Surgery in Inflammatory Bowel Disease. Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh
|
|
|
- Barrie Sherman
- 5 years ago
- Views:
Transcription

1 Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1
2 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized by chronic inflammatory condition that affects the rectum and extends proximally into the colon for varying distances Many patients are treated effectively by a wide variety of medications Approx % of patients require or elect operative intervention 2
3 Surgical Options in UC Complete removal of all potential disease bearing tissue theoretically curative Operative options Emergency: Total or subtotal abdominal colectomy with end ileostomy Elective : Total proctocolectomy with ileostomy Total proctocolectomy with IPAA All these procedures may be performed by using open or MIS techniques 3
4 Ulcerative Colitis Indications for Surgery Intractability : Failure to respond to medical therapy the most common indication Inability to control symptoms Poor quality of life Risks/Side effects of chronic medical therapy (especially long term corticosteroids) Noncompliance Growth failure Patients may opt for surgery in the elective or semi elective setting 4
5 Ulcerative Colitis Indications for Surgery contd Acute Colitis Clinical e/o actual or impending perforation Grade of Recommendation: 1B Surgery required in 20 30% of pts with toxic colitis, & typically consists of a subtotal colectomy with end ileostomy. 5

6 6
7 7

8 8
9 Acute Colitis contd Perforation in patients with Toxic Colitis a.w. high mortality 27 57%, regardless of whether the perforation is contained or free Mortality rate also increases as the time interval between perforation and surgery increases Pertinent to identify signs of impending perforation 9
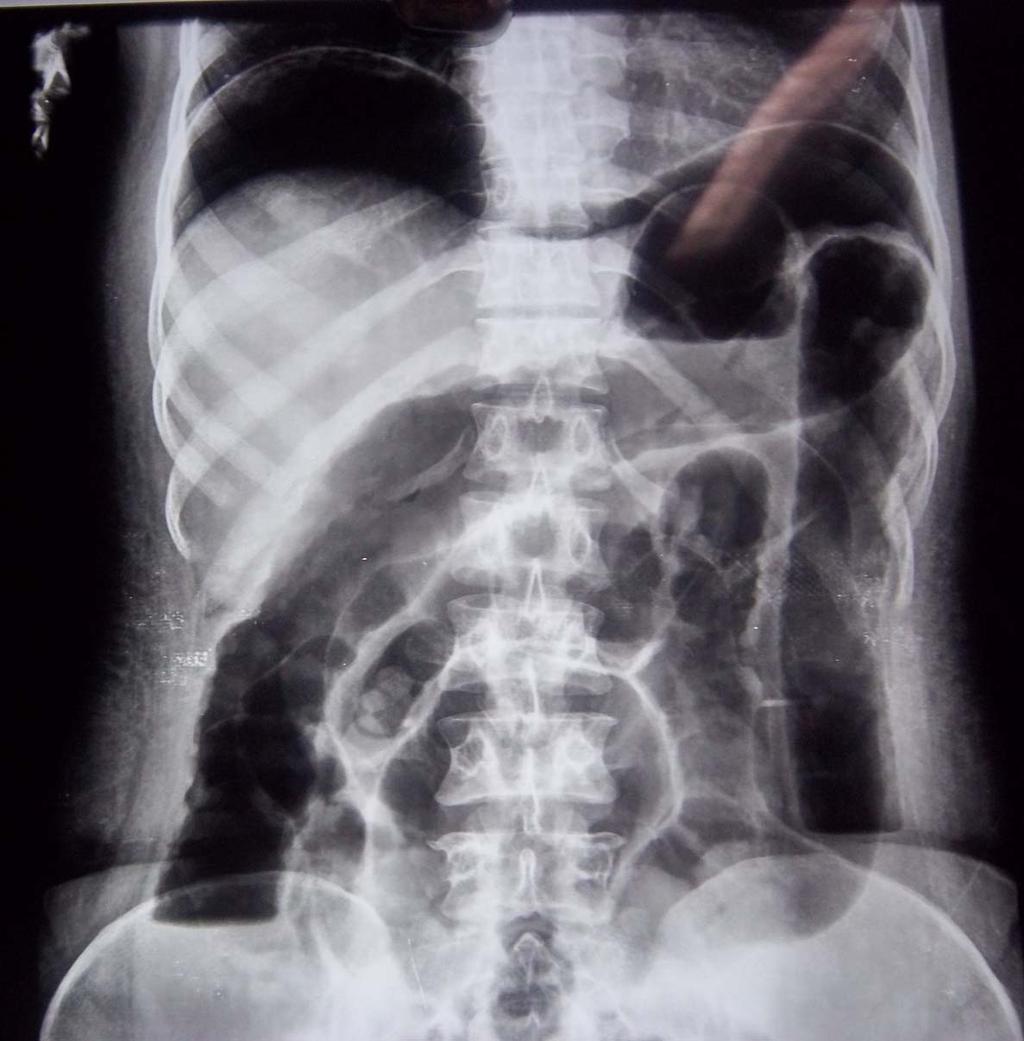
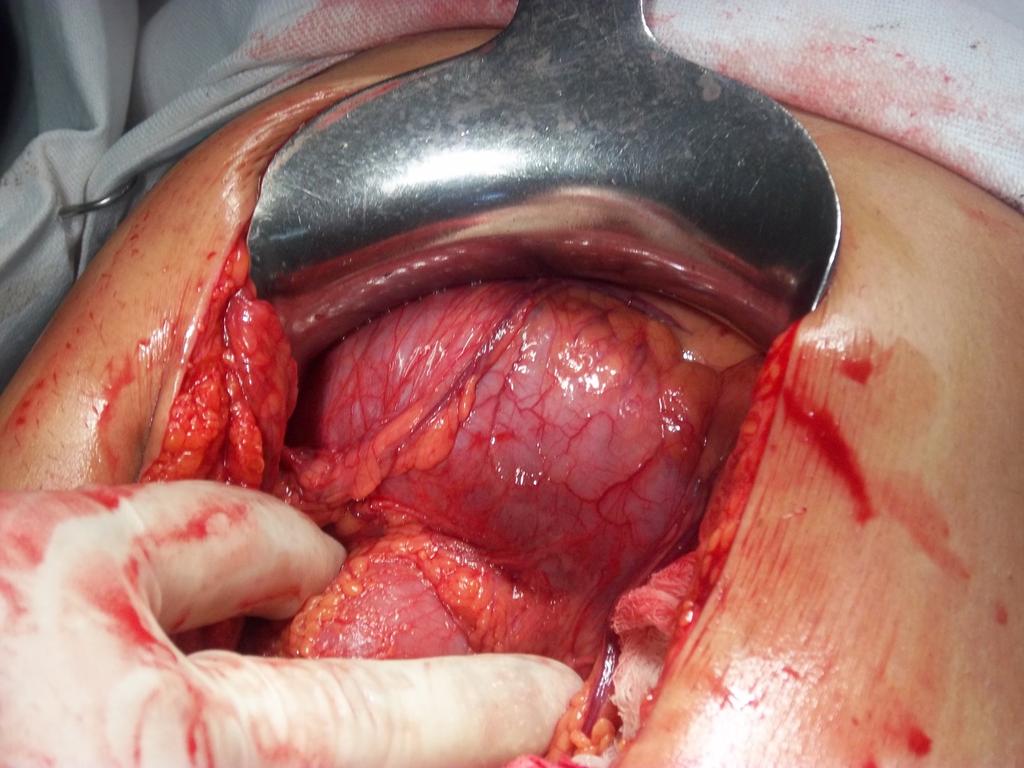
10 Cecal Perforation 10
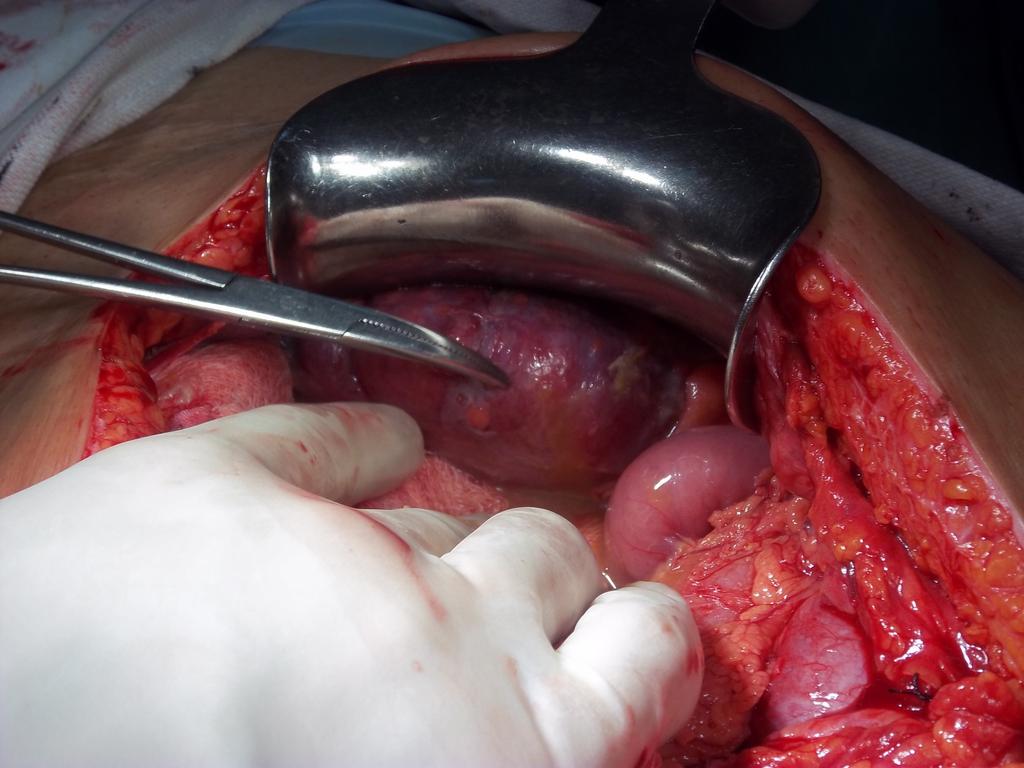
11 Cecal Perforation 11
12 Acute Colitis contd Signs of impending perforation Persistent or increasing colonic dilation Pneumatosis coli Worsening local peritonitis Development of MOF Signs may be masked by ongoing medical therapy 12
13 Acute Colitis contd Moderate to severe colitis Early surgical consultation should be obtained Grade of Recommendation: 1C Indications for surgical consultation in patients with a lesser degree of disease include Failure of primary therapy i.e., Pts. worsen on medical therapy or who do not make significant improvement after hrs Pts. being considered for 2 nd line Monoclonal antibody (Infliximab, Adalimumab) or cyclosporine therapy 13
14 Acute Colitis contd Moderate to severe colitis Timing of surgery Patients with more than 8 stools per day 3 to 8 stools and a CRP > 45 mg/ml after 3 days of therapy 85% chance of requiring colectomy during same hospitalization Patients with contraindication to (or do not desire) MAb or cyclosporine therapy, or when steroids fail Persistent colonic distention Toxic Megacolon 14
15 Acute Colitis contd Moderate to severe colitis Important tips: Decision regarding response to 2 nd line or rescue therapy be made within 5 to 7 days after initiation Mortality rates increase as operative timing progresses from within 3 6 days (OR 2.12) & 11 days (OR 2.89) Longer waiting times results in Worsening physiological reserve Further depletion in nutrition stores Inappropriate delay in surgery with no apparent gain 15
16 UC Indications of Surgery Disabling Extra intestinal Manifestations Typically Episcleritis Erythema nodosum Aphthous ulcerations Large joint arthropathy These are more likely to be responsive to colectomy Hepatic, vascular, hematologic, cardiopulmonary, & neurological comorbidities Not responsive Growth failure in children another form of intractability may require colectomy 16
17 Ulcerative Colitis Indications for Surgery contd Risk of Malignancy Risk factors: Extent of colonic disease Pancolitis (proximal to the splenic flexure) Greater than left sided colitis Prolonged disease duration (>8 years with pancolitis) Diagnosis of UC at a younger age a.w. increased risk of colorectal cancer Additional risk factors include Family history of IBD Concomitant primary sclerosing cholangitis 17
18 Ulcerative Colitis Indications for Surgery contd Risk of Malignancy Patients with low grade dysplasia Total proctocolectomy, or surveillance endoscopy Grade of Recommendation: 1C Non adenoma like dysplasia associated lesion or mass High grade dysplasia Patients with carcinoma Total proctocolectomy, with or without IPAA Grade of Recommendation: 1B 18

19 Cut section: smooth tubularized left colon with loss of mucosal fold 19

20 Cut section tumor at lower end in ulcerative colitis 20
21 Ulcerative Colitis Indications for Surgery contd Colonic stricture : Develop in 5% to 10% with UC Especially with long standing disease Grade of Recommendation: 1B 25% of strictures malignant Most common manifestations of CRC in chronic UC Biopsy may reveal dysplasia or malignancy a negative biopsy not reliable: risk of sampling error and more infiltrative nature of colitis associated malignancies In general all patients with strictures should undergo an oncological resection 21
22 Surgery in UC Emergency Procedure Procedure of choice: Total or subtotal abdominal colectomy with end ileostomy Surgical goals in the acute setting To remove the bulk of the diseased bowel Restore patient health with the greatest reliability and least risk Preserve reconstructive options after the patient has recovered and medications are withdrawn Subtotal colectomy with end ileostomy and Hartmann closure of the distal bowel or creation of a mucous fistula a safe and effective approach Completion proctectomy and IPAA can be performed later to remove the remaining disease & restore intestinal continuity 22
23 Surgery in UC Elective Procedure 1. Total proctocolectomy with ileostomy considered a benchmark with which all other operations compared Suitable for those at significant risk for pouch failure Patients with impaired anal sphincter muscles Previous anoperineal disease Limited physiological reserve secondary to comorbid conditions 2. Total proctocolectomy with IPAA an appropriate op. for selected pt. Most commonly performed elective surgery A.w. acceptable morbidity rate (19 27 %) extremely low mortality rate ( %) QOL approaches that of the healthy population Patient selection Baseline continence Ability to undergo major pelvic surgery and its complications Medical comorbidities 23

24 Proctocolectomy specimen 24

25 Cut Section Proctocolectomy Specimen 25

26 Pseudopolyps 26

27 27

28 28
29 Surgery in UC Post op Complications Risks arising from the pelvic dissection Infertility Sexual dysfunction Pouch specific complications Pouchitis Medical Rx to salvage pouch Antibiotics Immunomodulators Biologics Surgery Successful in more than 50% of cases Anastomotic leak Pelvic sepsis Fistula Stricture Cuff inflammation 29
30 Crohn s Disease Anywhere in GIT between the mouth and anus 50% have ileocolic disease 30% have ileal disease only 20% have colonic disease only 26.5% have perianal disease Felt to be a marker of more aggressive disease Vienna classification most commonly used (2000) Penetrating (fistulizing) Stricturing Nonpenetrating, nonstricturing disease 30
31 Crohn s Disease Indications of Surgery Tends to recur & cannot be cured Surgery is reserved for patients with Symptomatic disease refractory to medical management Or in those with complications : Retardation of growth in children Hemorrhage Perforation Abscess Fistula Stricture or Malignancy 31
32 Anorectal Crohn s Disease Large perianal skin tags with fissure Recurrent perirectal abscesses Complicated fistula in ano Strictures A careful anorectal examination (under anesthesia if necessary), including anoscopy and flexible sigmoidoscopy critical for diagnosis 32
33 CROHN S DISEASE Anal Fissure Typical anterior or posterior midline anal fissure Can be treated with standard medical treatments: Glyceryl trinitrate, Calcium channel blockers & Botulinum toxin Surgical Rx In absence of proctitis lateral internal anal sphincterotomy gives good results I.p.o. Proctitis Sphincterotomy be avoided 33
34 Abscess/Fistula in Ano/Rectovaginal Fistula EUA and drainage of abscesses in a timely fashion Incision as close to the anal verge as possible to minimize the risk of a long fistula tract Simple fistulas involving minimal muscle Fistulotomy with marsupialization of wound edges in patients with otherwise normal continence Repeat fistulotomy avoided : Risk of fecal incontinence Fistula in ano may have Internal opening above dentate line, Multiple internal openings, And/Or may involve a large amount (>50%) of the ext. anal sphincter Pelvic MRI or endorectal US with H 2 O 2 injected into the fistula tract can elucidate the anatomy of more complex fistulae 34
35 CROHN S DISEASE Fistula in Ano in CD Setons placed to control every internal opening Flexible sigmoidoscopy done to rule out proctitis Weak evidence anal fistula plug or the ligation of the intersphincteric fistula tract I.p.o proctitis Leave setons and continue with aggressive medical therapy to control rectal dis. Severe perianal disease refractory to setons Temporary or permanent fecal diversion (ileostomy vs colostomy) 35
36 CROHN S DISEASE Anorectal Stricture Can be extremely symptomatic Factors dictating therapy Presence or absence of Proctitis Exact location of stricture Anal stricture without anorectal inflamm. Dilated gently Anorectal strictures with severe proctitis refractory to medical Rx Proctectomy and end colostomy Rectal stricture without proctitis Initial attempt at dilation If it fails LAR & colo anal anastomosis 36
37 CROHN S DISEASE INTESTINAL FISTULA Patients often require multiple surgeries Function must be considered when deciding on the extent and aggressiveness of procedure 40 50% of patients require surgery < 10 years of diagnosis 16%, 28%, and 35% of patients require a second surgery at 5, 10, and 15 years after the first surgery respectively 37
38 CROHN S DISEASE INTESTINAL FISTULA Guiding Principles for surgery: 1.Nutrition should be optimized preop. if possible 2.Preop. esophagogastroduodenoscopy & colonoscopy are helpful. 3.CT enterography identifies both luminal & extraluminal intestinal dis. 4.Laparoscopy reasonable approach for complicated dis. 5.Only diseased bowel resected 6.Non diseased target of the fistula repaired safely 38
39 CROHN S DISEASE INTESTINAL FISTULA Guiding Principles for surgery (Contd.): 7. RM should be small (2 cm) & within grossly normal bowel 8. Increase the risk of anastomotic leak Steroid use (>10 mg of prednisone/day x 4 wks before surgery) Preop. abscess Although use of anti TNF biologics before surgery does not appear to increase the risk of a leak But still controversial with data supporting each side 39
40 CROHN S DISEASE Enteroenteric or Enterocolic Fistula Asymptomatic enteroenteric fistula should be left alone Large acute abscesses should be drained percutaneously if possible If fistula a.w. diarrhea Diseased bowel should be resected 40
41 CD Enterocutaneous Fistula Management Acute sepsis Treated with aggressive fluid resuscitation, iv antibiotics & drainage of large intra abdo. abscesses Skin opening should be pouched. Nutrition should be optimized Fistulogram or CT enterography helpful to delineate fistula anatomy Diseased bowel and fistula tract be resected 41

42 Diseased bowel with creeping fat and thickened mesentry 42
43 Surgery for bowel strictures Operative indications for stricturing dis. Persistent or recurrent obst. in the face of adequate medical management Significant weight loss Inability to tolerate a solid diet Inability to tolerate medication Inability to wean from steroids 43
44 Role of Preoperative TPN Severe malnutrition Moderate to severe Crohn s disease can improve their nutritional status and have significantly fewer postop. complications and mortality if treated for several weeks with hyperalimentation 44
45 CD Relevant Points in Patient s Course of Illness Reoperation rates for Crohn s disease approach 50% over the long term Smoking confers a 2.5 fold increased risk of postop. recurrence requiring surgery, and pts should be counseled extensivelyon smoking cessation techniques Every patient undergoing surgery should understand that there is some lifelong risk of intestinal failure and that bowel conservation is the goal Bowel sparing should be the guiding principle Pts. with IBD have a > 3 fold risk of VTE events in the postop. period 45
46 Carry Home Messsage UC Approx % of patients of UC require or elect operative intervention Intractability : the most common indication Complete removal of all potential disease bearing tissue theoretically curative Surgery required in 20 30% of pts with toxic colitis High mortality 27 57% in perforation with toxic colitis Imperative to know signs of impending perforation Some disabling extra intestinal manifestations may respond to surgery Risk of Malignancy a.w. extent of colonic disease, prolonged disease duration (>8 years with pancolitis) and diagnosis at younger age 46
47 Carry Home Messsage CD 26.5% have perianal disease a marker of more aggressive disease Tends to recur & cannot be cured Surgical Rx of anorectal disease depends on presence or absence of proctitis Patients often require multiple surgeries Function must be considered when deciding on the extent and aggressiveness of procedure 40 50% of patients require surgery < 10 years of diagnosis 47
48 Thank you 48
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma?
 17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
17 th Panhellenic IBD Congress Thessaloniki May 2018 Surgical Approach to Crohn s Colitis Segmental or Total Colectomy? Can We Avoid the Stoma? Janindra Warusavitarne Consultant Colorectal Surgeon, St
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Index. Surg Clin N Am 87 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Surgical Therapies for the Treatment of IBD!
 Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgical Therapies for the Treatment of IBD! Andrew A Shelton, MD Clinical Professor of Surgery Stanford Hospital and Clinics Section of Colon and Rectal Surgery! Ulcerative Colitis v. Crohn s! 30% of
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
Inflammatory Bowel Disease RTC 10/30/09
 Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
Surgical Treatment of Inflammatory Bowel Disease (IBD)
") Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Surgical Treatment of Inflammatory Bowel Disease (IBD) JMAJ 45(2): 55 62, 2002 Tetsuichiro MUTO Vice-Director, Cancer Institute Hospital Abstract: IBD, especially ulcerative colitis (UC) and Crohn s disease
Perianal Fistula of Crohn s Disease
 Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Ileo-rectal anastomosis for Crohn's disease of
 Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Ileo-rectal anastomosis for Crohn's disease of the colon W. N. W. BAKER From the Research Department, St Mark's Hospital, London Gut, 1971, 12, 427-431 SUMMARY Twenty-six cases of Crohn's disease of the
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Benign anorectal diseases
 Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Benign anorectal diseases Symptoms Bleeding Pruritus Discharge Fecal incontinence Diarrhea Constipation False need to defecate Examinations Clinical exam Anuscopy Rectosigmoidoscopy Endosonography MRI
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Epidemiology / Morbidity
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Ileoanal Pouch Solves the Problem
 Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
Ileoanal Pouch Solves the Problem Bruce D George Department of Surgery John Radcliffe Hospital, Falk Symposium 2-3 May 2008 Ileoanal Pouch Solves the Problem? Sometimes Not always Key Issues in Pouch Surgery
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
The role of Surgery and Stomas in IBD
 The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
The role of Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Laparoscopic Surgical Approaches for Ulcerative Colitis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/laparoscopic-surgicalapproaches-for-ulcerative-colitis/7261/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/laparoscopic-surgicalapproaches-for-ulcerative-colitis/7261/
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 29) A 54 year old man with colonic Crohn s disease is in remission following an 8 week course of prednisolone. Which one of the following medications is
Year 2002 Paper two: Questions supplied by Jo 1 29) A 54 year old man with colonic Crohn s disease is in remission following an 8 week course of prednisolone. Which one of the following medications is
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it?
 Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
Surgery and Stomas in IBD When do I need it? Can I avoid it? How do I live with it? Kyle G. Cologne, MD Assistant Professor of Surgery USC Division of Colorectal Surgery Topics Surgical Differences between
ULCERATIVE COLITIS. Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC
 ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula
 Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]
![Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]](/thumbs/87/96356608.jpg "Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan. [J Soc Colon Rectal Surgeon (Taiwan) 2009;20:1-6]") J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
J Soc Colon Rectal Surgeon (Taiwan) March 2009 Original Article Surgical Outcomes of Crohn s Disease: A Single Institutional Experience in Taiwan Ta-Wen Hsu 1,2 Feng-Fan Chiang 1 Hwei-Ming Wang 1 1 Division
SURGERY FOR COLITIS THE BOTTOM LINE
 SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
SURGERY FOR COLITIS THE BOTTOM LINE Speaker Declarations This presenter has the following declarations of relationship with industry None [Nov 2017] Surgeons just like to cut.. ABSOLUTE INDICATIONS Toxic
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent
 Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
Gastroenterology Research and Practice Volume 2010, Article ID 860394, 4 pages doi:10.1155/2010/860394 Case Report Successful Long-Term Use of Infliximab in Refractory Pouchitis in an Adolescent Jessica
The Road to Remission
 The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
Inflammatory Bowel Disease. Your Illness and Its Treatment
 Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
Inflammatory Bowel Disease Your Illness and Its Treatment What Is Inflammatory Bowel Disease? Inflammatory bowel disease (IBD) is inflammation (irritation and swelling) of the digestive tract. Your digestive
Acute Care Surgery: Diverticulitis
 Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS. crohnsandcolitis.ca
 THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca There are many treatments that help manage Crohn s and colitis. Crohn s and Colitis Canada urges you to become knowledgeable
THE CUTTING EDGE SURGERY FOR CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca There are many treatments that help manage Crohn s and colitis. Crohn s and Colitis Canada urges you to become knowledgeable
Case Presentations #2 Saturday November 13, Case #1 HPI 11/14/10. Uma Mahadevan-Velayos MD. Complicated Crohn s Pregnancy
 Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Research Article Temporary Fecal Diversion in the Management of Colorectal and Perianal Crohn s Disease
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
An Unusual Complication of Crohn s Disease. Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008
 An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn disease
 REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
REVIEW ARTICLE Medical and Surgical Management of Chronic Ulcerative Colitis Robert R. Cima, MD; John H. Pemberton, MD Idiopathic inflammatory bowel disease is divided into 2 major disease processes, Crohn
Understanding Learning is the first step to getting help.
 Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
World Journal of Colorectal Surgery Volume 5, Issue 1 2015 Article 1 Ileal U Pouch Reconstruction Proximal To Straight Sublevator Ileoanal Anastomosis Following Total Proctocolectomy For Low Rectal Cancer
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical therapy in Crohn s disease: Improving treatment strategies
: de Groof, E. J. (2017). Surgery and medical therapy in Crohn s disease: Improving treatment strategies") UvA-DARE (Digital Academic Repository) Surgery and medical therapy in Crohn s disease de Groof, E.J. Link to publication Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical
UvA-DARE (Digital Academic Repository) Surgery and medical therapy in Crohn s disease de Groof, E.J. Link to publication Citation for published version (APA): de Groof, E. J. (2017). Surgery and medical
Inflammatory Bowel Disease
 Inflammatory Bowel Disease Objectives: NOT FOUND. Team Members: Shrouq alsomali + Basel almeflh + Alaa alaqeel + Raneem alghamdi Team Leader: Haneen Alsubki Revised By: Maha AlGhamdi Resources: 435 team
Inflammatory Bowel Disease Objectives: NOT FOUND. Team Members: Shrouq alsomali + Basel almeflh + Alaa alaqeel + Raneem alghamdi Team Leader: Haneen Alsubki Revised By: Maha AlGhamdi Resources: 435 team
Adult organisational audit
 Adult organisational audit Health Information Coding Responses for this section require data for the period between 1/12/13-30/11/14. [Infliximab was introduced for the treatment of ulcerative colitis
Adult organisational audit Health Information Coding Responses for this section require data for the period between 1/12/13-30/11/14. [Infliximab was introduced for the treatment of ulcerative colitis
Surgical strategies in paediatric inflammatory bowel disease
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i20.6101 World J Gastroenterol 2015 May 28; 21(20): 6101-6116 ISSN 1007-9327 (print)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i20.6101 World J Gastroenterol 2015 May 28; 21(20): 6101-6116 ISSN 1007-9327 (print)
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT
 STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
STOMA SITING & PARASTOMAL HERNIA MANAGEMENT Professor Hany S. Tawfik Head of the Department of Surgery & Chairman of Colorectal Surgery Unit Benha University Disclosure No financial affiliation to disclose
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions
: Future Directions") Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
INFLAMMATORY BOWEL DISEASE
 National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
study was undertaken to assess the epidemiology, course and outcome of UC patients attending a hospital in Jordan.
 Ulcerative colitis (UC) is a relatively uncommon, chronic, recurrent inflammatory disease of the colon or rectal mucosa [1]. Often a lifelong illness, the condition can have a profound emotional and social
Ulcerative colitis (UC) is a relatively uncommon, chronic, recurrent inflammatory disease of the colon or rectal mucosa [1]. Often a lifelong illness, the condition can have a profound emotional and social
St Mark's Hospital from 1953 to 1968
 Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
Gut, 1970, 11, 235-239 The results of ileorectal anastomosis at St Mark's Hospital from 1953 to 1968 W. N. W. BAKER From St Mark's Hospital, London SUMMARY The popular view of ileorectal anastomosis for
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
A Comparitive Study of Laying Open of Wound Vs Primary Closure In Fistula in Ano
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 9 Ver. III (Sep. 214), PP 39-45 A Comparitive Study of Laying Open of Wound Vs Primary Closure
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 9 Ver. III (Sep. 214), PP 39-45 A Comparitive Study of Laying Open of Wound Vs Primary Closure
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Staying Healthy as an IBD patient
 Staying Healthy as an IBD patient Crohn s & Colitis Seattle Education Conference March 28, 2015 Karlee Ausk, MD Swedish Gastroenterology Epidemiology Affects >1.4 million Americans Economic burden $2.8
Staying Healthy as an IBD patient Crohn s & Colitis Seattle Education Conference March 28, 2015 Karlee Ausk, MD Swedish Gastroenterology Epidemiology Affects >1.4 million Americans Economic burden $2.8
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
ORIGINAL ARTICLE. Surgery for Ulcerative Colitis in Elderly Persons. Changes in Indications for Surgery and Outcome Over Time
 ORIGINAL ARTICLE Surgery for Ulcerative Colitis in Elderly Persons Changes in Indications for Surgery and Outcome Over Time Gidon Almogy, MD; David B. Sachar, MD; Carol A. Bodian, DrPH; Adrian J. Greenstein,
ORIGINAL ARTICLE Surgery for Ulcerative Colitis in Elderly Persons Changes in Indications for Surgery and Outcome Over Time Gidon Almogy, MD; David B. Sachar, MD; Carol A. Bodian, DrPH; Adrian J. Greenstein,
Treating Crohn s and Colitis in the ASC
 Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?