DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
|
|
|
- Randell Davis
- 5 years ago
- Views:
Transcription
1 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution of Telestroke Network Recent advances in endovascular stroke treatment Endovascular stroke treatment outcomes 1
2 Stroke System of Care A comprehensive, diverse, longitudinal system that address all aspects of stroke care in an organized and coordinated manner Spans the spectrum of stroke care from primary prevention, calling 9-1-1, acute care, secondary prevention, rehabilitation, return to the community As with any system, it is only as strong as its weakest link STROKE SYSTEMS: EMS EMS -First point of contact Trained dispatchers Paramedics trained in stroke recognition Deliver patients to nearest ER capable of acute stroke management Pre-arrival notification EMS Their initial assessments, actions, treatments, and decisions will have significant consequences in the patient s subsequent care Their role in patient triage, diversion, and routing cannot be under-estimated 2
3 Characteristics of Different Stroke Centers Comprehensive Stroke Center Academic Medical Center Tertiary Care facility Primary Stroke Center Wide range of hospitals; standard stroke care; stroke unit; use TPA Acute Stroke Ready Hospital Rural hospitals; basic care; drip and ship; use tele-technologies Acute Stroke Ready Hospitals Typically small facilities Located remotely away from a PSC or CSC Typically serve small cities or rural populations Stroke population small; likely 1 patient a week on average Limited staffing and bed availability Concept: EMS would take patient to nearest ASRH for: 1. initial diagnosis 2. acute stabilization 3. acute treatments 4. then send patient to nearest PSC or CSC STROKE SYSTEMS SPOKES / PRIMARY STROKE CENTER Able to care for uncomplicated stroke patients Have access to advance imaging (CT/CTA ± MRI/MRA) and emergent neurology support (In-house or via telestroke system) Initiate IV tpa treatment in safe and efficient manner Admit post IV tpa patient if they have stroke unit/primary stroke center designation 3
.")
4 STROKE SYSTEMs HUB / COMPREHENSIVE STROKE CENTER Able to care for complex stroke patients Endovascular stroke, aneurysm coiling/clipping, AVM/AV fistulas treatments Availability of Vascular neurologists & Neurosurgeons Neurointerventionalist Neurointensivists Neuroradiologist Neuro-rehab team The creation of PSCs is strongly recommended (Class I, Level B). The development of CSC is recommended (Class I, Level C) Certification of stroke centers by an external body, such as JCAHO, is encouraged (Class I, Level B) Patients should be transported rapidly to the closest available certified PSC or CSC or, if no such centers exist, the most appropriate institution that provides emergency stroke care as described in the statement (Class I; Level of Evidence A). In some instances, this may involve air medical transport and hospital bypass. (Revised from the previous guideline13) REGIONAL STROKE HUBS University of Toledo Medical Center Promedica Toledo Hospital DISCLAIMER: NEITHER OF THESE HOSPITALS HAVE COMPREHENSIVE STROKE CENTER DESIGNATION AS OF NOW 4


5 TELESTROKE NETWORK BRIDGE BETWEEN HUB & SPOKE NETWORK PARTNERS TOLEDO HOSPITAL Baypark Hospital Fostoria Hospital St. Luke s Hospital Bellevue Hospital Lima Memorial Hospital Defiance Hospital Fremont Hospital Flower Hospital Hillsdale Hospital, MI UTMC Henry County Hospital Wood County Hospital Firelands Regional Medical Center Magruder Hospital Fulton County Hospital Mercy Hospital at Monroe, MI Bixby and Herrick Hospitals, MI 5

 TELESTROKE Audebert et al.")

6 TELESTROKE SYSTEM Mobile cart at the spoke ER and ICUs Real time 2 way AV connectivity through desktop or portable device (laptop, smartphone etc.) TELESTROKE Audebert et al. Cerebrovasc Dis 2005 BENEFITS OF TELESTROKE SYSTEM OF CARE Outcomes comparable to Comprehensive Stroke Center No increase in complication rate 6

7 BENEFITS OF TELESTROKE SYSTEM OF CARE Increase # of tpa treatments Decreased instances of protocol deviation Improved timing and efficiency IMPACT OF TELESTROKE 12 months prior to telestroke networking # of IV tpa treatments = 2 12 months post telestroke networking # of IV tpa treatments = 8 NEUROINTERVENTIONAL STROKE SERVICE JUL 2012 nov


8 IMS 3 Started in 2004 NIH funded IV tpa + Intervention VS. IV tpa 2:1 NIHSS 8 or > Planned >900 Pt 8



9 9


10 10

11 IMS - CRITICISMS STUDY SPECIFIC Selection criteria Vessel imaging not a requirement: 100/434 patients in the IA arm did not receive any treatment. Perfusion studies not mandatory SITE SPECIFIC Poor rate of recanalization Selection Bias Plenty of low volume centers SNIS Statement The most reasonable way to perform an analysis of the IMS3 cohort is to look at patients with large vessel occlusion on CTA prior to randomization. There were 282 patients with confirmed large vessel occlusion on CTA. Statistically significant difference by the Van Elteren test with p value of 0.01 which meet the stringent predefined alpha value for secondary analysis of

12 Recent Studies MR CLEAN- Netherlands ESCAPE- North America- Europe EXTEND IA- Australia SWIFT PRIME- International REVASCAT- Spain HISTORY 33 year old woman post C section day # 10 Family history of hypercoagulable state Sudden onset stroke symptoms while visiting her newborn in NICU NIHSS 14 12




13 PRE & POST TREATMENT 13
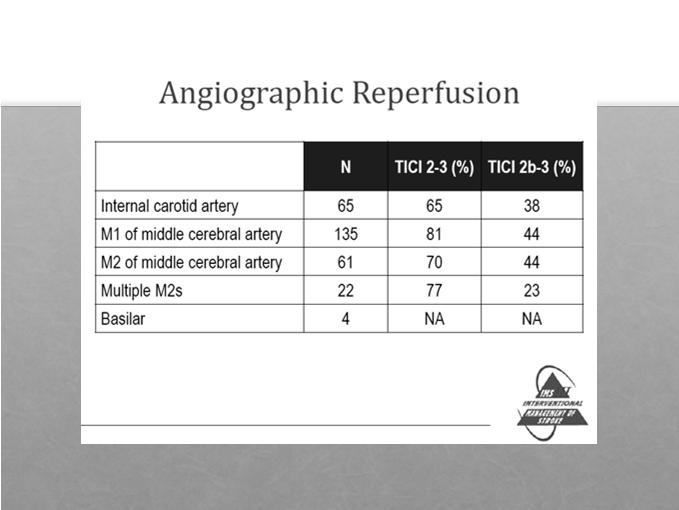
14 FOLLOW UP NIHSS 3 next Am Left facial droop Mild sensory loss Sensory extinction 90 days mrs = 1 TOLEDO ENDOVASCULAR STROKE EXPERIENCE JUL 2012 Nov PATIENTS 1 patient is currently in-hospital BASELINE DEMOGRAPHICS, CLINICAL & RADIOLOGICAL PRESENTATION, TREATMENT TIMES AND SPECIFICS 14
 CT Perfusion: 37 (23%) MRI DWI: 7 (4%) Mean ASPECT score 8 CASE: MULTIMODAL NEUROIMAGING 49 YO WOMAN WITH SLURRED SPEECH & MILD LHP X 24 HRS NIHSS")
15 DEMOGRAPHICS Mean Age 68 WOMEN 91/162 (56%) HTN 78% DM 40% AFIB 42% CAD 41% DYSLIPIDEMIA 70% SMOKING 30% Baseline Characteristics Median NIHSS 18, IQR (14-22) Pretreatment scan for selection: Plain Head CT: 118 (73%) CT Perfusion: 37 (23%) MRI DWI: 7 (4%) Mean ASPECT score 8 CASE: MULTIMODAL NEUROIMAGING 49 YO WOMAN WITH SLURRED SPEECH & MILD LHP X 24 HRS NIHSS 6 15



16 PRESENTATION CTA 30 HRS SINCE SYMPTOM ONSET NIHSS 13 16



17 PRE & POST INTERNVENTION POST PROCEDURE SCAN FOLLOW UP Clinically improved NIHSS 48 hrs Discharged to rehab mrs 90 days 17
18 TREATMENT TIMES TIME TO ONSITE ARRIVAL (MINS) Median 156 (IQR ) Mean 227 (SD 252) TIME TO GROIN PUNCTURE (MINS) Median 258 (IQR ) Mean 354 (SD 325) TIMES CONT. TIME TO RECANALIZATION (MINS) Median 339 (IQR ) Mean 430 (SD 351) PROCEDURE TIME (MINS) MEDIAN 60 (1QR 45-95) MEAN 71 (SD 41) OCCLUSION SITE MCA M1 91 (56%) MCA M2 ONLY 11 (7%) ICA T 30 (18%) Tandem 19(12%) Basilar 11 (7%) Side 52% Left hemispheric 18




19 81 yo woman with NIHSS 21. Last known well over 8 hrs ago PRESENTATION CT HEAD FIRST ANGIO RUN POST PROCEDURE RUN POST PROCEDURE MR 19
 IA tpa 21 (13%) IA tpa Only 6 (4%) TREATMENT SPECIFICS MERCI 25 (15%) Stentreiver 78")
20 FOLLOW UP Patient improved on the table Discharged home Mild expressive hesitancy no other deficits Clinically back to 3 months mrs - 0 TREATMENT SPECIFICS Pre treatment with IV tpa IV tpa:65/162 (40%) IA tpa 21 (13%) IA tpa Only 6 (4%) TREATMENT SPECIFICS MERCI 25 (15%) Stentreiver 78 (48%) 20
- ADAPT:12, Manual 32 MANUAL ASPIRATION MANUAL ASPIRATION - ADAPT TECHNIQUE")
21 TREATMENT SPECIFICS Penumbra separator 2 (1%) Proximal ICA stenting 14 (12%) Aspiration Alone 44 (27 %)- ADAPT:12, Manual 32 MANUAL ASPIRATION MANUAL ASPIRATION - ADAPT TECHNIQUE 21


22 22



23 RESULTS RECANALIZATION, CLINICAL OUTCOMES & COMPLICATIONS RECANALIZATION 23
24 RECANALIZATION SUCCESSFUL FAILED COMPLETE PARTIAL NONE TIMI/TICI 3 TIMI 2 TICI 2A&B WHAT IS GOOD RECANALIZATION? TICI Grade flow Higashida & Furlan. Stroke 2003;34;e109- e137 TICI 0 No Perfusion. No antegrade flow beyond the point of occlusion. TIMI Grade Flow Khatri P, Neff J, Broderick JP, et al. Stroke 2005; 36:2400 TIMI 0 No perfusion TICI 1 Penetration With Minimal Perfusion. The contrast material passes beyond the area of obstruction but fails to opacify the entire cerebral bed distal to the obstruction for the duration of the angiographic run. TIMI 1 Perfusion past the initial occlusion, but no distal branch filling TICI 2a Only partial filling (<2 3) of the entire vascular territory is visualized. TIMI 2 Perfusion with incomplete or slow distal branch filling TICI 2b Complete filling of all of the expected vascular territory is visualized, but the filling is slower than normal. TICI 3 Complete Perfusion. Antegrade flow into the bed distal to the obstruction occurs as promptly as into the obstruction and clearance of contrast material. TIMI 3 Full perfusion with filling of all distal branches, including M 3, 4 RESULTS - RECANALIZATION TIMI 2 & 3 138/162 (85%) TICI 2B & 3 116/162 (72%) 24


25 RESULTS - OUTCOMES Favorable outcome 66/162 (40.7%) ALL PATIENTS mrs 0 mrs 1 mrs 2 mrs 3 mrs 4 mrs 5 mrs RESULTS OUTCOMES BASED ON RECANALIZATION Favorable outcome in TICI2B/3 group: 51% Favorable Outcome in non- recanalized patients: 11% RECANALIZATION & OUTCOMES mrs 0 mrs 1 mrs 2 mrs 3 mrs 4 mrs 5 mrs 6 TICI 2B & TICI 0, 1, 2A % 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% RESULTS - OUTCOMES Overall mortality 39/162 (24%) 25



26 VARIABLES INFLUENCING OUTCOME Age Mean age in patients with favorable outcome 63 VS. 70, p Recanalization 51% VS. 11%, p <0.01 AGE THE KEY FACTOR 82 YEAR OLD WITH RT MCA OCCLUSION NIHSS 20 OTT 135 MINS R ICA TERMINUS OCCLUSION 26


27 FOLLOW UP Excellent clinical recovery NIHSS 24 hrs Discharged home on Day # 3 27





28 Sometimes you can not reach 56 yom with transient LOC and a residual visual field deficit became comatose on day of D/C. Not a tpa candidate Sometimes you can not reach Attempted access for 4 hours, injected 20 mg tpa in r occipital and L VA Sometimes you can not reach Patient was locked in for 45 days, died due to multi-system failure 28





29 Sometimes you should not try 75 yof with multiple comorbidities presented 2 hours after a R ICA syndrome with NIHSS of 18 Patient received IV tpa CTA showed tandem occlusion CTP showed severe perfusion profile Sometimes you should not try Sometimes you should not try Angio shows tandem occlusion, stenting of proximal lesion was performed 29




30 Sometimes you should not try Angioplasty and stenting was performed Sometimes you should not try Balloon was reinflated to stop the bleeding. Patient did poorly. Sometimes you can not WIN 48 YOF with multiple comorbidities was in cath lab holding area after NSTEMI when she had a severe L ICA syndrome, NIHSS 24 30



31 Sometimes you can not win CT head did not show any acute changes, tpa not given due to being on Heparin gtt and recent MI. Angio showed L ICA terminus occlusion, racanalized in 80 minutes from onset time Sometimes you can not win Patient had a large stroke with rapid edema (likely reperfusion injury). She herniated within 24 hours. Family did not want surgical tx. COMPLICATIONS HT 1 & 2 16% Parenchymal Hemorrhage 10 (6%) Perforation/SAH 2 Distal embolization to a new territory 5 31
32 SOME PERSPECTIVE TREVO SWIFT IMS 3 Recanalization % * Day mrs 0-2 % Day Mortality % Major Hemorrhage % TOLEDO Recanalization % 72% 90 Day mrs 0-2 % 41% 90 Day Mortality % 24% Major Hemorrhage % 5.1% MR CLEAN (N ) TOLEDO (N 162 ) AGE NIHSS % IV tpa % MCA % RECANALIZATION % FAV OUTCOME Thank you 32
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Stroke Systems of Care. Sharon Webb, MD, FAANS, FACS, FAHA
 Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Vote Using Your Phone!
 Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Primary Versus Comprehensive: What is the Difference?
 Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical Center Dallas, TX
 Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Mark J. Alberts, MD. Turning the Wheels of Stroke Care
 Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Mission: Lifeline Stroke Nebraska
 Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
DISCLOSURES. Learning Objectives. David Lee Gordon, MD, FAHA Update in Stroke 2007 FINANCIAL DISCLOSURE UNLABELED/UNAPPROVED USES DISCLOSURE
 Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Where are we heading and where are the big challenges?
 Where are we heading and where are the big challenges? Christopher Levi Neurologist, John Hunter Hospital, Newcastle & Liverpool Hospital, Sydney Executive Director, Sydney Partnership for Health Education
Where are we heading and where are the big challenges? Christopher Levi Neurologist, John Hunter Hospital, Newcastle & Liverpool Hospital, Sydney Executive Director, Sydney Partnership for Health Education
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs
 The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion
 How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS
 Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Optimizing Care for Patients with Acute Ischemic Stroke Thrombolytic Therapy for Low NIHSS Nerses Sanossian, MD, FAHA Presentation not eligible for CME credit Disclosures Today s objectives Case study:
Supplementary Online Content
 Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified