A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC
|
|
|
- Judith Pearson
- 5 years ago
- Views:
Transcription
1 A pregnant patient with a prosthetic valve Giacomo Boccuzzi, MD, FESC Department of Invasive Cardiology, Ospedale San Giovanni Bosco, Turin, Italy
 with mechanical valves Sorin")

2 *C.V. was born the 24th May 1980 Rheumatic fever during childhood Normal development until adulthood. At the age of 25 years she underwent a double valve replacement (aortic and mitral) with mechanical valves Sorin Bicarbon 21 Sorin Bicarbon 27 *Courtesy of M. Bollati 1, W. Grosso Marra 1, I. Sheiban 1, F.Gaita 1, V. Donvito 2, T. Todros 2. 1 Division of Cardiology, University of Torino, Molinette Hospital. 2 Division of Internal Medicine, O. San Anna, Torino.

3 She had excellent results after surgery. NYHA I. TTE: Normal left ventricular systolic function. LV Ejection fraction: 60%. Regular function of the mechanical valves. At the age of 28 years the patient came to us for preconceptional counselling. Preconceptional counselling has to address: 1. The risk for the mother 2. The risk for the fetus 3. The maternal life expectancy 4. The risk of recurrence in the offspring

4 According to the WHO risk classification, what is the maternal cardiovascular risk of this patient? in press
5 According to the WHO risk classification, what is the maternal cardiovascular risk of this patient? 1. RISK CLASS 1 2. RISK CLASS 2 3. RISK CLASS 3 4. RISK CLASS 4


6 1. RISK CLASS 1 2. RISK CLASS 2 3. RISK CLASS 3 4. RISK CLASS 4
7 Why are the maternal and offspring risks elevated in a patient with a prosthetic valve? Haemodynamically, women with well-functioning mechanical valves tolerate pregnancy well. The physiological changes of pregnancy induce a prothrombotic environment, reinforcing the requirement for effective anticoagulation.

8 Why are the maternal and offspring risks elevated in a patient with a prosthetic valve? The need for anticoagulation therapy raises concerns because of: Oral anticoagulation therapy: provide effective protection against thromboembolism but --- cross the placenta Heparin-type drugs do not cross the placenta but are less effective in protection against thromboembolism Haemorragic complications MOTHER Increased risk of valve thrombosis
9 Why are the maternal and offspring risks elevated in a OACs patient with a prosthetic valve? direct Fetal Haemorrage secondary Spontaneous abortion Stillbirth Teratogenicity Offspring complications
 Prior cardiac events (heart failure, TIA/Stroke, arrthymias)? No 4) Prior pregnancies? No 5) Therapy? Out of warfarin (coumadin 1+1/2 tablets die: 7.")
10 How can we estimate the magnitude of the maternal and fetal risk in this patient? History: 1) Symptoms? No. 2) Functional capacity? NYHA I 3) Prior cardiac events (heart failure, TIA/Stroke, arrthymias)? No 4) Prior pregnancies? No 5) Therapy? Out of warfarin (coumadin 1+1/2 tablets die: 7.5 mg die) no other therapy Physical examination: Negative for signs of heart failure. ECG: Normal sinus rhythm. TTE: Normal left ventricular systolic function. Ejection fraction: 60%. Regular function of mechanical valves (aortic and mitral bileaflet valves). No gradient or significant regurgitation.
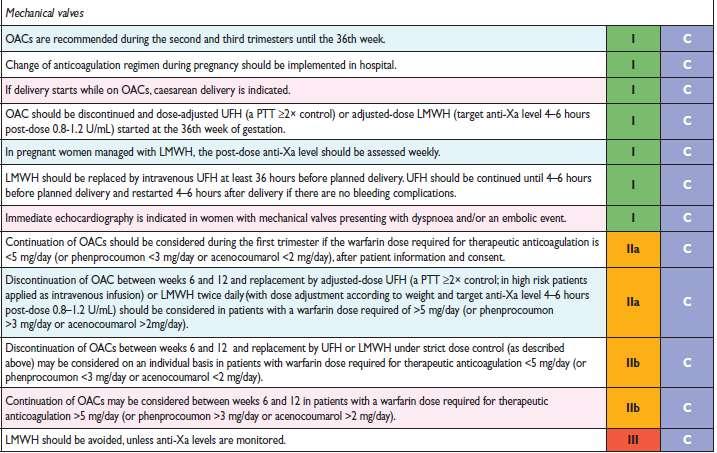
11 There are several regimens for pregnant women with mechanical heart valves. Which will be your choice? 1. Unfractioned heparin throughout pregnancy 2. Unfractionated heparin (UFH) and warfarin combination 3. LMWH and warfarin combination 4. LMWH throughout the pregnancy 5. Warfarin throughout pregnancy
12 Counseling We discuss with the patient the different therapeutic options and we planned our strategy: 1)The importance of very early diagnosis of pregnancy was stressed (if she misses a menstrual period she should be tested immediately for pregnancy) 2)Discontinuation of OAC between weeks 6 and 12 and replacement by LMWH twice daily (with dose adjustment according to weight and target anti-xa level)
13 The character and magnitude of the risk depend on the anticoagulation regimen used during pregnancy and the quality of anticoagulation control. Maternal thromboembolic complications % Spontaneous abortions % OAC throughout [1-7] Congenital fetal anomalies % Unfractionated heparin 1st trimester + OACs [1-7] Heparin use between 6-12 wk Heparin use after 6 wek Unfractionated heparin throughout LMWH throughout LMWH 1st trimester + OACs (limited data) [1-7] Vitale N, J Am Coll Cardiol 1999 May;33(6): Fuster V Circulation 1982;66(Suppl 1): Yeh TJ Circulation 1967;35(Suppl 1): Chan WS Arch Intern Med 2000 Jan 24;160(2): Nassar AH, Am J Obstet Gynecol 2004 Sep ;191(3): Meschengieser SS. Heart 1999 Jul;82(1): Lee JH J Korean Med Sci 2007 Apr;22(2):258 61
14 LABOUR/DELIVERY Last menstrual period: February 10 th Positive pregnancy test weeks: she discontinued coumadin and started enoxaparin 6000 U.I (1mg/kg body weight) twice daily subcutaneously. The anti Xa level was repeatedly checked:
15 What is the optimal sampling time of anti Xa level? Immediately after injection 12 hours after injection 4-6 hours after injection Sampling time is not relevant
16 What is the optimal sampling time of anti Xa level? Immediately after injection 12 hours after injection 4-6 hours after injection Sampling time is not relevant The therapeutic antifactor Xa range is: U/mL
17 LABOUR/DELIVERY Last menstrual period: February 10 th Positive pregnancy test weeks: she discontinued coumadin and started enoxaparin 6000 U.I (1mg/kg body weight) twice daily subcutaneously. The anti Xa level was repeatedly checked: March 24 th 0.8, April 17 th : 0.9 May 26 th :0.77 Visit + Tranthoracic Echo was performed at weeks. (Fetal echo was performed weeks) 33 week. Planned vaginal delivery was decided. 34 week she discontinued coumadin and started enoxaparin 6000 U.I (1mg/kg body weight) twice daily subcutaneously. October 28 th she stopped enoxaparin and October 29 th (37 weeks gestation) She had an uneventful induced vaginal delivery resulting in delivery of a healthy boy (Apgar 5/7).
18 POSTPARTUM PERIOD The enoxaparin was restarted 12 hours after the delivery. She was discharged three days after delivery. She still was taking enoxaparin 6000 U.I twice daily and coumadin (INR <2). The anti-xa level was not checked The same day the patient came to the emergency department complaining of sudden but self-resolving diplopia. Physical examination was negative for signs of heart failure. A grade 2/4 aortic diastolic murmur was heart
19 Differential Diagnosis? TIA in atrial fibrillation Intracerebral Hemorrhage in a patient on oral anticoagulation therapy + LMWH TIA in Prosthesis malfunction

20 CT scan of head: no lesion ECG: normal sinus rythm

21 Transthoracic Doppler echocardiography Severe aortic prosthesis regurgitation due to incomplete leaflet apposition, with a significantly increased prosthetic aortic transvalvular gradient (peak velocity 4.4 m/s, peak gradient 76mmHg, mean gradient 49mmHg), whereas the mitral valve prosthesis appeared normal.
22 Differential Diagnosis? TIA in atrial fibrillation Intracerebral Hemorrhage in a patient on oral anticoagulation therapy + LMWH TIA in Prosthesis malfunction

23 Transoesophageal echocardiography Revealed a thrombus (about 8 x 6 mm) located between the two prostheses, causing intermittent aortic valve malfunction Due to the stable clinical condition, no thrombolytic therapy was started, but intravenous unfractioned heparin was initiated and maintained.
, but an oval thrombus (with length 15mm and width 2mm) was detected")
 was evident adhering to the aortic prosthesis annulus, without")
24 3 days later Transoesophageal echocardiogram revealed: a decreased aortic transvalvular gradient (peak 35mmHg), but an oval thrombus (with length 15mm and width 2mm) was detected adhering to the mitral prosthesis and fluctuating through the prosthetic valve. Another smaller thrombus (7mm) was evident adhering to the aortic prosthesis annulus, without prosthesis malfunction.

25
 and intravenous infusion (0.6mg/kg in 30min).")
 were placed in both common")
26 Due to the high embolic risk, alteplase was given as a bolus (0.27 mg/kg) and intravenous infusion (0.6mg/kg in 30min). To minimize the risk of cerebral embolization, carotid filters (Filter Wire EZ, Boston Scientific) were placed in both common carotid arteries.


27 No complication occurred during and after the procedure, and after evidence of thrombus dissolution 30min after the end of alteplase infusion at transoesophageal echocardiography, filters were removed The patient continued intravenous heparin + coumadin until achievement of therapeutic international normalized ratio range ( ) and she was asymptomatic when discharged the following week.

28 Where did we went wrong? Oral anticoagulant (OACs) therapy until 5 week gestation We stopped OACs between weeks 6 and 12 and replacement by LMWH twice daily. The change of anticoagulation regimen was done at home. We stopped OACs at the 34 week gestation and replacement by LMWH twice daily. The vaginal delivery was planned 24 hours prior delivery we stopped LMWH. LMWH was restarted 12 h after delivery. OACs was restarted after 3 day and patient discharged in double therapy OACs +LMWH
29 in press
30 1 years follow up NYHA I. TTE: Normal left ventricular systolic function. LV Ejection fraction: 60%. Regular function of the mechanical valves. Take home message Pregnancy in women with mechanical heart valves is (very)? high risk. The role of the clinician is to discuss the pros and cons of the available options and when the strategy has been decided be very caution because just one mistake can change the outcome.

31 Grazie
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG)
") ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG) Beytullah ÇAKAL, MD Koşuyolu Kartal Heart Training and Research Hospital, Istanbul,
ThROmbolytIc TherApy of Prosthetic Heart Valve Thrombosis in PREGnancy with Low Dose Slow Infusion of t-pa (TROIA-PREG) Beytullah ÇAKAL, MD Koşuyolu Kartal Heart Training and Research Hospital, Istanbul,
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy
 ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy Task force on the management of CVD during pregnancy of the ESC Chair: Vera Regitz-Zagrosek, Charite, Berlin None DECLARATION
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism. Luigi P. Badano, MD, FESC
 EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
EAE RECOMMENDATIONS FOR TRANSESOPHAGEAL ECHO. Cardiac Sources of Embolism Luigi P. Badano, MD, FESC Background Stroke is the 3 cause of death in several industrial countries; Embolism accounts for 15-30%
Maternal Cardiac Disease Diagnosis and Management
 Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Maternal Cardiac Disease Diagnosis and Management Dr. Şevki ÇELEN ZTB Maternity and Teaching Hospital Department of Perinatology Heart diseases in pregnancy Today, 0.2-4% of all pregnancies are accompanied
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy
 Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Using an anti-xa level nomogram to adjust intravenous unfractionated heparin infusion for arrhythmia in pregnancy W. Sia, E. Toor, N. Wahab, J. Windram, R. Khurana Cardiac Problems in Pregnancy Congress
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
Images in Cardiovascular Medicine
 Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Images in Cardiovascular Medicine Management of Severe Mitral Stenosis During Pregnancy Rebecca S. Norrad, MBBS; Omid Salehian, MSc, MD, FRCPC, FACC, FAHA A 37-year-old woman originally from Iraq was referred
Anticoagulation Therapy and Valve Surgery. Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon
 Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη
 The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
The dos and don ts των νέων Κατευθυντηρίων Οδηγιών της Ευρωπαϊκής Καρδιολογικής Εταιρείας Για την καρδιαγγειακή νόσο στην εγκυμοσύνη Θωμάς Κ. Μακρής, MD FA, FES Συντονιστής Διευθυντής Καρδιολογικού Τμήματος
Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis
 Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Središnja medicinska knjižnica
 Središnja medicinska knjižnica Vincelj, J., Sokol, I., Pevec, D., Sutlić, Ž. (2007) Infective endocarditis of aortic valve during pregnancy: A case report. International Journal of Cardiology, [Epub ahead
Središnja medicinska knjižnica Vincelj, J., Sokol, I., Pevec, D., Sutlić, Ž. (2007) Infective endocarditis of aortic valve during pregnancy: A case report. International Journal of Cardiology, [Epub ahead
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Primary Care practice clinics within the Edmonton Southside Primary Care Network.
 INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
INR Monitoring and Warfarin Dose Adjustment Last Review: November 2016 Intervention(s) and/or Procedure: Registered Nurses (RNs) adjust warfarin dosage according to individual patient International Normalized
Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 19 Number 1 Maternal And Fetal Outcome In Pregnancies Complicated With Maternal Cardiac Diseases: Experience At A Tertiary Care Hospital
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Antithrombotic therapy for patients with congenital heart disease. George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki
 Antithrombotic therapy for patients with congenital heart disease George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki Disclosures Educational fees from Astra Zeneca, GSK Research fees from
Antithrombotic therapy for patients with congenital heart disease George Giannakoulas, MD, PhD AHEPA University Hospital Thessaloniki Disclosures Educational fees from Astra Zeneca, GSK Research fees from
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Clinical Practice Guideline for Anticoagulation Management
 Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Cardiovascular disease complicates 1% to 3% of all
 Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy Complicated by Valvular Heart Disease: An Update Michael Nanna, MD; Kathleen Stergiopoulos, MD, PhD, FASE, FACC, FAHA Cardiovascular disease complicates 1% to 3% of all pregnancies and is responsible
Pregnancy in Non-Peripartum Cardiomyopathy
 Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
Pregnancy in Non-Peripartum Cardiomyopathy Avraham Shotan, Lubov Vasilenco, Michael Shochat, Mark Kazatsker, David Blondheim, Yaniv Levi, Simcha Meisel, Alicia Vazan Heart Institute, Hillel Yaffe Medical
Peripartum Cardiomyopathy. Lavanya Rai Manipal
 Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Peripartum Cardiomyopathy Lavanya Rai Manipal Definition - PPCM - Dilated cardiomyopathy of unknown cause resulting in cardiac failure that occurs in the peripartum period in women without any preexisting
Congenital Heart Disease Patient and Pregnancy
 Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Congenital Heart Disease Patient and Pregnancy Gurur Biliciler-Denktas, M.D. Assistant Professor Division of Pediatric Cardiology, Department of Pediatrics The University of Texas Health Science Center
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
2.5 Other Hematology Consult:
 The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE?
 PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE? DR TARAKESWARI S DR SUBHASHINI Y Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary
PRIMARY PULMONARY ARTERIAL HYPERTENSION AND PREGNANCY HOW PREPARED ARE WE? DR TARAKESWARI S DR SUBHASHINI Y Pulmonary hypertension (PH) is an increase of blood pressure in the pulmonary artery, pulmonary
Transcatheter closure of right coronary artery fistula to the right ventricle
 Case Report Transcatheter closure of right coronary artery fistula to the right ventricle Abstract Coronary artery fistula (CAF) is an uncommon anomaly usually congenital but can be acquired. Although,
Case Report Transcatheter closure of right coronary artery fistula to the right ventricle Abstract Coronary artery fistula (CAF) is an uncommon anomaly usually congenital but can be acquired. Although,
Pregnancy and Cardiovascular Disease
 Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
Pregnancy and Cardiovascular Disease Cindy M. Martin, M.D. Co-Director, Adult Congenital and Cardiovascular Genetics Center No Disclosures Objectives Discuss the hemodynamic changes during pregnancy Define
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Safety of Expedited Anticoagulation in Patients Undergoing Transesophageal Echocardiographic-guided Cardioversion
 The American Journal of Medicine (2006) 119, 142-146 CLINICAL RESEARCH STUDY Safety of Expedited Anticoagulation in Patients Undergoing Transesophageal Echocardiographic-guided Cardioversion Lambert A.
The American Journal of Medicine (2006) 119, 142-146 CLINICAL RESEARCH STUDY Safety of Expedited Anticoagulation in Patients Undergoing Transesophageal Echocardiographic-guided Cardioversion Lambert A.
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome
 Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Non-cardiac Surgery in Valvular Heart Disease
 Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Jafar Golshahi, MD; Shahnaz Aram, MD Abstract Background- Valvular heart disease is one of the common complications of acute rheumatic fever, which manifests its clinical complications one or two decades
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Management of Valvular Heart Disease. Management of Valvular Heart Disease
 Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
I (312) Mitral Regurgitation What Should You Know?
 Mitral Regurgitation What Should You Know?") Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
Mitral Regurgitation What Should You Know? Table of Contents What is Mitral Regurgitation? 3 What are the Symptoms? 4 What are the risks? 5 Who Gets Mitral Regurgitation? 6 Diagnosing Mitral Regurgitation
Anticoagulant Therapy During Pregnancy
 Anticoagulant Therapy During Pregnancy AIM - June 2007 Russell K. Laros, Jr., MD Thromboembolism and Pregnancy Leading Non-Obstetrical Cause of Maternal Mortality Early recognition and proper treatment
Anticoagulant Therapy During Pregnancy AIM - June 2007 Russell K. Laros, Jr., MD Thromboembolism and Pregnancy Leading Non-Obstetrical Cause of Maternal Mortality Early recognition and proper treatment
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy
 Curriculum in Cardiology Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy Syed M. Jafri, MD, FACC Detroit, Mich Patients receiving chronic anticoagulation therapy
Curriculum in Cardiology Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy Syed M. Jafri, MD, FACC Detroit, Mich Patients receiving chronic anticoagulation therapy
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Case Report. Ilias K Karabinos, MD, FESC, 1 Athanasios Kranidis, MD, FESC, 2 Vassilios N Spanos, MD 1
 HOSPITAL CHRONICLES 2010, 5(1): 1 5 Case Report Acute Myocardial Infarction Presumably Embolic, in a Patient With a Mechanical Aortic Valve: a Rare Cause of Non-Atherosclerotic Coronary Artery Occlusion
HOSPITAL CHRONICLES 2010, 5(1): 1 5 Case Report Acute Myocardial Infarction Presumably Embolic, in a Patient With a Mechanical Aortic Valve: a Rare Cause of Non-Atherosclerotic Coronary Artery Occlusion
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
PERIPARTUM CARDIOMYOPATHY
 PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
PERIPARTUM CARDIOMYOPATHY Dr.T.Venkatachalam. Professor of Anaesthesiology Madras Medical College, Chennai Peripartum cardiomyopathy is defined as the onset of acute heart failure without demonstrable
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It. Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN
 The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN Disclosures Consultant Advisory Board, Medtronic Atrial fibrillation
The Emerging Atrial Fibrillation Epidemic: Treat It, Leave It or Burn It Chandra Kumbar MD FACC FHRS The Heart Group, Evansville IN Disclosures Consultant Advisory Board, Medtronic Atrial fibrillation
Disclosures. Overview. Have you ever. The Perioperative Management of Anticoagulants. No financial conflicts of interest to disclose
 Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
What to do when a heart failure patient becomes pregnant
 BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
BSH Heart Failure Day for Revalidation and Training 2017 What to do when a heart failure patient becomes pregnant Dr Diane Barker Consultant Cardiologist Royal Stoke Hospital Conflicts of interest - sponsorship,
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD
 Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Long-term results (22 years) of the Ross Operation a single institutional experience
 of the Ross Operation a single institutional experience") Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Long-term results (22 years) of the Ross Operation a single institutional experience Authors: Costa FDA, Schnorr GM, Veloso M,Calixto A, Colatusso D, Balbi EM, Torres R, Ferreira ADA, Colatusso C Department
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation
 Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation Marissa L. Kauss, M.D. Fellow, Cardiovascular Anesthesia Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Peripartum Anesthetic Management in Patients with Left Ventricular Hypertrabeculation Marissa L. Kauss, M.D. Fellow, Cardiovascular Anesthesia Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiac Disease in Pregnancy
 Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
Cardiac Disease in Pregnancy DATE: SEPTEMBER 11, 2016 PRESENTED BY: ABIGAIL KHAN, MD Outline Scope of the problem Physiology of pregnancy Cardiac risk in pregnancy Pregnancy management Contraception 1
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
(For items 1-12, each question specifies mark one or mark all that apply.)
") Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Management of Patients With Valvular Heart Disease. ACC/AHA Pocket Guidelines
 ACC/AHA Pocket Guidelines Management of Patients With Valvular Heart Disease A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines July 2000 ACC/AHA
ACC/AHA Pocket Guidelines Management of Patients With Valvular Heart Disease A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines July 2000 ACC/AHA
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Pregnancy and Heart Disease
 Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Pregnancy and Heart Disease Heidi M. Connolly, MD No disclosures 2011 MFMER 3138928-1 Regitz-Zagrosek V, Lundqvist C, Borghi C, et al. Pregnancy and the Heart 2% of pregnancies involve maternal CV disease
Should We Reconsider using Anticoagulation for Biological Tissue Valves
 Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Rotation: Echocardiography: Transthoracic Echocardiography (TTE)
") Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
In Whom and When Should Atrial Fibrillation Ablation be Considered?
 In Whom and When Should Atrial Fibrillation Ablation be Considered? Christian de Chillou, MD, PhD Department of Cardiology University Hospital Nancy, France ESC 2010 Stockholm, August 30. 2010 2 In Whom?
In Whom and When Should Atrial Fibrillation Ablation be Considered? Christian de Chillou, MD, PhD Department of Cardiology University Hospital Nancy, France ESC 2010 Stockholm, August 30. 2010 2 In Whom?
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı
 ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC
 Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Ventricular tachyarrhythmia during pregnancy in women with heart disease: data from the ROPAC Ebru Ertekin MD, Iris M. Van Hagen MD, Amar M. Salam MD, Titia P.E. Ruys MD PhD, Jolien W. Roos-Hesselink MD
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation
 Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Heart Failure treatment during pregnancy
 Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Heart Failure treatment during pregnancy Angeles Alonso García Hospital Universitario Puerta de Hierro. Majadahonda. Madrid. Spain European Society of Cardiology. Stockholm. 29 August 2010 Starting Point
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question.
 Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
The Pendulum of Bridging Periprocedural Anticoagulant Therapy. Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA
 The Pendulum of Bridging Periprocedural Anticoagulant Therapy Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA Disclosures Department of Veterans Affairs Industry Relationships:
The Pendulum of Bridging Periprocedural Anticoagulant Therapy Alan K. Jacobson, MD Cardiology Section Loma Linda VA Medical Center Loma Linda, CA Disclosures Department of Veterans Affairs Industry Relationships:
CASE IN... Anticoagulation: When to Start,When to Stop. The management of patients who require an. Meet Tracey. Anticoagulation
 Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Doppler-echocardiographic findings in a patient with persisting right ventricular sinusoids
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
WARFARIN: PERI-OPERATIVE MANAGEMENT
 WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
MitraClip World Wide Commercial Experience
 MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral
MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral