Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
|
|
|
- Silvia Rogers
- 6 years ago
- Views:
Transcription
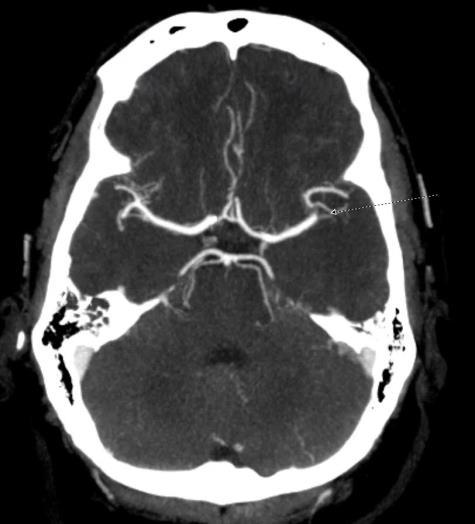
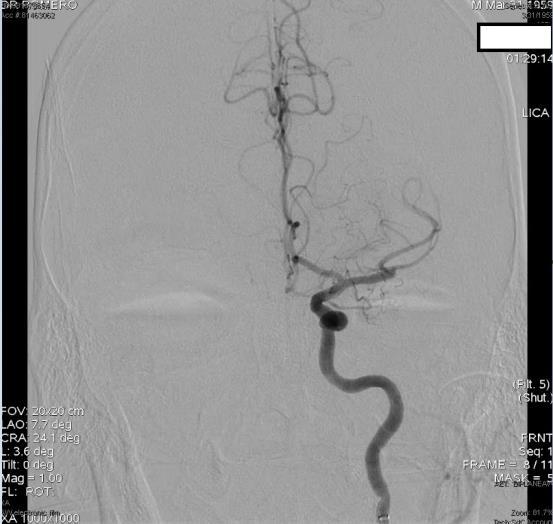
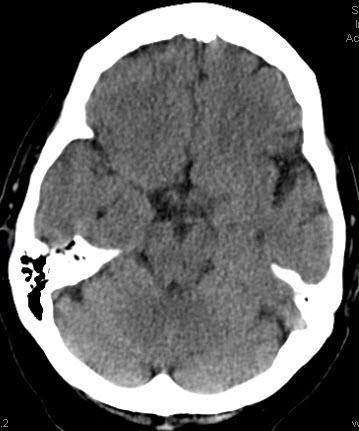
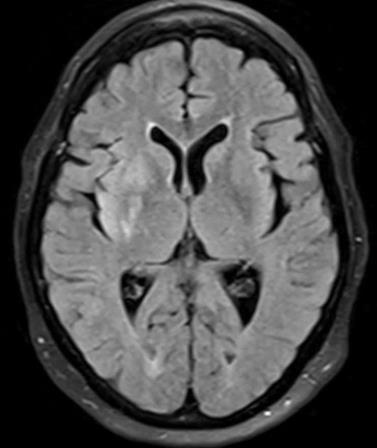
1 Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with PMhx of Dementia, HTN, HLD, hypothyroid presents to UPMC Hamot on 9/24/16 as regional stroke alert for sudden onset left-sided flaccidity and right gaze preference. Last seen well at approximately 7:30 am At 8:15 am she was noted to be walking into the wall She developed left-sided weakness and right gaze preference She was evaluated at OSH, reported NIH was 21 Head ct reported to be without ICH and patient was given iv tpa at am No CD of images performed was sent with patient On arrival she has LUE weakness, moved BL LE to commands Fixed R gaze, and was mute. NIH = 24 She had SBP in 170s and appeared to be in no acute respiratory distress 1
 0 = Ask patient current month and age (answers both=0, one=1, neither=2) 0 = Ask patient to open and close eyes (performs both=0, one task=1,")

2 Neurologic Examination (NIH Stroke Scale) = Level of consciousness (alert=0, arouses minor=1, arouses pain=2, unresponsive=3) 0 = Ask patient current month and age (answers both=0, one=1, neither=2) 0 = Ask patient to open and close eyes (performs both=0, one task=1, neither=2) 0 = Best gaze (normal=0, partial gaze palsy=1, forced deviation=2) 0 = Visual field testing (no loss=0, partial HA=1, complete HA=2, bilateral HA=3) 0 = Facial palsy (normal=0, minor ie. smile=1, partial ie. lower face=2,complete=3) 0 = Motor function left arm (no drift=0, drift=1, gravity=2, no gravity=3, no movement=4) 0 = Motor function right arm (no drift=0, drift=1, gravity=2, no gravity=3, no movement=4) 0 = Motor function left leg (no drift=0, drift=1, gravity=2, no gravity=3, no movement=4) 0 = Motor function right leg (no drift=0, drift=1, gravity=2, no gravity=3, no movement=4) 0 = Limb ataxia (absent=0,present 1 limb=1,present 2 limb=2) 0 = Sensory (normal=0, diminished=1, total=2) 0 = Best language (no aphasia=0, mild=1,severe=2,global/mute=3) 0 = Dysarthria (none=0, mild/mod=1, inintelligible=2) 0 = Extinction and inattention (normal=0, inattention=1, profound=2) = Total score Case 1 No CD of images performed was sent with patient 2

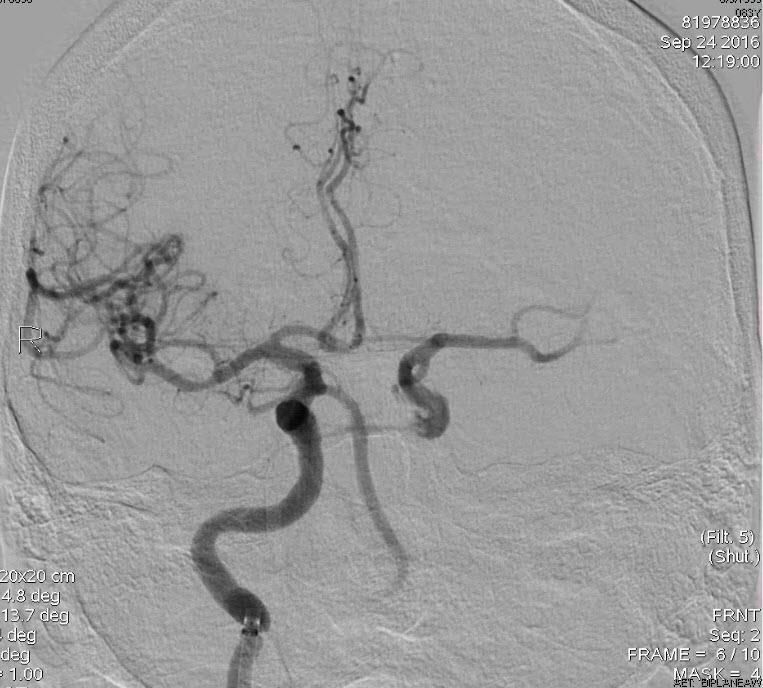
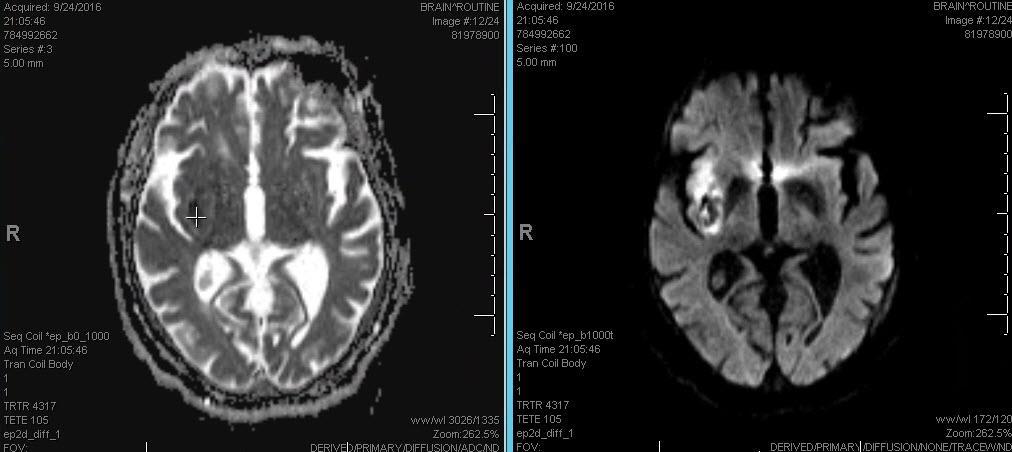
3 Case 1 Case 1 POD#4 NIHSS=4 3

4 Hemorrhagic Transformation Subtypes Cerebrovasc Dis 2010;29: Overview Background Does Size Matter? Small vessel occlusion? Large vessel occlusion? Additional Comments 4
5 Background Background - The US Food and Drug Administration approval of IV tpa in The concept of stroke as a treatable emergency was a major shift in clinical practice - Following tpa approval - in-hospital stroke code teams were formed - primary and comprehensive stroke centers were developed and proliferated - vascular neurology emerged as a discrete specialty 5
6 Background Effects of Stroke Centers - maximize the number of patients treated with tpa - minimize delays to initiation of tpa treatment - held hospitals to evidence-based standards for inpatient management across the spectrum of cerebrovascular diseases - developed emergency medical systems (EMS) stroke protocols & guidelines - transport patients to stroke centers where they were most likely to receive tpa with the shortest delays Stroke 2016: 316:12654 Background Effects of Stroke Centers (cont) - Public education campaigns for the recognition of stroke signs and urgency of calling now more common on billboards and public service announcements - Tele-stroke programs were developed to direct stroke thrombolysis decisions at hospitals without the in-house expertise - Developed large stroke registries to track tpa statistics and performance metrics - provided insights about stroke risk factors, demographics, prevention, and outcomes - More recently, established the efficacy of endovascular thrombectomy for reducing disability from large artery ischemic stroke Stroke 2016: 316:
 2 Does Size Matter?")
7 Background Evolution of Thrombectomy Approaches and Devices J NeuroInterv Surg 2015:(7) 2 Does Size Matter? 7
 had symptomatic hemorrhage Among 104 patients, 28 patients were treated conservatively and 76 with thrombolysis Studied showed that resolution of a HMCAS confirmed to be M1-MCA")
8 Size Matters 114 patients acute M1- MCA stroke & hyperdense MCA sign Confirmed CT angiography or conventional angiogram Ten patients were excluded due to unavailable or uninterpretable follow-up scans; half (5/10) had symptomatic hemorrhage Among 104 patients, 28 patients were treated conservatively and 76 with thrombolysis Studied showed that resolution of a HMCAS confirmed to be M1-MCA thrombus on CT angiography is highly length dependent J Neuroimaging 2014;24:7-10 Size Matters Studied showed that resolution of a HMCAS confirmed to be M1-MCA thrombus on CT angiography is highly length dependent Disappearance of the HMCAS on the follow up scans was noted in 43 (41%) patients and was length dependent with thrombus length <10mm showing nearly 70% resolution (P <.001) and volume dependent (P <.002) In all treatment groups, shorter thrombus length and smaller volumes were associated with a greater probability of resolution at follow-up. J Neuroimaging 2014;24:7-10 8

9 Small vessel occlusion? Small Vessel Stroke Lacunar Infarction: small subcortical infarcts that result from occlusion of a single perforating artery. Typically caused by intrinsic disease of small vessels called lipohyalinosis, resulting from HTN and DM Literature demonstrates that emboli can too be the cause of lacunes Most lacunar infarcts do not present with stroke. That is, unrecognized ( silent ) lacunar infarcts are at least 5 times more common than symptomatic infarcts When symptomatic, lacunar infarcts present with lacunar syndromes, 5 of which are well documented: pure motor stroke, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis, and dysarthria (ie, clumsy hand) Stroke 2004;35:


10 Large vessel occlusion? Large Vessel Stroke 10



11 Treatment Helps Patients With Worst Kind of Stroke Systematic Review of Recent Trials - Endovascular treatment versus medical care - 10 randomized controlled trials enrolling 2925 patients with ischemic stroke - pooled analysis of these trials yielded statistically significant and clinically relevant effects - statistically significant heterogeneity was found among the results of the studies Heterogeneity was driven by - differences in methodological and clinical features between studies - disparities in inclusion criteria and in the interventions considered - the proportion of patients who underwent intravenous thrombolysis & adjunctive i-a mechanical thrombectomy - the type of devices used for thrombectomy BMJ 2016: 353:i

 In the intervention arm, use of intravenous rt-pa ranged from 0% in SYNTHESIS to 100% in IMS III, EXTEND-IA, SWIFT PRIME, THERAPY, and THRACE.")
12 Systematic Review of Recent Trials - Endovascular treatment versus medical care - Allowed posterior circulation strokes Included strokes within the internal carotid artery and/or M1 and/or M2 portions of the middle cerebral artery Utilized perfusion imaging depicting potentially salvageable brain tissue BMJ 2016: 353:i1754 Systematic Review of Recent Trials - Endovascular treatment versus medical care - allowed other endovascular interventions (intra-arterial rt-pa and urokinase-type plasminogen activator) in addition to thrombectomy (>68% also received IV rt-pa) (77% - 100%) (28.1%) In the intervention arm, use of intravenous rt-pa ranged from 0% in SYNTHESIS to 100% in IMS III, EXTEND-IA, SWIFT PRIME, THERAPY, and THRACE. BMJ 2016: 353:i1754 In SYNTHESIS, intravenous rt-pa was not administered owing to the study design (the study compared endovascular treatments, such as intra-arterial rt-pa and thrombectomy, with intravenous thrombolysis). 12
 was more than 86% (86.1% to 100%) BMJ 2016: 353:i1754 Recanalization rates varied between 25.0% - 88.")
 Systematic Review of Recent Trials - Good functional outcomes & Mortality at 90 days - Overall, 1129 out of 2907 patients (38.")
13 Systematic Review of Recent Trials - Endovascular treatment versus medical care - MR RESCUE and THERAPY no stent retrievers were used Most 2015 studies the rate of stent retriever use (such as Solitaire FR, Solitaire 2, Trevo, Catch) was more than 86% (86.1% to 100%) BMJ 2016: 353:i1754 Recanalization rates varied between 25.0% % according to a score of 2b/3 (perfusion of half or greater of the vascular distribution of the occluded artery) Recanalization rates greater than 58% observed in MR CLEAN, ESCAPE, EXTEND-IA, SWIFT PRIME, REVASCAT, and THERAPY (most were treated with stent retrievers) Systematic Review of Recent Trials - Good functional outcomes & Mortality at 90 days - Overall, 1129 out of 2907 patients (38.8%) achieved a good functional outcome at 90 days BMJ 2016: 353:i1754 Pooled risk ratio for 2015 trials was 1.56, representing an increase of 167 patients attaining a good outcome (modified Rankin scale score 2) for each 1000 additional patients receiving endovascular treatment compared with medical care alone. 13
14 Systematic Review of Recent Trials - Good functional outcomes & Mortality at 90 days - At 90 days, 482 out of 2880 participants (16.7%) died, without differences between arms in all cause mortality BMJ 2016: 353:i1754 Overall, 129 out of 2526 patients (5.1%) experienced symptomatic intracerebral hemorrhage, with no significant differences between treatment groups. Furthermore, there were no significant differences between the results of trials published in 2013 and Systematic Review of Recent Trials - Endovascular treatment versus medical care - Pivotal factors explaining statistically significant and clinically relevant results of 2015 randomized controlled trials (but not among the 2013 trials) - focus on large vessel occlusion scenarios - the selection of patients with less extensive brain tissue damage - the use of two simultaneous endovascular reperfusion techniques (IV rt-pa and thrombectomy) - the use of more efficient devices 14
15 Systematic Review of Recent Trials - Endovascular treatment versus medical care - Weaknesses of current trials despite multicenter RCT - Not powered enough to evaluate the safety of endovascular treatment - including adjunctive intra-arterial mechanical thrombectomy. - Observational studies may be more adequate than RCT to evaluate safety - as these may include patients who are usually excluded from RCT, and follow-up is often longer - Lastly, the magnitude of effects may have been exaggerated - by stricter patient selection - by a higher level of study site selection - by increased interventionist proficiency compared with the real world BMJ 2016: 353:i1754 Systematic Review of Recent Trials - Endovascular treatment versus medical care - Considering the pathophysiology of ischemic stroke - Faster, more efficient recanalization is of paramount importance - reduce the infarction of penumbral brain tissue - contribute to improved clinical outcomes - Prompt administering of intravenous rt-pa as well as timely intravascular intervention like achieved in the 2015 studies may have contributed to less brain tissue damage - Patients undergoing adjunctive intra-arterial mechanical thrombectomy for anterior LVO are - twice as likely to be without disability times as likely to be functionally independent 90 days 15
 Pooled individual patient data from the 5 positive trials Investigate efficacy in subgroups too")

16 Systematic Review of Recent Trials - Endovascular treatment versus medical care - JAMA Sep2016: 316(12)1279 Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES collaboration) Pooled individual patient data from the 5 positive trials Investigate efficacy in subgroups too small to be conclusive in the individual trials Study results showed no heterogeneity of the treatment effect across pre-specified subgroups Number needed to treat with thrombectomy of 2.6 patients to achieve a reduction in disability of at least 1 level on the modified Rankin score JAMA Sep2016: 316(12)
 - only 15% were 80 years of age or older - same proportion had contraindications to IV thrombolysis The trials covered only a very")

17 Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES collaboration) Several clinically important areas are under-represented in HERMES. Although older patients (better represented than in previous trials) - only 15% were 80 years of age or older - same proportion had contraindications to IV thrombolysis The trials covered only a very narrow range onset-to-treatment time - only 208 patients were randomized later than 5 h from onset - and only 69 patients beyond 6 h Questions regarding technical issues (remain unanswered) - the place for aspiration techniques - need for balloon guiding catheter - the need for additional intra-arterial thrombolytic drugs Lancet Apr2016 Vol387 'faster is better' it's all about speed." Pooled data from 1287 patients (5 Trials) 634 who received endovascular thrombectomy plus thrombolysis 653 who received thrombolysis alone time from symptom onset to randomization = 196 minutes (~3 hrs) In the endovascular group, mean time: symptom onset to arterial puncture = 238 minutes (~4 hrs) mean time: symptom onset to reperfusion = 286 minutes (~5 hrs) At 90 days, the mean mrs score was 2.9 in the endovascular group and 3.6 in the thrombolysis-alone group JAMA Sep2016: 316(12)
18 'faster is better' it's all about speed." Among every 1000 patients achieving substantial endovascular reperfusion for every 15-minute faster emergency department door-to-reperfusion time: -an estimated 39 patients would have a lessdisabled outcome at 3 months JAMA Sep2016: 316(12)1279 -including 25 more who would achieve functional independence (mrs 0-2) 'faster is better - meta-analysis (cont) The odds of better disability outcomes at 90 days (mrs distribution) declined with longer time from symptom onset to arterial puncture: Odds ratio (OR) - 3 hours = hours = hours = 1.57 Statistical significance was retained through 7 hours and 18 minutes (438 minutes) JAMA Sep2016: 316(12)
1279 each 1-hour delay to reperfusion was associated with - less favorable degree of disability (OR, 0.")
 - no significant change in mortality 'faster is better - meta-analysis (cont) Considering outcome distributions across all mrs health states, for every 9-minute delay in symptom onset to")
19 'faster is better - meta-analysis (cont) Rates of functional independence after thrombectomy 64% with reperfusion at 3 hours 46% with reperfusion at 8 hours Among 390 patients who achieved substantial reperfusion with endovascular thrombectomy JAMA Sep2016: 316(12)1279 each 1-hour delay to reperfusion was associated with - less favorable degree of disability (OR, 0.84) - less functional independence (OR, 0.81) - no significant change in mortality 'faster is better - meta-analysis (cont) Considering outcome distributions across all mrs health states, for every 9-minute delay in symptom onset to substantial endovascular reperfusion time, 1 of every 100 treated patients had a worse disability outcome (higher score by 1 or more levels on the mrs). The probability of functional independence (mrs 0-2) at 3 months declined from 64.1% with symptom onset to-reperfusion time of 180 minutes to 46.1% with symptom onset to-reperfusion time of 480 minutes. JAMA Sep2016: supp2 19
 The")

20 Systematic Review of Individual Patient Data - Endovascular treatment versus medical care - Distribution of mrs scores by treatment population at 90 days For the primary outcome, pooled data showed reduced chance of disability at 90 days in patients assigned to thrombectomy versus those assigned to control (adjusted cor 2 49, 95% CI ; p<0 0001) The number needed to treat for one patient to have reduced disability of at least 1 point on mrs was 2.6 Lancet Apr2016 Vol387 Systematic Review of Individual Patient Data - Endovascular treatment versus medical care - Mortality at 90 days and risk of parenchymal hematoma type 2 and symptomatic intracranial hemorrhage did not differ between populations Lancet Apr2016 Vol387 20
21 ? Eligibility by Time and by Imaging Mechanical thrombectomy 6 hours after symptom onset is the new standard of care However, when faced with the scenario of a patient presenting at 10 hours after symptom onset who fulfills the imaging and clinical criteria, should this patient be offered endovascular treatment? Does time of onset or neuroimaging determine patient eligibility for endovascular treatment? The best answer would be a combination of both features The ischemic tissue core grows with time Case 2 57 y.o. white male with PMH of HTN, HLD, PVD with peripheral stents who presented to the ED as a stroke alert from home. Per EMS, patient went to bed at 6PM, around 11:00PM wife was up and heard him coughing in the bedroom, and then heard a thud. She found him on the ground next to the bed. He was not able to get up and would not answer her and that is when she called 911. On arrival (11:28PM), he is awake, alert but globally aphasic, not speaking or following commands. He has obvious right facial droop and right sided weakness. He has diminished pain response on the right. NIH 21 CTA showed a left MCA trifurcation clot. Neurointervention was called. 21


22 Case 2 Case 2 22

 formal assessment for revascularization by CEA or CAS at a later time (2)")
23 Case 2 NIHSS=21 Next morning NIHSS=3 Discharge (day 2) NIHSS=1? Tandem Extracranial and Intracranial Lesions One interesting finding is that patients with cervical carotid artery occlusive lesion in addition to the intracranial occlusion showed a dramatic treatment effect ESCAPE = cor 9.6 in favor of the endovascular treatment REVASCAT = cor 4.3 in favor of the endovascular treatment Optimal management of the cervical carotid artery occlusion is still unclear (1) formal assessment for revascularization by CEA or CAS at a later time (2) immediate angioplasty/stenting of the lesion before attending the intracranial occlusion (3) angioplasty/stenting of the lesion after attending the intracranial occlusion The efficacy and safety of periprocedural antiplatelet management of patients with carotid artery stents is also uncertain 23
24 New practice guidelines recommends thrombectomy for patients -patients who are free from disability prior to the stroke -have occlusion of the internal carotid artery or proximal middle cerebral artery -received treatment with tpa within 4.5 hours from of onset (if eligible) -have clinical severity of 6 or greater on the National Institutes of Health Stroke Scale -have a small infarct core defined as a score of 6 or greater (ASPECTS) -and can have the procedure (arterial puncture) initiated < 6 hours from symptom onset The guidelines also include recommendations about -the need to optimize systems of care to increase access -reduce times to treatment, without a specific prescription for how to do so Additional Comments 24
25 Additional comments Transfers from local hospitals to endovascular-capable stroke centers must increase and must be accomplished with the utmost speed Sharing of vascular imaging by video links between the referring facilities and receiving facilities could potentially save an estimated 30 to 45 minutes by allowing for patients to be transported directly to the angiography suite Patients transferred between facilities had a delay of 2 hours compared with those taken straight to an endovascular center Less than 5% of all stroke patients may be candidates for endovascular thrombectomy therapy, new triage approaches for stroke need to be evaluated, as has previously occurred in the successful evolution of care for trauma and acute coronary syndrome. Additional comments Meta analysis provides evidence that potentially supports strengthening of recommendations for treatment from 6 through 7 hours 18 minutes after symptom onset The potential benefit of earlier times to thrombectomy require substantial system changes to reduce workflow delays. Aggressive goals of Endovascular-capable stroke centers - 60 minutes from hospital arrival to arterial puncture - 90 minutes from hospital arrival to achievement of substantial reperfusion 25
26 Case 3 symptom onset 13:15 pre hospital stroke alert called at 13:47 patient arrived 14:21 blood glucose 97 ct clear 14:33 tpa started 14:47 thrombectomy procedure start time 15:33 Case 3 74 year old female with no known past medical history. She denies any medical history or medications. She was an event today with her daughter and had a witnessed onset of sudden left sided flaccidity and facial droop. This occurred at precisely At that time she dropped her purse and the bags she was carrying. She admits to having a headache but denies chest pain, sob or palpitations. She has never had symptoms such as these before. Air transferred to UPMC and arrived as a prehospital stroke alert. NIHSS=17 26




27 Case 3 NIHSS=17 Case 3 27

28 Case 3 NIHSS=1 28
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
BGS Spring Conference 2015
 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows
Supplementary Online Content
 Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
HERMES Time and Workflow Primary Paper. Statistical Analysis Plan
 HERMES Time and Workflow Primary Paper Statistical Analysis Plan I. Study Aims This is a post-hoc analysis of the pooled HERMES dataset, with the following specific aims: A) To characterize the time period
HERMES Time and Workflow Primary Paper Statistical Analysis Plan I. Study Aims This is a post-hoc analysis of the pooled HERMES dataset, with the following specific aims: A) To characterize the time period
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
From interventional cardiology to cardio-neurology. A new subspeciality
 From interventional cardiology to cardio-neurology. A new subspeciality in the future? Prof. Andrejs Erglis, MD, PhD Pauls Stradins Clinical University Hospital University of Latvia Riga, LATVIA Disclosure
From interventional cardiology to cardio-neurology. A new subspeciality in the future? Prof. Andrejs Erglis, MD, PhD Pauls Stradins Clinical University Hospital University of Latvia Riga, LATVIA Disclosure
Patient selection for i.v. thrombolysis and thrombectomy
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
AHA/ASA Guideline. Downloaded from by on November 7, 2018
 AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health
 what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
what do the numbers really mean? NIHSS Timothy Hehr, RN MA Stroke Program Outreach Coordinator Allina Health NIHSS The National Institutes of Health Stroke Scale (NIHSS) is a tool used to objectively quantify
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Pr Roman Sztajzel Service de Neurologie HUG
 Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Overview. Introduction. New Interventions for Acute Stroke. New Approaches to hemorrhagic Strokes
 Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Supplementary Online Content
 Supplementary Online Content Lapergue B, Blanc R, Gory B, et al; ASTER Trial Investigators. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic
Supplementary Online Content Lapergue B, Blanc R, Gory B, et al; ASTER Trial Investigators. Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Interventional Revolution in Treatment of Stroke
 TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Acute Management of Stroke due to Intracranial Steno-occlusion. Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital
 Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
Acute Stroke Treatment KPNC Stroke EXPRESS
 Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Acute Stroke Treatment 2018 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke 1 Jeffrey G. Klingman, MD The Permanente Medical Group Stroke Treatment in the old days Prior to 1996:
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention
 Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Epidemiology. Epidemiology 6/1/2015. Cerebral Ischemia
 Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,
Presenter Disclosure Information Paul Nyquist MD/MPH FCCM FAHA Updates on the Acute Care of Ischemic Stroke and Intracranial Hemorrhage Updates on the Acute Care of Ischemic Stroke Paul Nyquist MD/MPH,