THE HIP JOINT IN CEREBRAL PALSY
|
|
|
- Ilene Gallagher
- 5 years ago
- Views:
Transcription


1 HOSPITAL FOR JOINT DISEASES THE HIP JOINT IN CEREBRAL PALSY David S. Feldman, MD Professor of Orthopedic Surgery and Pediatrics Chief, Pediatric Orthopedic Surgery NYU/Hospital for Joint Diseases
2 Define the Problem (This review is meant to aid in knowledge but is no way is intended to be a thorough and comprehensive analysis of each topic)
3 Why The Hip?? Hip is particularly sensitive to muscle imbalance. Large number of large muscles crossing the joint. Psoas Adductors Rectus Hamstrings ITB G max/med/min Short Ext Rotators
4 Cerebral Palsy Children with CP develop hip subluxation 80% of Patients with Spastic Quadraplegia develop hip subluxation Spastic Diplegia and hemiplegia is associated with Acetabular Dysplasia Excessive Femoral Antetversion is common. This often causes the ambulating child to walk with his or her turned in excessively.
5 Progressive Hip Subluxation Often Painful Leads to assymetry and pelvic obliquity Dislocated hips become contracted Wind Swept Deformity Sitting imbalance


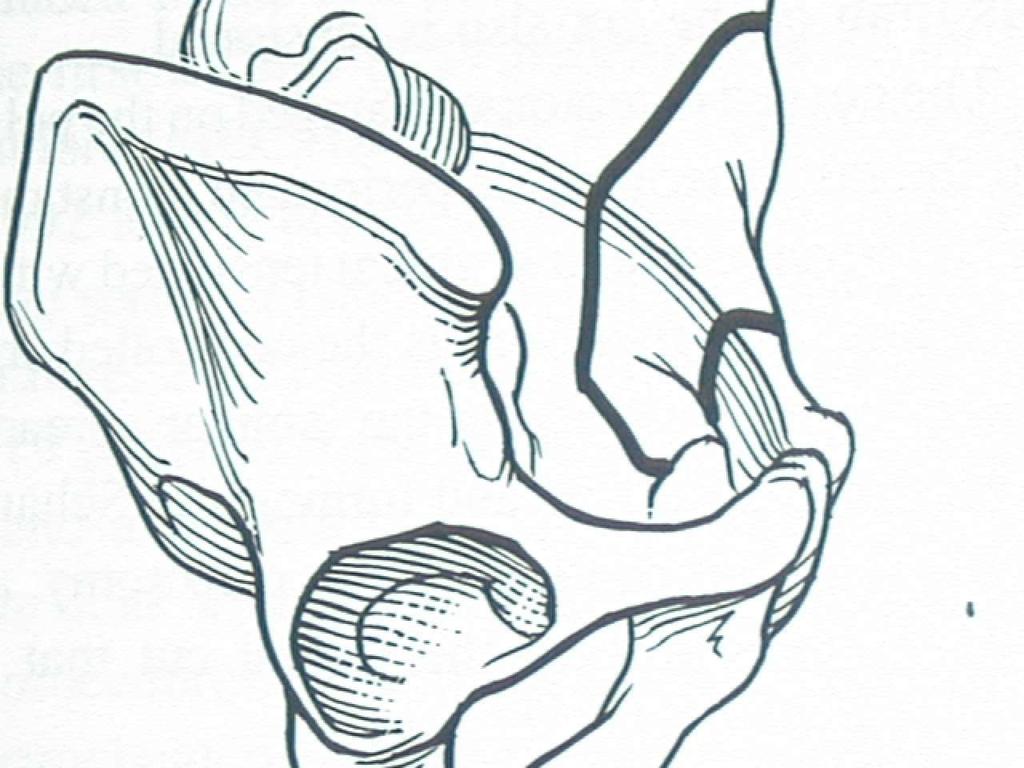
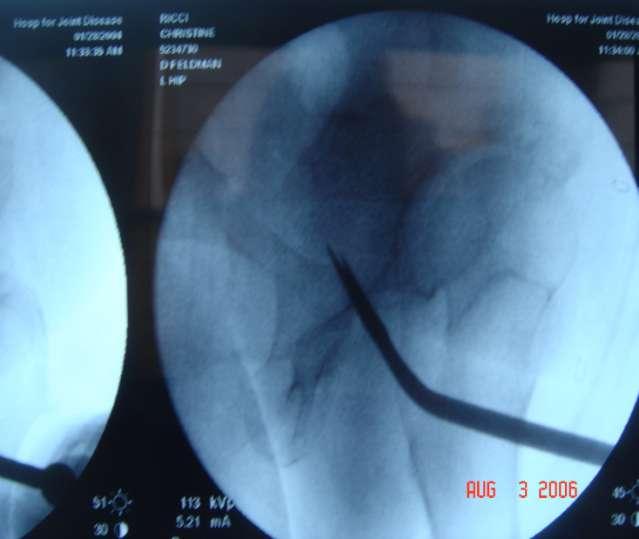
6 HIP DYSPLASIA (Acetabular Rim Syndrome)
7 Evaluation Contracture versus spasticity (R1 and R2)? Is there antagonist spasticity? Is there a dystonic or an athetoid component? Age of the patient and growth potential. Is there dynamic tone? Is there a contracture/spasticity a joint above or below the joint you are dealing with? Is the joint subluxated, dislocated or at risk?

8 Evaluation Is there pain? When, where and with which activities? Groin, thigh and buttock pain and prolonged sitting or standing. Is there a limp? Trendelenburg Is the problem femoral, acetabular, both or neither? I.e. Anteversion or Retroversion Is there joint congruency? If loss of congruity then type of surgery will change. Does the Joint Reduce on the abduction-internal rotation view (Van Rosen)? Reducible hip is needed for Osteotomy
, Van Rosen CT scan for femoral anteversion and acetabular")
9 Evaluation PE How much Flexion/ Extension of the hip? Abduction/adduction? Pain with IR? Gait abnormalities? ROM? LLD? X-ray- AP Pelvis, Judet (false profile view), Van Rosen CT scan for femoral anteversion and acetabular anatomy
10 What is femoral anteversion? Internal rotation of the femur Children are born with degrees of femoral anteversion Resolves to degrees by age 8 CP Increasing or nonresolved femoral anteversion

11 1 yo female - Left dislocated hip, Right subluxated hip

12 After open reduction - 3 yo

13 Age 14

14 Age 16 - s/p L VDO

15 Age 16 s/p R VDO

16 Age 28

17 Age 43

18 Age 43

19 Age 43 s/p THR
20 Goals SYMMETRY Agonist and antagonist complimentary function Protect joint Minimal or no immobilization NO SPICA CASTS ON CHILDREN WITH CP The spasticity does not tolerate casting Early return to standing and ambulation Minimize strength loss

21 GOALS Stable Reduced Joint Reduced Joint Contact Pressures Painless Joint Functional Range of Motion Decrease incidence of advanced OA
22 Working Together for Ambulation and Function Physical/Occupational Therapist Geneticist Pediatrician Developmental Pediatrician Pediatric Neurologist Pediatric Physiatrist Pediatric Neurosurgeon Pediatric Urologist Pediatric Orthopedic Surgeon Pediatric Social Worker
23 Still More Pediatric Psychologist Nurse Orthotist Special Education Teacher Pediatric Speech Therapist Pediatric Nurse Specialist Parent or Caregiver SPARE THE PATIENT FROM TAKING PART IN INTERPROFESSIONAL GAMES
24 Choices Botox/PT Tenotomies NSAID and/or Chondroitin/Glucosamine Intra-articular Steroid injection Hip Arthroscopy Femoral osteotomy/acetbular Osteotomy Trochanteric Advancement Total Hip Replacement

25 1 Yo Spastic Diplegic in 1999



26

27 2006
28 Surgical Options Percutaneous tendon releases (lengthening) Open tendon lengthening Muscle Recession Tendon Transfer Complete vs. Split Rhizotomy Baclofen pump Osteotomy Hip Reduction Bone/joint Resection Scoliosis Surgery
29 Which Procedure for Whom? Rhizotomy- Less than age 6, SPASTIC DIPLEGIA. Good trunk control. NO DYSTONIA. Orthopedic Surgery afterwards if there is contracture. Baclofen Pump When Spasticity is the main issue. Can treat dystonic component with high dosage. Will impair trunk stability if patient has truncal hypotonia. May increase scoliosis. May improve speec. May increase drooling.
30 Types of Releases/Transfers Percutaneous tenotomies- PERCS Percutaneous lengthenings -PERCS Open lengthening Open intramuscular recession Complete Transfer in Phase Complete Transfer out of Phase Split Transfer Muscle Slide
31 Hip Soft Tissue Contractures Hip Flexion - Psoas, Rectus and sartorius Hip Extension Gluteus Maximus Adduction Adductors and Medial Hamstring Abduction - ITB and Gluteus Medius Internal Rotation Gluteus Medius and Medial Hamstring External Rotation Short External Rotators, and Gluteus Maximus
32 Hip Contracture Solutions Hip Flexion Psoas (Psoas Recession) Hip Extension Gluteus Maximus (Osteotomy) Adduction Adductors (Percutaneous tenotomy) Abduction - ITB (Percutaneous tenotomy) Internal Rotation Gluteus Medius (Anterior Trochanteric Transfer) External Rotation Short External Rotators (Osteotomy)
33 Knee Contractures Flexion Medial and Lateral Hamstrings Extension Rectus Femoris and Vastus lateralis Hadley et al. JPO 1992 Abel et al JPO 1999


34 Knee Contracture Solutions Flexion Medial and Lateral Hamstrings (Pecutaneous/Open Hamstring lengthening, tenotomies and possible osteotomy) Extension Rectus Femoris (Rectus transfer or possible proximal release)
35 SYMMETRY Range of motion Neck Shaft Angle Limb length Femoral Anteversion Tibial rotation
36 Management of Acetabular Dysplasia

37 Pelvic Osteotomies Salter Ostetomy - Below age 8, degrees of Antero-lateral coverage Pemberton/Dega- Used for a voluminous acetabulum, The tri-radiate cartilage must be open Tonnis/Steel/Sutherland Osteotomy- Triple Ostetomies with varying degrees of freedom, ages 6 to adulthood. Ganz/Dial Osteotomy- Marked ability to move acetabulum, Triradiate closure to adulthood Chiari/Shelf- Incongruous hip coverage, Salvage, metaplasia

38 14 yo with Spastic Diplegia Subluxated Left hip Dysplastic Acetabulum



39 Arthrogram


40 4 yo with spastic Diplegia


41

42 DO NOT IMMOBILIZE THE HIP AND KNEE

43 Periacetabular Osteotomy (PAO) Bern Periacetabular Osteotomy Described in CORR in 1988 by Reinhold Ganz Periacetabular Osteotomy that leaves the posterior column intact Allows for medialization of the hip----biomechanically Advantageous Allows for immediate weight bearing Need a Congruous and Reducible Hip
44
45

46

47


48


49
50


51

52


53 16 yo with Spastic Diplegia
54 Commonly Asked Questions
55 What Age Does One Go form Botox or Soft Tissue Peocedures to Osteotomies?
56 ANSWER Historically age 6-8 If there are boney changes, i.e flattening or misshapen femoral head then age is irrelevant. Often early Botox and/or Percs may prevent the need for boney surgery
57 HIP DISLOCATION SHOULD WE PREVENT? YES SHOULD WE REDUCE/ Resect? IF PAINFUL

58 5 yo Spastic Quadraplegia

59


60 Surgical and 18 month f/u


61 14 yo Spastic Quadrplegia

62
63 Etiology (CAUSE) of Internal Rotation Gait??

64 Internal Rotation Gait Medial Hamstring Adductors Gluteus Medius Spasticity Femoral Anteversion? Capsular tightness/hip anatomy
65 IS SURGERY ALWAYS BILATERAL??
66 Answer Always achieve Symmetry. Different sides may require different procedures.

67 9 yo boy with Spastic Diplegia
68 May a Child with Hip Subluxation: Bear Weight? Be in a Stander?
69 YES There are no special precautions needed for these children aside from avoiding painful positioning
70 DYSTONIA and the Subluxed Hip??

71 Unanswered Question??S.L.O.B.


72
73 Lever Arm Disease?? What is it? Prevention?? Treatment??

74


75
76 Lever arm disease is the adolescent with calcaneus feet, knee flexion contractures, hip flexion contractures and lumbar lordosis. Should we stop doing heel cord lengthenings in diplegics and use extensive serial casting? Definitely DO NOT OVER LENGTHEN THE HEEL CORD!!!!!!!! Treat before patella alta occurs.
77 Lever Arm Disease Most likely Osteotomies unless caught very early is the only solution. Hip and knee extension osteotomies. Patella tendon imbrication.
78 SCOLIOSIS and the HIP

79 SCOLIOSIS IN CEREBRAL PALSY SURGICAL INDICATIONS: Progressive deformity Sitting imbalance Pelvic obliquity

80 Cerebral Palsy Scoliosis Spastic quadriplegia highest risk Custom seats
")
81 SCOLIOSIS IN CEREBRAL PALSY SURGICAL MANAGEMENT ASF/PSF vs. PSF only Segmental fixation Fuse to the pelvis (Galveston)

82

83

84
85 ROM of the HIP Particularly important if the the Spine is being fused to the pelvis Be especially cognizant of lack of true flexion of the hip
86 DO NOT!!!!!! Lengthen a muscle without addressing the antagonist Miss the dynamic, dystonic or athetoid component Miss a joint subluxation or dislocation Miss the opportunity to correct a problem before secondary changes occur. Over lengthen heel cords or hamstrings Create assymetry Immobilze the knee and hip of a child with CP for a prolonged period
Lower Extremity Orthopedic Surgery in Cerebral Palsy
 Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Lower Extremity Orthopedic Surgery in Cerebral Palsy Hank Chambers, MD San Diego Children s Hospital San Diego, California Indications Fixed contracture Joint dislocations Shoe wear problems Pain Perineal
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Biomechanics and Osteotomies
 Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
Hip Biomechanics and Osteotomies Organization Introduction Hip Biomechanics Principles of Osteotomy Femoral Osteotomies Pelvic Osteotomies Summary Inroduction Osteoarthritis is very prevalent Primary OA
10/26/2017. Comprehensive & Coordinated Orthopaedic Management of Children with CP. Objectives. It s all about function. Robert Bruce, MD Sayan De, MD
 Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
SWASH CERTIFICATION EXAM
 SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
SWASH CERTIFICATION EXAM Sitting Walking And Standing Hip Orthosis Today s Date: Location: Name: License #: Employer: Address: Ste/Apt #: City: State: Zip: Email Address: 1) Which of the following are
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Case Study: Christopher
 Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Case Study: Christopher Conditions Treated Anterior Knee Pain, Severe Crouch Gait, & Hip Flexion Contracture Age Range During Treatment 23 Years to 24 Years David S. Feldman, MD Chief of Pediatric Orthopedic
Considerations in the selection of patients for Selective Dorsal Rhizotomy
 Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
Management of knee flexion contractures in patients with Cerebral Palsy
 Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
Management of knee flexion contractures in patients with Cerebral Palsy Emmanouil Morakis Orthopaedic Consultant Royal Manchester Children s Hospital 1. Introduction 2. Natural history 3. Pathophysiology
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
Management of the Hip in Cerebral Palsy
 Management of the Hip in Cerebral Palsy Tom F. Novacheck, MD Pediatric Orthopaedic Surgeon Director, James R Gage Center for Gait and Motion Analysis St. Paul, MN, USA Associate Professor, Univ of MN Dept
Management of the Hip in Cerebral Palsy Tom F. Novacheck, MD Pediatric Orthopaedic Surgeon Director, James R Gage Center for Gait and Motion Analysis St. Paul, MN, USA Associate Professor, Univ of MN Dept
1/15/ year old male. Hip Preservation Surgery for Acetabular Dysplasia in Adolescents and Young Adults PATHOMECHANICS OF ACETABULAR DYSPLASIA
 29 year old male Hip Preservation Surgery for Acetabular Dysplasia in Adolescents and Young Adults Eduardo Novais, MD Assistant Professor of Orthopedic Surgery PATHOMECHANICS OF ACETABULAR DYSPLASIA Static
29 year old male Hip Preservation Surgery for Acetabular Dysplasia in Adolescents and Young Adults Eduardo Novais, MD Assistant Professor of Orthopedic Surgery PATHOMECHANICS OF ACETABULAR DYSPLASIA Static
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort
 Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Hip Preservation Timothy J Sauber MD Orthopaedic Update March 22, 2015 Nemacolin Woodlands Resort Disclosures No disclosures relevant to this topic Objectives Evaluate and recognize common hip pathology
Adult Hip Dysplasia David S. Feldman, MD
 Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
The Young Adult Hip: FAI. Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California
 The Young Adult Hip: FAI Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California Introduction Femoroacetabular Impingment(FAI) Presentation and Exam Imaging Surgical Management
The Young Adult Hip: FAI Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California Introduction Femoroacetabular Impingment(FAI) Presentation and Exam Imaging Surgical Management
Why Would Your Child Need to See Me?
 Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
Why Would Your Child Need to See Me? Deborah M Eastwood Great Ormond St Hospital for Children, London The Royal National Orthopaedic Hospital, UK Disclosures I am an orthopaedic surgeon and I do operate
DR. (PROF.) ANIL ARORA MS
 ANIL ARORA MS") Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Case Study: Nadine. Conditions Treated Hip Dysplasia. Age Range During Treatment 39 years
 Case Study: Nadine Conditions Treated Hip Dysplasia Age Range During Treatment 39 years David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone
Case Study: Nadine Conditions Treated Hip Dysplasia Age Range During Treatment 39 years David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie
 Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
Surgical release of neurological hip luxation in children H. Klima Ostschweizer Kinderspital St. Gallen Abteilung für Kinderorthopädie Development of hip luxation At birth these hips are normal developed,
אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים
 אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP היח' ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים 1 CP- Spectrum of pathology 2 Lower Limb problems in CP Spastic Quadriplegia- Hip,Pelvis, Spine
אתגרים ופתרונות ניתוחיים סביב מפרק הברך בילדי CP היח' ד"ר טלי בקר לאורטופדית ילדים,מרכז שניידר לרפואת ילדים 1 CP- Spectrum of pathology 2 Lower Limb problems in CP Spastic Quadriplegia- Hip,Pelvis, Spine
Muscles to know. Lab 21. Muscles of the Pelvis and Lower Limbs. Muscles that Position the Lower Limbs. Generally. Muscles that Move the Thigh
 Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
Muscles to know Lab 21 Muscles of the Pelvis, Leg and Foot psoas major iliacus gluteus maximus gluteus medius sartorius quadriceps femoris (4) gracilus adductor longus biceps femoris semitendinosis semimembranosus
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CLINICS IN SPORTS MEDICINE
 Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Anatomy & Physiology. Muscles of the Lower Limbs.
 Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Anatomy & Physiology Muscles of the Lower Limbs http://www.ishapeup.com/musclecharts.html Muscles of the Lower Limbs Among the strongest muscles in the body. Because pelvic girdle is composed of heavy,
Main Menu. Joint and Pelvic Girdle click here. The Power is in Your Hands
 1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies
 Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study
 Prague Medical Report / Vol. 106 (2005) No. 2, p. 159 166 159) Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study Al Razi Orthopedic Hospital,
Prague Medical Report / Vol. 106 (2005) No. 2, p. 159 166 159) Combined Pelvic Osteotomy in the Treatment of Both Deformed and Dysplastic Acetabulum Three Years Prospective Study Al Razi Orthopedic Hospital,
Young Adult Hip problems. Aresh Hashemi-Nejad FRCS(Orth)
") Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Myology of the Knee. PTA 105 Kinesiology
 Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
The Hip (Iliofemoral) Joint. Presented by: Rob, Rachel, Alina and Lisa
 Joint. Presented by: Rob, Rachel, Alina and Lisa") The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
The Hip (Iliofemoral) Joint Presented by: Rob, Rachel, Alina and Lisa Surface Anatomy: Posterior Surface Anatomy: Anterior Bones: Os Coxae Consists of 3 Portions: Ilium Ischium Pubis Bones: Pubis Portion
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Orthopedic Issues in Children with Special Healthcare Needs
 Orthopedic Issues in Children with Special Healthcare Needs Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department
Orthopedic Issues in Children with Special Healthcare Needs Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department
Ganzosteotomy Description and indications. Dr. Jaak Roos - A.Z. Turnhout
 Ganzosteotomy Description and indications Dr. Jaak Roos - A.Z. Turnhout Welcome Turnhout Flanders Cultural Capital 2012 Turnhout: Stad van m n hert Hip Dysplasia Natural history of HD without subluxation:
Ganzosteotomy Description and indications Dr. Jaak Roos - A.Z. Turnhout Welcome Turnhout Flanders Cultural Capital 2012 Turnhout: Stad van m n hert Hip Dysplasia Natural history of HD without subluxation:
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
AACPDM IC#21 DFEO+PTA 1
 Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Roles of Distal Femoral Extension Osteotomy and Patellar Tendon Advancement in the Treatment of Severe Persistent Crouch Gait in Adolescents and Young Adults with Cerebral Palsy Instructional Course #21
Peggers Super Summaries: Paediatric Hip
 EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
Non-Arthroplasty Hip Surgery. Javad Parvizi MD FRCS Professor of Orthopaedic Surgery
 Non-Arthroplasty Hip Surgery Javad Parvizi MD FRCS Professor of Orthopaedic Surgery Subcapital reduction osteotomy Relative lengthening of femoral neck (Perthes) AVN surgery Femoral osteotomy Trap door
Non-Arthroplasty Hip Surgery Javad Parvizi MD FRCS Professor of Orthopaedic Surgery Subcapital reduction osteotomy Relative lengthening of femoral neck (Perthes) AVN surgery Femoral osteotomy Trap door
The hip: Built for endurance and mobility
 The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty. Faculty Disclosures. Objectives 11/17/2017
 Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Muscles of the Thigh. 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group
 Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Muscles of the Thigh 6.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Sartorius: This is a long strap like muscle with flattened tendons at each
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Degenerative arthritis of Hip Bone Bangalore. Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal
 Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
Degenerative arthritis of Hip Prof Sharath Rao Head, Dept. of Orthopaedics KMC Manipal Hip joint Classical Synovial joint Biomechanics of hip Force coincides with trabecular pattern Hip joint Acetabulum
Keith Bachmann, MD UVA Department of Orthopaedic Surgery
 Keith Bachmann, MD UVA Department of Orthopaedic Surgery Definition Spinal deformity secondary to either neurologic or muscle pathology. Etiology Imbalance of muscle forces Lack of truncal support Similar
Keith Bachmann, MD UVA Department of Orthopaedic Surgery Definition Spinal deformity secondary to either neurologic or muscle pathology. Etiology Imbalance of muscle forces Lack of truncal support Similar
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016
 Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
Human Anatomy Biology 255
 Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Lectures of Human Anatomy
 Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Lectures of Human Anatomy Lower Limb Gluteal Region and Hip Joint By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D.
Changes in lower limb rotation after soft tissue surgery in spastic diplegia
 Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
Acta Orthopaedica 2010; 81 (2): 245 249 245 Changes in lower limb rotation after soft tissue surgery in spastic diplegia 3-dimensional gait analysis in 28 children Bjørn Lofterød 1 and Terje Terjesen 2
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Hip joint and pelvic girdle. Lower Extremity. Pelvic Girdle 6/5/2017
 Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
Hip joint and pelvic girdle Lower Extremity The relationship between the pelvic girdle and hip is similar to that between the shoulder girdle and shoulder joint. The lower limbs are attached to the axial
DDH: Pathology Diagnosis, and Treatment before Walking Age
 DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
Swiss Medical Network Musculoskeletal Conference Surgical Technique and 30-Year Results of the Periacetabular Osteotomy (PAO)
") Swiss Medical Network Musculoskeletal Conference 2017 Surgical Technique and 30-Year Results of the Periacetabular Osteotomy (PAO) Simon D. Steppacher Department of Orthopedic Surgery, Inselspital, University
Swiss Medical Network Musculoskeletal Conference 2017 Surgical Technique and 30-Year Results of the Periacetabular Osteotomy (PAO) Simon D. Steppacher Department of Orthopedic Surgery, Inselspital, University
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES
 DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
DEFICIENCE MOTRICE CEREBRALE: INTERVENTIONS EN ORTHOPEDIE PEDIATRIQUE CAROLINE FORSYTHE MD, FRCSC RESUME SURVEILLANCE DES HANCHES TRAITMENTS NONCHIRURGICALES BOTOX PLATRES D INHIBITION APPROCHE CHIRURGICALE
The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular rim during normal hip range of motion.
 RIM SYNDROME [femoroacetabular impingement] It has been suggested to be a preosteoarthritic mechanism. The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular
RIM SYNDROME [femoroacetabular impingement] It has been suggested to be a preosteoarthritic mechanism. The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular
Triple Pelvic Osteotomy
 Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? TRAMA Project. January th Clinical case presentation
 Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
Second Course Motion Analysis and clinics: why set up a Motion Analysis Lab?? - Clinical cases presentation - TRAMA Project January 14-17 th 2008 Iván Carlos Uribe Prada Instituto de Ortopedia Infantil
DDH New Developments and Timeless Classics. DDH Define Treatment Group. (by age) DDH Imaging Choice in 6wk old Infant?
 DDH Imaging Choice in 6wk old Infant?") The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
The 59 th Annual Edward T. Smith Orthopaedic Lectureship Emerging Concepts in the Surgical Management of the Hip: Deformity, Impingement and Fracture DDH New Developments and Timeless Classics Perry L.
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit. Evaluation and Diagnosis of Osteoarthritis in Primary Care
 Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip
 of the Hip") A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Femoroacetabular Impingement in the Throwing Athlete. Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute
 Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP?
 HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
 Case Reports in Orthopedics Volume 2015, Article ID 854151, 4 pages http://dx.doi.org/10.1155/2015/854151 Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
Case Reports in Orthopedics Volume 2015, Article ID 854151, 4 pages http://dx.doi.org/10.1155/2015/854151 Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
Chapter 3: Applied Kinesiology. ACE Personal Trainer Manual Third Edition
 Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
Chapter 3: Applied Kinesiology ACE Personal Trainer Manual Third Edition Introduction Kinesiology is the study of the body s infinite number of movements, positions, and postures and is grounded in the
Stephanie W. Mayer, MD. Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado
 Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
Stephanie W. Mayer, MD Director of Child and Young Adult Hip Preservation Sports Medicine Center Children s Hospital Colorado University of Colorado Sports Medicine Assistant Team Physician, Colorado Avalanche
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
PediLoc Extension Osteotomy Plate (PLEO)
") PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
PediLoc Extension Osteotomy Plate (PLEO) Left PLEO Plates Sizes: 6, 8 and 10 hole plates Right PLEO Plates Sizes: 6, 8 and 10 hole plates PediLoc Extension Osteotomy Plate The technique description herein
L side 65% Torticollis, Plagiocephaly, Metatarsus varus Flat foot.
 DEVELOPMENTAL DISLOCATION OF THE HIP [DDH] Older terminology was Congenital dislocation of the hip. DDH means developmental dysplasia of the hip. DDH is better than CDH as dislocation is not always congenital.
DEVELOPMENTAL DISLOCATION OF THE HIP [DDH] Older terminology was Congenital dislocation of the hip. DDH means developmental dysplasia of the hip. DDH is better than CDH as dislocation is not always congenital.
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Human anatomy reference:
 Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus. Alfred D. Grant, M.D. David Feldman, M.D.
 The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
The Valgus Foot in Cerebral Palsy Equinovalgus not Plano-Valgus Alfred D. Grant, M.D. David Feldman, M.D. Norman Otsuka, MD M.D. THE PURPOSE OF THIS PRESENTATION IS TO STATE CLEARLY THAT THE VALGUS FOOT
Pediatric Orthopaedic Fellowship Curriculum
 Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Pediatric Orthopaedic Fellowship Curriculum The Fellowship Pediatric Orthopaedic Curriculum is designed for the fellow to spend three months each in four content areas. There are five content areas comprising
Sports Medicine 15. Unit I: Anatomy. The knee, Thigh, Hip and Groin. Part 4 Anatomies of the Lower Limbs
 Sports Medicine 15 Unit I: Anatomy Part 4 Anatomies of the Lower Limbs The knee, Thigh, Hip and Groin Anatomy of the lower limbs In Part 3 of this section we focused upon 11 of the 12 extrinsic muscles
Sports Medicine 15 Unit I: Anatomy Part 4 Anatomies of the Lower Limbs The knee, Thigh, Hip and Groin Anatomy of the lower limbs In Part 3 of this section we focused upon 11 of the 12 extrinsic muscles
Biomechanics of the Upper Extremity Shoulder and Hip
 Biomechanics of the Upper Extremity Shoulder and Hip www.fisiokinesiterapia.biz The Shoulder Common Injuries Shoulder Joint - Bones Anatomical Structures Bursa - Fibrous, fluid-filled sac that reduces
Biomechanics of the Upper Extremity Shoulder and Hip www.fisiokinesiterapia.biz The Shoulder Common Injuries Shoulder Joint - Bones Anatomical Structures Bursa - Fibrous, fluid-filled sac that reduces
Case Presentations The Child with a Limp
 Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Joints of the lower limb
 Joints of the lower limb 1-Type: Hip joint Synovial ball-and-socket joint 2-Articular surfaces: a- head of femur b- lunate surface of acetabulum Which is deepened by the fibrocartilaginous labrum acetabulare
Joints of the lower limb 1-Type: Hip joint Synovial ball-and-socket joint 2-Articular surfaces: a- head of femur b- lunate surface of acetabulum Which is deepened by the fibrocartilaginous labrum acetabulare
CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT
 SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB
 ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
ASSESSING GAIT IN CHILDREN WITH CP: WHAT TO DO WHEN YOU CAN T USE A GAIT LAB Robert M. Kay, MD Vice Chief, Children s Orthopaedic Center Children s Hospital Los Angeles Professor of Orthopaedic Surgery
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
EXAMINATION OF HIP. A. Inspection Examination
 EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Temporalis Elevates & retracts mandible. Masseter Elevates mandible. Sternocleidomastoid Neck flexion. Trapezius Elevates & depresses shoulders
 Anterior Posterior Temporalis Elevates & retracts mandible Masseter Elevates mandible Sternocleidomastoid Neck flexion Trapezius Elevates & depresses shoulders Masseter Elevates mandible Temporalis Elevates
Anterior Posterior Temporalis Elevates & retracts mandible Masseter Elevates mandible Sternocleidomastoid Neck flexion Trapezius Elevates & depresses shoulders Masseter Elevates mandible Temporalis Elevates
Hip Region. PHTY2020: Lecture
 Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Topic 7: Hip and pelvis. Parts of the hip. Parts of the femur
 Topic 7: Hip and pelvis Parts of the hip Parts of the femur Classifying the hip joint Ball and socket Synovial Multiaxial Movements of the hip: Abduction/adduction Flexion/extension Medial/lateral rotation
Topic 7: Hip and pelvis Parts of the hip Parts of the femur Classifying the hip joint Ball and socket Synovial Multiaxial Movements of the hip: Abduction/adduction Flexion/extension Medial/lateral rotation
Lesson 24. A & P Hip
 Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
5/14/2013. Acute vs Chronic Mechanism of Injury:
 Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Pilates for the Post Periacetabular Osteotomy (PAO) Client
 Client") Pilates for the Post Periacetabular Osteotomy (PAO) Client Stacey Barnes September 28, 2014 Oceanside, CA 1 Abstract This paper examines how Pilates is used as a conditioning program for a client post
Pilates for the Post Periacetabular Osteotomy (PAO) Client Stacey Barnes September 28, 2014 Oceanside, CA 1 Abstract This paper examines how Pilates is used as a conditioning program for a client post
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
Multiapical Deformities p. 97 Osteotomy Concepts and Frontal Plane Realignment p. 99 Angulation Correction Axis (ACA) p. 99 Bisector Lines p.
 p. 99 Bisector Lines p.") Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
Normal Lower Limb Alignment and Joint Orientation p. 1 Mechanical and Anatomic Bone Axes p. 1 Joint Center Points p. 5 Joint Orientation Lines p. 5 Ankle p. 5 Knee p. 5 Hip p. 8 Joint Orientation Angles
The Hip Joint. Exercises and Injuries
 The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
The University Of Jordan Faculty Of Medicine THE LOWER LIMB. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous
The University Of Jordan Faculty Of Medicine THE LOWER LIMB Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Gluteal Region Cutaneous nerve supply of (Gluteal region) 1. Lateral cutaneous