Jeffrey A. Hertz, MD FACS Nursing & Cath Lab Symposium August 26, 2011
|
|
|
- Eugene Merritt
- 5 years ago
- Views:
Transcription


1 Jeffrey A. Hertz, MD FACS Nursing & Cath Lab Symposium August 26, 2011
2 Definition History Epidemiology Pathophysiology Signs and Symptoms Evaluation Management Complications Outcomes

3 Aneurysm Focal dilatation of an artery at least 50% greater than its normal diameter Abdominal aortic aneurysms typically are at least 3 cm in size
4 First described in 16 th century by Vesalius Initial attempts at repair were ligation, first successfully done by Matas in Rea wrapped aneurysm in cellophane 1949 Nissen treated Einstein with wrapping of aneurysm Einstein died 6 years later of ruptured AAA
5 1951 Resection and graft replacement Dubost and coworkers first reported it Shaffer and Hardin actually did it first Current open repair with endoaneurysmorrhaphy and graft placement popularized by Creech, DeBakey, and their colleagues 1991 Endovascular stent grafting successfully performed by Parodi
6 Generally affect elderly white men Increase in frequency after age 50 Five times more common in men 3.5 times more common in white men Usually begin developing in men at age 50 and in women about age 60 AAA 3 cm prevalence of 3-10% 15-25% of patients undergoing AAA repair have 1 st degree relative with AAA May be present in up to 85% of patients with femoral aneurysms and up to 62% in patients with popliteal aneurysms
7 Risk Factor Odds Ratio Smoking history 5.6 Family history of AAA 2.0 Older age (per 7-year interval) 1.7 Coronary artery disease 1.6 Hypercholesterolemia 1.5 COPD 1.3 Height (per 7-cm interval) 1.2 From Lederle, et al. Prevalence and associations of abdominal aortic aneurysm detected through screening: Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med 126(6): 441, 1997.
8 Symptom AAA Development AAA Expansion AAA Rupture Risk Factors Tobacco use Hypercholesterolemia Hypertension Male gender Family history (male predominance) Advanced age Severe cardiac disease Previous stroke Tobacco use Cardiac or renal transplant Female gender Decreased FEV1 Larger initial AAA diameter Higher mean blood pressure Current tobacco use (length of time smoking >> amount) Cardiac or renal transplant Critical wall stress wall strength relationship
9 Degenerative process Often attributed to atherosclerosis Significant decrease in elastin content in aortic wall at infrarenal level Elastin not synthesized in adult aorta Half-life of years, accounts for reduction with age Other potential causes include hemodynamic, structural, autoimmune factors
10 Increased expression and activity of matrix metalloproteinases (MMPs) in wall of aortic aneurysms Infectious organisms found in aneurysm wall, specifically Chlamydia pneumoniae *No isolated factor yet identified as single cause of degenerative AAA
11 Other less frequent causes Infection Cystic medial necrosis Arteritis Trauma Inherited connective tissue disorders Pseudoaneurysms from anastamotic disruption
12 Usually asymptomatic Pulsatile mass on physical exam Incidental finding on imaging Back or abdominal pain* If tenderness is elicited with palpation of aneurysm, suggests symptomatic aneurysm Acute thrombosis with ischemic legs* Possible associated paraplegia from spinal cord ischemia Ischemic toes with embolism* Rupture More than half of ruptures die prior to hospitalization Of those that reach OR, mortality with open repair is ~50% Require *urgent or emergent repair

13 Thin patient with large pulsatile mass

14 Patient without knowledge of aneurysm Presented to ER with back and abdominal pain Tender over aneurysm Suggestive of symptomatic aneurysm


15 Plug in left internal iliac artery Underwent urgent endovascular repair within 24 hours Required exclusion of left hypogastric artery
 to toes and feet Livedo")
16 Aneurysm with distal emboli Trash foot Cholesterol emboli (atheroemboli) to toes and feet Livedo reticularis

17 Presented to ER with back pain and hypotension Ruptured aneurysm until proven otherwise CT Scan confirmed suspicion
18 Physical exam Pulsatile mass Size Tenderness Back or abdomen Always check peripheral pulses Ultrasound CT Scan MRA Least used imaging modality for AAA
19 Pulsatile mass Focused exam detects about 50% of AAA cm in diameter Positive predictive value of physical exam for identifying AAA larger than 3.5 cm only 15% Chervu* 38% of 243 patients undergoing elective AAA repair were initially detected by physical exam 62% detected by incidental radiologic studies 43% of these were palpable on subsequent exam 23% of all clinically significant AAA not palpable even when diagnosis was known 2/3 of AAA in obese patients not palpable *Chervu, A, et al. Role of physical examination in detection of abdominal aortic aneurysms. Surgery 117:454,1995.
20 Ultrasound Sensitivity and specificity approach 100% Aorta cannot be visualized in 1-3% of patients due to bowel gas or obesity Ideal for screening, but can be imprecise in measuring aneurysm size Technologist dependent Aneurysm growth rate of > 0.7 cm per 6 months or 1 cm per year suggested as threshold for proceeding to surgery
21 CT Scan Primary imaging modality for surgical planning IV contrast is preferred to better delineate anatomy CT-Angiography Best imaging modality to plan procedure Stent graft protocol Specific imaging protocol to plan endovascular repair Slice thickness and contrast dose/timing considerations Can also image legs simultaneously if lower extremity occlusive disease is concern on physical exam

22
23 Aneurysm Screening Recommendations One time ultrasound for: All men older than 65 Men 55 years old with family history Women 65 or older who have smoked or have family history
24 Aneurysm Surveillance Imaging at 12-month intervals for 3.5 to 4.4 cm Imaging at 6-month intervals for 4.5 to 5.4 cm 3-year intervals for cm and 5-year intervals for cm Recommendations for repair Elective repair if 5.5 cm, in absence of significant co-morbidities Elective repair if saccular aneurysm Urgent repair if symptomatic Emergent repair if ruptured
25 Open versus endovascular repair Open repair is traditional approach Endovascular repair now commonplace Accounts for over 50% of all AAA repairs Has supplanted open repair as procedure of choice in most cases Newer technology and refinements in devices Better understanding of hemodynamic and biomechanical factors affecting use and durability Will be applied to more complex anatomies Branched and fenestrated endografts for visceral and iliac involvement


26 OPEN REPAIR ENDOVASCULAR REPAIR


27 83 year old man with large asymptomatic aneurysm


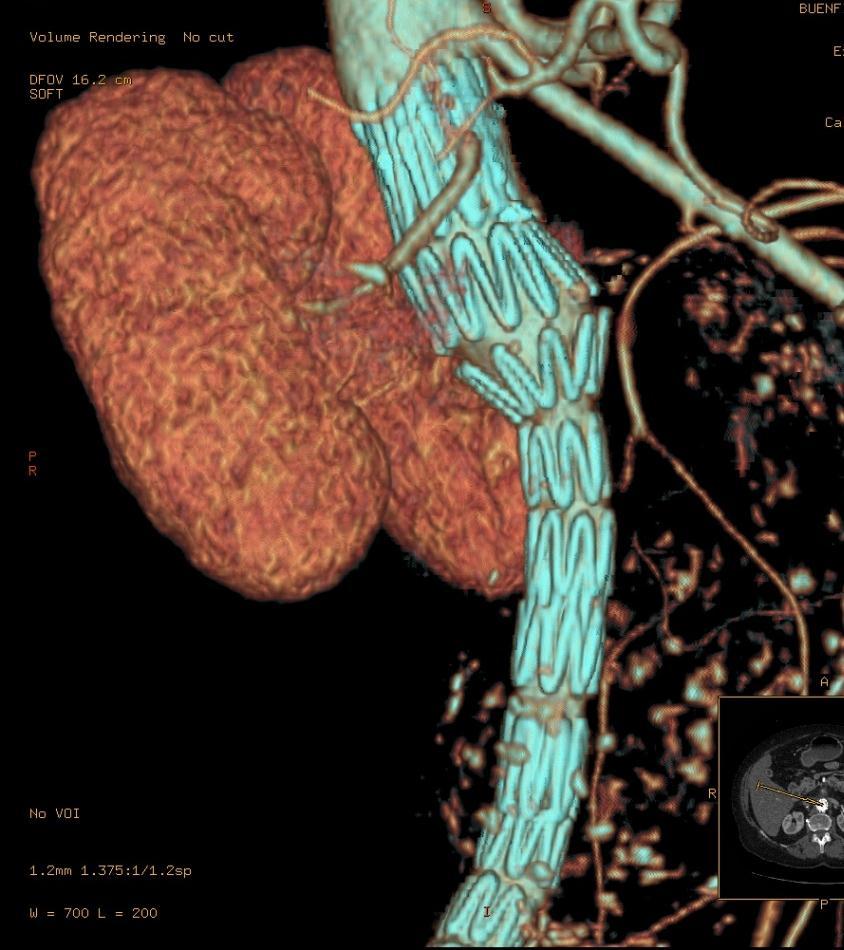
28 Endovascular repair performed Successful aneurysm exclusion
29 Factors favoring open repair Younger patient Hostile proximal infrarenal aorta Renal artery or visceral involvement Juxtarenal or thoracoabdominal aneurysm Extensive iliac occlusive disease Factors favoring endovascular repair Medical co-morbidities Hostile abdomen Less surgical stress and easier recovery
30 67 year old hypertensive male Colon resection for carcinoma one year ago Known AAA with suprarenal and infrarenal component Underwent ultrasound a few days prior to presentation with apparently stable aneurysm
31 Presented to emergency room with new onset back pain Normotensive Underwent CT scan
32 Supraceliac aorta normal
33 Suprarenal involvement
34 Aneurysmal at level of renal arteries



35 Ruptured at infrarenal level
36 Patient was taken to OR for emergent repair Not candidate for endovascular approach Retroperitoneal approach with exposure of distal thoracic aorta for proximal control Beveled repair of visceral/infrarenal aorta with bifurcated graft to common iliac arteries Unable to obtain pulses in left leg after closure, prior to leaving OR Performed right to left femoral-femoral bypass, with return of pulses
37 Prolonged ICU course with difficulty weaning from ventilator Failed extubation on multiple attempts Required tracheostomy and then rapidly improved Also developed wound hematoma, requiring wound care and VAC device placement Transferred to rehab unit soon after and then discharged home
38 Patient readmitted about one month later with bowel obstruction (from previous colon resection) CT scan obtained
39
40 Aneurysm improved at level of SMA without mural thrombus

41 Good flow within graft below renal arteries
42 Left limb of bifurcated graft occluded

43 Right common iliac artery patent
44 Patent femoral-femoral bypass supplying left leg

45 67 year old woman presented to ER with 8-12 hour history of back and abdominal pain Mild hypotension Extensive smoking history On exam, tender abdomen, normal right leg pulses, absent left leg pulses CT scan performed in ER

46 CT scan showed ruptured AAA and left external iliac artery occlusion Based on these findings, taken to OR for endovascular repair Large retroperitoneal hematoma

47 Underwent aorto-uniiliac graft placement, exclusion of left common iliac artery and femoralfemoral bypass Successful exclusion of aneurysm Required left brachial thrombectomy on postoperative day one Discharged home on postoperative day 4

48
49 Perioperative considerations in open repair Cardiac Disease Coronary revascularization if: Acute STEMI, unstable angina, stable angina with left main or 3-vessel disease Stable angina with 2-vessel disease that includes LAD and either ischemia on noninvasive testing or EF < 0.5 Preferable to wait 4-6 weeks after bare metal stent or CABG or 12 months after DES Continue β-blockers if used for angina, arrhythmias, or hypertension
50 Pulmonary Disease Smoking cessation is recommended for at least two weeks prior to aneurysm repair Bronchodilators recommended for at least two weeks prior to repair for symptomatic COPD or abnormal PFTs Renal Impairment Hold ACE-inhibitors and ARBs the morning of surgery and restart when patient is euvolemic Preoperative hydration Intraoperative diuresis with furosemide or mannitol probably does not reduce risk of postoperative renal insufficiency
51 Diabetes Maintain blood glucose below 180 mg/dl Hematologic disorders Should transfuse if preoperative hematocrit less than 28% Decreases risk of postoperative MI Further assessment is recommended if preoperative platelet count less than 130,000/μL


52 Mobilization of aneurysm Open repair requires full laparotomy Tube graft replacement
53 Anesthetic General anesthesia for open repair Select cases can be done with epidural agents Retroperitoneal approach or mini-laparotomy General or locoregional anesthesia for endovascular repair Antibiotics First generation cephalosporin, or if allergic, vancomycin within 30 minutes of skin incision Should be discontinued within 24 hours
54 Intraoperative blood conservation Cell saver recommended for all cases Transfusion recommended for hematocrit < 30% in presence of ongoing blood loss If intraoperative hematocrit < 30% and blood loss is ongoing, use of FFP and platelets in a ratio of 1:1:1 should be considered
55 Intra- and postoperative cardiovascular monitoring PA catheters should not be routinely used Central venous catheters should be routinely used ST segment monitoring in all cases of open repair and select cases of endovascular repair Monitor troponins postoperatively in cases of EKG changes or chest pain after repair
56 Body temperature Core body temperature should be maintained at or above 36⁰C throughout repair ICU Care Most open repair patients should be monitored in ICU following open repair Select patients should be monitored in ICU after endovascular repair
57 Nasogastric decompression Intraoperative use in all patients undergoing open repair and in select (most) patients postoperatively Nutrition Elective repair should not be performed unless nutritional status is optimized Parenteral nutrition recommended in patients unable to tolerate enteral support seven days after open or endovascular repair
58 Postoperative pain management Epidural anesthetic or IV PCA for open repair Oral or IV analgesics usually adequate following endovascular repair Intramuscular opiates not recommended DVT prophylaxis SCDs and early ambulation for all patients undergoing AAA repair Low-dose (subcutaneous) heparin prophylaxis for patients at high risk for DVT
59 Complication Frequency (%) All cardiac 15 Myocardial infarction 2-8 All pulmonary 8-12 Pneumonia 5 Renal insufficiency 5-12 Dialysis 1-6 Bleeding 2-5 Wound infection <5 Leg ischemia 1-4 Deep venous thrombosis 5-8 Colon ischemia 1-2 Stroke 1-2 Graft thrombosis <1 Graft infection <1 Ureteral injury <1 From Schermerhorn ML, Cronenwent JL. Abdominal aortic and iliac aneurysms. In: Rutherford RB, editor. Vascular surgery, 6 th ed. Philadelphia: Elsevier Saunders, p. 1431
60 Mortality Selected centers of excellence report 1-4% for elective infrarenal AAA repair Population-based series report 4-8% Higher-volume centers have lower AAA mortality rate than lower volume centers Surgeon volume impacts mortality rate Vascular surgeons (4.4%) have lower mortality rate than cardiothoracic surgeons (5.4%) and general surgeons (7.3%)
61 Graft infection Patient underwent AAA repair with aortobifemoral bypass graft several months earlier at another institution Persistent low-grade leukocytosis and malaise Treated with steroids for polymalgia rheumatica by PCP Admitted via ER and CT Scan obtained


62 Fat stranding and fluid around graft
63 Repair Options Removal of infected graft and extra-anatomic bypass Axillofemoral bypass Oversewing of aortic stump Removal of infected graft and direct repair Cryopreserved tissue graft Antibiotic soaked prosthetic graft Autologous femoral-popliteal vein reconstruction
64 Taken to OR for bilateral femoralpopliteal vein harvest and graft excision Aortoiliac reconstruction with aortobifemoral bypass graft composed of bilateral femoral veins Remained hospitalized for approximately ten days post-operatively No significant lower extremity edema and normal pedal pulses at follow-up

65 Good flow via replaced graft


66 Good flow via replaced graft
67 Endovascular Repair Most acute complications are due to groin wound issues Mortality should be less than 3% Endoleaks remain problematic Type I proximal or distal graft-vessel interface Type II collateral branches feed into sac Type III graft component separation or tears Type IV graft permeability Type V sac expansion without identified leak (Endotension, not seen with current devices)
68 Endovascular Repair Type I Should be treated when identified Proximal stent or balloon often seals leak If leak persists, will require conversion to open repair Type II Most common type of endoleak Should be treated if aneurysm sac expansion is identified If sac regression occurs, do not need treatment Controversy remains regarding stable sac size
69 Endovascular Repair Type III Should be treated Type IV Typically resolve after discontinuation of intraoperative heparin Do not require treatment Secondary interventions range from 9% to 35% over 1-3 years To some degree, represents a moving target of indications for interventions as technology and understanding evolve

70 85 year old man underwent endovascular aneurysm repair several years earlier in New York Presented to ER with abdominal pain and hypotension CT scan obtained Ruptured aneurysm with large type III endoleak

71 Type III Endoleak Taken to OR Right femoral cutdown Angiogram via left femoral sheath Endoleak at right limb overlap identified

72 Placement of new graft limb Successful exclusion of endoleak


73 Follow-up CT showing no further endoleak

74 77 year old underwent endovascular aneurysm repair six years ago Lost to follow-up CT scan performed for abdominal pain


75 CT scan revealed contrast extravasation into sac Underwent angiogram to identify source of endoleak

76 Multiple images obtained Type III endoleak at bifurcation (flow-divider) Options Endovascular conversion and femoral-femoral bypass Conversion to open repair with graft explantation


77 Aorto-uni-iliac device into left limb Right iliac occlusion device
78 Aorto-uni-iliac endovascular conversion Endoleak resolved Femoral-femoral bypass graft to restore flow to right leg Discharged home on post-operative day two
79 Additional endovascular issues Device migration, graft limb occlusion Post-operative fever not uncommon Due to sac thrombosis Need for long-term surveillance Currently requires serial CT scans 1 month, (6 months), annually May be followed by ultrasound under specific circumstances (severe renal dysfunction)

80 Long-term outcome of open repair better than endovascular repair Need for reintervention higher in endovascular group Mortality curves cross at about 5-6 years
81 Initial report by Parodi recommended stent grafts be used for patients unfit for open repair Was he right? Have we gone to far? Should repair be offered to everyone? What s next?
82 Endovascular technologies advancing Branch grafts and fenestrated grafts for visceral aorta Ascending aorta and aortic arch stent grafts Endovascular glue to fill sac Smaller introducer sheaths allow for fully percutaneous delivery
83 Questions
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
Abdominal Aortic Aneurysms (AAA): Management in 2012
: Management in 2012") Abdominal Aortic Aneurysms (AAA): Management in 2012 Matthew S. Edwards, MD, MS, FACS Associate Professor of Surgery and Public Health Sciences Department of Vascular and Endovascular Surgery General Considerations
Abdominal Aortic Aneurysms (AAA): Management in 2012 Matthew S. Edwards, MD, MS, FACS Associate Professor of Surgery and Public Health Sciences Department of Vascular and Endovascular Surgery General Considerations
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster
 Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
Care of Patients with an Abdominal Aortic Aneurysm
 Care of Patients with an Abdominal Aortic Aneurysm 2018 Practice Guidelines from the Society for Vascular Surgery vsweb.org/guidelines About the guidelines Published January 2018 in Journal of Vascular
Care of Patients with an Abdominal Aortic Aneurysm 2018 Practice Guidelines from the Society for Vascular Surgery vsweb.org/guidelines About the guidelines Published January 2018 in Journal of Vascular
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Experience of endovascular procedures on abdominal and thoracic aorta in CA region
 Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Experience of endovascular procedures on abdominal and thoracic aorta in CA region May 14-15, 2015, Dubai Dr. Viktor Zemlyanskiy National Research Center of Emergency Care Astana, Kazakhstan Region Characteristics
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Acute arterial embolism
 Acute arterial embolism Definition Thrombus come from heart or blood vessel or other embolus such as tumor,air gas or fat flow with blood stream and occlude distal limb or visceral arteries which causes
Acute arterial embolism Definition Thrombus come from heart or blood vessel or other embolus such as tumor,air gas or fat flow with blood stream and occlude distal limb or visceral arteries which causes
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
VASCULAR SURGERY, PART I VOLUME
 CME Pretest VASCULAR SURGERY, PART I VOLUME 42 7 2016 To earn CME credit, completing the pretest is a mandatory requirement. The pretest should be completed BEFORE reading the overview and taking the posttest.
CME Pretest VASCULAR SURGERY, PART I VOLUME 42 7 2016 To earn CME credit, completing the pretest is a mandatory requirement. The pretest should be completed BEFORE reading the overview and taking the posttest.
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
AORTIC GRAFT INFECTION
 NURSING CARE Theresa O Keefe NUM Vascular Unit PAH Vascular infections are serious They are associated with high morbidity and mortality The primary cause of surgical wound infections is contamination
NURSING CARE Theresa O Keefe NUM Vascular Unit PAH Vascular infections are serious They are associated with high morbidity and mortality The primary cause of surgical wound infections is contamination
Abdominal Aortic Aneurysm 가천대길병원 이상준
 Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Javier Marquez Graciani, MD Attending Dr F. Joglar
 Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Hypogastric Preservation Using Retrograde Endovascular Bypass
 Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD
 Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm
 Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
3 : 37. Kirit Patel, USA CLASSIFICATION DIAGNOSIS
 3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
3 : 37 Management of Aortic Aneurysms Clinical features and diagnosis of thoracic aortic aneurysm An aneurysm is currently defined as a localized dilatation of the aorta, 50 percent over the normal diameter,
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Management of the persistent sciatic artery with coexistent aortoiliac aneurysms; endovascular and open techniques.
 ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 14 Number 2 Management of the persistent sciatic artery with coexistent aortoiliac aneurysms; endovascular and open A Rodriguez-Rivera,
ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 14 Number 2 Management of the persistent sciatic artery with coexistent aortoiliac aneurysms; endovascular and open A Rodriguez-Rivera,
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Promising first experience of endovascular treatment of ruptured abdominal aortic aneurysms
 Promising first experience of endovascular treatment of ruptured abdominal aortic aneurysms Stevo Duvnjak, EBIR,FCIRSE Tomas Balezantis Jes Lindholdt Faculty disclosure Stevo Duvnjak, Tomas Balezantis,
Promising first experience of endovascular treatment of ruptured abdominal aortic aneurysms Stevo Duvnjak, EBIR,FCIRSE Tomas Balezantis Jes Lindholdt Faculty disclosure Stevo Duvnjak, Tomas Balezantis,
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Stanford Division of Vascular Surgery
 Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
Stanford Division of Vascular Surgery Interesting Cases 10/11/10 Vascular Surgery HPI: 62yoM with h/o CAD, HTN, ETOH abuse. S/P EVAR in 5/08 for 6cm AAA and right CIA aneurysm. Cook 30x96mm Main Body 24
Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication vs Benefit? Mortality? Morbidity?
 Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Preoperative intraaortic balloon counterpulsation in high-risk CABG Stefan Klotz, M.D. Preoperative IABP in high-risk CABG Questions?? Useful? Definition of High-risk? Pre-OP/Intra-OP/Post-OP? Complication
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant Week of November 19, 2018 Abdominal Aortogram, Bilateral Runoff
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
AAA Management: A Review of Current Therapy, Techniques, Outcomes and Best Practices
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians Frank R. Arko, III, MD Professor, Cardiovascular Surgery Co Director, Aortic Institute Director, Endovascular
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians Frank R. Arko, III, MD Professor, Cardiovascular Surgery Co Director, Aortic Institute Director, Endovascular
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
Abdominal Aortic Aneurysm (AAA)
") Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type 1b Endoleak following an EVAR for Ruptured AAA
 Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Is EVAS a proper choice in women?
 Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
Intended Learning Outcomes
 2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical Department National Taiwan University Hospital
 Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
Comparisons of Aortic Remodeling and Outcomes after Endovascular Repair of Acute and Chronic Complicated Type B Aortic Dissections I-Hui Wu, M.D. Ph.D. Clinical Assistant Professor Cardiovascular Surgical
AORTIC DISSECTIONS Current Management. TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida
 AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
AORTIC DISSECTIONS Current Management TOMAS D. MARTIN, MD, LAT Professor, TCV Surgery Director UF Health Aortic Disease Center University of Florida DISCLOSURES Terumo Medtronic Cook Edwards Cryolife AORTIC
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Case Report Surgical Treatment for Profunda Femoris Artery Aneurysms: Five Case Reports
 Case Reports in Vascular Medicine Volume 2015, Article ID 375278, 5 pages http://dx.doi.org/10.1155/2015/375278 Case Report Surgical Treatment for Profunda Femoris Artery Aneurysms: Five Case Reports Kimihiro
Case Reports in Vascular Medicine Volume 2015, Article ID 375278, 5 pages http://dx.doi.org/10.1155/2015/375278 Case Report Surgical Treatment for Profunda Femoris Artery Aneurysms: Five Case Reports Kimihiro
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE)
") US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE) Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Maimonides Aortic Center Maimonides Medical Center
US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE) Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Maimonides Aortic Center Maimonides Medical Center
CPT 2018 Radiology Code Changes
 CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
Endovascular treatment of acquired arteriovenous fistula with severe hemodynamic effects: a case report
 Endovascular treatment of acquired arteriovenous fistula with severe hemodynamic effects: a case report The Leipzig Interventional Course, January 24 27, 2017 El Samman K., Šedivý P., Šnajdrová A., Přindišová
Endovascular treatment of acquired arteriovenous fistula with severe hemodynamic effects: a case report The Leipzig Interventional Course, January 24 27, 2017 El Samman K., Šedivý P., Šnajdrová A., Přindišová
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Surgical Privileges Form: Vascular Surgery
 Surgical Form: Vascular Surgery Clinical Request Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. CATEGORY I: GENERAL PRIVILEGES 1. Admitting privileges
Surgical Form: Vascular Surgery Clinical Request Applicant s Name:. License No. (If Any):... Date:... Scope of Practice:. Facility:.. Place of Work:. CATEGORY I: GENERAL PRIVILEGES 1. Admitting privileges
How to manage the left subclavian and left vertebral artery during TEVAR
 How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
How to manage the left subclavian and left vertebral artery during TEVAR Jürg Schmidli Chief of Vascular Surgery Inselspital Hamburg 2017 Dept Cardiovascular Surgery, Bern, Switzerland Disclosure No Disclosures
Thoracoabdominal Aorta: Advances and Novel Therapies
 Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Thoracoabdominal Aorta: Advances and Novel Therapies Robert Meisner, MD FACS Sidney Kimmel Medical Center Assistant Professor of Surgery Vascular / Endovascular Surgeon at Lankenau Medical Center November
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
INL No. A0083 Project Medtronic Thoracic patients guide Description Version 18
 INL No. A0083 Project Medtronic Thoracic patients guide Description Version 18 www.inl-agency.com PATIENT INFORMATION BOOKLET Endovascular Stent Grafts: A treatment for Thoracic Aortic disease Table of
INL No. A0083 Project Medtronic Thoracic patients guide Description Version 18 www.inl-agency.com PATIENT INFORMATION BOOKLET Endovascular Stent Grafts: A treatment for Thoracic Aortic disease Table of
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag
 Let the CAT Scan Out of the Bag") Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Clinical trial and real-world outcomes of an endovascular iliac aneurysm repair with the GORE Iliac Branch Endoprosthesis (IBE)
") Clinical trial and real-world outcomes of an endovascular iliac aneurysm repair with the GORE Iliac Branch Endoprosthesis (IBE) Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon The Netherlands
Clinical trial and real-world outcomes of an endovascular iliac aneurysm repair with the GORE Iliac Branch Endoprosthesis (IBE) Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon The Netherlands
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
Diseases of the aorta
 Diseases of the aorta Aneurysm, dissection and aortitis are the main pathologies (Fig. 18.79 ). data:text/html;charset=utf-8,%3ch2%20id%3d%22cc5a0836d6aa490ca26dd7c15632b559%22%20style%3d%22margin%3a%201.3em%200px%200.5em%3b%20padding%3a%200px%3b%20border%3a%200px%3b%20font-fa
Diseases of the aorta Aneurysm, dissection and aortitis are the main pathologies (Fig. 18.79 ). data:text/html;charset=utf-8,%3ch2%20id%3d%22cc5a0836d6aa490ca26dd7c15632b559%22%20style%3d%22margin%3a%201.3em%200px%200.5em%3b%20padding%3a%200px%3b%20border%3a%200px%3b%20font-fa
2018 CPT CODING CHANGES
 17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
17 2018 CPT coding changes by Samuel Smith, MD, FACS; Megan McNally, MD, FACS; and Jan Nagle, MS, RPh JAN 2018 BULLETIN American College of Surgeons 18 Significant changes in Current Procedural Terminology
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS)
") Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Mid-term results of 300+ patients treated by endovascular aortic sealing (EVAS) Jean-Paul P.M. de Vries Dept Vascular Surgery St. Antonius Hospital, Nieuwegein,The Netherlands On behalf of the DEVASS study
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Supplementary Online Content
 Supplementary Online Content Smith D, Chudgar A, Daly B, Cooper M. Evaluation of potential renal transplant recipients with computed tomography angiography. Arch Intern Med. doi: 10.1001/archsurg.2012.1466.
Supplementary Online Content Smith D, Chudgar A, Daly B, Cooper M. Evaluation of potential renal transplant recipients with computed tomography angiography. Arch Intern Med. doi: 10.1001/archsurg.2012.1466.
Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm
 Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially