Anticoagulation Therapy and Valve Surgery. Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon
|
|
|
- Elvin Shelton
- 5 years ago
- Views:
Transcription


1 Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon
2 Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic heart valves 4. Managing anticoagulation treatment 5. Managing sub-therapeutic anticoagulation 6. Managing a high INR 7. Managing patients in need of peri-procedure temporary reduction / discontinuation of anticoagulation


3 Open Heart Surgery done in IJN
4 Valve Surgery (1) Human has 4 heart valves mitral, aortic, tricuspid and pulmonary Any valve may be diseased Indication for surgery varies If the valve disease is mild, it may be managed with medication only Severe valve disease often need surgery Timing of surgery is important some heart may be too sick for surgery
5 Valve Surgery (2) Commonest mitral and aortic valve Type of valve surgery Repair vs replacement Choice of heart valve mechanical vs tissue valve Factors determine type of valve age of patient female fertile age and plan for pregnancy Control of warfarin Bleeding tendency Patient life style
6 Mitral Valve Disease (1) Cause of mitral valve disease Rheumatic, Degenerative, Congenital, Infective, Type of lesion stenosis, regurgitation, mixed Surgery Repair vs replacement choice of heart valve mechanical vs tissue
7 Mitral Valve Disease (2) Mitral Regurgitation (MR) Many MR can be repaired Advantages no need long term anticoagulation better preservation of LV function Disadvantages more technical demanding not durable in some disease e.g. rheumatic
8 Mitral Valve Disease (3) Mitral Stenosis Valvotomy (a repair technique) is possible in some patient Can be done by cardiologist (PTMC) Present of LA clot need open heart surgery May need replacement surgery of too disease
9 Type of Heart Valve Repair surgery Commonest valve repair mitral valve Repair with annuloplasty ring need anticoagulation (warfarin) Repair without ring, no need Warfarin. Other valve repair Aortic valve repair no need anticoagulation Tricuspid valve repair with ring need anticoagulation Pulmonary valve repair no need anticoagulation
10 Advantages of Mitral Valve Repair (1) Mitral valve repair is preferred whenever technically feasible over valve replacement. Mechanical and biological prosthetic heart valves have distinct disadvantages. Mechanical valves need anticoagulation to prevent thromboembolism. Tissue valves have a relatively short durability (7 14 years).
11 Advantages of Mitral Valve Repair (2) Better preservation of LV function Avoidance of prosthesis related events Reduced hospital mortality Reduced morbidity and LOS Improved long term survival Thourani et al, Circulation 2003; 108: Zaho et al, JTCVS 2007; Shuhaiber J et al, EJCTS 2007; 31: Perrier P et al, Circulation 1984;70:187 Akins CW, et al. ATS 1994; 58:

; Type IIIa restricted")

12 Carpentier Classification of MV disease a Functional Approach Type I, normal leaflet motion; Type II, increased leaflet motion (leaflet prolapse); Type IIIa restricted leaflet motion during diastole and systole; Type IIIb restricted leaflet motion predominantly during systole.*
13 Etiology of Mitral Regurgitation Organic Degenerative Barlow s Dystrophic Marfan s Other Endocarditis Rheumatic Post-traumatic Functional Ischemic DCM Secondary to AS

14 Mitral Valve Nomenclature - a surgeon view P2 prolapse

15 Mitral Valve Repair with ring
16 Aortic Valve Disease (2) Aortic Regurgitation (AR) May be repairable in some cases e.g. bicuspid, infective endocarditis with perforation, ruptured sinus of valsalva secondary to congenital lesion like VSD Aortic root aneurysm with severe AR Might be repair with valve sparing procedure (David s procedure) Rheumatic AR usually replacement

17 Aortic Valve Disease (1) Aortic Stenosis Usually more difficult to repair especially in older patients Replacement more common Many elderly valve are severely calcified thus surgery can be quite challenging
18 Aortic Valve Disease (2) Aortic Regurgitation (AR) May be repairable in some cases e.g. Bicuspid, Infective endocarditis with perforation, Ruptured sinus of valsalva Secondary to congenital lesion like VSD Aortic root aneurysm with severe AR Might be repair with valve sparing procedure (David s procedure) Rheumatic AR usually replacement
19 Tricuspid Valve Disease (1) Tricuspid regurgitation usually repairable De Vega Tricuspid Annuloplasty commonest: Easy to do, cheap However, may be less durable Repair with ring More expensive Might be more durable Other technique
20 Tricuspid Valve Disease (2) Tricuspid Stenosis Not common May be congenital or rheumatic Some repairable
21 Pulmonary Valve Disease Pulmonary Valve Stenosis Mostly congenital Valvotomy may be possible if annulus of adequate size If pulmonary annulus too small- may need crossing of the valve (transannular patch repair)

22 Pulmonary Valve Disease Regurgitation usually well tolerated Severe pulmonary regurgitation Not common Possible cause Endocarditis Post, TOF repair
23 Anticoagulation requirements: All patients with a mechanical heart valve replacement need life-long anticoagulation with Warfarin. Some patients with bio-prosthetic heart valve replacements (or mitral valve repair) also may need anticoagulation. The level of anticoagulation (target INR) is defined by the cardiac surgeon at the time of the operation, and this information needs to be passed on to primary, and secondary care.
24 Anticoagulation requirements: - Biological (tissue) prosthetic heart valve Aortic position: No warfarin anticoagulation needed (current recommendation is only for an anti-platelet aggregatory agent, such as Aspirin, for 3 months post surgery), provided patient is in normal sinus rhythm and there is no other indication for anticoagulation. Mitral and Tricuspid position: Post-operative anticoagulation with Warfarin is recommended for 3 months only (Target INR 2.5), provided in normal sinus rhythm and there is no other indication for continued anticoagulation.
 are NOT licensed and are clearly CONTRA-INDICATED for use in patients with mechanical prosthetic heart valves.")
25 Anticoagulation requirements: (Mechanical (Metallic ) prosthetic heart valve) All patients with mechanical heart valves require life-long anticoagulation with a Vitamin K antagonist, i.e. Warfarin guided by regular monitoring of the international normalised ratio (INR) to inform dosing. New novel oral anticoagulants (e.g. Dabigatran, Rivaroxaban, Apixaban, Edoxaban, etc) are NOT licensed and are clearly CONTRA-INDICATED for use in patients with mechanical prosthetic heart valves.
26 Managing Anticoagulation Treatment Optimal anticoagulation in patients with mechanical heart valves is achieved by using a target INR. A median target INR value rather than a range is recommended in order to avoid considering extreme values in the range as being a valid INR, since values at either end of a range are not as safe and effective as median values. The optimal target INR with mechanical heart valves, depends on the varying thrombotic risk associated with different valve types, and patient-related risk factors:
27 Risk factors of Patient with higher thrombogenicity Previous thromboembolism; Atrial fibrillation Mitral stenosis of any degree, Left ventricular ejection fraction < 35%. (Ref 1)
28 Target INR in mechanical heart valve replacement Mechanical Prosthesis of low thrombogenicity Most current valve * Isolated Aortic Valve Replacement no risk factors 2.5 (2.0 to 3.0) Mitral or Tricuspid Valve Replacement 3.0 (2.5 to 3.5) Carbomedics, Medtronic Hall, St Jude Medical, On-X We currently do NOT endorse the company advertised claims that On-X aortic valve can have target INR s lower than that recommended in the above table

29 Target INR The target INR should be defined, and documented, in all cases by the cardiac surgeon performing the valve replacement at the time of the operation. Prior to discharge, tertiary care will make arrangements for ongoing INR monitoring and Warfarin dosing, either seamlessly through the GP surgery of the patient, or referral to the INR clinic responsible for overseeing the anticoagulation from here onwards.

30 Managing Sub-therapeutic anticoagulation (INR falls more than 0.5 below target INR) Point of Care testing machines may have a variance of ~ 0.5 and therefore in the first instance immediate repeat of INR is recommended with borderline low INR results. Review reason for sub-therapeutic anticoagulation and increase Warfarin accordingly. These patients will need bridging cover with Heparin.
31 Managing Sub-therapeutic anticoagulation (Bridging therapy) Intravenous unfractionated heparin (UFH) is the primary recommended treatment for patients with mechanical prosthesis. However, subcutaneous Low Molecular Weight Heparin (LMWH) at a therapeutic dosage, is accepted as an alternative for bridging especially in an outpatient setting. LMWH is relatively contraindicated, as it accumulates, in cases of severe renal failure (egfr 30 ml/min/1.73 m2 ). Contact Haematology for advice in these patients. The INR needs to be retested in 2 3 days, in order to guide warfarin dosage (after altering warfarin dosage, it takes ~ 48 hrs for the INR to change) until therapeutic
32 Managing a High INR Life threatening bleeding: Admit to hospital. Omit Warfarin. Intravenous vitamin K 5mg Prothrombin complex concentrate, usually units/kg, but dose-adjusted according to INR (under the supervision of a haematologist).
33 Managing a High INR Minor bleeding from mucosa (nose, oropharynx, urinary tract, rectum, anus) and High INR : INR < 6.0 but > 0.7 above target INR Reduce the warfarin dose (by 10 25%) & recheck INR in 1-2 days (half-life of warfarin is hours) INR > 6. Omit Warfarin for 1 2 days & recheck INR in 1-2 days, reintroducing at a lower maintenance dose when bleeding is under control or when INR < 5.0 Bleeding whilst in the therapeutic range is usually related to a pathological cause and needs to be identified and treated INR > 6 Omit Warfarin for 1 2 days & recheck INR in 1-2 days, reintroducing at a lower maintenance dose when bleeding is under control or when INR < 5.0 Bleeding whilst in the therapeutic range is usually related to a pathological cause and needs to be identified and treated
34 Managing a High INR No bleeding and High INR (INR > 6) Omit Warfarin for 1 2 days & recheck INR in 1-2 days, restart warfarin at a lower dose when INR <5.0,Where the perceived risk of bleeding is high, e.g. INR >8, or other risk factors for bleeding are present, consider administration of oral vitamin K (5.0 mg). In the presence of mechanical valves, reversal of anticoagulation with Vit K must be carefully assessed against perceived bleeding risk. If given, INR should be rechecked within hrs as heparin may be required if INR subsequently becomes subtherapeutic
35 Major surgical procedures require an INR of less than 1.5 depending upon bleeding risk: Warfarin anticoagulant therapy should be stopped 3 5 days before surgery (depending on current INR) and bridging using heparin is recommended once the INR falls more than 0.5 below target INR, usually 1 2 days after stopping Warfarin.
36 Intravenous unfractionated heparin Intravenous unfractionated heparin remains the only recommended heparin treatment in patients with mechanical prostheses and should be favoured over subcutaneous LMWH. The effects of LMWH cannot be fully reversed whereas UFH can be reversed with Protamine. If UFH is used: admit 2-3 days prior to
37 Intravenous unfractionated heparin If UFH is used: admit 2-3 days prior to surgery. Start IV UFH infusion once INR falls more than 0.5 below target, and aim for an APTT of Stop UFH 4 hours before surgery. [4] Restart IV heparin (no loading dose) as soon as post op bleeding risk is low (usually 6 8 hrs after procedure) and surgeon is happy with haemostasis. Restart Warfarin: at the patient s usual maintenance dose (no loading) 24 hrs after procedure. Continue IV heparin until the INR is within 0.5 of target INR (4) Standardized Low-Molecular-Weight Heparin bridging regimen in outpatients on oral anticoagulant undergoing invasive procedure or surgery. Italian Federation of centers for the diagnosis of thrombosis and management of antithrombotic therapies (FCSA). Circulation 2009;119:
 The Joint Task Force of the European Society of Cardiology (ESC) and the European Association for Cardio- Thoracic Surgery (EACTS) Eur J Cardiothorac Surg. 2012 Oct;42(4):S1-44, Eur Heart J.")
38 References: 1. Guidelines on the management of valvular heart disease (version 2012.) The Joint Task Force of the European Society of Cardiology (ESC) and the European Association for Cardio- Thoracic Surgery (EACTS) Eur J Cardiothorac Surg Oct;42(4):S1-44, Eur Heart J Oct;33(19): Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. The Task Force of the European Society of Cardiology (ESC) and endorsed by the European Society of Anaesthesiology (ESA. ) Europ Heart J 2009; 30: The perioperative management of antithrombotic therapy. Douketis JD, Berger PB Dunn AS et al. (Am Coll Chest Phys). Chest 2008;133:299S-339S 4. Standardized Low-Molecular-Weight Heparin bridging regimen in outpatients on oral anticoagulant undergoing invasive procedure or surgery. Italian Federation of centers for the diagnosis of thrombosis and management of antithrombotic therapies (FCSA). Circulation 2009;119:
39 Guideline for warfarin dosing in hospital Check patient warfarin previous dose. If no previous dose, starting 3 mg daily x 2 days (standard healthy adult) INR on day 3 INR < 1.2, increase dose to 5 mg daily x 2 days, rpt INR INR increase dose to 4mg daily x 2 days, rpt INR INR 1.6 to 1.9 decrease dose to 2mg daily, rpt INR INR > 2.0, omit warfarin, check INR next day.
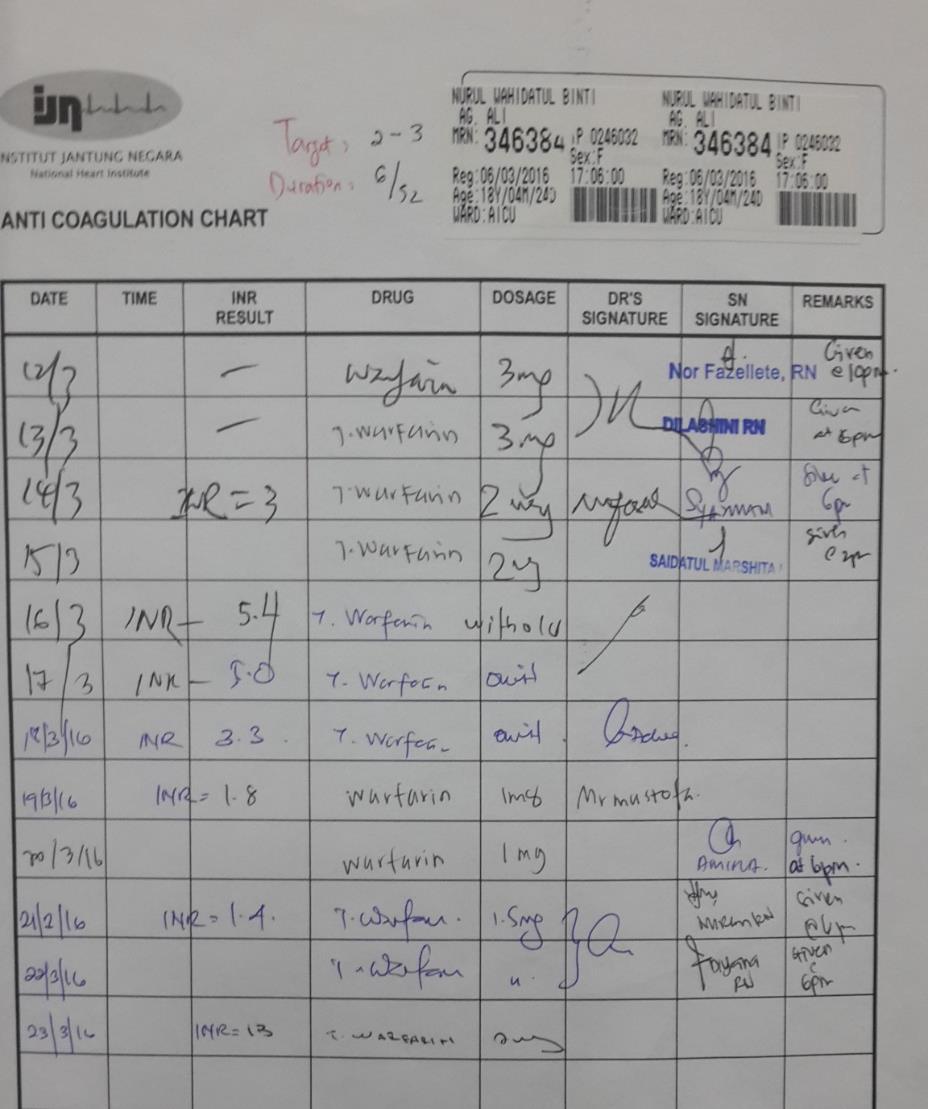
40 INR monitoring chart

41 INR monitoring chart




42 THANK YOU IJN Expansion 2005 onwards
Intrinsic + Common = aptt. Extrinsic + Common = PT. Common Pathway
 Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
Anticoagulant Cases 12 11 Intrinsic + Common = aptt 9 8 10 7 4 Extrinsic + Common = PT 5 2 Common Pathway 1 Xa Inhibitors rivaroxaban (Xarelto) apixaban (Eliquis) edoxaban (Savaysa) What is true regarding
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Guidelines for Anticoagulation in Paediatric Cardiac Patients
 Leeds Children s Hospital Guidelines for Anticoagulation in Paediatric Cardiac Patients SURGICAL PATIENTS Preoperative Management Blalock-Taussig (BT) Shunt / Fontan circulation / Sano Shunt and Severe
Leeds Children s Hospital Guidelines for Anticoagulation in Paediatric Cardiac Patients SURGICAL PATIENTS Preoperative Management Blalock-Taussig (BT) Shunt / Fontan circulation / Sano Shunt and Severe
Oral anti-thrombotic therapy-management in patients requiring endoscopy
 Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Primary Care practice clinics within the Edmonton Southside Primary Care Network.
 INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Warfarin in Adults : Guidelines for the use of. These guidelines apply to all patients commenced or continuing on warfarin
 Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
Warfarin in Adults : Guidelines for the use of Document Type: Clinical Guideline Clinical Lead: Ian Neilly Author/s: Ian Neilly/Paul Barbieri Directorate: Haematology Approved by Haematology Specialty
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Clinical Practice Guideline for Anticoagulation Management
 Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC
 A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy *C.V. was born the 24th May 1980 Rheumatic fever during
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Management of Anticoagulation during Device Implants; Coumadin to Novel Agents
 Management of Anticoagulation during Device Implants; Coumadin to Novel Agents DR D Birnie Invited Faculty Core Curriculum Heart Rhythm Society May 8 th 2014 Disclosures Boehringer Ingleheim Research Support
Management of Anticoagulation during Device Implants; Coumadin to Novel Agents DR D Birnie Invited Faculty Core Curriculum Heart Rhythm Society May 8 th 2014 Disclosures Boehringer Ingleheim Research Support
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Pathology Service User Guide Haematology
 Pathology Service User Guide Haematology St Richard s This section of the Pathology Service User Guide includes: Anticoagulant Therapy Information about the Anticoagulant Clinic Low Molecular Weight Heparin
Pathology Service User Guide Haematology St Richard s This section of the Pathology Service User Guide includes: Anticoagulant Therapy Information about the Anticoagulant Clinic Low Molecular Weight Heparin
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
The Pendulum of Bridging Periprocedural Anticoagulant Therapy. Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA
 The Pendulum of Bridging Periprocedural Anticoagulant Therapy Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA Disclosures Department of Veterans Affairs Industry Relationships:
The Pendulum of Bridging Periprocedural Anticoagulant Therapy Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA Disclosures Department of Veterans Affairs Industry Relationships:
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Joost van Veen Consultant Haematologist
 Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY
 EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve. Diana Aicher. September 16 th - 18 th 2015
 Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Reconstruction of the Aortic Valve and Root A Practical approach Why and when to repair the aortic valve Diana Aicher September 16 th - 18 th 2015 Why repair the aortic valve? Aortic Valve Replacement
Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF
 or stroke prevention in non-valvular AF") Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF Traffic light classification- Amber 2 specialist initiation / recommendation Information
Edoxaban for the treatment and prevention of venous thromboembolism (DVT or PE) or stroke prevention in non-valvular AF Traffic light classification- Amber 2 specialist initiation / recommendation Information
Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Maternal Cardiac Disease Diagnosis and Management
 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
NOAC Prescribing in Patients with Non-Valvular Atrial Fibrillation: Frequently Asked Questions
 AC Prescribing in Patients with Non-Valvular Atrial Fibrillation: Frequently Asked Questions FAQ document jointly prepared by NHSGGC Haematology Service & Medicines Infmation On behalf of the Heart MCN
AC Prescribing in Patients with Non-Valvular Atrial Fibrillation: Frequently Asked Questions FAQ document jointly prepared by NHSGGC Haematology Service & Medicines Infmation On behalf of the Heart MCN
North East Essex Medicines Management Committee
 Colchester Hospital University NHS Foundation Trust North East Essex Clinical Commissioning Group North East Essex Medicines Management Committee ORAL ANTICOAGULANT (Vit K antagonist only) MANAGEMENT GUIDELINES
Colchester Hospital University NHS Foundation Trust North East Essex Clinical Commissioning Group North East Essex Medicines Management Committee ORAL ANTICOAGULANT (Vit K antagonist only) MANAGEMENT GUIDELINES
Appendix 3 PCC Warfarin Reversal
 Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı
 ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
Results of Aortic Valve Preservation and Repair
 Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
Results of Aortic Valve Preservation and Repair Department of Cardiothoracic and Vascular Surgery Cliniques Universitaires St. Luc Brussels, Belgium Gebrine Elkhoury Institutional experience in AV preservation
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT
 WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
WMC PHARMACY ANTICOAGULATION PROTOCOL Current Revision: July 2017 GENERAL ORDER PROCESSING AND MANAGEMENT - Entering orders for anticoagulation in Cerner Providers will enter individual orders (oneoffs)
Edoxaban For preventing stroke and systemic embolism in people with non-valvular atrial fibrillation (NICE TA 355)
") Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban For preventing stroke and systemic embolism in people with non-valvular atrial fibrillation (NICE TA 355) This document supports
Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban For preventing stroke and systemic embolism in people with non-valvular atrial fibrillation (NICE TA 355) This document supports
PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR
 PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR ARE MEDTRONIC HEART VALVE REPAIR THERAPIES RIGHT FOR YOU? Prosthetic (artificial) heart valve repair products are used by physicians to
PATIENT BOOKLET MEDTRONIC MITRAL AND TRICUSPID HEART VALVE REPAIR ARE MEDTRONIC HEART VALVE REPAIR THERAPIES RIGHT FOR YOU? Prosthetic (artificial) heart valve repair products are used by physicians to
WARFARIN: PERI OPERATIVE MANAGEMENT
 WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart van Putte, Nabil Saouti. St. Antonius Hospital, Nieuwegein, The Netherlands
 Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Minimal Invasive Mitral Valve Surgery After Previous Sternotomy Without Aortic Clamping: Short- and Long Term Results of a Single Surgeon Single Institution Kinsing Ko, Thom de Kroon, Najim Kaoui, Bart
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
A new era in cardiac valve surgery has begun...
 THE CENTER FOR VALVE SURGERY A new era in cardiac valve surgery has begun... Good Help to Those in Need Rawn Salenger, MD, FACS, Director, The Center for Valve Surgery Edward F. Lundy, MD, PhD, Chief of
THE CENTER FOR VALVE SURGERY A new era in cardiac valve surgery has begun... Good Help to Those in Need Rawn Salenger, MD, FACS, Director, The Center for Valve Surgery Edward F. Lundy, MD, PhD, Chief of
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
NOACS/DOACS*: COAGULATION TESTS
 NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
NOACS/DOACS*: COAGULATION TESTS OBJECTIVES: To describe the effect of the newer direct oral anticoagulants (DOACs) on laboratory coagulation tests which are widely available: prothrombin time (PT), international
pat hways Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16
 pat hways Anticoagulants, including non-vitamin K antagonist oral anticoagulants (NOACs) Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16 Options for local implementation NICE
pat hways Anticoagulants, including non-vitamin K antagonist oral anticoagulants (NOACs) Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16 Options for local implementation NICE
Anticoagulation. MPharm Programme & OSPAP Programme. Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics
 MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
Perioperative Management. Perioperative Management of Cardiovascular Medications
 of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
WARFARIN: PERI-OPERATIVE MANAGEMENT
 WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation
 HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
HEART OF THE MATTER: cardiac issues in safe endoscopy & sedation YUVAL KONSTANTINO M.D. CARDIOLOGY DEPARTMENT, ELECTROPHYSIOLOGY UNIT, SOROKA MEDICAL CENTER, BEN-GURION UNIVERSITY OUTLINE 1 2 3 Anticoagulation
Bridging Anticoagulation: The Peri-Procedural Management of Patients on Oral Anticoagulants
 Bridging Anticoagulation: The Peri-Procedural Management of Patients on Oral Anticoagulants Dr Stuti Kaul Consultant Haematologist Dr Ruth Medlock Consultant Haematologist Lee Wilson Consultant Pharmacist
Bridging Anticoagulation: The Peri-Procedural Management of Patients on Oral Anticoagulants Dr Stuti Kaul Consultant Haematologist Dr Ruth Medlock Consultant Haematologist Lee Wilson Consultant Pharmacist
Is there a place for new anticoagulants in prosthetic valves?
 Is there a place for new anticoagulants in prosthetic valves? Patrizio Lancellotti, MD, PhD, FESC, FACC University of Liège Hospital, GIGA Cardiovascular Sciences, Heart Valve Clinic, Department of Cardiology,
Is there a place for new anticoagulants in prosthetic valves? Patrizio Lancellotti, MD, PhD, FESC, FACC University of Liège Hospital, GIGA Cardiovascular Sciences, Heart Valve Clinic, Department of Cardiology,
Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins
 Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Transoesophageal echocardiography and decision making in valve surgery
 Transoesophageal echocardiography and decision making in valve surgery Intraoperative evaluation of the surgical results in aortic valve / root surgery Catherine Szymanski Disclosures None Sino-tubular
Transoesophageal echocardiography and decision making in valve surgery Intraoperative evaluation of the surgical results in aortic valve / root surgery Catherine Szymanski Disclosures None Sino-tubular
2 Summary of NICE TA 249: Atrial fibrillation - Dabigatran Etexilate
 Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy
 Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
VALVULAR HEART DISEASE AND PULMONARY CIRCULATION
 ESC CONGRESS HIGHLIGHTS VALVULAR HEART DISEASE AND PULMONARY CIRCULATION N. Ajmone Marsan (Leiden, NL) MD, PhD, FESC Conflicts of Interest None CONTENTS Pulmonary arterial hypertension Rheumatic heart
ESC CONGRESS HIGHLIGHTS VALVULAR HEART DISEASE AND PULMONARY CIRCULATION N. Ajmone Marsan (Leiden, NL) MD, PhD, FESC Conflicts of Interest None CONTENTS Pulmonary arterial hypertension Rheumatic heart
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline on the management of excessive coumarin anticoagulation in adults
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline on the management of excessive coumarin anticoagulation in adults
Rivaroxaban film coated tablets are available in 2 strengths for this indication: 15mg and 20mg.
 Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Valvular heart disease (VHD) is present in 2.5% of the
 is present in 2.5% of the") 2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
Indications and Late Results of Aortic Valve Repair
 Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Indications and Late Results of Aortic Valve Repair Prof. Gebrine El Khoury Department of Cardiovascular and Thoracic Surgery Cliniques St. Luc Brussels, Belgium Aortic Valve Repair Question # 1 Can the
Valve Analysis and Pathoanatomy: THE MITRAL VALVE
 : THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
: THE MITRAL VALVE Marc R. Moon, M.D. John M. Shoenberg Chair in CV Disease Chief, Cardiac Surgery Washington University School of Medicine, St. Louis, MO Secretary, American Association for Thoracic Surgery
t. Recommendations for periprocedural anticoagulation are available lhrough the American College of Chest Physicians Clinical Practice Guidelines.
 Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Date 29 th March 2018 Our Ref FA_Anticoag/MGPG/Mar18 Enquiries to Frances Adamson Extension Direct Line tadamson(anhs.
 NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS NHS Grampian Date 29 th March 2018 Our Ref FA_Anticoag/MGPG/Mar18 Enquiries to Frances Adamson Extension 56689 Direct Line 01224 556689
NHS Grampian Westholme Woodend Hospital Queens Road ABERDEEN AB15 6LS NHS Grampian Date 29 th March 2018 Our Ref FA_Anticoag/MGPG/Mar18 Enquiries to Frances Adamson Extension 56689 Direct Line 01224 556689
An Audit of the Post-Operative Management of Patients taking Warfarin
 An Audit of the Post-Operative Management of Patients taking Warfarin Helen Wrightson Pre-Registration Pharmacist, Salisbury District Hospital March 2014 An Audit of the Post-Operative Management of Patients
An Audit of the Post-Operative Management of Patients taking Warfarin Helen Wrightson Pre-Registration Pharmacist, Salisbury District Hospital March 2014 An Audit of the Post-Operative Management of Patients