Polling Question #1. Risk Adjustment in the Inpatient Hospital Setting
|
|
|
- Marshall Weaver
- 5 years ago
- Views:
Transcription



 in addition to")
 in addition to SOI/ROM and O/E No, we do not")
1 1 Risk Adjustment in the Inpatient Hospital Setting Mark N. Dominesey, RN, BSN, MBA, CCDS, CDIP, CHTS CP Manager of CDI Children s National Medical Center Washington, DC 2 Polling Question #1 Does your facility educate inpatient physicians, coders, and CDI professionals on risk methodologies? Yes, we educate on APR DRG (SOI/ROM) only Yes, we educate on observed to expected ratios (O/E) in addition to SOI/ROM Yes, we educate on HCC based methodologies (MSPB, MA plans) in addition to SOI/ROM and O/E No, we do not educate physicians on risk methodologies at this time 3 1

2 4 Learning Objectives At the completion of this educational activity, the learner will be able to: Identify three risk adjustment schemes Describe the HCC risk adjustment scheme and which inpatient quality programs it impacts Detail at least five secondary diagnoses that impact inpatient risk adjustment Inpatient Risk Adjustment VS. My hospital s patients are sicker than their hospital s patients Oh brother, not again! My hospital s complication rate cannot be compared to their hospital s complication rate because my hospital s patients are at higher risk for adverse outcomes. Image source: 5 Why Should CDI Be Interested in Risk Adjustment? healthgrades publishes list their 100 best hospitals
3 7 Risk Adjustment Concepts Definition of risk adjustment A methodology used to adjust for clinically relevant patient factors outside of the hospital s control such as demographic characteristics, comorbidities, and patient frailty (think of handicapping ) Why is risk adjustment needed? Compares providers, organizations, and payers Encourages the continued documentation of resource intensive chronic conditions Ensures proper allocation of funds and resources for treatment Facilitates more accurate comparisons by accounting for differences in case mix Fee for Service Payment/PhysicianFeedbackProgram/Downloads/Risk Adjustment Fact Sheet.pdf fee for service payment/acuteinpatientpps/readmissions reduction program.html Risk Adjustment Concepts What is the intent of risk adjustment? To accurately reflect the health of the patient population, adjusting for outcome measures such as Mortality Readmissions Complications Length of stay Resource utilization Costs Fee for Service Payment/PhysicianFeedbackProgram/Downloads/Risk Adjustment Fact Sheet.pdf fee for service payment/acuteinpatientpps/readmissions reduction program.html 8 Methodologies That Use Risk Adjustment APR DRG Hierarchical Condition Categories CMS (Medicare) and HHS (ACA) (HCCs) AHRQ (PSI 90) Hospital Compare/Physician Compare University Hospital Consortium (UHC) Joint Commission s ORYX (Healthchek) Others (U.S. News, Truven, MedeAnalytics, CareScience, etc.) 9 3
 or a major comorbid")
4 10 Why the Focus on Inpatient Risk Adjustment? We capture CCs and MCCs! Isn t that enough? What? Are you joking? MS DRG is intended to be a reimbursement mechanism only MS DRGs only provide a limited ability to integrate risk adjustment one, two, or three tiers Once a comorbid condition (CC) or a major comorbid condition (MCC) is coded, there are no additional financial incentives to document more comorbid conditions Opportunity lost in increasing patient, provider, and hospital severity and risk Image Sources: Universally Accessible Risk Adjustment The APR DRG Risk Adjustment Model The All Patient Refined Diagnosis Related Group (APR DRG) model was created by 3M to provide greater insight into severity and risk across all populations The APR DRG system expands on MS DRGs to address patient severity of illness (SOI) and risk of mortality (ROM) Severity of illness (SOI) relates to the extent of physiologic decompensation or organ system loss of function Risk of mortality (ROM) relates to the likelihood of dying Both SOI and ROM are further divided into four subclasses: 1: Minor, 2: Moderate, 3: Major, 4: Extreme Patients with high subclass levels are usually characterized by multiple serious diseases or illnesses Like the MS DRG model, each APR DRG has a relative weight that can be used in CMI calculations 11 Constructing an APR DRG APR DRG Severity classification Base APR DRG Age Gender Discharge status Diagnoses Procedures Birth weight Four levels of each: Severity of illness (SOI) Risk of mortality (ROM) Source: us.ahrq.gov/db/nation/nis/apr DRGsV20MethodologyOverviewandBibliography.pdf, pg
 = high quality hospital or practitioner I want this practitioner or hospital to care for me they are better at preventing death High")
 so do quality")
5 13 Observed to Expected Mortality Image source: Why Measure Mortality? Patients Low mortality rates (expressed as mortality index) = high quality hospital or practitioner I want this practitioner or hospital to care for me they are better at preventing death High mortality rates = low quality hospital Is there something wrong with this hospital/practitioner? Public perception of O/E Publicly available Quality Measures are displayed in many publications and venues The public makes judgments based on old data (two years in some cases) so do quality agencies 14 Calculating Observed to Expected (O/E) Ratios Example: Mortality We will walk through using O/E for measuring mortality, but the concept applies no matter the outcome measured (mortality, readmissions, LOS, cost, severity, complications) The number, expressed as a fraction or a ratio, represents actual mortality rates to the expected rate of mortality for that practitioner, hospital, or organization. The "observed to expected mortality" rate is a risk adjusted measure of a hospital's mortality rate. This ratio is created from two sets of numbers: Observed mortality: The actual number of patients that died in the hospital each measured time period (month, quarter, year) Expected mortality: The expected average of hospitalized patient deaths with a particular illness or condition that are beyond the control of the practitioner or organization, such as age, gender, and other medical problems Observed mortality is divided by expected mortality to create the O/E ratio The meaning of an O/E ratio depends on the score: Equal to 1.5. The hospital's mortality rate is higher than expected. Equal to 1.0. The hospital's mortality rate is equal to what is expected. Equal to The hospital's mortality rate is 25% lower than expected. Equal to The hospital's mortality rate is 50% lower than expected. A lower score typically represents higher quality care 15 5
6 16 Denominator Issues Expected Mortality Influences: Patient acuity Expected mortality is calculated using a mathematical risk adjustment tool Robustness of risk adjustment calculation method Some are unable to capture demographic or psychosocial factors that influence mortality risk (e.g., lack of access to care) Reliability of methodology Comparison of risk adjustment models yields variable results APR DRG Mortality Drivers 17 Common Mortality Risk Adjustment Variables APR DRG ROM subclass for mortality SOI subclass for LOS and costs Patient age Patient sex Admit source = Transfer from another acute care hospital Transfer from skilled nursing Renal failure facility AIDS Long term care facility Obesity Low socio economic status Weight loss (based on Medicaid, self pay, charity as primary payer) Drug abuse Psychoses Admit status = emergency Patient race Agency for Healthcare Research and Quality (AHRQ) Comorbid conditions (not all inclusive): Congestive heart failure Pulmonary circulation disorders Hypertension (complicated and uncomplicated) Chronic pulmonary disease Diabetes (complicated and uncomplicated) Alcohol abuse Source: Depression patient safety/quality resources/tools/mortality/meurer.pdf 18 6
 HAC Reduction Program Hospital")
7 19 Condition Categories (Learning Example: HCCs) Image source: Where are HCCs Used in Inpatient Settings? Condition categories are used for risk adjustment in CMS quality initiatives including: Value Based Purchasing Program PSI 90 Medicare Spend Per Beneficiary (MSPB) HAC Reduction Program Hospital Compare 20 HCCs: Overview Demographic factors Carries a Risk Adjustment Factor (RAF) score Age Gender Disability status Condition Categories are diagnosis specific and each carries a RAF score Condition Categories group patients that are clinically similar (think DRGs) In some risk adjustment mechanisms, hierarchies are applied (e.g., multiple categories of diabetes, drop lower weighted category RAF) HCC risk adjustment is based on: Diagnoses RAF + Demographic (RAF) = Patient s RAF score 21 7
8 22 CMS HCC Risk Adjustment Model Patient presentation 69,000+ ICD 10 Codes 8,771 qualifying diagnoses 79 HCCs (CMS) Patient s Risk Adjustment Factor International Classification of Diseases specific diagnostic codes ICD 10 codes that contribute to HCCs Clinical syndromes with like or similar costs, outcomes, resource consumption Numeric calculation or normalization of patient s risk Risk Adjustment Example: CMS HCCs Selected ICD codes are grouped to a Condition Category ~ 8,800 ICD 10 CM codes Acute, chronic, or acute on chronic conditions ~ 75% are also MS DRG MCCs or CCs 79 Condition Categories in Version 22 model Each Condition Category has a risk value or weight/coefficient Risk values can change year to year For unrelated diseases, Condition Categories are cumulative e.g., a patient with heart disease, stroke, and cancer will have three separate Risk Adjustment Factors added together 23 HCC Risk Adjustment in Value Based Purchasing Medicare Spend Per Beneficiary (MSPB) is domainweighted for 25% of VBP (up to 0.5% penalty in 2017) MSPB is a publicly reported measure on Hospital Compare Broadly follows HCC version 22 Severity of illness is measured across 79 HCC indicators Look back period is 90 days before the encounter (to ascertain if beneficiary previously in long term care) Disease interactions are included Does not control for sex and race For unrelated diseases, Condition Categories are cumulative e.g., a patient with heart disease, stroke, and cancer will have three separate Risk Adjustment Factors added together Source: Fee for Service Payment/PhysicianFeedbackProgram/Downloads/2017 MSPBM MIF.pdf 24 8
9 25 MSPB Episode The period 3 days prior to an IPPS hospital admission (also known as the index admission ) through 30 days post hospital discharge Hospital admissions that are NOT considered as index admissions include: Admissions that occur within 30 days of discharge from another index admission Acute to acute transfers Episodes where the index admission claim has $0 payment Admissions having discharge dates fewer than 30 days prior to the end of the performance period Source: content/uploads/2016/06/mspb_slides_npc_2016may19_finalc508.pdf Calculating the MSPB Ratio MSPB amount: Sum of a hospital s standardized, risk adjusted spending across all of the hospital s eligible episodes divided by the number of episodes MSPB measure: A hospital s MSPB amount divided by the episode weighted median MSPB amount across all hospitals Normalized MSPB amount so that median MSPB measure equals 1.0 Source: content/uploads/2016/06/mspb_slides_npc_2016may19_finalc508.pdf 26 Interpreting the MSPB Ratio A ratio equal to the national average means that Medicare spends ABOUT THE SAME per patient for an episode of care initiated at this hospital as it does per episode of care across all inpatient hospitals nationally A ratio that is more than the national average means that Medicare spends MORE per patient for an episode of care initiated at this hospital than it does per episode of care across all inpatient hospitals nationally A ratio that is less than the national average means that Medicare spends LESS per patient for an episode of care initiated at this hospital than it does per episode of care across all inpatient hospitals nationally Source: Hospital Compare 27 9


10 28 HCC Risk Adjustment Contribution to MSPB Accounts for variation in patient case mix across hospitals by using a linear regression to estimate the relationship between risk adjustment variables and standardized episode cost Risk adjustment variables include factors such as age, severity of illness, and comorbidity interactions Each Major Diagnostic Category uses a separate linear regression model Source: content/uploads/2016/06/mspb_slides_npc_2016may19_finalc508.pdf Version 22 CMS HCC List 29 Disease Hierarchies for the CMS HCC Model 30 10




11 31 MSPB Risk Adjustment Variables MSPB Risk Adjustment Variables 32 Risk Adjustment in PSI 90 Image source:
12 34 Patient Safety Indicators (PSIs) Used to support CMS quality initiatives such as: Hospital Acquired Condition (HAC) Reduction Program Separate program from the Deficit Reduction Act: Hospital Acquired Conditions (Present on Admission [POA] program) Hospital Inpatient Quality Reporting (IQR) Program Hospital Value Based Purchasing (VBP) Program Measure of hospital quality of care for adult patients focusing on potentially avoidable complications and iatrogenic effects Source: PSI 90, Patient Safety and Adverse Events Composite Component PSIs of PSI 90 PSI 03 Pressure Ulcer Rate PSI 06 Iatrogenic Pneumothorax Rate PSI 08 In Hospital Fall with Hip Fracture PSI 09 Perioperative Hemorrhage and Hematoma Rate PSI 10 Physiologic and Metabolic Derangement Rate PSI 11 Postoperative Respiratory Failure Rate PSI 12 Perioperative Pulmonary Edema or Deep Vein Thrombosis Rate PSI 13 Postoperative Sepsis Rate PSI 14 Wound Dehiscence Rate PSI 15 Accidental Puncture and Laceration Rate 35 Risk Adjustment in PSI 90 Each PSI is risk adjusted by two overarching mechanisms: Exclusions (absolute risk adjustment) Risk factors as defined by the Agency for Healthcare Research and Quality (AHRQ) Rates are risk adjusted using (AHRQ) risk factor coefficients version 6.0 Source: ICD09/Parameter_Estimates_PSI_60.pdf 36 12
13 37 Strategies to Incorporate Risk Adjustment in PSI 90 Example: PSI 03 Pressure Ulcer Rate Selected exclusions (absolute risk adjustment) LOS < 3 days, transfer from hospital, SNF or ICF, MDC 14 Any listed diagnosis codes for hemiplegia, paraplegia, or quadriplegia, spina bifida, or anoxic brain damage POA major skin disorders Selected risk factor Identification Comorbid Conditions Hypertension with complications Chronic lung disease (COPD) Diabetes with and without complications Neurological conditions Renal failure AIDS/HIV Hypothyroidism Deficiency anemias Weight loss Presence of solid tumors without metastases Drug abuse Psychiatric conditions Source: ICD10/TechSpecs/PSI_03_Pressure_Ulcer_Rate.pdf Strategies to Incorporate Risk Adjustment in PSI 90 Example: PSI 06 Iatrogenic Pneumothorax Rate Selected exclusions (absolute risk adjustment) Pneumothorax POA Chest trauma, pleural effusion, cardiac procedure, thoracic surgery, lung/pleural biopsy, diaphragmatic repair, cardiac repair MDC 14 Selected risk factor identification Patient Related Body habitus (Obesity) Effusion size Localized fluid COPD chronic lung disease Cardiogenic pulmonary edema Acute respiratory distress syndrome Procedure Related Transthoracic needle aspiration Thoracentesis and pleural biopsy Subclavian venipuncture Abdominal cavity operations Bronchoscopy Respiratory, mechanical and positive pressure ventilation *Patient coughing during procedure Source: ICD10/TechSpecs/PSI_06_Iatrogenic_Pneumothorax_Rate.pdf 38 Strategies to Incorporate Risk Adjustment in PSI 90 Example: PSI 08 In Hospital Fall with Hip Fracture Selected exclusions (absolute risk adjustment) Self inflicted injury Principal diagnosis of hip fracture Secondary diagnosis of hip fracture present on admission (POA) Susceptible to falls Selected diagnosis codes: Seizure disorder, stroke, occlusion of arteries, coma, cardiac arrest, poisoning, trauma, delirium or other psychoses, anoxic brain injury, metastatic cancer, lymphoid and bone malignancy, disorders of musculoskeletal system and connective tissue Risk factor identification Patient Related Body habitus (Obesity) Hypertension Drug abuse Liver disease Psychoses Procedure Related COPD Diabetes w/ chronic complications Immune disorders Neurological disease Renal failure, sepsis, heart failure Source: ICD10/TechSpecs/PSI_08_In_Hospital_Fall_with_Hip_Fracture_Rate.pdf 39 13


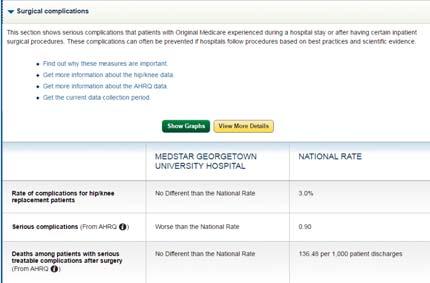
14 40 Risk Adjustment in Hospital Compare Image source: _they_do_not_compare.jpg
15 43 Medicare.gov/Hospital Compare Risk adjustment To make comparison of hospital performance fair and level the playing field: 30 day unplanned readmission and death measures adjust for patient characteristics that may make death more likely, even if the hospital provided higher quality of care Risk adjustment calculated using the AHRQ Comorbid Conditions methodology (CC) Characteristics include Patient s age Past medical history, and other diseases or conditions (comorbidities) the patient had on admission that are known to increase the patient s risk of dying or having an unplanned readmission Medicare.gov/Hospital Compare Hospital Compare reports on the following 30 day mortality measures: Medical conditions: 30 day death rate for COPD patients 30 day death rate for heart attack patients 30 day death rate for heart failure patients 30 day death rate for pneumonia patients 30 day death rate for stroke patients Surgical procedures: 30 day death rate for coronary artery bypass graft (CABG) patients *Risk adjustment variables are the same for unplanned readmission and death rates* 44 Medicare.gov/Hospital Compare Hospital Compare reports on the following 30 day readmission measures: Medical conditions: 30 day unplanned readmission for COPD patients 30 day unplanned readmission for heart attack patients 30 day unplanned readmission for heart failure patients 30 day unplanned readmission for pneumonia patients 30 day unplanned readmission for stroke patients Surgical procedures: 30 day unplanned readmission for coronary artery bypass graft (CABG) patients 30 day unplanned readmission for hip/knee replacement Hospitalwide: 30 day unplanned readmission for any cause 45 15
 Elective CABG Staged procedures or planned readmissions Age < 65, length of stay < 2 days Transfer to another acute care facility Selected risk factor identification History of old")
16 46 Risk Adjustment in Hospital Compare Strategies to Incorporate Risk Adjustment in Hospital Compare Example: 30 Day Unplanned Readmission / Mortality for Heart Attack Selected exclusions (absolute risk adjustment) Elective CABG Staged procedures or planned readmissions Age < 65, length of stay < 2 days Transfer to another acute care facility Selected risk factor identification History of old myocardial infarction Valvular disease Diabetes with and without complications Asthma Peptic ulcer Delirium/senility/dementia Stroke Cerebrovascular disease Patient Related Source: Coronary atherosclerosis or other ischemic heart disease Metastatic cancer/leukemia/other cancers Decubitus ulcer Renal failure Deficiency anemias Drug/alcohol abuse with and without dependence Hemiplegia/paraplegia/paralysis/functional disability COPD 47 Strategies to Incorporate Risk Adjustment in Hospital Compare Example: 30 Day Unplanned Readmission / Mortality for Pneumonia Selected exclusions (absolute risk adjustment) Planned readmission Age < 65 Transfer to another acute care facility Left against medical advice Selected risk factor identification Patient Related History of CABG Diabetes with and without complications Liver disease Pneumonia Acute coronary syndrome Malnutrition Hemiplegia/paraplegia/paralysis/functional disability Dementia or senility Sepsis and septic shock Malnutrition Disorders of fluid/electrolyte/acid base Metastatic cancer/leukemia/other cancers Urinary tract infection Other endocrine/metabolic/nutritional disorders Deficiency anemias Drug or alcohol induced dependence/psychosis Source:
17 49 Strategies to Incorporate Risk Adjustment in Hospital Compare Example: 30 Day Unplanned Readmission Following TKA/THA Selected exclusions (absolute risk adjustment) Fracture of femur, hip, pelvis (implies emergent/urgent admission) Includes a partial hip arthroplasty with knee arthroplasty Revision of TKA/THA / resurfacing / removal of implanted device Mechanical complication of arthroplasty as principal diagnosis Malignant neoplasm of pelvis, sacrum, coccyx, lower limbs, bone marrow Selected risk factor identification Patient Related Skeletal deformities Morbid obesity Diabetes with and without complications Disorders or fluid/electrolyte/acid base Hemiplegia/paraplegia/paralysis/functional disability COPD Decubitus ulcer Post traumatic osteoarthritis Metastatic cancer/leukemia/other cancers Malnutrition Rheumatoid arthritis Polyneuropathy Renal failure Stroke Source: Medicare.gov/Hospital Compare Hospital Compare reports on the following Surgical Complications of Care Rates: Complication rate following elective total hip arthroplasty or total knee arthroplasty Patient Safety Indicator (PSI) composite measure 90 covered in VBP section PSI 4: Deaths Among Patients With Serious Treatable Complications After Surgery PSI 6: Iatrogenic Pneumothorax covered in VBP section PSI 12: Perioperative Pulmonary Embolism or Deep Vein Thrombosis covered in VBP section PSI 14: Postoperative Wound Dehiscence covered in VBP section PSI 15: Accidental Puncture or Laceration covered in VBP section *Risk adjustment variables are the same for unplanned readmission and death rates* 50 Strategies to Incorporate Risk Adjustment in Hospital Compare Example: Complications Following THA/TKA Selected exclusions (absolute risk adjustment) Left against medical advice (AMA); transfer from another acute care facility for the THA/TKA Femur, hip, or pelvic fractures as principal or secondary discharge diagnosis fields of the index admission Partial hip arthroplasty (PHA) procedures with a concurrent THA/TKA Revision procedures with a concurrent THA/TKA; resurfacing procedures with a concurrent THA/TKA Mechanical complication coded in the principal discharge diagnosis field Malignant neoplasm of the pelvis, sacrum, coccyx, lower limbs, or bone/bone marrow or a disseminated malignant neoplasm codedinthe principal discharge diagnosis field Removal of implanted devices/prostheses Selected risk factor identification Osteoporosis Morbid obesity Diabetes with and without complications Disorders or fluid/electrolyte/acid base Hemiplegia/paraplegia/paralysis/functional disability COPD Vertebral fractures or trauma Patient Related Source: Bone/joint/muscle infection or necrosis Metastatic cancer/leukemia/other cancers Malnutrition Rheumatoid arthritis Osteoarthritis of hip/knee Renal failure Vascular or circulatory diseases 51 17
18 52 Provider Strategies to Reduce Risk Exposure Image source: Documentation and Coding for Risk Documentation of conditions as chronic or acute on chronic While acuity is important to capture for the severity of the current condition, not documenting the chronic means from a risk standpoint, the current condition is an isolated event Chronicity of conditions means the person s health status is impacted over a greater length of time Is the acute condition an exacerbation or an aggravation of an underlying condition? 53 Documentation and Coding for Risk Examples Acute systolic/diastolic/combined heart failure Is this brand new heart failure? Is the event indicative of an undiagnosed chronic heart failure? Is the decompensation related to or caused by something else? Renal insufficiency Insufficiency is a nonspecific descriptor Does the patient have an underlying chronic kidney disease? Hepatitis B New or chronic? Manifestations? Cor pulmonale Acute or chronic? Higher risk and severity when chronic condition vs. an isolated acute condition Bronchitis Chronic, such as in COPD Seasonally related or viral (different implications for risk) 54 18
19 55 Documentation and Coding for Risk Examples (cont.) Respiratory failure Acute due to pneumonia, other lung disease, sepsis Acute on chronic (is the patient on oxygen at home?) Are other risk factors documented? Obesity Smoking status or history Sleep apnea Environmental exposure or history Hypertension Always document cause and effect or linkages Hypertensive heart disease or heart failure Hypertensive chronic kidney disease Hypertensive heart and chronic kidney disease Secondary hypertension (cause?) Documentation for Accurate Risk Adjustment Avoid the use of abbreviations Does your facility have an accepted abbreviations list? Is the abbreviation on the list? If not, write/type it out or select from a list Include all diagnoses and carry them through from admission to discharge If ruled out clearly state ruled out If resolved state resolved, then always include the diagnosis on the discharge summary Appropriate documentation of history of If currently being treated, it is a current condition Document any and all history that affects medical decision making 56 Documenting Neoplasms History of cancer does not typically influence risk adjustment Manifestation of the cancer may affect risk adjustment Organ removal or transplantation Ongoing treatment Recurrence Is the patient undergoing active treatment? If metastasis, documentation of primary site often carries risk adjustment Documenting primary site is appropriate even if primary site is no longer receiving active treatment What treatment is the patient undergoing? 57 19
20 58 Documenting Depression In ICD 10, depression is required to be coded as a single episode Consider if your patient is on medication or other treatment for depression does the patient have a singleissue depression, or is it a longer term depression? Consider other providers documentation for specificity of depression Many SSRIs are toxic to pregnant women and to breastfeeding children would a patient be on a long term toxic medication for a single episode of depression? Tools used to validate depression may be impacted by the current treatment being received if in doubt, query the provider Documenting Malnutrition Failure to thrive, cachexia, cachectic appearing are nonspecific diagnoses Are nutrition notes visible to providers? Consider ASPEN criteria (two or more present for diagnosis of malnutrition): Insufficient energy intake Weight loss Loss of subcutaneous fat Localized of generalized fluid accumulation Diminished functional status When documenting malnutrition, always include severity and type and consider the following elements: History and clinical diagnosis; clinical signs and physical examination, anthropometric data, lab indicators, dietary data/history, functional outcomes 59 Documenting Medical History History is commonly missed because providers believe that it has little or no impact on the current problem Many conditions treated and resolved should be documented because they are factual and impact risk adjustment as well as medical decision making Amputee Old MI Addiction/substance abuse/smoking Providers should document all medical history that impacts medical decision making History or current smoking status Status of device implantation History of interventional radiology procedures such as angiography, ERCP History of cancer (status or surgeries? Organ removal?) Surgical history 60 20


21 61 Documenting the Contributions of Other Providers Diagnoses from laboratory reports, radiology reports, and other non treating providers are not able to be submitted (coded) unless the treating provider also documents the diagnosis Much specificity and higher risk adjustment is lost when the surgeon or the current provider defaults to an unspecified diagnosis Common examples: Surgical clearance letters Cardiologist will include specific heart disease conditions such as type of atrial fibrillation or type of angina Surgeon only documents a fib or angina PCP clearance for surgery Wealth of medical history and specificity is not included in the surgical H&P Leveraging the EHR poor implementation of problem lists Commonly Missed Diagnoses That Increase Risk Adjustment Major depression Protein calorie malnutrition Dementia Obesity (diagnosis carries severity) Chronic obstructive pulmonary disease Manifestations of diabetes Chronic disease states DM Kidney disease Heart failure Cancer Status Amputee CABG Stents Organ transplants 62 Thank you. Questions? mdominesey@childrensnational.org In order to receive your continuing education certificate(s) for this program, you must complete the online evaluation. The link can be found in the continuing education section at the front of the program guide
6/30/2015. Lunch and Learn. Objectives. Who owns Quality and Patient Safety? We all do It s a Balance of Responsibility
 Lunch and Learn Patient Safety Indicators June 11, 2014 Objectives List at least 3 entities that drive patient quality and safety initiatives Define AHRQ Patient Safety Indicators Describe the 10 diagnoses
Lunch and Learn Patient Safety Indicators June 11, 2014 Objectives List at least 3 entities that drive patient quality and safety initiatives Define AHRQ Patient Safety Indicators Describe the 10 diagnoses
Supplementary Online Content
 Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Objectives. Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers
 Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Medicare Spending per Beneficiary: Analyzing MSPB Data to Identify Primary Drivers August 22, 2017 Objectives Understand the basics of the hospital specific MSPB data files and reports Review the factors
Measure Applications Partnership. Hospital Workgroup In-Person Meeting Follow- Up Call
 Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
Measure Applications Partnership Hospital Workgroup In-Person Meeting Follow- Up Call December 21, 2016 Feedback on Current Measure Sets for IQR, HACs, Readmissions, and VBP 2 Previously Identified Crosscutting
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Readmission Measures Set
Present-on-Admission (POA) Coding
 Coding") 1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
Mandatory Elements of Healthcare Reform Walter Coleman. healthcare consulting
 Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
Mandatory Elements of Healthcare Reform Walter Coleman 1 Agenda ACA Mandatory Elements of Reform Value Based Purchasing Readmission Reduction Program Hospital Acquired Conditions Best practices to analyze
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach
 A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
A Pause in the Availability of Risk Adjusted National Benchmarks for AHRQ Indicators and an Alternative Measurement Approach Joseph Greenway, MPH Director of the Center for Health Information Analysis
APPENDIX EXHIBITS. Appendix Exhibit A2: Patient Comorbidity Codes Used To Risk- Standardize Hospital Mortality and Readmission Rates page 10
 Ross JS, Bernheim SM, Lin Z, Drye EE, Chen J, Normand ST, et al. Based on key measures, care quality for Medicare enrollees at safety-net and non-safety-net hospitals was almost equal. Health Aff (Millwood).
Ross JS, Bernheim SM, Lin Z, Drye EE, Chen J, Normand ST, et al. Based on key measures, care quality for Medicare enrollees at safety-net and non-safety-net hospitals was almost equal. Health Aff (Millwood).
Supplementary Online Content
 Supplementary Online Content Khera R, Dharmarajan K, Wang Y, et al. Association of the hospital readmissions reduction program with mortality during and after hospitalization for acute myocardial infarction,
Supplementary Online Content Khera R, Dharmarajan K, Wang Y, et al. Association of the hospital readmissions reduction program with mortality during and after hospitalization for acute myocardial infarction,
Hu J, Gonsahn MD, Nerenz DR. Socioeconomic status and readmissions: evidence from an urban teaching hospital. Health Aff (Millwood). 2014;33(5).
. 2014;33(5).") Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Appendix Definitions of Index Admission and Readmission Definitions of index admission and readmission follow CMS hospital-wide all-cause unplanned readmission (HWR) measure as far as data are available.
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix Identification of Study Cohorts
 Appendix Identification of Study Cohorts Because the models were run with the 2010 SAS Packs from Centers for Medicare and Medicaid Services (CMS)/Yale, the eligibility criteria described in "2010 Measures
Appendix Identification of Study Cohorts Because the models were run with the 2010 SAS Packs from Centers for Medicare and Medicaid Services (CMS)/Yale, the eligibility criteria described in "2010 Measures
Mortality Risk Adjustment and HCCs: Is This the New 'Sweet Spot' for Physician Buy In?
 Mortality Risk Adjustment and HCCs: Is This the New 'Sweet Spot' for Physician Buy In? Kyra Brown, RHIA, CCS, CCDS Clinical Documentation Manager/Educator Erlanger Chattanooga, TN 1 Learning Objectives
Mortality Risk Adjustment and HCCs: Is This the New 'Sweet Spot' for Physician Buy In? Kyra Brown, RHIA, CCS, CCDS Clinical Documentation Manager/Educator Erlanger Chattanooga, TN 1 Learning Objectives
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
Last Updated: Version 4.3a NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
2018 Diagnosis Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
ICD-10 Physician Education. Palliative Care SIP
 ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
ICD-10 Physician Education Palliative Care SIP 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
 CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2020 Payment Update
 Program Measures for the FY 2020 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
CMS Inpatient Quality Reporting (IQR) Program Measures for the Payment Update Measures Required to Meet IQR Program APU Requirements Healthcare-Associated Infection on CAUTI National Healthcare Safety
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs)
") What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
What ASMBS Members Need to Know About: New Medicare Payment Policy Governing Bariatric Surgery and Hospital Acquired Conditions (HACs) Robin Blackstone, MD, FACS, FASMBS Beginning October 1, 2008, Medicare
Acute Coronary Syndrome
 ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
ACUTE CORONOARY SYNDROME, ANGINA & ACUTE MYOCARDIAL INFARCTION Administrative Consultant Service 3/17 Acute Coronary Syndrome Acute Coronary Syndrome has evolved as a useful operational term to refer to
SCORES FOR 4 TH QUARTER, RD QUARTER, 2014
 SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
SCORES FOR 4 TH QUARTER, 2013 3 RD QUARTER, 2014 PATIENT SATISFACTION SCORES (HCAHPS): 4 STARS OUT OF 5 (ONLY 4 AREA ACUTE CARE HOSPITALS RECEIVED A 4-STAR RATING. NONE ACHIEVED 5-STARS). STRUCTURAL MEASURES:
CMS Hospital Inpatient Quality Reporting (IQR) Program Measures for the FY 2019 Payment Update
 Program Measures for the FY 2019 Payment Update") CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
CMS Inpatient Quality Reporting (IQR) Program Measures for the Update Measures Required to Meet IQR Program APU Requirements NHSN Submission CAUTI National Healthcare Safety Network (NHSN) Catheter-Associated
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE. Measure Information Form Collected For: CMS Outcome Measures (Claims Based)
") Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARDS FOR HOSPITAL CARE Measure Information Form Collected For: CMS Outcome Measures (Claims Based) Measure Set: CMS Mortality Measures Set
Appendix 1: Supplementary tables [posted as supplied by author]
![Appendix 1: Supplementary tables [posted as supplied by author]](/thumbs/81/83505567.jpg "Appendix 1: Supplementary tables [posted as supplied by author]") Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
Appendix 1: Supplementary tables [posted as supplied by author] Table A. International Classification of Diseases, Ninth Revision, Clinical Modification Codes Used to Define Heart Failure, Acute Myocardial
DRG Code DRG Description FY18 Average Charge
 DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
DRG Code DRG Description FY18 Average Charge 3 ECMO OR TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W MAJ O $ 665,511 4 TRACH W MV 96+ HRS OR PDX EXC FACE, MOUTH & NECK W/O MAJ O.R. $ 422,497 37 EXTRACRANIAL
ICD 10 CM Coding and Documentation
 ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management
 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management") Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
Fiscal Year (FY) 2019 Hospital Inpatient Proposed Rule Interventional Cardiology, Peripheral Interventions & Rhythm Management On April 24, 2018, the Centers for Medicare & Medicaid Services (CMS) released
The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis
 Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
Client Report Milliman Client Report The Cost Burden of Worsening Heart Failure in the Medicare Fee For Service Population: An Actuarial Analysis Prepared by Kathryn Fitch, RN, MEd Principal and Healthcare
Risk Adjustment and Hierarchical Condition Category Coding
 Risk Adjustment 101 Agenda Risk Adjustment Model Hierarchical Condition Categories (HCC) Patient Example Documentation MEAT Documentation Guidance Chronic Conditions Risk Score Calculations Steps for Physician
Risk Adjustment 101 Agenda Risk Adjustment Model Hierarchical Condition Categories (HCC) Patient Example Documentation MEAT Documentation Guidance Chronic Conditions Risk Score Calculations Steps for Physician
ACOFP 55th Annual Convention & Scientific Seminars. How Complicated is Your Panel? Effective Risk Coding in Primary Care. Alison Mancuso, DO, FACOFP
 8 ACOFP 55th Annual Convention & Scientific Seminars How Complicated is Your Panel? Effective Risk Coding in Primary Care Alison Mancuso, DO, FACOFP How Complicated is Your Panel?: Effective Risk Coding
8 ACOFP 55th Annual Convention & Scientific Seminars How Complicated is Your Panel? Effective Risk Coding in Primary Care Alison Mancuso, DO, FACOFP How Complicated is Your Panel?: Effective Risk Coding
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Learning Objectives. Guidance Hierarchy. AHA Coding Clinic Update
 1 AHA Coding Clinic Update Nelly Leon Chisen, RHIA Director, Coding and Classification Executive Editor, Coding Clinic American Hospital Association Chicago, IL Learning Objectives At the completion of
1 AHA Coding Clinic Update Nelly Leon Chisen, RHIA Director, Coding and Classification Executive Editor, Coding Clinic American Hospital Association Chicago, IL Learning Objectives At the completion of
CMS Measures - Fiscal Year 2019
 ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) ID Me asure Name NQF # Value- (VBP) - (HACRP) (HRRP) CMS s - Fiscal Year 2019 ID Name NQF # The Centers for Medicare & Medicaid Services (CMS) Improvement
Episodes of Care Risk Adjustment
 Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
Episodes of Care Risk Adjustment Episode Types Wave 1 Asthma Acute Exacerbation Perinatal Total Joint Replacement Wave 2 Acute Percutaneous Coronary Intervention COPD Acute Exacerbation Non-acute Percutaneous
Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised
 MEMORANDUM TO: Sophia Chan SUBJECT: Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised Reliability of an outcome measure is the extent to which variation in the measure
MEMORANDUM TO: Sophia Chan SUBJECT: Reporting Period and Reliability of AHRQ, CMS 30-day and HAC Quality Measures - Revised Reliability of an outcome measure is the extent to which variation in the measure
TOTAL HIP AND KNEE REPLACEMENTS. FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES
 TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
TOTAL HIP AND KNEE REPLACEMENTS FISCAL YEAR 2002 DATA July 1, 2001 through June 30, 2002 TECHNICAL NOTES The Pennsylvania Health Care Cost Containment Council April 2005 Preface This document serves as
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 4 Episodes Attention deficit hyperactivity disorder (ADHD); Opposition defiance disorder (ODD); Coronary artery bypass
Appendix. Potentially Preventable Complications (PPCs) identify. complications that can occur during an admission. There are 64
 identify. complications that can occur during an admission. There are 64") Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Calikoglu S, Murray R, Feeney D. Hospital pay-for-performance programs in Maryland produced strong results, including reduced hospital-acquired infections. Health Aff (Millwood). 2012;31(12). Appendix
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC NPSS Asheville, NC
 Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Documentation Tips for Pulmonary/Critical Care
 Documentation Tips for Pulmonary/Critical Care ICD-10 classifications: The HARD WAY! J44 Other chronic obstructive pulmonary disease Includes: asthma with chronic obstructive pulmonary disease chronic
Documentation Tips for Pulmonary/Critical Care ICD-10 classifications: The HARD WAY! J44 Other chronic obstructive pulmonary disease Includes: asthma with chronic obstructive pulmonary disease chronic
SEPTICEMIA OR SEVERE SEPSIS W/O MV >96 HOURS W MCC 84, ,037.80
 Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
Inpatient Visits by DRG Inpatient Discharges between 10/01/17 and 09/30/18 DRG DRG Description Average Charge Self-Pay Price VAGINAL DELIVERY W/O COMPLICATING 775 DIAGNOSES 14,680.67 5,578.66 795 NORMAL
The Centers for Medicare & Medicaid Services (CMS) Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures
 Acute Care Hospital Fiscal Year (FY) 2018 Quality Improvement Program Measures") ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ID M easure Name NQF # H os pital M easurement Period H os pital H os pital Value-Bas ed Purchas ing M easurement Period H os pital H ealth Record (EH R) Incentive M easurement Period H os pital H os pital-
ICD-10 Physician Education. General Surgery
 ICD-10 Physician Education General Surgery 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
ICD-10 Physician Education General Surgery 1 Training Objectives ICD-9 to ICD-10 Comparison Documentation Tips Additional Educational Opportunities Questions 2 ICD-9 to ICD-10 Comparison Code Structure
TECHNICAL NOTES APPENDIX SUMMER
 TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM JULY 1, 2006 THROUGH JUNE 30, 2007 The Pennsylvania Health Care Cost Containment
79 HCCs CMS-HCC Risk Adjustment Model. ICD-10-CM to CMS-HCC Crosswalk. Over 9,500 ICD-10-CM codes map to one or more.
 2017 CMS-HCC Risk Adjustment Model Over 9,500 ICD-10-CM codes map to one or more 79 HCCs ICD-10-CM to CMS-HCC Crosswalk CMS-HCC Model On April 4, 2016, the Centers for Medicare & Medicaid Services (CMS)
2017 CMS-HCC Risk Adjustment Model Over 9,500 ICD-10-CM codes map to one or more 79 HCCs ICD-10-CM to CMS-HCC Crosswalk CMS-HCC Model On April 4, 2016, the Centers for Medicare & Medicaid Services (CMS)
Nov FromAtoZCodesMatter
 Nov 2017 FromAtoZCodesMatter From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA The implementation of ICD-10 brought tens of thousands of new codes. Ranging from A to Z, they portray
Nov 2017 FromAtoZCodesMatter From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA The implementation of ICD-10 brought tens of thousands of new codes. Ranging from A to Z, they portray
Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis MedPartners CDI: Karen Newhouser, RN, BSN,
7th Annual Association for Clinical Documentation Improvement Specialists Conference Who's Driving the DRG Bus: Selecting the Appropriate Principal Diagnosis MedPartners CDI: Karen Newhouser, RN, BSN,
WATCHMAN. For questions regarding WATCHMAN reimbursement, please contact:
 WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
WATCHMAN IMPORTANCE OF DOCUMENTATION & THE IMPACT ON MS- DRG ASSIGNMENT This guide stresses the importance of documentation in capturing the appropriate acuity level for patients considered WATCHMAN candidates.
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 CDI and Hospital Readmissions: What Impact Can You Have? Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation & Publisher of VBPmonitor Michelle A. Leonard Mays, RN, MSN, CCDS Senior Healthcare
CDI and Hospital Readmissions: What Impact Can You Have? Kim Charland, BA, RHIT, CCS Senior Vice President Clinical Innovation & Publisher of VBPmonitor Michelle A. Leonard Mays, RN, MSN, CCDS Senior Healthcare
Proprietary Acute Care Indicators
 Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
Proprietary Acute Care Indicators Indicator 1a: Device-Associated Infections in the Intensive Care Unit Central Line-Associated Bloodstream Infections in the APICU, CCU, MICU, M/S ICU, & SICU Ventilator-Associated
APR-DRG Description Ave Charge
 Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
Abdominal Pain 16,500.25 2.8 6,000.09 Acute & Subacute Endocarditis 15,339.30 3.0 5,113.10 Acute Myocardial Infarction 17,687.46 2.6 6,802.87 Alcohol Abuse & Dependence 19,126.64 4.2 4,553.96 Alcoholic
From A to Z-Codes Matter
 From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA While ALL ICD-10-CM codes are important, the Z-codes in ICD-10-CM are frequently considered step-children, supplemental codes
From A to Z-Codes Matter Susan Wallace, MEd, RHIA, CCS, CDIP, CCDS, FAHIMA While ALL ICD-10-CM codes are important, the Z-codes in ICD-10-CM are frequently considered step-children, supplemental codes
4/1/2014 ICD-10 CM/PCS. Benefits to ICD-10. Fewer queries and/or requests for additional clarification. Fewer denials based on medical necessity
 Clinical Documentation and ICD-10 Presented by: Altegra Health 1 ICD-10 CM/PCS ICD-10 will be the official HIPAA-transaction set to communicate all patient conditions and all inpatient treatments, beginning
Clinical Documentation and ICD-10 Presented by: Altegra Health 1 ICD-10 CM/PCS ICD-10 will be the official HIPAA-transaction set to communicate all patient conditions and all inpatient treatments, beginning
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
Registry Highlights. Dale Daniel Symposium Hip Fracture Registry. Overall Volume by Year and Region 3/7/2014
 Dale Daniel Symposium 2014 Registry Highlights Overview: Updated Volume NCAL/SCAL Snapshot Hip Fracture Registry Update Gary Zohman, MD SCAL Regional Lead Anaheim, CA Quarterly Quality Report Review Future
Dale Daniel Symposium 2014 Registry Highlights Overview: Updated Volume NCAL/SCAL Snapshot Hip Fracture Registry Update Gary Zohman, MD SCAL Regional Lead Anaheim, CA Quarterly Quality Report Review Future
NATIONAL QUALITY FORUM
 TO: NQF Members and Public FR: NQF Staff RE: Pre-comment review of an addendum to National Voluntary Consensus Standards: Cardiovascular Endorsement Maintenance 2010: A Consensus Report DA: October 6,
TO: NQF Members and Public FR: NQF Staff RE: Pre-comment review of an addendum to National Voluntary Consensus Standards: Cardiovascular Endorsement Maintenance 2010: A Consensus Report DA: October 6,
ICD-10-CM: The Sage Continues
 ICD-10-CM: The Sage Continues UHIMA Kathy DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA UASI Kathy.devault@uasisolutions.com Objectives Review quality documentation Discuss use of unspecified codes Discuss opportunities
ICD-10-CM: The Sage Continues UHIMA Kathy DeVault, MSL, RHIA, CCS, CCS-P, FAHIMA UASI Kathy.devault@uasisolutions.com Objectives Review quality documentation Discuss use of unspecified codes Discuss opportunities
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title
 Status Type NQF Measure Title") End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
End-Stage Renal Disease Quality Incentive Program (ESRD QIP) Status Type NQF Measure Title NQF Status ID Implemented Outcome 1454 Proportion of patients with hypercalcemia 0256 Vascular Access Type Catheter
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
Quality ID #358: Patient-Centered Surgical Risk Assessment and Communication National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL MEASURES:
ICD-10-CM Coding and Documentation for Long Term Care
 ICD-10-CM Coding and Documentation for Long Term Care June 3, 2014 Chris Hoskins, MA, RHIA, CTR, CHC Karen Fabrizio, RHIA CHTS-CP AHIMA Approved ICD-10-CM/PCS Trainers Objectives Review 2014 Coding Guidelines
ICD-10-CM Coding and Documentation for Long Term Care June 3, 2014 Chris Hoskins, MA, RHIA, CTR, CHC Karen Fabrizio, RHIA CHTS-CP AHIMA Approved ICD-10-CM/PCS Trainers Objectives Review 2014 Coding Guidelines
CMS Hospital IQR Program Measure Comparison Tables FY 2018 (CY 2016) Measures Required to Meet Hospital IQR APU Requirements NHSN Submission
 Measures Required to Meet Hospital IQR APU Requirements NHSN Submission") CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
CMS IQR Program Measure Comparison Tables (CY 2016) NHSN Submission CLABSI Central Line-Associated Bloodstream Infection (CLABSI) Required NHSN CAUTI Catheter-Associated Urinary Tract Infection (CAUTI)
Comparison of Medicare Fee-for-Service Beneficiaries Treated in Ambulatory Surgical Centers and Hospital Outpatient Departments
 Comparison of Medicare Fee-for-Service Beneficiaries Treated in Ambulatory Surgical Centers and Hospital Outpatient Departments Prepared for: American Hospital Association April 4, 2019 Berna Demiralp,
Comparison of Medicare Fee-for-Service Beneficiaries Treated in Ambulatory Surgical Centers and Hospital Outpatient Departments Prepared for: American Hospital Association April 4, 2019 Berna Demiralp,
Supplementary Digital Content Section A Procedural codes to define study population
 Supplementary Digital Content Section A Procedural codes to define study population Procedure CCI codes ORTHOPEDIC Total hip replacement 1.VA.53.LA-PN ; 1.VA.53.PN-PN Total knee replacement 1.VG.53 VASCULAR
Supplementary Digital Content Section A Procedural codes to define study population Procedure CCI codes ORTHOPEDIC Total hip replacement 1.VA.53.LA-PN ; 1.VA.53.PN-PN Total knee replacement 1.VG.53 VASCULAR
2015 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 A Matter of Life or Death: CDI Impact on Mortality Risk Adjustment Allison Clerval, RN, BSN, CCDS Kathleen Shindle, RN, BSN, CCDS Clinical Documentation Supervisors Thomas Jefferson University Hospital
A Matter of Life or Death: CDI Impact on Mortality Risk Adjustment Allison Clerval, RN, BSN, CCDS Kathleen Shindle, RN, BSN, CCDS Clinical Documentation Supervisors Thomas Jefferson University Hospital
Determining MS-DRGs. Kimberly Cunningham CPC, CIC, CCS. Copyright/Disclaimer text
 Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
Determining MS-DRGs Kimberly Cunningham CPC, CIC, CCS Copyright/Disclaimer text No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or
This presentation was current at the time it was published or uploaded onto the web. Medicare and commercial payers change their policies frequently.
 Cost, The Forgotten Component of the Medicare Merit-based Incentive Payment System (MIPS) for National Society of Certified Healthcare Business Consultants Presented By Maxine Lewis, CMM, CPC, CPC-I, CCS-P,
Cost, The Forgotten Component of the Medicare Merit-based Incentive Payment System (MIPS) for National Society of Certified Healthcare Business Consultants Presented By Maxine Lewis, CMM, CPC, CPC-I, CCS-P,
DRG Pitfalls: What to look for in Documentation to Code Comorbid Conditions. Heather Greene, MBA, RHIA, CPC, CPMA
 DRG Pitfalls: What to look for in Documentation to Code Comorbid Conditions Heather Greene, MBA, RHIA, CPC, CPMA Agenda Acronyms & Definitions MCD & MS-DRG Hierarchies MCC/CC Documentation Acronyms &
DRG Pitfalls: What to look for in Documentation to Code Comorbid Conditions Heather Greene, MBA, RHIA, CPC, CPMA Agenda Acronyms & Definitions MCD & MS-DRG Hierarchies MCC/CC Documentation Acronyms &
Understanding Hierarchical Condition Categories (HCC)
") Understanding Hierarchical Condition Categories (HCC) How hierarchical condition category coding will impact your practice and how you can use these codes to increase quality, improve the patient experience,
Understanding Hierarchical Condition Categories (HCC) How hierarchical condition category coding will impact your practice and how you can use these codes to increase quality, improve the patient experience,
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TECHNICAL NOTES APPENDIX SUMMER
 TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM July 1, 2005 through June 30, 2006 The Pennsylvania Health Care Cost Containment
TECHNICAL NOTES APPENDIX SUMMER Hospital Performance Report Summer Update INCLUDES PENNSYLVANIA INPATIENT HOSPITAL DISCHARGES FROM July 1, 2005 through June 30, 2006 The Pennsylvania Health Care Cost Containment
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment
 TN Bundled Payment Initiative: Overview of Episode Risk Adjustment United Healthcare, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
TN Bundled Payment Initiative: Overview of Episode Risk Adjustment United Healthcare, April 2014 The State of Tennessee has implemented an episode-based approach to reimburse providers for the care delivered
THE NATIONAL QUALITY FORUM
 THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
THE NATIONAL QUALITY FORUM National Voluntary Consensus Standards for Patient Outcomes Table of Measures Submitted-Phase 1 As of March 5, 2010 Note: This information is for personal and noncommercial use
How R are you coding severe sepsis? Why the R-code matters
 How R are you coding severe sepsis? Why the R-code matters WHITE PAPER Summary: This article briefly reviews aspects of differing definitions of severe sepsis, and provides commentary on perceived areas
How R are you coding severe sepsis? Why the R-code matters WHITE PAPER Summary: This article briefly reviews aspects of differing definitions of severe sepsis, and provides commentary on perceived areas
A chapter by chapter look at the ICD-10-CM code set Coding Tip Sheet
 Coding Tip Sheet Chapter 1 - Certain Infectious and Parasitic Diseases Terminology changes: The term Sepsis (ICD-10-CM) has replaced the term Septicemia (ICD-9-CM) Urosepsis is a nonspecific term and is
Coding Tip Sheet Chapter 1 - Certain Infectious and Parasitic Diseases Terminology changes: The term Sepsis (ICD-10-CM) has replaced the term Septicemia (ICD-9-CM) Urosepsis is a nonspecific term and is
Medicare and Medicaid Payments
 and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
and Payments The following table includes information about payments made by and for the 17 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on
Average Gross Charges ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC ,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280
 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W CC - 281 15,254 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W MCC - 280 24,827 ACUTE MYOCARDIAL INFARCTION, DISCHARGED ALIVE W/O CC/MCC - 282 11,575 AFTERCARE,
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
FY2015 Proposed Hospital Inpatient Rule Summary
 FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
FY2015 Proposed Hospital Inpatient Rule Summary Cardiac Rhythm Management (CRM) Electrophysiology (EP) Interventional Cardiology (IC) Peripheral Intervention (PI) On April 30, 2014, the Centers for Medicare
Capturing the Activity in Activity based funding
 Capturing the Activity in Activity based funding Activity Based Funding - The National Health Reform Agreement 2011 provided for the introduction of Activity Based Funding from July 1, 2012. - The aim
Capturing the Activity in Activity based funding Activity Based Funding - The National Health Reform Agreement 2011 provided for the introduction of Activity Based Funding from July 1, 2012. - The aim
Risk Mitigation in Bundled Payment
 Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Risk Mitigation in Bundled Payment When to Hold Them and When To Fold Them Lily Pazand, MPH NYU Langone Medical Center Jonathan Pearce, MBA, CPA, FHFMA Singletrack Analytics Jessica Walradt, MS Association
Evidence-Based Measure (EBMs) Definitions
 Definitions") Evidence-Based (EBMs) s This guide is a brief summary of the most commonly-used EBMs. All information is based on the MedInsight Evidence Based s (EBMs) User Guide (October 2015), compiled in a way most
Evidence-Based (EBMs) s This guide is a brief summary of the most commonly-used EBMs. All information is based on the MedInsight Evidence Based s (EBMs) User Guide (October 2015), compiled in a way most
Policy Brief June 2014
 Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
Policy Brief June 2014 Which Medicare Patients Are Transferred from Rural Emergency Departments? Michelle Casey MS, Jeffrey McCullough PhD, and Robert Kreiger PhD Key Findings Among Medicare beneficiaries
Appropriate documentationwhy it matters. Eric Cornatzer MD Baptist Princeton Hospital
 Appropriate documentationwhy it matters Eric Cornatzer MD Baptist Princeton Hospital Disclosures Nothing to disclose Purpose Why Clinical documentation is important To provide general overview of Clinical
Appropriate documentationwhy it matters Eric Cornatzer MD Baptist Princeton Hospital Disclosures Nothing to disclose Purpose Why Clinical documentation is important To provide general overview of Clinical
ENROLLMENT : Line of Business Summary
 ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
ENROLLMENT : Line of Business Summary Date Range : JAN 2017 through DEC 2017 COMPREHENSIVE MAJOR MEDICAL Print Date : 1/19/2018 9:43:49AM Page 1 of 1 Month Year Single 2 Person : Emp/Spouse 2 Person :
Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi.
 A Venture of Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi HIPAA Code Sets HIPAA legislation required use of the International
A Venture of Cheryl Ericson, MS, RN, CCDS, CDIP, AHIMA Approved ICD 10 CM/PCS Trainer Clinical Documentation Program Manager for ezdi HIPAA Code Sets HIPAA legislation required use of the International
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond
 PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
PfP Quality Metrics: Readmissions, Value-Based Purchasing and Beyond Presented to ASHNHA Alaska Partnership for Patients Advisory Group February 4, 2015 Gloria Kupferman Readmissions Calculation methods
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations
 50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
50198 Federal Register / Vol. 75, No. 157 / Monday, August 16, 2010 / Rules and Regulations mstockstill on DSKH9S0YB1PROD with RULES2 VerDate Mar2010 17:02 Aug 13, 2010 Jkt 220001 PO 00000 Frm 00158
Medicare Payments. PHC4 Hospital Performance Report Oct 2015 through Sept 2016 Data 2015 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from calendar
Medicare Payments. PHC4 Hospital Performance Report Oct 2016 through Sept 2017 Data FFY 2017 Medicare Payments 1
 The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
The following table includes information about payments made by for the 16 medical conditions/surgical procedures included in this Hospital Performance Report. This analysis is based on data from federal
Yes No Unknown. Major Infection Information
 Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Medicare Hospital Acquired Conditions Reduction Program Andrew B. Wheeler Vice President of Federal Finance
 Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Medicare Hospital Acquired Conditions Reduction Program - 201 Andrew B. Wheeler Vice President of Federal Finance Value-Based Hospital Acquired Purchasing Conditions FFY 2018 FFY -2016 2020 AHRQ Claims
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Krumholz HM, Wang K, Lin Z, et al. Hospital-readmission risk
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Krumholz HM, Wang K, Lin Z, et al. Hospital-readmission risk
Cardiothoracic and Cardiothoracic Surgery ICD-10-CM 2014: Reference Mapping Card
 2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
Chapter 1 Certain Infectious and Parasitic Diseases
 Chapter 1 Certain Infectious and Parasitic Diseases 1.1 A patient is seen for right lower leg muscle atrophy that is the result of a previous bout of polio. Chapter 2 Neoplasms 2.1 Small cell carcinoma
Chapter 1 Certain Infectious and Parasitic Diseases 1.1 A patient is seen for right lower leg muscle atrophy that is the result of a previous bout of polio. Chapter 2 Neoplasms 2.1 Small cell carcinoma
Top 10 ICD-10 Coding Errors (and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus
 Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus") (and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus Top 10 ICD-10 Coding Errors (and how to fix them!) Top 10 Primary Diagnoses In ICD-10 ICD-10 Codes
(and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus Top 10 ICD-10 Coding Errors (and how to fix them!) Top 10 Primary Diagnoses In ICD-10 ICD-10 Codes
ICD-9 to ICD-10 Crosswalk Adult Codes
 ICD- to ICD- Crosswalk Adult Codes On October 1, 2015, the Centers for Medicare & Medicaid Services (CMS) transitioned to the new International Classification of Diseases, th Revision System (ICD-), which
ICD- to ICD- Crosswalk Adult Codes On October 1, 2015, the Centers for Medicare & Medicaid Services (CMS) transitioned to the new International Classification of Diseases, th Revision System (ICD-), which
HCC s and Providers: Get Paid For What You Do! Speaker s Disclaimer
 HCC s and Providers: Get Paid For What You Do! D. Scott Jones, CHC Chief Compliance Officer, Augusta Health Compliance Official, Augusta Care Partners ACO Speaker s Disclaimer D. Scott Jones, CHC has no
HCC s and Providers: Get Paid For What You Do! D. Scott Jones, CHC Chief Compliance Officer, Augusta Health Compliance Official, Augusta Care Partners ACO Speaker s Disclaimer D. Scott Jones, CHC has no