Basic Concepts in Pharmacokinetics. Leon Aarons Manchester Pharmacy School University of Manchester
|
|
|
- Aileen McGee
- 5 years ago
- Views:
Transcription
1 Basic Concepts in Pharmacokinetics Leon Aarons Manchester Pharmacy School University of Manchester
2 Objectives 1. Define pharmacokinetics 2. Describe absorption 3. Describe distribution 4. Describe elimination
 because we seek a certain effect (response), but a complex chain of events")
3 Why do we study PK? We administer drugs (dose) because we seek a certain effect (response), but a complex chain of events links the administered dose to the observed response Pharmacokinetics Pharmacodynamics

, the drug concentration in the desired matrix")
4 Drug concentration PK is based on the analysis of drug concentrations. After one or more doses ( measured (- -). ), the drug concentration in the desired matrix is Image from
5 (L)ADME The processes that characterize PK are summarized in the (L)ADME scheme. 1. Liberation 2. Absorption 3. Distribution 4. Metabolism 5. Excretion Elimination Disposition Image from
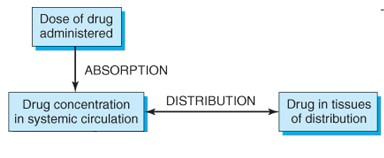
6 Absorption Absorption Distribution Elimination Dose of drug I N P U T Drug in blood Drug at active site Pharmacological effect L O S S Metabolism (M) + Excretion (E) Need to maintain plasma concentration of a drug to achieve a therapeutic effect
7 Absorption Absorption - Passage of compound from the site of administration into the bloodstream (or lymph), usually across a membrane Systemic routes of drug administration: Intravascular placement of the drug directly into blood (intravenous (iv) or intra-arterial) Extravascular oral, sublingual, subcutaneous, intramuscular, rectal Most drugs administered extravascularly act systemically. In such cases, systemic absorption is a prerequisite for efficacy Local effect - systemic absorption is a safety issue.
8 Absorption after oral administration Movement of unchanged drug from the site of administration to the site of measurement Few potential sites of loss contributes to decrease in systemic absorption
9 Bioavailability Bioavailability (F) refers to the extent of absorption of intact drug. Generally, refers to the fraction of an extravascularly administered dose that reaches the systemic circulation intact BA studies provide useful information on the dosage/dosage regimen BA studies provide information regarding the performance of a formulation

10 Bioavailability Relative F comparison of F between formulations of a drug given by the same or different routes of administration Absolute F is usually assessed with reference to an intravenous dose Relative F Absolute F
11 Bioequivalence (BE) Bioequivalence: Formulations containing the same dose of same chemical entity, generally in the same dosage form, intended to be interchangeable BE documentation may be useful to: Link early and late phase clinical formulations Compare clinical versus to-be-marketed formulation Evaluate change of formulation (tablet vs. capsule) Compare generic versus branded drug
12 Bioequivalence C-t profiles similar, NOT likely to cause clinically relevant differences in therapeutic and adverse effects! A and B are the limits set (often ± 20%) around the reference product. Bioequivalent preparations generally considered to be therapeutically equivalent
13 Rate limiting steps for oral absorption 1. Disintegration time and dissolution rate 2. Movement through membranes a) perfusion or b) permeability limitations 3. Gastric emptying and intestinal transit 4. First-pass metabolism in the gut/liver Can cause delay or loss of drug alteration of drug concentration!
14 Absorption from solution: Movement through membrane 3. Efflux transporters Absorption site 1. Transcellular 2. Paracellular Cell Blood and lymph
15 Distribution Absorption Distribution Elimination Dose of drug I N P U T Drug in blood Drug at active site Pharmacological effect L O S S Metabolism (M) + Excretion (E) Need to maintain plasma concentration of a drug to achieve a therapeutic effect
16 Distribution
17 Distribution Volume of Distribution (V d ) = Apparent and hypothetical volume in which the drug is dispersed An equilibrium concept Relates measured plasma (or blood) drug concentration (C) to the amount of drug in the body (A) Important for drug dosage regimen to determine the loading dose V = A C
18 Distribution Value depends on reference fluid measured (plasma, blood, unbound drug) Cb, C and Cu can differ as a consequence of binding to cells and plasma proteins However, at equilibrium: A = V C = V b C b = V u C u amount plasma blood plasma water



19 Distribution Relative size of various distribution volumes within a 70-kg individual Plasma: 4 liters. Interstitial volume: 10 liters. Intracellular volume: 28 liters


20 Distribution Vd: around 5 L. Very high molecular weight drugs, or drugs that bind to plasma proteins excessively Example: heparin 4L (3-5)

21 Extracellular fluid Distribution Vd: between 4 and 14 L. Drugs that have a low molecular weight but are hydrophilic. Example: Atracuronium 11 L (8-15)
 Alfentanyl 56 L (35-77) Drug that binds strongly to tissues. Vd higher than total body water.")
22 Vd equal or higher than total body water Distribution Diffusion to intracellular fluid. Vd equal to total body water. Ethanol 38 L (34-41) Alfentanyl 56 L (35-77) Drug that binds strongly to tissues. Vd higher than total body water. Fentanyl: 280 L Propofol: 560 L Digoxin:385 L
23 Volume of Distribution L/70kg 50,000 10, Quinacrine Chloroquine Desmethylimipramine Nortriptyline Pethidine Propranolol Digitoxin Warfarin Tolbutamide L/kg Cautious interpretation of V that are in the range of physiological values Drug can bind to plasma proteins, blood cells and tissue components
24 Plasma Protein Binding 1. Generally reversible, very rapid D + P DP 2. Extent of binding fu = fraction of drug unbound in plasma (Cu/C) 1 fu = fraction of drug bound 3. fu varies widely among the drugs Total plasma concentration (C) usually measured rather than the more important unbound concentration (Cu)
25 Distribution WHY IS UNBOUND CONCENTRATION IMPORTANT? Assumption only unbound drug diffuses into tissues, have pharmacological/toxicological effect and can be eliminated Plasma C bound Tissue C boundt Receptor Cu Cu T Elimination
26 Distribution V = V P + V T fu/fu T V V fu fu T
27 Elimination Absorption Distribution Elimination Dose of drug I N P U T Drug in blood Drug at active site Pharmacological effect L O S S Metabolism (M) + Excretion (E) Need to maintain plasma concentration of a drug to achieve a therapeutic effect
28 Elimination Elimination = irreversible removal of the drug from the body Metabolism liver and intestine as major sites main mechanism of drug elimination metabolites more polar than the parent drug and renally excreted Excretion kidneys - renal liver biliary excretion of drugs (hepatic) lungs - pulmonary (volatiles)


29 Concept of Clearance PROPORTIONALITY CONSTANT CLEARANCE is the parameter that relates rate of elimination to concentration: CL = Rate of Elimination / C plasma Units of flow (mg/h)/(mg/l) = L/h If CL= 1L/hr and C=0.5 mg/l steady-state concept Rate of elimination =0.5 mg/hr - A
30 Concept of Clearance CL is the apparent volume of plasma (or blood or plasma water) completely cleared of drug per unit of time. Rate of elimination = CL C = CL b C b = CL u C u plasma blood plasma water Value of clearance depends upon site of measurement
31 Dependence of elimination on both V and CL Drug Reservoir Sample Pump Flow rate Q Filter Volume of reservoir (V)= 1000mL Dose = 10 mg Initial concentration = 10 mg/l Perfect filter (organ), removes all drug: Flow rate 100 ml/min Clearance (Volume of blood completely cleared of drug per unit of time = Flow Rate, Q = 100 ml/min) CL = 100 ml/min Fractional rate of removal, k = 100 ml/min/1000 ml = 0.1 or 10% /min
32 Dependence of elimination on both V and CL Amount in body (A) A = V C Fractional elimination rate constant, k, defined as: k = Rate of elimination Amount = CL C V C = CL V CL = k V
33 Dependence of elimination on both distribution and CL CL t 1/2 t 1/2 = V CL V
34 Relationship of PK parameters The elimination half-life is defined as the time for the drug concentration to reach half of its value. Clinically interesting because intuitive, used to calculate when steady state is reached. It is a secondary parameter, which can be derived from CL and V t 1 2 = ( 2) ln V CL Rate of elimination = CL*C Remember that Amount eliminated = AAAAAA = CC(tt)dddd 0 0 If CL is constant with time CCCC. CC tt dddd = CCCC CC tt dddd = CCCC. AAAAAA 0 Amount eliminated = Dose*F = CL*AUC CL = Dose F AUC
35 1. Loss Across Organ of Elimination Mass balance Rate In Rate Out Q C A Q C V Rate of Elimination Q C A - Q C V Rate of Elimination = Rate In Rate Out Extraction ratio (E) = Rate of Elim. Rate In = Q C A CV Q C A = C A CV C A
36 1. Loss Across Organ of Elimination Rate In Q C A Rate Out Q (1-E) C A Rate of Elimination Q (E C A ) CL = Rate of Elimination Entering concentration = Q (C A -C V ) C A = Q E

37 Extraction ratio E = Q (C A -C V ) C A E 0 1 E = 0 No elimination E = 1 Complete elimination Typical blood flow values Liver ml/min Kidney 1100 ml/min Cardiac output 6000 ml/min
38 2. Additivity of Clearance Liver and kidney are major organs of elimination Rate of Elimination = Rate of Excretion + Rate of Hepatic Metabolism CL C = CL R C + CL H C Dividing by C: CL = CL R + CL H
39 Hepatic Elimination MAJOR ROUTES: 1. Metabolism 2. Biliary Excretion Two blood supplies: Hepatic Portal Vein (1.1 L/min) Hepatic vein (1.5 L/min) Hepatic Artery (0.4 L/min)
40 Metabolism The drug is changed so it can be eliminated Generates more polar (water soluble), inactive metabolites Metabolites may still have potent biological activity (or may have toxic properties)
41 Metabolism Metabolic enzymes and reactions Phase 0 Passive diffusion Carrier mediated uptake (OATP, OCT) Phase I non-polar OH Phase II polar O = O S=O O - Phase III sometimes referred to carrier mediated efflux/uptake (eg. BCRP, MRP2, ABCB1,3, BSEP) or additional conjugation Phase I In most cases, generation or exposing of functional groups (eg. -OH, -NH 2, -SH, -COOH) Reactions: oxidation reduction hydrolysis dealkylations deamination Phase II Enzymes: Hydrolysis Reactions: esterase glucuronide conjugation peptidase epoxide hydrolase sulfate conjugation Reduction glutathione conjugation azo and nitro reductase amino acid conjugation carbonyl reductase methylation quinone reductase acetylation Oxidation hydration cytochrome P450s (P450s or CYP) flavin-containing monooxygenases (FMO) monoamine oxidase (MAO) alcohol dehydrogenase aldehyde dehydrogenase and oxidase Conjugation with endogenous substrates, large increase in drug polarity Enzymes: UDP-glucuronosyltransferases (UGT) sulfotransferase (ST) glutathione S-transferase (GST) amino acid conjugating enzymes methyl transferase N-acethyltransferase
42 Metabolism Phase I Converts the parent drug to a more polar metabolite by introducing or unmasking a functional group (-OH, -NH2, -SH) via oxidation, reduction, and hydrolysis Usually results in loss of pharmacological activity Sometimes may be equally or more active than parent Occurs primarily in the liver
43 Metabolism Phase II (conjugation reactions) Subsequent reaction in which a covalent linkage is formed between the parent compound or Phase I metabolite and an endogenous substrate such as glucuronic acid, sulfate, acetate, or an amino acid Highly polar rapidly excreted in urine and feces Usually inactive - notable exception is morphine 6-glucuronide Usually occurs in liver and kidney (other organs sometimes involved)

44 Metabolism Most oxidative metabolism occurs via CYP450 system Image from: Guzman, Cambridge MedChem Consulting



45 3. Hepatic extraction and clearance Blood Cell a b Unbound drug Q H,B Hepatocyte c d P450 enzyme - CL int metabolites e Bile a binding to blood cells b binding to plasma proteins c transport into (and out of) hepatocytes d biliary excretion e - metabolism

46 Saturable kinetics Saturable kinetics can be approximated as 1 st order for lower concentrations, and 0 order for higher concentrations, as the system saturates. Described by the Michaelis-Menten equation: dc dt = V max K m C + C Maximum rate Michaelis constant Concentration at which V max /2 is reached Image from

47 RENAL EXCRETION Rate of excretion = CL R C RENAL CLEARANCE: CL R = Rate of Urinary Excretion /C plasma = V urine.c urine / C midpoint Units of flow = L/h
48 Renal Excretion A net effect 1. Glomerular filtration GFR= 120 ml/min 2. Secretion proximal tubule 3. Reabsorption distal tubule Urine 1-2 ml/min; ph = 5 7.8
49 F R - fraction of filtered and secreted drug reabsorbed Components of Renal Clearance Rate of = [ Excretion Rate of Filtration + Rate of Secretion ] X [ 1- Fraction reabsorbed ] /C plasma CL R = (CL RF + CL RS )(1- F R ) CL RF renal filtration clearance CL RS renal secretion clearance
50 Glomerular Filtration Passive process, only plasma water containing unbound drug (Cu) is filtered GFR - Glomerular Filtration Rate - usually constant and relatively independent of renal blood flow CL RF = Filtration Rate (Cu GFR) = fu GFR Plasma Concentration (C)
51 o GFR Determined using inulin or creatinine (fu=1 and not secreted or reabsorbed) Renal clearance, CL R = fu GFR o GFR depends on body size, gender and age Men (20 yr) 120 ml/min per 1.73 m2 Women (20 yr) 110 ml/min per 1.73 m2 o GFR decreases by 1% per year after age 20
52 ACTIVE SECRETION o Facilitates excretion o Transporters exist for basic and acidic drugs o Dissociation of plasma drug-protein complex as unbound drug is transported o If no reabsorption occurs, all drug presented to the kidney may be excreted in the urine CL RS Q R (1.1 L/min; e.g PAH)
53 Excretion Rate No reabsorption T M Secretion Plasma Drug Conc.
54 PASSIVE REABSORPTION Lipophilicity and degree of ionization affect rate and extent of reabsorption Plasma Tubular Fluid Cu + Cu 0 C 0 ur C + ur C bound Equilibrium not always achieved, especially for polar strong acids and bases Rate of reabsoption is important
55 Passive reabsorption effect of ph Urine ph varies: Weak acids - CL R is ph-sensitive if: pka = and lipophilic in un-ionised form pka < 3 strong acids, mostly ionised - little reabsorbed pka > 7.5 very weak acids, mostly un-ionised over urine ph range
56 CL R (ml/min) 20 Sulphamethoxazole Urine ph
57 Passive reabsorption effect of ph Urine ph varies: Weak bases - CL R is ph-sensitive if: pka = 6 12 and lipophilic in un-ionised form pka < 6 - mostly un-ionised over urine ph range pka > 12 - mostly ionised; little reabsorbed
58 Effect of ph on urinary excretion e.g. Amphetamine Urine ph Urinary recovery unchanged 24h Normal (ph 6.3) 40% Acidic (ph = 5.3) 70% Alkaline (ph = 7.3) 3%
59 Passive reabsorption effect of urine flow o Flow-dependent CL R occurs when drug is reabsorbed o If equilibrium is achieved a higher urine volume means a higher amount of drug in urine and higher CL R CL R = Rate of excretion /C plasma = Urine Flow x Urine conc /C plasma At equilibrium: Cu = Urine Conc CL R = fu x Urine Flow
60 FORCED ALKALINE DIURESIS - Phenobarbitone CL R (ml/min) 12 Urinary alkalisation 8 pka = 7.2 Normal urine ph Urine Flow (ml/min) o Drug overdose- forced diuresis and altered ph may be used to increase elimination of the drug
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues.
 and/ or cells of tissues.") It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
INTRODUCTION TO PHARMACOKINETICS
 INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
Pharmacokinetics of Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
Renal Function. 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular reabsorption 4. Excretion
 59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
BASIC PHARMACOKINETICS
 BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
General Principles of Pharmacology and Toxicology
 General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
ADME Review. Dr. Joe Ritter Associate Professor of Pharmacology
 ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
Unit 2b: EXCRETION OF DRUGS. Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)
 Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)") Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Excretion of Drugs. Prof. Hanan Hagar Pharmacology Unit Medical College
 Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
WHY... 8/21/2013 LEARNING OUTCOMES PHARMACOKINETICS I. A Absorption. D Distribution DEFINITION ADME AND THERAPEUIC ACTION
 PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations
 Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations Rosenbaum, Sara E. ISBN-13: 9780470569061 Table of Contents 1 Introduction to Pharmacokinetics and Pharmacodynamics.
Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations Rosenbaum, Sara E. ISBN-13: 9780470569061 Table of Contents 1 Introduction to Pharmacokinetics and Pharmacodynamics.
Chapter 4. Drug Biotransformation
 Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Renal Excretion of Drugs
 Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Drug elimination and Hepatic clearance Chapter 6
 Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
Pharmacokinetics. Karim Rafaat
 Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
PHA Second Exam Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2013 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points Set I 20 pts Set II 20 pts Set III 20 pts Set IV 20 pts Set
PHA 5127 Second Exam Fall 2013 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points Set I 20 pts Set II 20 pts Set III 20 pts Set IV 20 pts Set
Toxicant Disposition and Metabolism. Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine
 Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
BIOPHARMACEUTICS and CLINICAL PHARMACY
 11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
Metabolism. Objectives. Metabolism. 26 July Chapter 28 1
 Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect
Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
PHA First Exam. Fall 2004
 PHA 5127 First Exam Fall 2004 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet. If you need to comment or question a problem
PHA 5127 First Exam Fall 2004 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet. If you need to comment or question a problem
Pharmacokinetics in Drug Development. Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core
 Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
Click to edit Master title style
 A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
PHA First Exam Fall 2003
 PHA 5127 First Exam Fall 2003 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points 1. /14 pts 2. /6 pts 3. /15 pts 4. /12 pts 5. /20 pts 6. /10pts
PHA 5127 First Exam Fall 2003 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question/Points 1. /14 pts 2. /6 pts 3. /15 pts 4. /12 pts 5. /20 pts 6. /10pts
Industrial Toxicology
 Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
PHA Final Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Final Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE
 UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
PHA 5127 FINAL EXAM FALL On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 FINAL EXAM FALL 1997 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question Points 1. /14 pts 2. /10 pts 3. /8 pts 4 /8 pts 5. /12 pts 6. /8 pts
PHA 5127 FINAL EXAM FALL 1997 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Question Points 1. /14 pts 2. /10 pts 3. /8 pts 4 /8 pts 5. /12 pts 6. /8 pts
Basic Concepts of TDM
 TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
One-Compartment Open Model: Intravenous Bolus Administration:
 One-Compartment Open Model: Intravenous Bolus Administration: Introduction The most common and most desirable route of drug administration is orally by mouth using tablets, capsules, or oral solutions.
One-Compartment Open Model: Intravenous Bolus Administration: Introduction The most common and most desirable route of drug administration is orally by mouth using tablets, capsules, or oral solutions.
B. Incorrect! Compounds are made more polar, to increase their excretion.
 Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
General Principles of Pharmacology and Toxicology
 General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
General Principles of Pharmacology and Toxicology Parisa Gazerani, Pharm D, PhD Assistant Professor Center for Sensory-Motor Interaction (SMI) Department of Health Science and Technology Aalborg University
Drug Distribution. Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room
 Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Define the terms biopharmaceutics and bioavailability.
 Pharmaceutics Reading Notes Define the terms biopharmaceutics and bioavailability. Biopharmaceutics: the area of study concerning the relationship between the physical, chemical, and biological sciences
Pharmaceutics Reading Notes Define the terms biopharmaceutics and bioavailability. Biopharmaceutics: the area of study concerning the relationship between the physical, chemical, and biological sciences
The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
 1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
PRESCRIBING IN LIVER AND RENAL DISEASE
 THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
Pharmacodynamics & Pharmacokinetics 1
 PCTH 325 Pharmacodynamics & Pharmacokinetics 1 Dr. Shabbits jennifer.shabbits@ubc.ca September 9, 2014 Learning objectives 1. Describe the categories of intended drug action 2. Compare and contrast agonists
PCTH 325 Pharmacodynamics & Pharmacokinetics 1 Dr. Shabbits jennifer.shabbits@ubc.ca September 9, 2014 Learning objectives 1. Describe the categories of intended drug action 2. Compare and contrast agonists
PHAR 7632 Chapter 16
 PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
Chapter Questions. Modern Pharmacology With Clinical Applications. Sixth Edition
 Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA
 METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
PHA5128 Dose Optimization II Case Study I Spring 2013
 Silsamicin is an investigational compound being evaluated for its antimicrobial effect. The route of administration for this drug is via intravenous bolus. Approximately 99.9% of this drug is eliminated
Silsamicin is an investigational compound being evaluated for its antimicrobial effect. The route of administration for this drug is via intravenous bolus. Approximately 99.9% of this drug is eliminated
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION
 DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
Pharmacokinetics I. Dr. M.Mothilal Assistant professor
 Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics for Physicians. Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne
 Pharmacokinetics for Physicians Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne The Important Therapeutic Questions What drug? What dose? How long? Drug Dosage
Pharmacokinetics for Physicians Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne The Important Therapeutic Questions What drug? What dose? How long? Drug Dosage
PHA Final Exam Fall 2006
 PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
Tamer Barakat. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
Lippincott Questions Pharmacology
 Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Determination of bioavailability
 Pharmaceutics 2 Bioavailability Bioavailability is the rate and extent to which an administered drug reaches the systemic circulation. For example, if 100 mg of a drug is administered orally and 70 mg
Pharmaceutics 2 Bioavailability Bioavailability is the rate and extent to which an administered drug reaches the systemic circulation. For example, if 100 mg of a drug is administered orally and 70 mg
Biopharmaceutics. Tips Worth Tweeting. Contributor: Sandra Earle
 Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
Rational Dose Prediction. Pharmacology. φαρμακον. What does this mean? pharmakon. Medicine Poison Magic Spell
 1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017
 Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017") Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION
 CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
Pharmacokinetics Overview
 Pharmacokinetics Overview Disclaimer: This handout and the associated lectures are intended as a very superficial overview of pharmacokinetics. Summary of Important Terms and Concepts - Absorption, peak
Pharmacokinetics Overview Disclaimer: This handout and the associated lectures are intended as a very superficial overview of pharmacokinetics. Summary of Important Terms and Concepts - Absorption, peak
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics
 Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Pharmacokinetics Dr. Iman Lec. 3
 Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Principles of Drug Action. Intro to Pharmacology: Principles of Courework Drug Action Intro to Pharmacology
 Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
1. If the MTC is 100 ng/ml and the MEC is 0.12 ng/ml, which of the following dosing regimen(s) are in the therapeutic window?
 are in the therapeutic window?") Page 1 PHAR 750: Biopharmaceutics/Pharmacokinetics October 23, 2009 - Form 1 Name: Total 100 points Please choose the BEST answer of those provided. For numerical answers, choose none of the above if your
Page 1 PHAR 750: Biopharmaceutics/Pharmacokinetics October 23, 2009 - Form 1 Name: Total 100 points Please choose the BEST answer of those provided. For numerical answers, choose none of the above if your
Pharmacokinetics in the critically ill. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
What is pharmacokinetics?
 Pharmacokinetics What is pharmacokinetics? Study of the time course of a drug s movement through the body. Understanding of what the body does to (or with) the drug. Application of Therapeutic Drug Monitoring
Pharmacokinetics What is pharmacokinetics? Study of the time course of a drug s movement through the body. Understanding of what the body does to (or with) the drug. Application of Therapeutic Drug Monitoring
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2011 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2011 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
Metabolic Changes of Drugs and Related Organic Compounds
 Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy
 Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy I. General principles Applied pharmacokinetics - the process of using drug concentrations, pharmaco-kinetic
Basic Pharmacokinetic Principles Stephen P. Roush, Pharm.D. Clinical Coordinator, Department of Pharmacy I. General principles Applied pharmacokinetics - the process of using drug concentrations, pharmaco-kinetic
A primer on pharmacology
 A primer on pharmacology Universidade do Algarve Faro 2017 by Ferdi Engels, Ph.D. 1 2 1 3 Utrecht university campus de Uithof Dept. of Pharmaceutical Sciences Division of Pharmacology 4 2 Bachelor and
A primer on pharmacology Universidade do Algarve Faro 2017 by Ferdi Engels, Ph.D. 1 2 1 3 Utrecht university campus de Uithof Dept. of Pharmaceutical Sciences Division of Pharmacology 4 2 Bachelor and
Mechanisms of Drug Action
 10/31/05 Page 1 20.201 Mechanisms of Drug Action Lecture #18: Pharmacokinetics October 31, 2005 Review Dose-response Protein binding, drug transport(ers) Metabolism NOW: PHARMACOKINETICS Circulatory System
10/31/05 Page 1 20.201 Mechanisms of Drug Action Lecture #18: Pharmacokinetics October 31, 2005 Review Dose-response Protein binding, drug transport(ers) Metabolism NOW: PHARMACOKINETICS Circulatory System
PHA Final Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Final Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
Pharmacokinetics Metabolism
 Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate
 Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate") Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine. (iii) Predicting drug combinations
Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine. (iii) Predicting drug combinations
Section 5.2: Pharmacokinetic properties
 Section 5.2: Pharmacokinetic properties SmPC training presentation Note: for full information refer to the European Commission s Guideline on summary of product characteristics (SmPC) SmPC Advisory Group
Section 5.2: Pharmacokinetic properties SmPC training presentation Note: for full information refer to the European Commission s Guideline on summary of product characteristics (SmPC) SmPC Advisory Group
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /200 pts 1 Question Set I (True or
Slide 1. Slide 2. Slide 3. Drug Action and Handling. Lesson 2.1. Lesson 2.1. Drug Action and Handling. Drug Action and Handling.
 Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Regulation of fluid and electrolytes balance
 Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Regulation of fluid and electrolytes balance Three Compartment Fluid Compartments Intracellular = Cytoplasmic (inside cells) Extracellular compartment is subdivided into Interstitial = Intercellular +
Pharmacokinetics PCTH 325. Dr. Shabbits September 12, C t = C 0 e -kt. Learning Objectives
 PCTH 325 Pharmacokinetics Dr. Shabbits jennifer.shabbits@ubc.ca September 12, 2013 Learning Objectives 1. Interpret Concentration vs graphs and use them to calculate half life and predict drug concentration
PCTH 325 Pharmacokinetics Dr. Shabbits jennifer.shabbits@ubc.ca September 12, 2013 Learning Objectives 1. Interpret Concentration vs graphs and use them to calculate half life and predict drug concentration
DRUG DISTRIBUTION. Distribution Blood Brain Barrier Protein Binding
 DRUG DISTRIBUTION Distribution Blood Brain Barrier Protein Binding DRUG DISTRIBUTION Drug distribution is a reversible transport of drug through the body by the systemic circulation The drug molecules
DRUG DISTRIBUTION Distribution Blood Brain Barrier Protein Binding DRUG DISTRIBUTION Drug distribution is a reversible transport of drug through the body by the systemic circulation The drug molecules
Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University
 Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University Estimating renal function An accurate estimation of renal
Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University Estimating renal function An accurate estimation of renal
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics)
") TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
Renal Clearance. Dr. Eman El Eter
 Renal Clearance Dr. Eman El Eter Concept of clearance Clearance is the volume of plasma that is completely cleared of a substance each minute. Example: Renal clearance of Substance X is defined as the
Renal Clearance Dr. Eman El Eter Concept of clearance Clearance is the volume of plasma that is completely cleared of a substance each minute. Example: Renal clearance of Substance X is defined as the
Drug dosing in Extremes of Weight
 Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Orientation for New Child and Adolescent Psychiatry Residents: Module Four Pediatric Psychopharmacology
 Orientation for New Child and Adolescent Psychiatry Residents: Module Four Pediatric Psychopharmacology Objective: To discuss basic principles of psychopharmacology in children and adolescents. Pharmacokinetics:
Orientation for New Child and Adolescent Psychiatry Residents: Module Four Pediatric Psychopharmacology Objective: To discuss basic principles of psychopharmacology in children and adolescents. Pharmacokinetics:
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
MODULE No.26: Drug Metabolism
 SUBJECT Paper No. and Title Module No. and Title Module Tag PAPER No. 9: Drugs of Abuse MODULE No. 26: Drug Metabolism FSC_P9_M26 TABLE OF CONTENTS 1. Learning Outcomes 2. Introduction 3. Sites of Drug
SUBJECT Paper No. and Title Module No. and Title Module Tag PAPER No. 9: Drugs of Abuse MODULE No. 26: Drug Metabolism FSC_P9_M26 TABLE OF CONTENTS 1. Learning Outcomes 2. Introduction 3. Sites of Drug
BIOL 2402 Renal Function
 BIOL 2402 Renal Function Dr. Chris Doumen Collin County Community College 1 Renal Clearance and GFR Refers to the volume of blood plasma from which a component is completely removed in one minute by all
BIOL 2402 Renal Function Dr. Chris Doumen Collin County Community College 1 Renal Clearance and GFR Refers to the volume of blood plasma from which a component is completely removed in one minute by all
Pharmacogenetics and Pharmacokinetics
 Chapter 2 Pharmacogenetics and Pharmacokinetics Mauro Saivezzo/ShutterStock, Inc. L earning O bjectives Upon completion of this chapter, the student will be able to: 1. Recognize the influence of genetic
Chapter 2 Pharmacogenetics and Pharmacokinetics Mauro Saivezzo/ShutterStock, Inc. L earning O bjectives Upon completion of this chapter, the student will be able to: 1. Recognize the influence of genetic
The kidney. (Pseudo) Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella
 Practical questions. The kidneys are all about keeping the body s homeostasis. for questions Ella") The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
The kidney (Pseudo) Practical questions for questions Ella (striemit@gmail.com) The kidneys are all about keeping the body s homeostasis Ingestion Product of metabolism H 2 O Ca ++ Cl - K + Na + H 2 O
Brand and Generic Drugs. Educational Objectives. Absorption
 Peter J. Rice, PharmD, PhD Associate Professor of Pharmacology East Tennessee State University Educational Objectives Pharmacokinetic Processes Distribution Metabolism Excretion Similarities Active ingredient(s)
Peter J. Rice, PharmD, PhD Associate Professor of Pharmacology East Tennessee State University Educational Objectives Pharmacokinetic Processes Distribution Metabolism Excretion Similarities Active ingredient(s)
Nontraditional PharmD Program PRDO 7700 Pharmacokinetics Review Self-Assessment
 Nontraditional PharmD Program PRDO 7700 Pharmacokinetics Review Self-Assessment Please consider the following questions. If you do not feel confident about the material being covered, then it is recommended
Nontraditional PharmD Program PRDO 7700 Pharmacokinetics Review Self-Assessment Please consider the following questions. If you do not feel confident about the material being covered, then it is recommended
CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE
 CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE Joseph K. Ritter, Ph.D. Assoc. Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@vcu.edu This self study module will reinforce the
CLINICAL PHARMACOKINETICS INDEPENDENT LEARNING MODULE Joseph K. Ritter, Ph.D. Assoc. Professor, Pharmacology and Toxicology MSB 536, 828-1022, jritter@vcu.edu This self study module will reinforce the
Metabolic Changes of Drugs and Related Organic Compounds. Oxidative Reactions. Shokhan J. Hamid. 3 rd stage/ 1 st course Lecture 6
 Metabolic Changes of Drugs and Related Organic Compounds Oxidative Reactions 3 rd stage/ 1 st course Lecture 6 Shokhan J. Hamid B. OXIDATION INVOLVING CARBON OXYGEN SYSTEMS: Oxidative O-dealkylation of
Metabolic Changes of Drugs and Related Organic Compounds Oxidative Reactions 3 rd stage/ 1 st course Lecture 6 Shokhan J. Hamid B. OXIDATION INVOLVING CARBON OXYGEN SYSTEMS: Oxidative O-dealkylation of
Assem Al Refaei. Sameer Emeish. Dr.Alia. Hodaifa Ababneh & Abdullah Shurafa
 8 Assem Al Refaei Sameer Emeish Hodaifa Ababneh & Abdullah Shurafa Dr.Alia Sheet Checklist Bioequivalence and Therapeutic equivalence. Factors Influencing Absorption. Revising Bioavailability. Factors
8 Assem Al Refaei Sameer Emeish Hodaifa Ababneh & Abdullah Shurafa Dr.Alia Sheet Checklist Bioequivalence and Therapeutic equivalence. Factors Influencing Absorption. Revising Bioavailability. Factors
PHARMACOKINETICS SMALL GROUP I:
 PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
Principles of Pharmacology. Pharmacokinetics & Pharmacodynamics. Mr. D.Raju, M.pharm, Lecturer PHL-358-PHARMACOLOGY AND THERAPEUTICS-I
 Principles of Pharmacology Pharmacokinetics & Pharmacodynamics PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr. D.Raju, M.pharm, Lecturer Pharmacokinetics Movement of drugs in the body Four Processes Absorption
Principles of Pharmacology Pharmacokinetics & Pharmacodynamics PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr. D.Raju, M.pharm, Lecturer Pharmacokinetics Movement of drugs in the body Four Processes Absorption
Comparison Between the US FDA, Japan PMDA and EMA In Vitro DDI Guidance: Are we Close to Harmonization?
 Comparison Between the US FDA, Japan PMDA and EMA In Vitro DDI Guidance: Are we Close to Harmonization? Brian Ogilvie, Ph.D. VP Scientific Consulting XenoTech, LLC bogilvie@xenotechllc.com 14 Jun, 2018
Comparison Between the US FDA, Japan PMDA and EMA In Vitro DDI Guidance: Are we Close to Harmonization? Brian Ogilvie, Ph.D. VP Scientific Consulting XenoTech, LLC bogilvie@xenotechllc.com 14 Jun, 2018
Lecture 8: Phase 1 Metabolism
 Lecture 8: Phase 1 Metabolism The purpose of metabolism is to detoxify a drug, eliminate a drug or activate a drug. In metabolism there are two phases, Phase I and Phase II. Phase I is the introduction
Lecture 8: Phase 1 Metabolism The purpose of metabolism is to detoxify a drug, eliminate a drug or activate a drug. In metabolism there are two phases, Phase I and Phase II. Phase I is the introduction
Chapter 3 Drug Absorption and Bioavailability
 Chapter 3 Drug Absorption and Bioavailability Debra Si Mui Sim Abstract Most drugs are prescribed as oral preparations or extravascular injections (other than intravenous injections) for the treatment
Chapter 3 Drug Absorption and Bioavailability Debra Si Mui Sim Abstract Most drugs are prescribed as oral preparations or extravascular injections (other than intravenous injections) for the treatment
Effects of Liver Disease on Pharmacokinetics
 Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or
 Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or inactivation of the drug (i.e. therapeutic effects or toxicity)
Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or inactivation of the drug (i.e. therapeutic effects or toxicity)