State of GWTG-Heart Failure 2018 Tuesday February 13, 2018
|
|
|
- Marion Williamson
- 5 years ago
- Views:
Transcription

1 State of GWTG-Heart Failure 2018 Tuesday February 13, 2018 Presenters: Clyde Yancy, MD, MSc, MACC, FAHA, MACP, FHFSA Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Adam DeVore, MD, MHS Pamela Peterson, MD, MPH, MSPH Larry Allen, MD, MHS Nancy Albert, PhD, CCNS, CHFN, CCRN, NE-BC, FAHA, FCCM, FAAN






2 Our Presenters Clyde Yancy, MD, MSc Professor of Medicine, Professor, Medical Social Science Chief, Cardiology Associate Director, Bluhm CV Institute Vice-Dean, Diversity & Inclusion Northwestern University, FSM Deputy Editor, JAMA Cardiology Gregg C. Fonarow, MD Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology Director, Ahmanson UCLA Cardiomyopathy Center Co-Chief, UCLA Division of Cardiology Pamela Peterson, MD, MPH Associate Professor of Medicine-Cardiology University of Colorado Larry Allen, MD, MHS Associate Professor of Medicine, Medical Director of Advanced Heart Failure University of Colorado School of Medicine Adam DeVore, MD, MHS Assistant Professor of Medicine Duke University Medical Center and the Duke Clinical Research Institute Nancy Albert, PhD, CCNS, CHFN Associate Chief Nursing Officer, Office of Nursing Research and Innovation Cleveland Clinic Health System Clinical Nurse Specialist Kaufman Center for Heart Failure Cleveland Clinic Main Campus 2/13/2018 2

3 No relevant disclosures American Heart Association Get With The Guidelines- HF Guideline Directed Care Algorithms Clyde W. Yancy, MD, MSc Professor of Medicine, Professor, Medical Social Science Chief, Cardiology Associate Director, Bluhm CV Institute & Vice-Dean, Diversity & Inclusion Northwestern University, FSM & Deputy Editor, JAMA Cardiology

4

5 New ACC/AHA/HFSA Guidelines

6 Michael R. Bristow et al. JCHF 2017;5: American College of Cardiology Foundation
7 Stages, Phenotypes and Treatment of HF At Risk for Heart Failure Heart Failure STAGE A At high risk for HF but without structural heart disease or symptoms of HF STAGE B Structural heart disease but without signs or symptoms of HF STAGE C Structural heart disease with prior or current symptoms of HF STAGE D Refractory HF e.g., Patients with: HTN Atherosclerotic disease DM Obesity Metabolic syndrome or Patients Using cardiotoxins With family history of cardiomyopathy Structural heart disease e.g., Patients with: Previous MI LV remodeling including LVH and low EF Asymptomatic valvular disease Development of symptoms of HF e.g., Patients with: Known structural heart disease and HF signs and symptoms Refractory symptoms of HF at rest, despite GDMT e.g., Patients with: Marked HF symptoms at rest Recurrent hospitalizations despite GDMT HFpEF HFrEF THERAPY Goals Heart healthy lifestyle Prevent vascular, coronary disease Prevent LV structural abnormalities Drugs ACEI or ARB in appropriate patients for vascular disease or DM Statins as appropriate THERAPY Goals Prevent HF symptoms Prevent further cardiac remodeling Drugs ACEI or ARB as appropriate Beta blockers as appropriate In selected patients ICD Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Improve HRQOL Prevent hospitalization Prevent mortality Strategies Identification of comorbidities Treatment Diuresis to relieve symptoms of congestion Follow guideline driven indications for comorbidities, e.g., HTN, AF, CAD, DM Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Patient education Prevent hospitalization Prevent mortality Drugs for routine use Diuretics for fluid retention ACEI or ARB Beta blockers Aldosterone antagonists Drugs for use in selected patients Hydralazine/isosorbide dinitrate ACEI and ARB Digoxin In selected patients CRT ICD Revascularization or valvular surgery as appropriate THERAPY Goals Control symptoms Improve HRQOL Reduce hospital readmissions Establish patient s endof-life goals Options Advanced care measures Heart transplant Chronic inotropes Temporary or permanent MCS Experimental surgery or drugs Palliative care and hospice ICD deactivation Yancy C, et al. JACC, 2013
8 Prevalence and prognostic significance of HF Stages Survival (years) Ammar et al. Circulation 2007; 115:1563

9 Biomarkers Indications for Use *Other biomarkers of injury or fibrosis include soluble ST2 receptor, galectin-3, and high-sensitivity troponin. ACC indicates American College of Cardiology; AHA, American Heart Association; ADHF, acute decompensated heart failure; BNP, B-type natriuretic peptide; COR, Class of Recommendation; ED, emergency department; HF, heart failure; NT-proBNP, N- terminal pro-b-type natriuretic peptide; NYHA, New York Heart Association; and pts, patients.

10 Lifetime risk for HF; indexed to blood pressure & sex
 Stage 1 hypertension (BP 130 139/80-89 mm Hg) Stage 2 hypertension (BP 140/90 mm Hg) Promote optimal lifestyle habits Nonpharmacologic therapy (Class I) Clinical")
11 Blood Pressure (BP) Thresholds and Recommendations for Treatment and Follow-Up (continued on next slide) BP thresholds and recommendations for treatment and follow-up Normal BP (BP <120/80 mm Hg) Elevated BP (BP /<80 mm Hg) Stage 1 hypertension (BP /80-89 mm Hg) Stage 2 hypertension (BP 140/90 mm Hg) Promote optimal lifestyle habits Nonpharmacologic therapy (Class I) Clinical ASCVD or estimated 10-y CVD risk 10%* No Yes Reassess in 1 y (Class IIa) Reassess in 3 6 mo (Class I) Nonpharmacologic therapy (Class I) Nonpharmacologic therapy and BP-lowering medication (Class I) Nonpharmacologic therapy and BP-lowering medication (Class I)
12 Hypertension Treating Hypertension to Reduce the Incidence of HF COR LOE Recommendations I B-R In patients at increased risk, stage A HF, the optimal blood pressure in those with hypertension should be less than 130/80 mm Hg. Comment/ Rationale NEW: Recommendation reflects new RCT data.

13 Simplified Schematic of the Renin Angiotensin Aldosterone System Copyright American Heart Association, Inc. All rights reserved. von Lueder T G et al. Circ Heart Fail. 2013;6:

14 Simplified Schematic of the Natriuretic Peptide System (NPS) Copyright American Heart Association, Inc. All rights reserved. von Lueder T G et al. Circ Heart Fail. 2013;6:
15 Pharmacological Treatment for Stage C HF With Reduced EF Renin-Angiotensin System Inhibition With ACE-Inhibitor or ARB or ARNI COR LOE Recommendations I ARNI: B-R In patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE inhibitor or ARB, replacement by an ARNI is recommended to further reduce morbidity and mortality. Comment/ Rationale NEW: New clinical trial data necessitated this recommendation.
16 Pharmacological Treatment for Stage C HF With Reduced EF Renin-Angiotensin System Inhibition With ACE-Inhibitor or ARB or ARNI COR LOE Recommendations III: Harm B-R ARNI should not be administered concomitantly with ACE inhibitors or within 36 hours of the last dose of an ACE inhibitor. ARNI should not be administered to III: Harm C-EO patients with a history of angioedema. Comment/ Rationale NEW: Available evidence demonstrates a potential signal of harm for a concomitant use of ACE inhibitors and ARNI. NEW: New clinical trial data.
17 Pharmacological Treatment for Stage C HF With Reduced EF Ivabradine COR LOE Recommendations IIa B-R Ivabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III) stable chronic HFrEF (LVEF 35%) who are receiving GDEM*, including a beta blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of 70 bpm or greater at rest. Comment/ Rationale NEW: New clinical trial data. *In other parts of the document, the term GDMT has been used to denote guideline-directed management and therapy. In this recommendation, however, the term GDEM has been used to denote this same concept in order to reflect the original wording of the recommendation that initially appeared in the 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure.

18 From: Potential Mortality Reduction With Optimal Implementation of Angiotensin Receptor Neprilysin Inhibitor Therapy in Heart Failure JAMA Cardiol. Published online June 22, doi: /jamacardio Demonstrated Benefits of Evidence-Based Therapies for Patients With Heart Failure and Reduced Ejection Fraction Date of download: 7/11/2016 Copyright 2016 American Medical Association. All rights reserved.
19 Palliative Care Works:

20 Treatment of HFrEF Stage C and D Hydral-Nitrates green box: The combination of ISDN/HYD with ARNI has not been robustly tested. BP response should be carefully monitored. See 2013 HF guideline. Participation in investigational studies is also appropriate for stage C, NYHA class II and III HF. ACEI indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor-blocker; ARNI, angiotensin receptor-neprilysin inhibitor; BP, blood pressure; bpm, beats per minute; C/I, contraindication; COR, Class of Recommendation; CrCl, creatinine clearance; CRT-D, cardiac resynchronization therapy device; Dx, diagnosis; GDMT, guideline-directed management and therapy; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; ICD, implantable cardioverter-defibrillator; ISDN/HYD, isosorbide dinitrate hydral-nitrates; K+, potassium; LBBB, left bundle-branch block; LVAD, left ventricular assist device; LVEF, left ventricular ejection fraction; MI, myocardial infarction; NSR, normal sinus rhythm; and NYHA, New York Heart Association.

21

22 2018 by American College of Cardiology Clyde W. Yancy et al. JACC 2018;71:

23 2018 by American College of Cardiology Clyde W. Yancy et al. JACC 2018;71:
24 New Guideline Takeaway messages: New effective medical therapies have now been fully incorporated in evidence based guideline directed treatment algorithms There is an increasing complexity in the treatment of HFrEF; this will require careful assessment of the clinical context/scenario Powerful new data should drive the PREVENTION of heart failure Avoiding entry into the HF Club is the best therapeutic approach
25 GWTG-HF Update and Reducing Readmissions Safely Gregg C. Fonarow, MD FACC, FAHA, FHFSA Eliot Corday Chair of Cardiovascular Medicine and Science Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA Cardiomyopathy Center, Los Angeles, CA

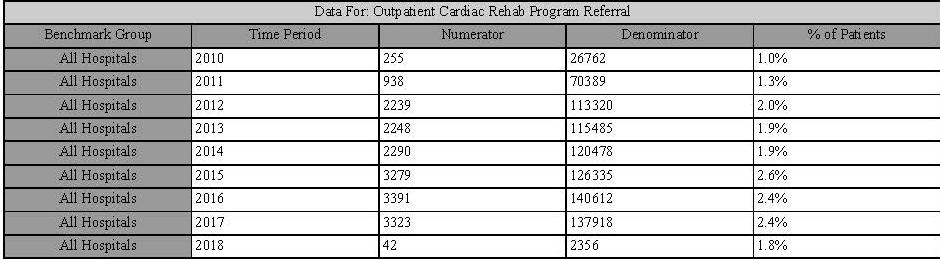
26 2/13/2018 GWTG-HF Hospital Participation

27 GWTG-HF: Hospitalization Episodes Entered Data as of Number of records

28


29

30
31


32
33
34
35

36


37

38

39
40
41 Evidence-Based HFrEF Therapies Guideline Recommended Therapy Relative Risk Reduction in Mortality Number Needed to Treat for Mortality NNT for Mortality (standardized to 36 months) Relative Risk Reduction in HF Hospitalizations ACEI/ARB 17% 22 over 42 months 26 31% ARNI 16% 36 over 27 months 27 21% Beta-blocker 34% 28 over 12 months 9 41% Aldosterone Antagonist 30% 9 over 24 months 6 35% Hydralazine/Nitrate 43% 25 over 10 months 7 33% CRT 36% 12 over 24 months 8 52% ICD 23% 14 over 60 months 23 NA Ivabradine NA NA NA 26% Updated from Fonarow GC, et al. Am Heart J. 2011;161:
 occurred in subjects assigned to sacubitril/valsartan and 1,307 (54.")
42 Influence of Sacubitril/Valsartan on Readmission Rates After HF Hospitalization: PARADIGM HF 30 Day All Cause Readmission Odds Ratio: 0.74; 95% CI Day HF Readmission Odds Ratio: 0.62; 95% CI ,383 investigator-reported HF hospitalizations, of which 1,076 (45.2%) occurred in subjects assigned to sacubitril/valsartan and 1,307 (54.8%) occurred in subjects assigned to enalapril. Desai, A.S. et al. J Am Coll Cardiol. 2016;68(3):241 8.
43 Hospital Readmission Reduction Program Up to 3% cut to all DRGs for readmissions over the expected % Up to 1% in fiscal year 2013, 2% in fiscal year 2014, and 3% in fiscal year 2015 and beyond Initially AMI, heart failure, and pneumonia Expand to COPD, CABG, PCI, and other vascular conditions in year decrease in reimbursement to hospitals $7.1 billion Public reporting began in 2010 and the hospital financial penalties began October 2012 (beginning of fiscal year 2013) Medicare Penalizing 2,211 Hospitals For Excess Readmissions
44 HRRP Impact: Decreasing 30-Day HF Readmissions Accompanied by Increasing 30 Day Risk-Adjusted Mortality Risk-Adjusted Rate, % Observed 30-Day Risk- Adjusted Readmission Rate with HRRP Observed 30-Day Risk- Adjusted Mortality Rate after Discharge with HRRP HRRP Implementation HRRP Penalties Expected 30-Day Risk-Adjusted Mortality Rate after Discharge without HRRP ,200 additional deaths in 2014 may be related to the HRRP 10,400 additional deaths a year if previous declines in mortality had continued Year Year Outcomes Delta 30-Day Risk Adjusted Readmission with HRRP 30-Day Mortality after discharge with HRRP 30-Day Mortality after discharge without HRRP (projected) 23.5% 23.5% 23.4% 23.0% 22.5% 21.6% 21.4% -2.1% 7.9% 8.1% 8.4% 8.7% 8.8% 9.1% 9.2% +1.3% 7.9% 7.8% 7.5% 7.2% 7.0% 6.7% 6.6% -1.3% Fonarow GC et al JACC 2017 Oct 10;70(15): Data from Dharmarajan K et al. J Am Med Assoc. 2017;318:
 after vs before the HRRP implementation, 0.91; 95%CI, 0.87-0.95; P <.001). In contrast, the 30-day risk-adjusted mortality rate increased from 7.")
45 Has HRRP Reporting of Hospital Readmission Rates and Penalties Affected Patient Outcomes? The 30-day risk-adjusted readmission rate declined from 20.0% before the HRRP implementation to 18.4% in the HRRP penalties phase (hazard ratio (HR) after vs before the HRRP implementation, 0.91; 95%CI, ; P <.001). In contrast, the 30-day risk-adjusted mortality rate increased from 7.2% before the HRRP implementation to 8.6% in the HRRP penalties phase (HR after vs before the HRRP implementation, 1.18; 95%CI, ; P <.001). The 1-year risk-adjusted mortality rate increased from 31.3% to 36.3% (HR, 1.10; 95%CI, ; P <.001) after vs before the HRRP implementation.
46 Increase in Risk-Adjusted Mortality after the HRRP Implementation among FFS Medicare Beneficiaries Hospitalized for HF Study GWTG-HF Registry linked to FFS Medicare Data 1 100% Sample of FFS Medicare Data 2 5% Random Sample of FFS Medicare Data 3 Risk Adjustment Clinical Administrative Administrative Time Period Pre-HRRP ( ) vs Post-HRRP ( ) 2008 to to Day Mortality 1.4% 1.3% - 90-Day Mortality - 2.2% - 1-Year Mortality 5.0% - 3.3% 1. Gupta et al. JAMA Cardiol 2017; doi: /jamacardio Dharmarajan et al. JAMA 2017;318: Khera et al. Circ Heart Fail 2017; 10:e
47 Conclusions GWTG-HF is focused on improving on meaningful processes of care and patient-centered outcomes The CMS 30 day readmission metric is fundamentally flawed in measuring quality and driving patient benefit The CMS HRRP has created a perfect storm for suboptimal care, both by side-stepping the best interests of the patient and by thwarting assessment of risk for both clinicians, in their care, and for CMS in its attempt at adjudication and penalty assignment to hospitals It is critical to move entirely away from artificial metrics and penalties and toward greater direct responsibility of health care systems for quality, safety, and value, with any potential rewards linked to long-term patientcentered benefit, through innovative approaches to care Fonarow GC et al JACC 2017 Oct 10;70(15): and Konstam M et al. JACC: Heart Failure, Volume 4, Issue 1, January 2016, Pages 12-20
48 Heart Failure Treatments in Special Populations Adam DeVore, MD, MHS Assistant Professor of Medicine Duke University School of Medicine

49 PARADIGM-HF Baseline Characteristics 2/13/2018 McMurray JJ et al. N Engl J Med 2014;371:
50 Elderly Populations of Interest Females Racial and ethnic minorities Specific cardiomyopathies Comorbid conditions 2/13/2018

51 Heart Failure Care in the Elderly 2/13/2018 Mozaffarian D. et al. Circulation Jan 27;131(4):e29-322
52 Heart Failure Care in the Elderly High prevalence and poor outcomes Different presentations (e.g., different causes of peripheral edema) More likely to have non-cv causes of symptoms and more likely to have comorbid conditions (e.g., hypertension, atrial fibrillation) Low lean body mass and impaired renal function may increase adverse effects from medical therapy (e.g., hyperkalemia with MRAs or increased risk of digoxin toxicity) Increased risk of polypharmacy May require more frequent visits and laboratory monitoring 2/13/2018


53 Heart Failure Care in the Elderly in 2018 Bibas, L. et al. JACEP 2016;2: /13/2018

54 2/13/2018


55 Precision Medicine in Heart Failure? 2/13/2018 Taylor et al. N Engl J Med 2004;351: McNamara et al. J Am Coll Cardiol HF 2014;2:551 7)

56


57 2/13/2018 Important Comorbidites in Heart Failure
58 EMPA-REG: Hospitalizations for Heart Failure HR 0.65 (95% CI ) p= /13/2018 Zinman B et al. N Engl J Med 2015 Fitchett D et al. Eur Heart J 2016
59 2/13/2018 Conclusions HF care in the elderly deserves special consideration to improve outcomes and decrease risk of adverse effects Opportunities for precision medicine exist in HF through the study of differences in biology by race/ethnicity and specific cardiomyopathies Comorbid conditions in HF are common and may offer opportunities to improve care Pam Peterson will speak next on women with heart failure
60 Women with Heart Failure Pamela N Peterson, MD MSPH Associate Professor of Medicine University of Colorado Anschutz Medical Center Denver Health Medical Center 2/13/ , American Heart Association 60
61 Lifetime Risk of Heart Failure Loyd-Jones DM et al. Circulation 2002; 106:3068
62 Incidence of HF with Preserved vs. Reduced EF in Men and Women Ho JE et al. Circ Heart Fail 2013

63 No Differences in In-Hospital Mortality by Gender or LVEF Hsich EM et al. Am Heart J 2012
64 Characteristics by Sex Among those with LVEF <40% Female Male Age Hypertension Diabetes CAD Anemia Valvular Disease Atrial Fibrillation Depression 11 7 Hsich EM et al. Am Heart J 2012

65 Characteristics by Sex Among those with LVEF >50% Female Male Age Hypertension Diabetes CAD Anemia Valve Disease Atrial Fibrillation Depression 13 9 Hsich EM et al. Am Heart J 2012
66 No Sex Differences in Treatment of HF Women are under-represented in RCTs However, available data: Stratified analyses of RCTs Pooled data/ meta-analyses Observational data Guidelines do not differ based on sex All quality metrics apply equally to men and women

67 Quality Metrics in Women vs. Men Klein L et al. Circ Heart Fail 2011

68 Sex differences in ICD Counseling % 19.3% Among those counseled, women and men were similarly likely to receive an ICD (OR 1.13; ) Hess PL, et al. Circulation 2016

69 Improvement in care and reduction in sex differences with GWTG participation Klein L, et al. Circ Heart Fail 2011
70 Improvement in care and reduction in sex differences with GWTG participation Klein L, et al. Circ Heart Fail 2011



71



72 Advanced Heart Failure: Marking a Difference Larry A. Allen, MD, MHS GWTG-HF Webinar
73 Stage C Stage D Clinical course of heart failure Transition to Advanced Heart Failure: Oral therapies failing A time for many major decisions

74 Timing of transplant, LVAD, hospice Too Early Too Late

75 Difficult to know where a patient is

76 I-NEED-HELP I: IV inotropes N: NYHA IIIB/IV Natriuretic peptides persistently elevated E: End-organ dysfunction E: Ejection fraction <25% D: Defibrillator shocks H: Hospitalizations >1 E: Edema, escalating diuretics L: Low blood pressure, high heart rate P: Prognostic medication progressive intolerance or down-titration of GDMT Right heart cath? Palliative care? Referral to Advanced HF Center? 2/13/



77 Not for Everyone: Complex Trade-Offs


78 NNT<2 McIlvennan, et al. Circ Heart Fail. 2014





79 McIlvennan, et al. Circ Heart Fail. 2014


80 MagLev: no bearings, less friction/heat Large rotor gaps: less shear, hemolysis Artificial pulse: flush clot, angiodysplasia Smaller size: easier implant

81 MOMENTUM HM3 Endpoints Mehra M, et al. NEJM. 2016

82 Transplant remains the Gold Standard
83 Heart transplant outcomes Average Age of Recipient: 54 years old Median Survival 10.7 years cohort Better in post 2002 cohorts 93% 1 year survival ISHLT 2013 Report. J Heart Lung Txplt. 2013; 32: 952.


84 Limited supply of donors
 ++ +++ RV failure and ventricular tachycardia Maybe Yes")
85 Which option? Factor LVAD Transplant Survival, median 4-5 yr yr Quality of life (and swimming) RV failure and ventricular tachycardia Maybe Yes Complications!!!!!!! Stroke, infection, bleeding, HF Rejection, infection, cancer, CKD, DM Availability of therapy Unlimited Limited Cost $$$$ $$$


86 1) Advanced age (median HF hosp 78 years) 2) Comborbidity (50% have 5+ diagnoses)
 with stage D 60,000 (25%) may benefit from")

87 Final Perspective 6,000,000 with HF 2,400,000 (40%) HFrEF 240,000 (10%) with stage D 60,000 (25%) may benefit from advanced Rx (LVAD/Tx) 2,800 transplants 4,000 LVADs but large benefit in carefully selected patients LVAD and Transplant Heart Failure

88 GWTG-HF - STATE OF THE ART Quality of Life in Heart Failure - A Goal Not to be Missed Nancy M. Albert PhD, CCNS, CHFN, NE-BC, FAHA, FHFSA, FAAN February 2018
89 Quality of Life in Heart Failure- A Goal Not to be Missed Objective: Discuss the value of understanding quality of life data in patients with heart failure
90 Quality of Life in HF Efficacy of Treatments from Health Care Providers Based on parameters Clinical status Hemodynamics Neurohormonal status Echo/MRI indices Nieminen MS et al. Int J Cardiol. 2015;191: Perspectives Efficacy of Treatments from Patients Based on: Functional capacity Exercise performance Psychological status Frequency of rehospitalization 1) Under represented in clinical trials 2) No universal definition of quality of life endpoints 3) Difficult to standardize data collection
91 Quality of Life Tools in HF 25 tools discussed in the literature Instrument Name Minnesota Living w HF Q Kansas City Cardiomyopathy Q Euro HF QoL Q EuroQ-5D (generic; assesses problems) Chronic HF Q Description 21 items; lifestyle limitations; score = QoL 12/23 items; physical, symptoms, QoL, social impact and selfefficacy; score = QoL 40 items; functional status, etc.; score = QoL VAS; mobility, self-care, usual activities, pain & anxiety/depression domains; score = QoL 20 items; dyspnea, fatigue, emotional function domains; score = QoL Qual of Life in Severe HF Medical Outcomes Study 36- item Short Form Nottingham Health Profile Sickness Impact Profile 26 items; physical activity + VAS of life satisfactionsocial/emotional; score = QoL (less impairment) 36 items; 8 subscales; assesses negative health aspects; score = QoL 38 items based on WHO classification of disabilities; score = QoL 136 Y/N items; 12 areas of pts. life; score = QoL
92 Quality of Life in HF Correlates of QoL 1037 older ambulatory adults, (KCCQ & EQ-5D) 1 Tools were highly related; rho, Factors associated with worse QoL: u Older age, female u Worse functional class u Higher Charlson comorbidity index u Recent hospitalization for HF 1136 (MLHFQ) 2 & 52 (KCCQ) 3 hospitalized adults QoL improved during hospitalization 3 and after discharge in all patients; 2,3 despite intervention vs. control group Comı n-colet J et al. Rev Esp Cardiol. 2016;69(3): Riegel B et al. Nurs Res. 2002;51(4): Sauser K, et al. J Card Fail. 2014;20(5):378.e11-5.

93 Quality of Life in HF Event-Free Survival; by MLHFQ 425 pts. from ESCAPE study; 3 Month Event* p< group time interaction *, event = death or rehospitalization Moser DK, et al. J Cardiac Fail. 2009;15(9):763-
94 Quality of Life in HF Event-Free Survival by Change in MLHFQ 425 pts. from ESCAPE study; 6 Month Event *, adjusted for: LVEF Na+ BUN 6MWD Ability to obtain 6MWD Age SBP Pt gp. assignment p = 0.009, based on degree of improvement in HR-QoL at 1 month* Moser DK, et al. J Cardiac Fail. 2009;15(9):
95 Quality of Life in HF 1x Self-Rated Health (SF-12)* Score Predicts Healthcare Utilization 417 community pts. in MN; followed over mean of 2.1 yrs. HR (95% CI): 1.59 (1.23, 2.07) HR (95% CI): 1.48 (1.04, 2.11) HR (95% CI): 1.14 (0.94, 1.38) HR (95% CI): 1.73 (1.29, 2.32) HR (95% CI): 1.73 (1.16, 2.56) HR (95% CI): 1.14 (0.92, 1.41) 1033 Hospitalizations 1407 ED visits 19,780 OPD visits *, Low physical functioning, score 25; hazard ratios for SRH are for poor Chamberlain AM, et al. J Am. Heart Assoc. 2014;28(3):e
96 Quality of Life in HF Mortality Meta-Analysis (x17 papers w >100 pts ea) N= 10,793 KCCQ < 50 = poor health status MLHFQ > 45 = poor health status Mastenbroek MH, et al. Euro H Heart Fail. 2014;16(4):

97 Quality of Life in HF- A Goal NOT to Be Missed When it comes to HF, ~ 44% of patients do not recognize early HF symptoms, 1 & most patients do not recognize HF exacerbation 2 Assessment of physical functioning / symptoms via a HR- QoL tool may optimize assessment & treatment optimize QoL Year 1. Riegel B, et al. Heart Lung 2018; epub Jan Lee S, Reigel B. J Cardiovasc Nurs 2017; epub Aug 30 Males Females
98 Value of Assessing QoL If physical health impairments lead to hospitalization or mortality, and change in QoL score 1 month post hospitalization can predict early (60 day to 6 month) event free survival QoL score should be assessed at hospitalization and 1 month after discharge u To provide future hospitalization/survival risk u To help patients understand rationale for implementing interventions known to improve QoL
99 QoL Goals If we help patients understand QOL goals as part of usual care education (based on score improvements known to be associated with improved health status) We might enhance patient engagement and empowerment in HF self care Optimal self-care medication and nonpharmacologic management, including better HF monitoring might cost of care
100 Quality of Life in HF Predictors of Future Health Status 1458 pts. from EVEREST study; 6 Month Outcomes BNP BB dc BUN BL KCCQ h/o arrhythmia BNP h/o DM h/o arrhythmia Allen LA, et al. Circ. Cardiovasc Qual Outcomes. 2011;4(4):
101 QoL Goals More research is needed to determine if: A standard HF-related QoL tool should be systematically used Tool administration should be standardized in the OPD (every? months) and hospital at admission/post-discharge (? 30 days) u To determine CHANGE in scores Tool administration and FU burden is feasible - time to administer (~ 7 minutes), resources needed to administer/score/share results, communication with patient


102 102
103 Contact Us to Learn More Tanya Lane Truitt, RN MS Senior Manager QSI Programs & Operations: Resuscitation & HF Get With The Guidelines Liz Olson, CVA Program Manager, Get With The Guidelines Heart Failure Stay informed on the latest updates from all of the Get With The Guidelines programs. Sign Up for Focus on Quality e-communications
104 Thank you for your active participation and contributions to GWTG-Heart Failure! 2/13/ , American Heart Association
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
Tuesday October 18, :00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc
 Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
FINANCIAL DISCLOSURE: No relevant financial relationship exists
 The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works?
 UCSD Heart Failure Symposium Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA The Eliot Corday Professor of Cardiovascular
UCSD Heart Failure Symposium Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA The Eliot Corday Professor of Cardiovascular
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
The role of remote monitoring in preventing readmissions after acute heart failure
 The role of remote monitoring in preventing readmissions after acute heart failure October 20, 2017 Randall C Starling MD MPH FACC FAHA FESA FHFSA Professor of Medicine Kaufman Center for Heart Failure
The role of remote monitoring in preventing readmissions after acute heart failure October 20, 2017 Randall C Starling MD MPH FACC FAHA FESA FHFSA Professor of Medicine Kaufman Center for Heart Failure
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Case (Coding Nightmare) Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding. Current Dilemmas in Heart Failure :
 Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding. Current Dilemmas in Heart Failure :") Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding Interim Vice Chair for Clinical Affairs Department of Medicine, University of Florida 1 2 Case (Coding Nightmare) 69
Current Dilemmas in Heart Failure : Closing the Gap between Clinical Care and Coding Interim Vice Chair for Clinical Affairs Department of Medicine, University of Florida 1 2 Case (Coding Nightmare) 69
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine
 WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data Safety Monitoring Board SOPRANO (J&J), EVALUATE-HF
WHAT IS ADVANCED HEART FAILURE? James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data Safety Monitoring Board SOPRANO (J&J), EVALUATE-HF
HFA- ESC criteria for Advanced HF and US Requirements for Destination Therapy
 HFA- ESC criteria for Advanced HF and US Requirements for Destination Therapy ESC- HFA criteria for Adv-HF Severe symptoms of HF (NYHA class III or IV) with episodes of fluid retention and/or peripheral
HFA- ESC criteria for Advanced HF and US Requirements for Destination Therapy ESC- HFA criteria for Adv-HF Severe symptoms of HF (NYHA class III or IV) with episodes of fluid retention and/or peripheral
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 ACC/AHA/HFSA FOCUSED UPDATE 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure A Report of the American College of Cardiology/American Heart Association
ACC/AHA/HFSA FOCUSED UPDATE 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure A Report of the American College of Cardiology/American Heart Association
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed
 Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Known Actions of Digoxin
 Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management
 Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
The Role of Exercise in Management of Patients with Heart Failure
 The Role of Exercise in Management of Patients with Heart Failure Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Leadership Council and Section Director,
The Role of Exercise in Management of Patients with Heart Failure Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Leadership Council and Section Director,
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Heart Failure 2014: It's No Longer about Failure
 Ohio-ACC Spring Summit 2014: 7th Annual CCA Cardiovascular Update & 51st Annual Carl J. Wiggers Memorial Lecture Heart Failure 2014: It's No Longer about Failure Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP
Ohio-ACC Spring Summit 2014: 7th Annual CCA Cardiovascular Update & 51st Annual Carl J. Wiggers Memorial Lecture Heart Failure 2014: It's No Longer about Failure Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE. Marc Ferrini (Lyon Fr)
") What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
What s new in 2016 Guidelines of the European Society of Cardiology? HEART FAILURE Marc Ferrini (Lyon Fr) Palermo (I) 1 04 2017 Consulting Fees, Honoraria: BAYER PHARMA BOEHRINGER INGELHEIM BRISTOL MEYERS
3/2/2017. Identifying the Patient for Advanced Therapies. Why is Identifying the Adv HF patient important? CHF Stages and Steps of Treatment
 Identifying the Patient for Advanced Therapies Cindy Bither Chief NP- Adv HF Program Medstar Heart and Vascular Institute Stage A High risk with no symptoms Stage B Structural heart disease, no symptoms
Identifying the Patient for Advanced Therapies Cindy Bither Chief NP- Adv HF Program Medstar Heart and Vascular Institute Stage A High risk with no symptoms Stage B Structural heart disease, no symptoms
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Gerasimos Filippatos MD, FESC, FCCP, FACC
 Gerasimos Filippatos MD, FESC, FCCP, FACC Head of HF Unit at Athens University Hospital, Greece President (2014-2016) of the HF Association of the European Society of Cardiology (ESC) Served as Chair of
Gerasimos Filippatos MD, FESC, FCCP, FACC Head of HF Unit at Athens University Hospital, Greece President (2014-2016) of the HF Association of the European Society of Cardiology (ESC) Served as Chair of
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
All Roads Lead to HF. Presenter Disclosure Information. After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure CAD.
 Nothing Multiple New Therapies for Heart Failure CAD.") After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure Larry A. Allen, MD, MHS Director for Advanced Heart Failure October 18, 2016 Presenter Disclosure Information I will not discuss
After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure Larry A. Allen, MD, MHS Director for Advanced Heart Failure October 18, 2016 Presenter Disclosure Information I will not discuss
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
A Hospital-based Approach to Achieving Better Health Outcomes in Heart Failure
 A Hospital-based Approach to Achieving Better Health Outcomes in Heart Failure This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided by Postgraduate Institute
A Hospital-based Approach to Achieving Better Health Outcomes in Heart Failure This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided by Postgraduate Institute
Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association
 Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association We combed through both guidelines and summarized 3 recommendations
Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association We combed through both guidelines and summarized 3 recommendations
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs?
 How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target
 Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target JEFFREY S. BORER, M.D. Professor and Chairman, Department of Medicine and Chief, Division of Cardiovascular Medicine; Director,
Take-home Messages from Recent Heart Failure Trials: Heart Rate as a Target JEFFREY S. BORER, M.D. Professor and Chairman, Department of Medicine and Chief, Division of Cardiovascular Medicine; Director,
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal?
 Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal? Ileana L. Piña, MD, MPH Professor of Medicine, Epi/Biostats Case Western Reserve University Graduate VA Quality Scholar Cleveland
Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal? Ileana L. Piña, MD, MPH Professor of Medicine, Epi/Biostats Case Western Reserve University Graduate VA Quality Scholar Cleveland
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks
 Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks 12th Annual Leadership Summit on Health Disparities & Congressional Black Caucus Spring Health
Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks 12th Annual Leadership Summit on Health Disparities & Congressional Black Caucus Spring Health