L esercizio fisico e le patologie cardiorespiratorie: dalla valutazione funzionale alla prescrizione. M. Guazzi
|
|
|
- Alfred Hoover
- 5 years ago
- Views:
Transcription



1 La Riabilitazione Interdisciplinare L esercizio fisico e le patologie cardiorespiratorie: dalla valutazione funzionale alla prescrizione M. Guazzi Università di Milano Dipartimento Cardiologia Universitaria IRCCS Policlinico San Donato Milano
2 Functional Evaluation and Exercise Prescription In Cardiac Patients Background and Key Questions Background: Exercise is a Mainstay Physiological Stressor and VO 2 is a Key Measure of CV Health Questions: O 2 Transport and Utilization Chain: What The Wrong Pathways in HF? Gas Exchange Analysis and Exercise Prescription
 1992 1993 1994 1995 1996 1997 1998 1999 00 01 02 CPX and Ventilation")

3 Articles per annum Functional Evaluation in Heart Failure Applications of CPET in Cardiology CPX and Oscillatory Breathing CPET Statements Single variable CPX pathophysiol/clinical (Peak VO2) CPX and Ventilation (VE/VCO2 slope OUES, PETCO2) Pubmed search analysis: CPET/CPX cardiac patients, heart disease, cardiopulmonary disease,exercise gas exchange 60% of papers looking at prognosis 70% on HFrEF Multiparametric approach Cardiopulmonary Imaging/Reappraisal of Invasive CPET


4 From 9 plots to Score Risk Tables Universal Report Color-Coded Score Tables..the ultimate goal is to increase awareness of the value of CPET and to increase the number of healthcare professionals who are able to perform clinically meaningful interpretation.

5 Applications of NonInvasive Echo Combined Approach in the CPX Lab Diagnosis Instrumental Clinical follow-up Valvular heart disease HFrEF HFpEF Others Coronary Artery Disease (HCM, congenital ) Rest Echo MRI Pulmonary hemodynamics Rest Echo MRI Pulmonary Hemodyamics Ergometry Stress Echo Nuclear test Stress MRI Angio CT Rest Echo MRI Pulmonary hemodynamics Exercise Gas Exchange +Echo Angiography Medical LVAD HTx Surgery PCI Medical Surgery Medical post Surgery

6 Cardiopulmonary Imaging

7 Measurement Baseline Unloaded Effort Anaerobic Threshold Maximal Effort P Value for Each Group Within Group Between Groups Time-Group Interaction Stroke volume, ml Normal HFpEF HFrEF Cardiac output, l/min Normal HFpEF HFrEF Vo 2, l/min Normal HFpEF HFrEF Mitral regurgitation, ml Normal HFpEF HFrEF Avo 2 diff, l/l Normal HFpEF HFrEF 77.3 ± ± ± ± ± ± ± ± ± ± ± ± ± ± ± ± ± * 67.5 ± ± ± ± ± ± ± ± ± 3.4* 24.0 ± 27.0* 105 ± ± ± ± ± 3.5* 7.0 ± ± ± ± 0.34* 0.4 ± ± ± ± ± 19,0* 70.7 ± ± 2.9* 9.6 ± ± ± ± ± 0.56 AVO2 diff estimation by CO estim and VO ± ± ± 0.02* 0.10 ± ± ± 0.02* Values are mean ± SD, or n (%). *p< 0.01, p <0.001 AVo 2 Diff = arterial-venous oxygen content difference; EDV = end-diastolic volume; other abbreviations as in Table ± ± ± ± ± ± 0.01* < < < < < < < < < < < < < <




8 Determinants of the O 2 Transport and Utilization Chain Framed on the Fick Principle Signs and Symptoms HFpEF HFrEF Exercise Intolerance Dyspnea and Fatigue Organ limiting steps in O 2 uptake [convection (delivery), release, diffusion and use] VO 2 = C.O. x C (a-v) O 2 Low Pcap O 2 High PvO 2
9 Fick Principle: Determinants. Delivery or convection Extraction 2.5 times VO 2 = C.O. x c (a-v) O times 1.2 times C.O. = HR x SV Mixed Venous C = 1.34 x Sat O 2 x [Hb] Ventilation Gas diffusion Perfusion HYPOXIA ANEMIA
10 Cardiac Output (L/min) C.O. X C (a-v)o 2 = VO 2 2,525 AT Peak VO 2 (L/min) 4.0 Anemia Normal 3.5 1,515 COPD ,55 0 Rest C (a-v)o 2 (ml %)
11 Cardiac Output and O 2 Extraction at Maximum Exe. in Normal Individuals Stringer et al J Appl Physiol 1997;83: Normal A-V diff range
12 Cardiac Output and O 2 Extraction at Peak Exe. in HFrEF normals
13 Cardiac Output (L/min) C.O. X C (a-v)o 2 = VO 2 2,525 AT Peak VO 2 (L/min) 4.0 Normal 3.5 1, CHF 2.0 0,55 Rest Anemia C (a-v)o 2 (ml %)
14 Partitioning C (a-v) O 2 Contribution to VO 2 Increase in Severe HFrEF To define the C(a-v)O 2 phenotypes (high vs low) by estimating extraction from the CO/VO 2 ratio 104 HFrEF patients (mean age 64±11 y, male %, ischemic etiology 68%, mean LVEF 34±9%) Population divided by CO/VO 2 median value Group A (<0.49) vs Group B (>0.49) In preparation
15 Functional and Echocardiographic Characteristics According to the Extent of C (a-v) O 2 Extent Variables Group A (n=52) Group B (n=52) p value Rest Peak Rest Peak Rest Peak CPET VO 2, L/min 0.26± ± ± ± ns Peak VO 2, 11.8±4 12.6±3.1 ns ml O 2 *Kg -1 *min -1 C(a-v)O 2, ml/100ml 9±3 19±5 7±1 12± VE/VCO 2, slope 36±11 31±7.01 ECHO LVEDVi, ml/m 2 101±33 91±23.09 MR ERO, mm 2 22±10 33±13 16±9 25± E/e 28±15 22±11.02 CO, l/min 3.1± ± ± ±
16 Good Extractor (peak exercise CO/VO 2 <0.49) CO, L/min: Rest 2.9; Peak 3.72 VO 2 : L/min Rest 0.27; Peak 0.65 C(a-v)O 2 ml/100 ml Rest 9; Peak 17 Bad Extractor (peak exercise CO/VO ) CO, L/min: Rest 3.3; Peak 5.2 VO 2 : L/min Rest 0.19 ; Peak 0.61 C(a-v)O 2 ml/100 ml Rest 6; Peak Impaired ventilatory efficiency Preserved ventilatory efficiency
17 Effects of Exe. Central Blood Flow Distribution on Fick Principle in HFrEF To define the role of mitral regurgitation on C(a-v)O 2, CO and related functional phenotype 110 HFrEF patients (mean age 65±11 y, male %, ischemic etiology 64%, mean LVEF 32±8%) divided by severe MR 33 Controls In preparation
18 CO (L/min) 10 peak VO ± 0.6 L/min CONTROLS peak VO ± 0.32 L/min -% no MR % rest VO ± 0.08 ml/min MR 4 3 rest VO ± 0.06 ml/min peak VO ± 0.26 ml/min 2 1 rest VO ± 0.09 ml/min +% C (a-v)o 2 (ml/100ml)
19 Functional and Echocardiographic Characteristics According to MR Variables CPET Group A (n=24) Group B (n=80) p value Rest Peak Rest Peak Rest Peak Peak VO 2, ml O 2 *Kg -1 *min ±4 13.3±3.01 C(a-v)O 2, ml/100ml 8±3 19±4 7.5±1 14± VE/VCO 2, slope 37±10 31±6.01 ECHO LVEDVi, ml/m 2 111±30 89±22.07 E/e 28±15 22±11.02 CO, l/min 3.5± ± ± ±
 and LV dilatation")
 and LV dilatation (LVEDVi= 86")
20 Good Extractor Bad Extractor Severe mitral insufficiency (ERO=37 mm 2 ) and LV dilatation (LVEDVi= 117 ml/m 2 ) Mild mitral insufficiency (ERO=11 mm 2 ) and LV dilatation (LVEDVi= 86 ml/m 2 )
21 Determinants of mpap in HFrEF pump load mpap = Q x PVR + PCWP RV Function Compliance Mitral Insuff In the systemic circulation, downstream hydraulic pressure (in the right atrium) contributes little (<5%) to systemic arterial pressure. In the lung, downstream pressure (ie, LAP) is a much more important contributor to mean PAP ( 50%), and this proportion can become even greater in HF Vascular tone and remodeling resistive Increased LV filling pressure stiffness pulsatile
 in both HFrEF and HFpEF is prognostically relevant")



22 Mitral Regurgitation Induces PH and RV Dysfunction 1. MR (primary or secondary) in both HFrEF and HFpEF is prognostically relevant 1,2 especially when detected during exercise 3,4 2. Exercise-induced MR triggers PH and portends a severe outcome ò significance especially when RV dysfunction/failure coexists 5-7 Rest watt 40 watt peak 1: Tumminello G et al 2: Guazzi M et al Circulation 12; 3: Lancellotti P et al. Circulation 03;108: ; 4: Lancellotti P Eur Heart J 05;26: ; 5: Kusunose K Circ Cardiovasc Imaging. 13;6: : Bandera F et al Eur J Cardiov Imag 16 PASP: 50 mmhg PASP: 85 mmhg
23 Right Ventricular Contractile Reserve and Pulmonary Circulation Uncoupling During Exercise Challenge in Heart Failure: Pathophysiology and Clinical Phenotypes JACC HF 16; 4(8): HFrEF pts undergoing Echo stress test and CPX Group A (TAPSE > 16 mm) n= 60 Average TAPSE: 21 mm (TAPSE < 16 mm) n=37 Average TAPSE= 13 mm Rest Median TAPSE at peak exe 15.5 mm Group B (TAPSE > 15.5 mm) n=19 Group C (TAPSE < 15.5 mm) n=18 Peak Exe B C
24 Right Ventricular Contractile Reserve and Pulmonary Circulation Uncoupling During Exercise Challenge in Heart Failure: Pathophysiology and Clinical Phenotypes 97 HFrEF pts undergoing Echo stress test and CPX, divided according to TAPSE > 16 mm Group A or < 16 mmhg at rest with recovery (Group B) or not during exercise (Group C) Results- RV to PC Coupling PASP (mmhg) 80 PASP (mmhg) y = 13,721x + 4,5659 R² = 0,9953 y = 6,2162x + 16,495 R² = 0, y = 72,5x - 896,5 R² = 0,7758 y = 4,4426x - 26,23 R² = y = 5,7934x + 9,679 R² = 0, y = 5,5x - 82,833 R² = 0, Cardiac Output (ml/min) TAPSE (mm) Group A Group B Group C
 Non-survivors (n=47) y=-0,1107x+19,897 R 2 =0,1729 10 30 40 50 60 70 80 PASP, FORCE mmhg 8 4 0 TAPSE > 16 mm (n=176) TAPSE 16 mm")
25 LENGTH TAPSE (mm) TAPSE (mm) 293 HF patients (247 HFrEF; 46 HFpEF) Echocardiographic evaluation of RV function, PH, LV function and biomarkers y=-0,1407x+23,645 R 2 =0, y=-0,0277x+,579 R 2 =0, Survivors (n=246) Non-survivors (n=47) y=-0,1107x+19,897 R 2 =0, PASP, FORCE mmhg TAPSE > 16 mm (n=176) TAPSE 16 mm (n=117) y=-0,0473x+16,589 R 2 =0, PASP (mmhg)
26 Right Ventricular Contractile Reserve and Pulmonary Circulation Uncoupling During Exercise Challenge in Heart Failure: Pathophysiology and Clinical Phenotypes Results- RV Contractile Reserve (TAPSE vs PASP relationship at rest and peak exe) Group A Group B Group C TAPSE (mm) 30 y = -0,0151x + 23,32 TAPSE (mm) 30 TAPSE (mm) y = 0,0081x + 17, y = -0,0344x + 14, y = -0,0321x + 21, y = -0,0002x + 14,008 5 y = -0,0136x + 13, PASP (mmhg) PASP (mmhg) PASP (mmhg) Full simbols: Rest Empty symbols: Peak exercise
27 Right Ventricular Contractile Reserve and Pulmonary Circulation Uncoupling During Exercise Challenge in Heart Failure: Pathophysiology and Clinical Phenotype Clinical Characteristics Group A (n=60) Group B (n=19) Group C (n=18) P Age, y 62±10 65±8 64± BMI 26±4 26±4 27± Female gender, % BNP, pg/dl 1879 ± ± ± * LV Cardiac Data *:Group B and C vs Group A Group A (n=60) Group B (n=19) Group C (n=18) P Rest Peak Rest Peak Rest Peak Rest Peak LV ejection fraction, % 33±8 37±10 34±9 37±14 32±11 35±10 ns ns LV end diastolic vol. indexed, ml/m 2 90±23 95±28 113±47 ns LV mass indexed, g/m 2 126±30 121±22 154± Left atrial volume indexed, ml/m 2 47±18 52±24 80± E/e 22±11 25±16 38± Cardiac output, l*min ± ± ± ± ± ± Severe MR, %
28 Right Ventricular Contractile Reserve and Pulmonary Circulation Uncoupling During Exercise Challenge in Heart Failure: Pathophysiology and Clinical Phenotypes CPET Data HF (n= 97) Group A (n=60) Group B (n=19) Group C (n=18) P Value Maximal work, W 65 ± ± ± ± 18ⱡ Peak VO 2, ml/kg/min 13.0 ± ± ± ± 2.3ⱡ Predicted peak VO 2, % 53 ± ± ± ± Peak RER 1.17 ± ± ± ± Peak O 2 pulse, ml/beat 9.0 ± ± ± ± VE/VCO 2 slope 34 ± ± 7 35 ± ± End-tidal CO 2, mmhg 33 ± 6 35 ± 5 33 ± 6 28 ± Exercise Oscillatory Ventilation * Circulatory power, mmhg ml O 2 1,886 ± 672 2,144 ± 627 1,734 ± 508 1,182 ± kg -1 min -1 Ventilatory power, mmhg 4.8 ± ± ± ± 1.2 < Values are mean ± SD or %. *Chi-square test. Kruskal-Wallis test. p < 0.025, group B versus group C. BP= blood pressure; EOV= exercise oscillatory ventilation; HF= heart failure; RER= respiratory exchange ratio; VCO2= carbon dioxide output; VE= minute ventilation; VO2 = oxygen uptake. *:Group B and C vs Group A peak
29 HR (beats/min) HR (bpm) VE (L/min) VCO 2 (L/min) VO 2 (L/min) VO 2 /HR V T (L) VE (L/min) RR P ET O 2 (mmhg) VE (L/min) VO 2 (ml/min) VO 2 (ml/min) P ET CO 2 (mmhg) The 9-plot Analysis peak VO 2 : 8 ml/min/kg Ramp protocol (8 watt/min) Max workload: 45 watt Work Symptom-limited test 100 terminated because of DYSPNEA and Significant RV-PA UNCOUPLING Work VO 2 (L/min) Time (sec) VE/VCO0.8 2 : slope: VE/VO 2 0 VCO VCO 2 (L/min) Time (sec) Time (sec) VE/VCO Time (sec) VE (L/min) Time (sec) Guazzi M et al JACC 17 in press











30 Group B Rest Peak Rest TAPSE 13 mm Peak TAPSE 18 mm Rest Peak Rest PASP 30 mmhg Peak PASP 50 mmhg ERO 9 mm 2 ERO 13 mm 2 Peak VO ml/kg/min; VE/VCO 2 Slope 32; EOV no Group C Rest Peak Rest Peak Rest TAPSE 12 mm Peak TAPSE 13 mm Rest PASP 66 mmhg Peak PASP 78 mmhg ERO 41 mm 2 ERO 51 mm 2 Peak VO ml/kg/min; VE/VCO 2 Slope 42; EOV yes
31 Exercise Training in Heart Failure 1. Training Intensity (% of VO2 max or max HR) 2. Type of training (endurance, resistance, combined) 3. Methods of training (continuous or steady state, intermittent, interval) 4. Training modality (concentric vs eccentric) 5. Training target (systemic vs regional training, e.g. respiratory training) 6. Training control (supervised/non supervised) 7. Training location (hospital based, outpatient, home based) Moderate intensity endurance training has been proven prognostic benefits reduced hospitalization rate 1, mortality 2,3 1 O Connor CM et al, JAMA 09;301: Keteyan SJ et al JACC 12;60: Piepoli MF et al BMJ 04;328:189
32 Conclusions and Outlook CPET imaging seems now an evolving step to better phenotyping advanced HFrEF. Mitral regurgitation is a sort of central redistributor of O 2 delivery whose mechanistic implications on exercise are of novel interest for either extraction (exhaustion at maximum), RV to PC uncoupuling (increased load) and exercise ventilation inefficiency RV pump failure comes up as an early and quite underestimated mechanical cause of impaired performance and exhaustion. ET training in HF: the evidence is just for continuous, moderate intensity, supervised modalities
The role of CPX testing in the rehabilitation of cardiac patients.
 Cardiopulmonary exercise testing (CPX) for comprehensive cardiac evaluations The role of CPX testing in the rehabilitation of cardiac patients. Viviane M Conraads, MD, PhD Department of Cardiology Cardiac
Cardiopulmonary exercise testing (CPX) for comprehensive cardiac evaluations The role of CPX testing in the rehabilitation of cardiac patients. Viviane M Conraads, MD, PhD Department of Cardiology Cardiac
11/12/2018. Prof. Steven S. Saliterman. Options. Prof. Paul Iaizzo s Physiology Lab, PHSL 3701
 Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Prof. Paul Iaizzo s Physiology Lab, PHSL 3701 Options University of Minnesota Bricker, E. Compass, 5 Types of Cardiac
Department of Biomedical Engineering, University of Minnesota http://saliterman.umn.edu/ Prof. Paul Iaizzo s Physiology Lab, PHSL 3701 Options University of Minnesota Bricker, E. Compass, 5 Types of Cardiac
Basics of Cardiopulmonary Exercise Test Interpretation. Robert Kempainen, MD Hennepin County Medical Center
 Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Basics of Cardiopulmonary Exercise Test Interpretation Robert Kempainen, MD Hennepin County Medical Center None Conflicts of Interest Objectives Explain what normally limits exercise Summarize basic protocol
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
HFPEF Echo with Strain vs. MRI T1 Mapping
 HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
HFPEF Echo with Strain vs. MRI T1 Mapping Erik Schelbert, MD MS Director, Cardiovascular Magnetic Resonance Assistant Professor of Medicine Heart & Vascular Institute University of Pittsburgh Disclosures
Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic, A Djordjevic Dikic, B Beleslin, M Nikolic, M Petrovic, D Popovic
 Combined cardiopulmonary exercise stress echocardiography test: New test for assessment of diastolic dysfunction in patients with hypertension Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic,
Combined cardiopulmonary exercise stress echocardiography test: New test for assessment of diastolic dysfunction in patients with hypertension Ivana Nedeljkovic, M Ostojic, V Giga, V Stojanov, J Stepanovic,
CPX and Prognosis in Cardiovascular Disease
 CPX and Prognosis in Cardiovascular Disease Anselm K. Gitt, Piergiuseppe Agostoni Herzzentrum Ludwigshafen, Germany Instituto di Cardiologia Università di Milano, Milan, Italy Cardiopulmonary exercise
CPX and Prognosis in Cardiovascular Disease Anselm K. Gitt, Piergiuseppe Agostoni Herzzentrum Ludwigshafen, Germany Instituto di Cardiologia Università di Milano, Milan, Italy Cardiopulmonary exercise
Peripheral Contributions to HFpEF
 Peripheral Contributions to HFpEF Greg Lewis MD Heart Failure Section Head MGH Cardiology Division and Pulmonary Critical Care Unit Harvard Medical School March 12, 2018 Pathophysiology of HFpEF vs. HFrEF
Peripheral Contributions to HFpEF Greg Lewis MD Heart Failure Section Head MGH Cardiology Division and Pulmonary Critical Care Unit Harvard Medical School March 12, 2018 Pathophysiology of HFpEF vs. HFrEF
Diastolic Heart Failure Uri Elkayam, MD
 Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Diastolic Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu Diastolic Heart Failure Clinical Definition A
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH
 Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
Pulmonary Hypertension in patients with Heart Failure with Preserved Ejection Fraction Dr.Fayez EL Shaer Consultant cardiologist Assistant professor of cardiology KKUH Recent evaluation of available data
Diagnosis is it really Heart Failure?
 ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
ESC Congress Munich - 25-29 August 2012 Heart Failure with Preserved Ejection Fraction From Bench to Bedside Diagnosis is it really Heart Failure? Prof. Burkert Pieske Department of Cardiology Med.University
Atrial dysfunction and chronotropic incompetence
 Pathophysiology of heart failure with preserved ejection fraction Atrial dysfunction and chronotropic incompetence Vojtech Melenovsky IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST :
Pathophysiology of heart failure with preserved ejection fraction Atrial dysfunction and chronotropic incompetence Vojtech Melenovsky IKEM, Prague, Czech Republic DECLARATION OF CONFLICT OF INTEREST :
Clinical implication of exercise pulmonary hypertension: when should we measure it?
 Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
What is established? Risk of Benefit complica comp tion
 What s new in exercise training in CHF? Jean-Paul Schmid, MD, FESC Consultant Cardiologist, SpitalNetzBern Tiefenau Hospital, Dept. of Internal Medicine, Cardiology, Bern, Switzerland What is established?
What s new in exercise training in CHF? Jean-Paul Schmid, MD, FESC Consultant Cardiologist, SpitalNetzBern Tiefenau Hospital, Dept. of Internal Medicine, Cardiology, Bern, Switzerland What is established?
Exercise Stress Testing: Cardiovascular or Respiratory Limitation?
 Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
Exercise Stress Testing: Cardiovascular or Respiratory Limitation? Marshall B. Dunning III, Ph.D., M.S. Professor of Medicine & Physiology Medical College of Wisconsin What is exercise? Physical activity
The right ventricle in chronic heart failure
 The right ventricle in chronic heart failure ESC 2012 Christian Opitz, Berlin There are no conflicts of interest relevant to this presentation Percent of Population Prevalence of Heart Failure by Age and
The right ventricle in chronic heart failure ESC 2012 Christian Opitz, Berlin There are no conflicts of interest relevant to this presentation Percent of Population Prevalence of Heart Failure by Age and
The REDUCE LAP Heart Failure Trial. David M Kaye MD, PhD on behalf of the REDUCE LAP HF Investigators
 Transcatheter Intracardiac Shunt Device Provides Sustained Clinical Benefit at One Year in Heart Failure with Preserved or Mildly Reduced Ejection Fraction: The REDUCE LAP Heart Failure Trial David M Kaye
Transcatheter Intracardiac Shunt Device Provides Sustained Clinical Benefit at One Year in Heart Failure with Preserved or Mildly Reduced Ejection Fraction: The REDUCE LAP Heart Failure Trial David M Kaye
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
DECLARATION OF CONFLICT OF INTEREST ESC Congress 2011 Pathophysiology of HFPEF Vascular Remodeling & Pulmonary Hypertension Carolyn S.P. Lam MBBS, MRCP, MS Case Presentation 81 yo woman with dyspnoea &
Guide to the interpretation of Cardiopulmonary Exercise Testing
 Guide to the interpretation of Cardiopulmonary Exercise Testing Dr. Ines Frederix December 2014 Copyright: Ines Frederix 1 Ergospirometry: parameter description... 5 1.1 Cardiovascular parameters... 5
Guide to the interpretation of Cardiopulmonary Exercise Testing Dr. Ines Frederix December 2014 Copyright: Ines Frederix 1 Ergospirometry: parameter description... 5 1.1 Cardiovascular parameters... 5
CTED and the Value of Exercise Testing
 CTED and the Value of Exercise Testing leveraging cardiopulmonary physiology to uncover a disease even more elusive than CTEPH Paul Forfia, MD Professor of Medicine Director, PH, RHF, and PTE Programs
CTED and the Value of Exercise Testing leveraging cardiopulmonary physiology to uncover a disease even more elusive than CTEPH Paul Forfia, MD Professor of Medicine Director, PH, RHF, and PTE Programs
Καθετηριασμός δεξιάς κοιλίας. Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ
 Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Καθετηριασμός δεξιάς κοιλίας Σ. Χατζημιλτιάδης Καθηγητής Καρδιολογίας ΑΠΘ The increasing interest in pulmonary arterial hypertension (PAH), the increasing interest in implantation of LVADs, and the evolution
Annual Congress of the European Society of Cardiology Munich, August
 Annual Congress of the European Society of Cardiology Munich, August 26 2012 Gas exchange measurements during exercise show early pulmonary arterial hypertension in scleroderma patients Daniel Dumitrescu,
Annual Congress of the European Society of Cardiology Munich, August 26 2012 Gas exchange measurements during exercise show early pulmonary arterial hypertension in scleroderma patients Daniel Dumitrescu,
The Role of Cardiac Rehabilitation. The Role of Cardiac Rehabilitation. in Heart Failure. in Heart Failure. History of Cardiac Rehab.
 The Role of Cardiac Rehabilitation The Role of Cardiac Rehabilitation in Heart Failure in Heart Failure Kate Traynor RN MS FAACVPR Financial Disclosures No relevant financial relationship exists. History
The Role of Cardiac Rehabilitation The Role of Cardiac Rehabilitation in Heart Failure in Heart Failure Kate Traynor RN MS FAACVPR Financial Disclosures No relevant financial relationship exists. History
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
PHYSICAL AND SEXUAL ACTIVITIES
 Forgotten problems in HF PHYSICAL AND SEXUAL ACTIVITIES Massimo F Piepoli, MD, PhD, FESC, FACC Heart Failure Unit, Guglielmo da Saliceto Hospital, Piacenza m.piepoli@alice.it No disclosures Massimo Speaker
Forgotten problems in HF PHYSICAL AND SEXUAL ACTIVITIES Massimo F Piepoli, MD, PhD, FESC, FACC Heart Failure Unit, Guglielmo da Saliceto Hospital, Piacenza m.piepoli@alice.it No disclosures Massimo Speaker
Right Heart Catheterization. Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich
 Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
todays practice of cardiopulmonary medicine
 todays practice of cardiopulmonary medicine Concepts and Applications of Cardiopulmonary Exercise Testing* Karl T. Weber, M.D.; Joseph S. Janicki, Ph.D.; Patricia A. McElroy, M.D.; and Hanumanth K. Reddy,
todays practice of cardiopulmonary medicine Concepts and Applications of Cardiopulmonary Exercise Testing* Karl T. Weber, M.D.; Joseph S. Janicki, Ph.D.; Patricia A. McElroy, M.D.; and Hanumanth K. Reddy,
Brief View of Calculation and Measurement of Cardiac Hemodynamics
 Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Testing Clinical Implications
 Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Evolutionary origins of the right ventricle. S Magder Department of Critical Care, McGill University Health Centre
 Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction
 Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction JC Eicher, G Laurent, O Barthez, A Mathé, G Bertaux, JE Wolf Heart Failure Treatment Unit, Rhythmology and
Atrial dyssynchrony syndrome: An overlooked cause of heart failure with normal ejection fraction JC Eicher, G Laurent, O Barthez, A Mathé, G Bertaux, JE Wolf Heart Failure Treatment Unit, Rhythmology and
Cardiac Rehabilitation Program for LVAD Patients. Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR
 Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Cardiac Rehabilitation Program for LVAD Patients Dr Katherine Fan Consultant Cardiologist Grantham Hospital, Hong Kong SAR Left Ventricular Assist Devices (LVAD) Improved Survival Following LVAD Implantations
Cardiopulmonary Exercise Testing Cases
 Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Canadian Respiratory Conference - 217 Cardiopulmonary Exercise Testing Cases Darcy D Marciniuk, MD FRCPC FCCP Associate Vice-President Research, University of Saskatchewan Professor, Respirology, Critical
Dyspnea is a common exercise-induced
 MK pg 214 Mædica - a Journal of Clinical Medicine STATE-OF-THE-ART Cardiopulmonary exercise testing in differential diagnosis of dyspnea Nora TOMA, MD; Gabriela BICESCU, MD, PhD; Raluca ENACHE, MD; Ruxandra
MK pg 214 Mædica - a Journal of Clinical Medicine STATE-OF-THE-ART Cardiopulmonary exercise testing in differential diagnosis of dyspnea Nora TOMA, MD; Gabriela BICESCU, MD, PhD; Raluca ENACHE, MD; Ruxandra
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Josh Stanton and Michael Epton Respiratory Physiology Laboratory, Canterbury Respiratory Research Group Christchurch Hospital
 Josh Stanton and Michael Epton Respiratory Physiology Laboratory, Canterbury Respiratory Research Group Christchurch Hospital Setting Scene Advancements in neonatal care over past 30 years has resulted
Josh Stanton and Michael Epton Respiratory Physiology Laboratory, Canterbury Respiratory Research Group Christchurch Hospital Setting Scene Advancements in neonatal care over past 30 years has resulted
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF: Pathophysiology & Treatment
 HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
HFpEF: Pathophysiology & Treatment Barry A. Borlaug, MD Mayo Clinic, Rochester, MN borlaug.barry@mayo.edu Disclosure Financial Relationships Research Support: Aires Pharmaceuticals, Medtronic, GSK Consulting/Advisory
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Approach to CPET. CPET Cases. Case 1 4/4/2018. Impaired? Cardiac factors? Ventilatory factors?
 Approach to CPET CPET Cases Neil MacIntyre MD Duke University Medical Center Durham NC Impaired? Work,, /kg Cardiac factors?, /, BP, Rhythm Ventilatory factors? Ve/MVV (incl EIB, trapping), PaCO2 Gas exchange
Approach to CPET CPET Cases Neil MacIntyre MD Duke University Medical Center Durham NC Impaired? Work,, /kg Cardiac factors?, /, BP, Rhythm Ventilatory factors? Ve/MVV (incl EIB, trapping), PaCO2 Gas exchange
The Who, How and When of Advanced Heart Failure Therapies. Disclosures. What is Advanced Heart Failure?
 The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
Transcatheter InterAtrial Shunt Device for the Treatment of Heart Failure: Results From the REDUCE LAP-HF I Randomized Controlled Trial
 A M E R I C A N H E A R T A S S O C I A T I O N S C I E N T I F I C S E S S I O N S 2 0 1 7 Transcatheter InterAtrial Shunt Device for the Treatment of Heart Failure: Results From the REDUCE LAP-HF I Randomized
A M E R I C A N H E A R T A S S O C I A T I O N S C I E N T I F I C S E S S I O N S 2 0 1 7 Transcatheter InterAtrial Shunt Device for the Treatment of Heart Failure: Results From the REDUCE LAP-HF I Randomized
THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE
 Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Thierry C. Gillebert University of Ghent ESC Education Committee THE DIASTOLIC STRESS TEST: A NEW CLINICAL TOOL? THE CONCEPT OF DIASTOLIC RESERVE 1 Case: Ann, 63 years Suffered from metabolic syndrome
Heart failure is one of the most important
 Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2013; 8(2): 124-128 ORIGINAL PAPERS Worsening of Heart Failure after Abdominal Surgery Can we predict it? Nora TOMA; Ruxandra
Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2013; 8(2): 124-128 ORIGINAL PAPERS Worsening of Heart Failure after Abdominal Surgery Can we predict it? Nora TOMA; Ruxandra
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Cardiopulmonary Stress Testing: Beyond Transplant Evaluation
 Cardiopulmonary Stress Testing: Beyond Transplant Evaluation Ross Arena, PhD, PT, FAHA, FESC, FACSM Professor and Head College of Applied Health Sciences University of Illinois at Chicago Cardio- Pulmonary
Cardiopulmonary Stress Testing: Beyond Transplant Evaluation Ross Arena, PhD, PT, FAHA, FESC, FACSM Professor and Head College of Applied Health Sciences University of Illinois at Chicago Cardio- Pulmonary
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Cardiac Rehabilitation for Heart Failure Patients. Jia Shen MD, MPH Assistant Professor of Medicine UC San Diego Health System
 Cardiac Rehabilitation for Heart Failure Patients Jia Shen MD, MPH Assistant Professor of Medicine UC San Diego Health System Disclosures There are no conflict of interests related to this presentation.
Cardiac Rehabilitation for Heart Failure Patients Jia Shen MD, MPH Assistant Professor of Medicine UC San Diego Health System Disclosures There are no conflict of interests related to this presentation.
QUIZ 1. Tuesday, March 2, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Hemodynamics of Exercise
 Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Hemodynamics of Exercise Joe M. Moody, Jr, MD UTHSCSA and ALMMVAH, STVAHCS Exercise Physiology - Acute Effects Cardiac Output (Stroke volume, Heart Rate ) Oxygen Extraction (Arteriovenous O 2 difference,
Benefits of Combined Aerobic/Resistance/Inspiratory Muscle Training in Patients with Chronic Heart Failure. The Ideal Exercise Program for CHF?
 Benefits of Combined Aerobic/Resistance/Inspiratory Muscle Training in Patients with Chronic Heart Failure. The Ideal Exercise Program for CHF? I D. Laoutaris, S Adamopoulos, A Manginas, D B. Panagiotakos,
Benefits of Combined Aerobic/Resistance/Inspiratory Muscle Training in Patients with Chronic Heart Failure. The Ideal Exercise Program for CHF? I D. Laoutaris, S Adamopoulos, A Manginas, D B. Panagiotakos,
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management
: Natural History and Contemporary Management") Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
Heart Failure with Preserved Ejection Fraction (HFpEF): Natural History and Contemporary Management Jason L. Guichard, MD, PhD Greenville Health System Department of Medicine, Carolina Cardiology Consultants
Heart Failure with Preserved Left Ventricular Ejection Fraction. (HFpEF)
") Thessaloniki, May 27, 2017 Heart Failure with Preserved Left Ventricular Ejection Fraction Filippos Triposkiadis, MD, FESC, FACC Professor of Cardiology Director, Department of Cardiology Larissa University
Thessaloniki, May 27, 2017 Heart Failure with Preserved Left Ventricular Ejection Fraction Filippos Triposkiadis, MD, FESC, FACC Professor of Cardiology Director, Department of Cardiology Larissa University
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Content Display. - Introduction to Unit 4. Unit 4 - Cardiorespiratory Response to Exercise : Lesson 1. KINE xxxx Exercise Physiology
 Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING
 Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Heart Failure with preserved ejection fraction (HFpEF)
") Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
Heart Failure with preserved ejection fraction (HFpEF) Dr. Pierpaolo Pellicori Hull York Medical School Kingston-upon-Hull United Kingdom Conflict of interest: none Heart failure is a contemporary problem
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
Cardiopulmonary Exercise Testing: its principles, interpretation & application. DM Seminar Harshith
 Cardiopulmonary Exercise Testing: its principles, interpretation & application DM Seminar Harshith Outline Physiology of exercise Introduction Equipment and working Principles Interpretation and variables
Cardiopulmonary Exercise Testing: its principles, interpretation & application DM Seminar Harshith Outline Physiology of exercise Introduction Equipment and working Principles Interpretation and variables
Diastology State of The Art Assessment
 Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR?
 LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR? Juan Cinca Department and Chair of Cardiology Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona
LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR? Juan Cinca Department and Chair of Cardiology Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Chapter 21 Training for Anaerobic and Aerobic Power
 Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
Section 06: Exercise Training to Improve Performance Chapter 21 Training for Anaerobic and Aerobic Power Chapter 22 Muscular Strength: Training Muscles to Become Stronger Chapter 23 Special Aids to Exercise
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Assessing the Impact on the Right Ventricle
 Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
Advances in Tricuspid Regurgitation Congress of the European Society of Cardiology (ESC) Munich, August 25-29, 2012 Assessing the Impact on the Right Ventricle Stephan Rosenkranz, MD Clinic III for Internal
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Interest of PVO2 assesment in HFpEF patients
 Interest of PVO2 assesment in HFpEF patients Jean Yves TABET CRCB, Villeneuve Saint Denis Institut Jacques Cartier, Massy Conflits of interest none Interest of PVO2 in HFr EF Evaluation of exercise tolerance
Interest of PVO2 assesment in HFpEF patients Jean Yves TABET CRCB, Villeneuve Saint Denis Institut Jacques Cartier, Massy Conflits of interest none Interest of PVO2 in HFr EF Evaluation of exercise tolerance
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Cardiopulmonary Exercise Testing in Cystic Fibrosis
 Cardiopulmonary Exercise Testing in Cystic Fibrosis Owen Tomlinson MSc, AFHEA Children s Health & Exercise Research Centre University of Exeter James Shelley MSc Physical Activity Exchange Liverpool John
Cardiopulmonary Exercise Testing in Cystic Fibrosis Owen Tomlinson MSc, AFHEA Children s Health & Exercise Research Centre University of Exeter James Shelley MSc Physical Activity Exchange Liverpool John
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease. Alexander (Sandy) Dick, MD
 Dick, MD") Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
Ejection Fraction in Heart Failure: A Redefinition. Tarek Kashour King Fahad Cardiac Center King Saud University Riyadh, KSA
 Ejection Fraction in Heart Failure: A Redefinition Tarek Kashour King Fahad Cardiac Center King Saud University Riyadh, KSA Word of caution!!! Incomplete understanding of a disease process may lead to
Ejection Fraction in Heart Failure: A Redefinition Tarek Kashour King Fahad Cardiac Center King Saud University Riyadh, KSA Word of caution!!! Incomplete understanding of a disease process may lead to
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities
 The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
The Pathophysiology of Cardiogenic Shock Knowledge Gaps & Opportunities Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome
 Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
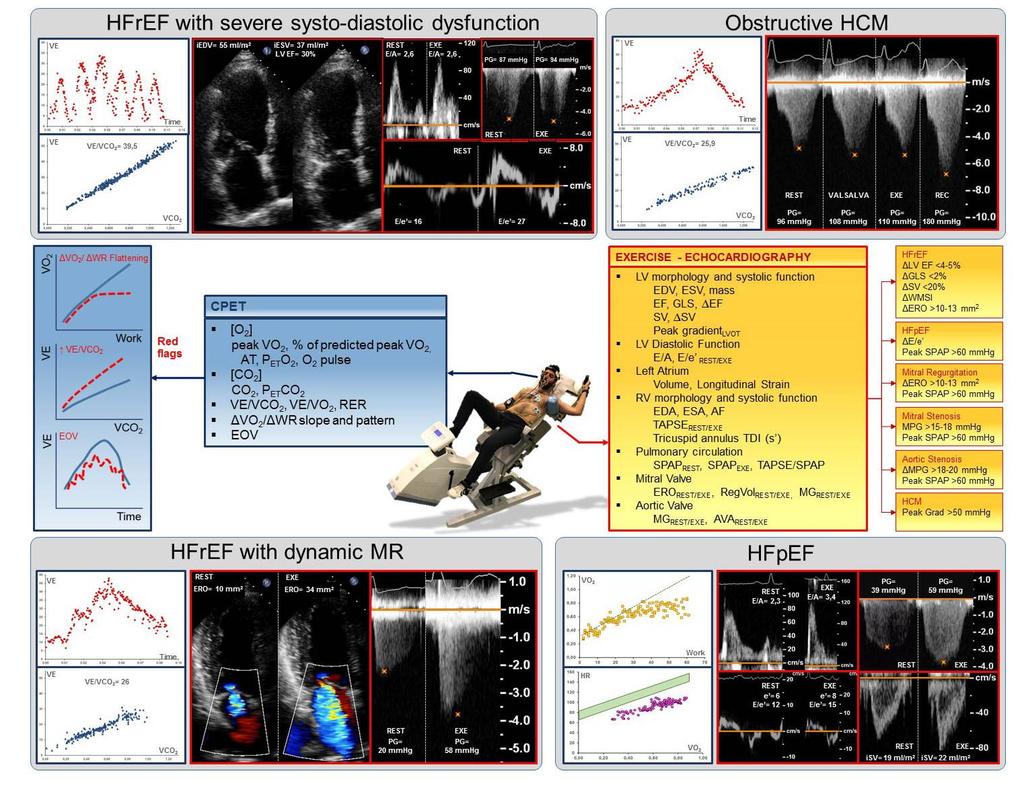
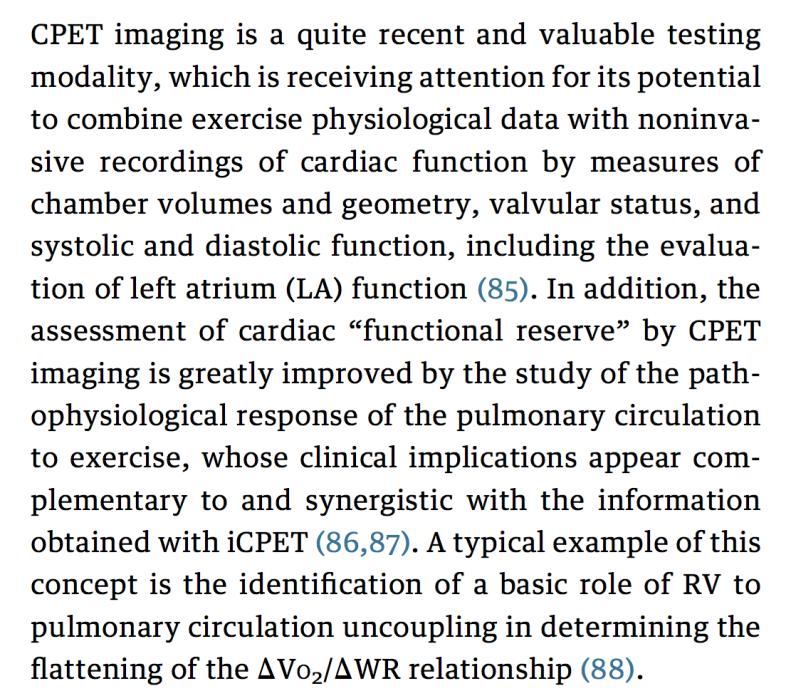
Original Article. Role of Right Ventricle and Dynamic Pulmonary Hypertension on Determining ΔVO 2
 Original Article Role of Right Ventricle and Dynamic Pulmonary Hypertension on Determining /ΔWork Rate Flattening Insights From Cardiopulmonary Exercise Test Combined With Exercise Echocardiography Francesco
Original Article Role of Right Ventricle and Dynamic Pulmonary Hypertension on Determining /ΔWork Rate Flattening Insights From Cardiopulmonary Exercise Test Combined With Exercise Echocardiography Francesco
Imaging in dilated cardiomyopathy : factors associated with a poor outcome
 Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
John G Lainchbury, A Mark Richards
 538 * Heart failure EXERCISE TESTING IN THE ASSESSMENT OF CHRONIC CONGESTIVE HEART FAILURE John G Lainchbury, A Mark Richards Heart 22;88:538 543 See end of article for authors affiliations c PRACTICAL
538 * Heart failure EXERCISE TESTING IN THE ASSESSMENT OF CHRONIC CONGESTIVE HEART FAILURE John G Lainchbury, A Mark Richards Heart 22;88:538 543 See end of article for authors affiliations c PRACTICAL
Pulmonary Hypertension Due to Left Heart Disease
 ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
ACC Middle East Conference 2018 Pulmonary Hypertension Due to Left Heart Disease Ammar Chaudhary, MBChB, FRCPC Advanced Heart Failure & Transplantation King Faisal Specialist Hospital and Research Center
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Advanced imaging of the left atrium - strain, CT, 3D, MRI -
 Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Advanced imaging of the left atrium - strain, CT, 3D, MRI - Monica Rosca, MD Carol Davila University of Medicine and Pharmacy, Bucharest, Romania Declaration of interest: I have nothing to declare Case
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
QATs. VCE Physical Education SCHOOL-ASSESSED COURSEWORK UNIT 3 OUTCOME 2. Introduction. Quality Assessment Tasks
 QATs Quality Assessment s Introduction UNIT 3 OUTCOME 2 VCE Physical Education SCHOOL-ASSESSED COURSEWORK Outcome 2 Use data collected in practical activities to analyse how the major body and energy systems
QATs Quality Assessment s Introduction UNIT 3 OUTCOME 2 VCE Physical Education SCHOOL-ASSESSED COURSEWORK Outcome 2 Use data collected in practical activities to analyse how the major body and energy systems
MASSACHUSETTS INSTITUTE OF TECHNOLOGY
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Cardiopulmonary Exercise Testing: Relevant But Underused
 Global reprints distributed only by Postgraduate Medicine USA. No part of Postgraduate Medicine may be reproduced or transmitted in any form without written permission from the publisher. All permission
Global reprints distributed only by Postgraduate Medicine USA. No part of Postgraduate Medicine may be reproduced or transmitted in any form without written permission from the publisher. All permission
Disclosure. RV is not the innocent bystander 10/1/16. Assessment and Management of Pulmonary Heart Disease in the Female Patient
 Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280
 Results Form #280") Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Revision of 10/27/2017 Form #280 Page 1 of 12 PVDOMICS STUDY Clinical Center Right Heart Catheterization (RHC) Results Form #280 Instructions: Review PVDOMICS MOP Chapter 100 prior to completing right
Surgery and device intervention for the elderly with heart failure: assessing the need. Devices and Technology for heart failure in 2011
 Surgery and device intervention for the elderly with heart failure: assessing the need Devices and Technology for heart failure in 2011 Assessing cardiovascular function / prognosis (in the elderly): composite
Surgery and device intervention for the elderly with heart failure: assessing the need Devices and Technology for heart failure in 2011 Assessing cardiovascular function / prognosis (in the elderly): composite
Echo assessment of the failing heart
 Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Lessons From An Advanced Dyspnea Center: New Approaches to An Old Problem. Robert Schilz DO, PhD
 Lessons From An Advanced Dyspnea Center: New Approaches to An Old Problem Robert Schilz DO, PhD Conflict of Interest Statement Robert Schilz DO, PhD No conflicts relevant to this talk Introduction, Definitions,
Lessons From An Advanced Dyspnea Center: New Approaches to An Old Problem Robert Schilz DO, PhD Conflict of Interest Statement Robert Schilz DO, PhD No conflicts relevant to this talk Introduction, Definitions,
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Pathophysiology Department
 UNIVERSITY OF MEDICINE - PLOVDIV Pathophysiology Department 15A Vasil Aprilov Blvd. Tel. +359 32 602311 Algorithm for interpretation of submaximal exercise tests in children S. Kostianev 1, B. Marinov
UNIVERSITY OF MEDICINE - PLOVDIV Pathophysiology Department 15A Vasil Aprilov Blvd. Tel. +359 32 602311 Algorithm for interpretation of submaximal exercise tests in children S. Kostianev 1, B. Marinov