25 mos Outcome DM - DM + Complete recovery 56% 0% CKD 27% 18% ESRD 17% 82% Nasr et al, Medicine 87:21, 2008

24 Acute infection-related GN Also think of: IgA-dominant post-infectious GN Bacterial endocarditis Shunt nephritis Nephritis with visceral abscesses


25 Post-staphlococcal IgA-dominant infection-related GN Older male, MRSA, diabetic, AKI IgA From Haas et al, Human Path 39, 1309, 2008
 Often older diabetics, usually male 50% have low C3 IgA/C3 by IF, deposits at all 3 sites by")

26 IgA- dominant infection-related GN RPGN, AKI, nephrotic syndrome (30%) Usually Staph infection, esp. MRSA (68%) Often older diabetics, usually male 50% have low C3 IgA/C3 by IF, deposits at all 3 sites by EM, usually include humps Differentiate from IgA by risk factors, infection history, humps, and usually more severe disease. Treatment: Antibiotics Satoskar et al, CJASN 1:1179, 2006; Wehbe et al NDT Plus 4:181, 2011
27 Clinical features of IgA-dominant post-infectious GN (78 patients, 28 reports) Clinical features Pathology: humps 100% Hematuria 97% Proteinuria 96% AKI 85% Active infection 100% Outcomes (after antibiotic therapy) GFR improved: 55% Persistent CKD: 12% ESRD 20% Died 14% Risk Factors for death/esrd: Age, diabetes Bu et al. Am J Nephrol. 41:98, 2015

28 Can/should IgA-dominant postinfectious GN be treated with steroids? Recommendation: Consider steroids (with antibiotics) if: OUTCOMES NUMBERS Total number reviewed Improved >30% crescents, with steroids acute interstial nephritis 15 or diffuse proliferative GN with progression. Remained dialysis-dependent 3 Outcomes Died 2. No improvement after 6 weeks of antibiotics. 3. Nephrotic-range Alive (1 year) proteinuria. 4 (3 from sepsis after steroids) 13 Eswarappa, et al. Use of steroid therapy in immunoglobulin A-dominant poststaphylococcal glomerulonephritis (Review). Hong Kong J Nephrol 24:336, 2014
29 Bacterial endocarditis-related GN (1) Demographics: 49 adult cases, 4:1 male, Mean age 48, 30% over 60 Presentation AKI (80%), acute GN (20%) Co-morbidities Cardiac valve disease (26%) (TC>MV>AV) 50% of infected valves are prosthetic IV drug abuse (18%) HCV (20%), Diabetes (18%) Organisms Staph 55% (MRSA 39%) Strep (24%) Boils, Couser et al. Renal Disease in Infective Endocarditis. An Update on Clinical and Pathologic Features. Kidney Int 87:1241, 2015
30 Bacterial endocarditis-related GN (2) Labs Hypocomplementemia (56%) (low C3, normal C4 = AP) Positive ANCA 28% Positive ANA 15% Pathology Focal necrotizing GN (78%) with crescents (55%) Diffuse proliferative GN (33%) C3 (100%); IgG (26%), IgA (29%) EM: 14% classical humps Boils, Couser et al. Renal Disease in Infective Endocarditis. An Update on Clinical and Pathologic Features. Kidney Int 87:1241, 2015
 May also develop AKI, allergic")
31 Shunt nephritis Chronic infection on ventriculoatrial or ventriculojugular shunts for hydrocephalus About 30% of shunts get infected, % of infected shunts get GN over 2 mos to many years Staph epidermidis, Staph aureus most common Chronic fever with hematuria and sometimes nephrotic syndrome (30%) May also develop AKI, allergic interstitial nephritis, TMA Biopsy: MPGN type I C-ANCA can be positive and justify steroids Treatment: Shunt removal, 4-6 weeks of antibiotics Iwata et al. Am J Kidney Dis. 43: e11-6, 2004
32 GN with occult visceral abscess Crescentic RPGN with AKI Abscess usually intra- abdominal or intrathoracic Serologies negative, C low in 40%, cryos may be positive. No glomerular immune deposits by IF or EM Blood cultures negative Treatment: May respond to steroids if no resolution with antibiotics Beaufils et al, NEJM 295:185, 1976, Clin Nephrol; 70:344, 2008
33 Many forms of GN may be post-infectious (Reviewed in Couser W, Johnson RJ. The etiology of glomerulonephritis: Roles of infection and autoimmunity Kidney Int 86:905-14, 2014) Post-streptococcal GN Nephritogenic streptococcal antigen (SpeB) activates complement directly through the MBL pathway. IgA nephropathy IgA dominant post-staph GN in older male diabetics Enteric microbiome activates TLR4 to induce abnormally glycosylated IgA 1 and anti-glycan antibodies. Anti-GBM disease Molecular mimicry between anti-gbm T cell epitope Pcol on gram negative organisms, esp. C bolinulum, induces autoimmunity to GBM antigen
34 Many forms of GN may be post-infectious (Reviewed in Couser W, Johnson RJ. The etiology of glomerulonephritis: Roles of infection and autoimmunity Kidney Int 86:905-14, 2014 and Expanding the domain of post-infectious GN, Amer J Kidney Dis 66:725, 2015) ANCA-positive vasculitis Staph or viral infections commonly precede MPA and GPA and molecular mimicry has been shown to lead to anti-complementary PR3 antibody linked to pathogenesis Molecular mimicry with fimbrial antigen on gram negative bacteria (FimH) induces HLAMP2 antibody that has ANCA and anti-endothelial reactivity and induces pauci-immune GN. Idiopathic minimal change/focal sclerosis Pathogen- associated molecular patterns (PAMPS) via TLR4 upregulate podocyte CD80 and induce T cells to release permeability factors Membranoproliferative glomerulonephritis, Type I HCV antigen-c1q form TLR4 agonist that activates mesangial cells to proliferate and B cells to make cryoglobulins with rheumatoid factor activity
35 Thank you! спасибо spasibo
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta
 Anjali Gupta") POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Infection related Glomerulonephritis. Asanga Abeyaratne Nephrologist, Royal Darwin Hospital
 Infection related Glomerulonephritis Asanga Abeyaratne Nephrologist, Royal Darwin Hospital 1 Overview Epidemiology Definitions Post-infectious (PIGN) vs. Infection related (IRGN) Post-infectious (PIGN)
Infection related Glomerulonephritis Asanga Abeyaratne Nephrologist, Royal Darwin Hospital 1 Overview Epidemiology Definitions Post-infectious (PIGN) vs. Infection related (IRGN) Post-infectious (PIGN)
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Objectives. Glomerular Diseases. Glomerulonephritis. Microscopic Hematuria 11/6/2016. Discuss diagnosis of glomerular diseases
 Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
Glomerulonephritis Associated with Bacterial Infection
 Glomerulonephritis Associated with Bacterial Infection The Emerging Role of Staphylococcus Tibor Nádasdy, MD Clinical history (Case #1) 60-year-old Caucasian male with insulin dependent DM, diabetic
Glomerulonephritis Associated with Bacterial Infection The Emerging Role of Staphylococcus Tibor Nádasdy, MD Clinical history (Case #1) 60-year-old Caucasian male with insulin dependent DM, diabetic
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
From MPGN to C3G. F Fakhouri, Nantes, France. «Membranoproliferative» is a pathological feature. Mesangial expansion «Doubles contours»
 From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
From MPGN to C3G F Fakhouri, Nantes, France Conflits d intérêt: consultant auprès d Alexion Pharmaceuticals «Membranoproliferative» is a pathological feature Mesangial expansion «Doubles contours» Immune
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016
 GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016 Wayne R. Kotzker, M.D. Renal Electrolyte & Hypertension Consultants of South Florida Affiliate Assistant Professor of Clinical Biomedical Sciences,
GLOMERULONEPHRITIS BRRH Grand Rounds January 12, 2016 Wayne R. Kotzker, M.D. Renal Electrolyte & Hypertension Consultants of South Florida Affiliate Assistant Professor of Clinical Biomedical Sciences,
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
1. SIGNIFICANCE 2. PREREQUISITES
 Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU
 Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Rapidly progressive glomerulonephritis. Alan Salama UCL Centre for Nephrology Royal Free Hospital
 Rapidly progressive glomerulonephritis Alan Salama UCL Centre for Nephrology Royal Free Hospital Remember this. AKI Acute tubular injury Not all AKI is caused by sepsis or volume depletion AKI is caused
Rapidly progressive glomerulonephritis Alan Salama UCL Centre for Nephrology Royal Free Hospital Remember this. AKI Acute tubular injury Not all AKI is caused by sepsis or volume depletion AKI is caused
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Clinical spectrum and outcome of crescentic glomerulonephritis in children in developing countries
 Pediatr Nephrol (2008) 23:389 394 DOI 10.1007/s00467-007-0647-3 ORIGINAL ARTICLE Clinical spectrum and outcome of crescentic glomerulonephritis in children in developing countries Deepak Dewan & Sanjeev
Pediatr Nephrol (2008) 23:389 394 DOI 10.1007/s00467-007-0647-3 ORIGINAL ARTICLE Clinical spectrum and outcome of crescentic glomerulonephritis in children in developing countries Deepak Dewan & Sanjeev
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018
 GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
AN APPROACH TO HEMATURIA. Dr Saima Ali
 AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Pathogenesis of IgA Nephropathy. Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS
 Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
Glomerular Disease. January 16, Katharine Dahl, MD
 Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Clinicopathologic Features of IgA-Dominant Postinfectious Glomerulonephritis
 The Korean Journal of Pathology 2012; 46: 105-114 ORIGINAL ARTICLE Clinicopathologic Features of IgA-Dominant Postinfectious Glomerulonephritis Tai Yeon Koo Gheun-Ho Kim Moon Hyang Park 1 Departments of
The Korean Journal of Pathology 2012; 46: 105-114 ORIGINAL ARTICLE Clinicopathologic Features of IgA-Dominant Postinfectious Glomerulonephritis Tai Yeon Koo Gheun-Ho Kim Moon Hyang Park 1 Departments of
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1
 Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
 Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Basic and Translational Concepts of Immune-Mediated Glomerular Diseases
 Basic and Translational Concepts of Immune-Mediated Glomerular Diseases William G. Couser Division of Nephrology, Department of Medicine, University of Washington School of Medicine, Seattle, Washington
Basic and Translational Concepts of Immune-Mediated Glomerular Diseases William G. Couser Division of Nephrology, Department of Medicine, University of Washington School of Medicine, Seattle, Washington
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers
 Pediatr Nephrol (2018) 33:65 69 DOI 10.1007/s00467-017-3626-3 CLINICAL QUIZ Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers Farah A. Falix 1 & Michiel J. S. Oosterveld 1 & Sandrine
Pediatr Nephrol (2018) 33:65 69 DOI 10.1007/s00467-017-3626-3 CLINICAL QUIZ Diagnostic dilemmas in a girl with acute glomerulonephritis: Answers Farah A. Falix 1 & Michiel J. S. Oosterveld 1 & Sandrine
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Clinico-histopathological correlation of Nephritic Syndrome in adults in urban population
 Original article: Clinico-histopathological correlation of Nephritic Syndrome in adults in urban population 1 Dr. Saurabh Ajit Deshpande, 2 Dr. Keshav Kale, 3 Dr. Nivedita D. Moulick 1Resident, Department
Original article: Clinico-histopathological correlation of Nephritic Syndrome in adults in urban population 1 Dr. Saurabh Ajit Deshpande, 2 Dr. Keshav Kale, 3 Dr. Nivedita D. Moulick 1Resident, Department
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Spectrum of Renal Involvement in Patients of Obstetrical and Gynaecological Disorders Presenting with Renal Abnormalities
 International Journal of Medical Research Professionals Spectrum of Renal Involvement in Patients of Obstetrical and Gynaecological Disorders Presenting with Renal Abnormalities Original Article Sharma
International Journal of Medical Research Professionals Spectrum of Renal Involvement in Patients of Obstetrical and Gynaecological Disorders Presenting with Renal Abnormalities Original Article Sharma
Russia Dialysis Society Peterhof, Russia June 8, 2016
 Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,
Russia Dialysis Society Peterhof, Russia June 8, 2016 TREATMENT OF GLOMERULONEPHRITIS XV Северо-Западная ( AAV, SLE, Нефрологическая Membranous) Школа What s changed in the past decade? William Couser,