APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
|
|
|
- Jason Robinson
- 6 years ago
- Views:
Transcription
1 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy
2 Objectives Review current literature related to the management of surgical and non-surgical hip pathologies Discuss the concept of the movement system Recognize key examination findings to support common movement system diagnoses for the hip Discuss interventions guided by the specific movement system diagnosis
3 Literature Review Cheatham, Enseki, & Kolber (2015) Yuan, Sierra, &Trousdale (2008) Mechanism of impingement, chronic impingement can stimulate excessive bone growth The goal of treatment in symptomatic patients with femoral-acetabular impingement is the restoration of the anatomy to as close to normal as possible while removing factors contributing to abutment of the femoral head and/or neck and the acetabular rim. p. 891

4 Chattle (2012) Surgery often opted for early due to restricted activity concerns
5
6 Short, Short, Strack, Anloague, & Brewster (2017) Article attached Dressendorfer & Callanen (2017) Article attached
7 Movement System Model The "movement system" represents the collection of systems (cardiovascular, pulmonary, endocrine, integumentary, nervous, and musculoskeletal) that interact to move the body or its component parts.
8 One Joint vs. Multi Joint Muscles Hip extensors Hip flexors
9 Standing Tests Posture Partial squat Single leg stance
10 Supine Tests Hip flexor length test Straight leg raise Iliopsoas muscle performance Single knee to chest
11 Side-lying Tests Hip abductor muscle performance
12 Prone Tests Knee flexion Hip medial and lateral rotation
13 Quadruped Alignment Quadruped rocking
14 Sitting Tests Knee extension Hip flexion Hip medial and lateral rotation
15 Gait Stance phase Swing phase
16 Movement System Diagnoses Syndrome Accessory Movement Associated Diagnoses Femoral anterior glide Hip adduction Femoral accessory hypermobility Without rotation With medial rotation With lateral rotation Without rotation With medial rotation Femoral hypomobility With superior glide DJD Iliopsoas tendinopathy; bursitis Adductor strain Gluteus medius strain, trochanteric bursitis, piriformis syndrome Early DJD, labral tears
17 Femoral Anterior Glide Syndrome with Medial Rotation Pathomechanics Inadequate posterior glide of the femoral head during hip flexion Medial femoral rotation during hip flexion
18 Symptoms Groin pain, particularly during hip flexion Iliopsoas tendinopathy Associated with activities involving hip extension (distance running, dancing, postural hip extension)
19 Key Examination Items Movement Patterns Supine hip flexion with knee extension evaluate passively and actively, femoral head will have insufficient posterior glide and associated medial rotation Prone hip extension excessive anterior translation of femur Quadruped rocking patient will prefer hips flexed to less than 90 degrees, affected hip will not flex as easily and ipsilateral pelvis will appear higher Seated knee extension active knee extension will be associated with medial rotation
20 Muscle Length and Recruitment Shortened and dominant TFL relative to iliopsoas Single leg stance associated with medial rotation Prone hip extension hamstring dominance Seated active knee extension increased motion when allowed to medially rotate
21 Intervention Goals Improve posterior femoral glide Strengthen the iliopsoas to counteract TFL dominance Correct hip hyperextension and medial rotation during postures and movements
22 Interventions Quadruped rocking Supine passive hip flexion Prone knee flexion Side lying gluteus medius strengthening Seated end-range iliopsoas strengthening Single leg stance
23 Postural and Movement Corrections Sit to stand practice performing without medial hip rotation or adduction Avoid sitting with legs crossed thigh over thigh Correct sway back posture Use a pillow between knees in side-lying Engage gluteus maximus at heel strike
24 Femoral Accessory Motion Hypermobility Pathomechanics Found in patients with early DJD and labral tears Rotational impairments associated with superior glide of the femur Pain results from compressive forces Distraction of femur alleviates pain
25 Symptoms Deep hip joint pain may radiate anteromedially Pain with walking Stiffness upon initial walking
26 Key Examination Items Movement Patterns Gait analysis mildly antalgic gait Single leg stance medial femoral rotation Prone passive knee flexion lateral femoral rotation Seated knee extension medial and possibly superior femoral movement
27 Muscle Length and Recruitment Rectus femoris and hamstrings stiff relative to the iliopsoas and intrinsic hip rotators Hamstring dominance during hip extension Gluteus medius and iliopsoas weakness
28 Intervention Goals Reduce hypermobility of accessory motions Improve quadriceps and hamstring flexibility
29 Interventions Quadruped rocking Prone knee flexion Side-lying hip abduction Seated knee extension
30 Postural and Movement Corrections Teach patient to monitor femoral movement Eliminate strength training of quadriceps and hamstrings Taping the proximal femur
31 Femoral Hypomobility with Superior Glide Pathomechanics Associated with DJD Marked limitation in both passive and active motion
32 Symptoms Deep joint pain with referral along medial and anterior thigh Joint stiffness Night pain
33 Key Exam Items Movement Patterns AROM and PROM Hip flexor length Gait assessment compensatory lumbar/pelvic motion due to restricted hip mobility, antalgic gait
34 Muscle Length and Recruitment Hip flexor dominance and stiffness Hip abductor/extensor weakness Joint hypomobility
35 Intervention Goals Maintaining maximum active and passive motion
36 Interventions Caudal long-axis distraction Standing exercises combined with distraction Hip flexor stretching Quadruped rocking Prone series knee flexion, hip lateral rotation with knee flexion, hip abduction Lower abdominal strengthening
37 Postural and Movement Corrections Focus on decreasing lumbar lordosis in standing Contract gluteus muscles at heel strike Teach knee flexion over compensatory lumbar motion in presence of hip flexor contracture Encourage sitting in less hip flexion Minimize active hip flexion during sit to stand
38 Hip Adduction with Medial Rotation Pathomechanics Lengthened posterior gluteus medius and hip lateral rotators with or without associated weakness Imbalance between flexors/medial rotators and extensors/lateral rotators Risk factors include wide pelvis, side sleeping, crossing legs, running, or cycling
39 Symptoms Pain in area of gluteus medius Trochanteric bursitis, ITB pain Piriformis syndrome May mimic L4-5 radiculopathy or peroneal nerve entrapment
40 Key Exam Items Movement Patterns Tenderness and nodules along ITB Pain reproduced by ITB stretching Extensor/lateral rotator weakness
41 Single-leg stance Trendelenburg Gait assessment
42 Muscle Length and Recruitment Increase flexibility/length of lateral rotators Hip adductors dominate May recruit sartorius or TFL to abduct
43 Intervention Goals Improve performance of the hip abductor and lateral rotator muscles
44 Interventions Use of assistive device if walking is painful and significant abductor weakness is present Prone hip abduction strengthening isometric hip lateral rotation, AROM hip abduction Side-lying exercises
45 Postural and Movement Corrections Stand with symmetrical weight bearing avoiding hip adduction Avoid crossing legs and minimize time in sitting Minimize hip adduction during sit to stand Use pillow between knees in side-lying Consider use of assistive device
46 References Yuan B, Sierra R, Trousdale R. Femoralacetabular impingement. Orthopedics. 2008;31(9), Chattle R. Amongst patients with femoral acetabular impingement does hip arthroscopy improve symptoms and functional outcomes when compared to other treatment options? A literature review of FAI And hip arthroscopy. SportEx Medicine. 2012;53(July), 7-13.
47 Short S, Short G, Strack D, Anloague P, Brewster B. A combined treatment approach emphasizing impairment-based manual therapy and exercise for hip-related compensatory injury in elite athletes: A case series. The International Journal of Sports Physical Therapy. 2017;12(6),
48 Cheatham S, Enseki K, Kolber M. Postoperative rehabilitation after hip arthroscopy: A search for the evidence. Journal of Sport Rehabilitation. 2015; 24, Dressendorfer R, Callanen A. Hip labral tears clinical review. Cinahl Information Systems. September 22, 2017.
49 Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes. St. Louis, MO: Mosby, Inc.; 2002.
Evaluation of the Hip
 Evaluation of the Hip Adam Lewno, DO PCSM Fellow, University of Michigan Primary Care Sports Update 2017 Disclosures Financial: None Images: I would like to acknowledge the work of the original owners
Evaluation of the Hip Adam Lewno, DO PCSM Fellow, University of Michigan Primary Care Sports Update 2017 Disclosures Financial: None Images: I would like to acknowledge the work of the original owners
HIP_CASE 2_OA. Hip Forces. Function of the Hip. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1
 HIP_CASE 2_OA Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT, OCS, FAAOMPT 62 yo female AM stiffness Hip pain diffuse, variable ant>lateral>post Gradual onset Tennis
HIP_CASE 2_OA Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT, OCS, FAAOMPT 62 yo female AM stiffness Hip pain diffuse, variable ant>lateral>post Gradual onset Tennis
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
APTA Intro to Identity. The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee THE HUMAN MOVEMENT SYSTEM
 The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
Hip pain: A comparison of Osteoarthritis and Femoroacetabular Impingement Kristine Flais, PT, DPT
 Hip pain: A comparison of Osteoarthritis and Femoroacetabular Impingement Kristine Flais, PT, DPT Most common cause of hip pain in older adults Prevalence of Hip OA Age Gender Race Developmental disorders
Hip pain: A comparison of Osteoarthritis and Femoroacetabular Impingement Kristine Flais, PT, DPT Most common cause of hip pain in older adults Prevalence of Hip OA Age Gender Race Developmental disorders
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies
 Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
Alejandro Verdugo, M.D.
 Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Bryan T. Kelly, MD Center for Hip Pain and Preservation Hospital for Special Surgery
 Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Functional Movement Screen (Cook, 2001)
") Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Total Hip Replacement Rehabilitation: Progression and Restrictions
 Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component. Limited external rotation to 20 degrees (2 weeks)
") General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement. Normalize gait pattern with brace (if indicated) and crutches
 and crutches") General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report
 58 Case Report A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report Jun-hyeok Jang, Ph.D., PT, Professor 1 ; In-cheol Jeon,
58 Case Report A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report Jun-hyeok Jang, Ph.D., PT, Professor 1 ; In-cheol Jeon,
Main Menu. Joint and Pelvic Girdle click here. The Power is in Your Hands
 1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
1 Hip Joint and Pelvic Girdle click here Main Menu K.6 http://www.handsonlineeducation.com/classes//k6entry.htm[3/23/18, 2:01:12 PM] Hip Joint (acetabular femoral) Relatively stable due to : Bony architecture
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Travis G. Maak, MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Overview. Overview. Introduction. Introduction Anatomy History Examination Common Disorders. Introduction Anatomy History Examination Common Disorders
 Common Hip Disorders in Figure Skaters 14 th Annual Meeting of Sports Medicine and Science in Figure Skating January 25, 2009 8:15-8:45am Robert J. Dimeff, MD Medical Director of Sports Medicine Overview
Common Hip Disorders in Figure Skaters 14 th Annual Meeting of Sports Medicine and Science in Figure Skating January 25, 2009 8:15-8:45am Robert J. Dimeff, MD Medical Director of Sports Medicine Overview
Internal Rotation (turning toes/knee toward other leg) 30 degree limit. limit
 30 degree limit. limit") Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ACUTE PROXIMAL HAMSTRING TENDON REPAIR BENJAMIN J. DAVIS, MD
 Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
WHEN THE HIP IS NOT THE HIP
 WHEN THE HIP IS NOT THE HIP M Cusí MBBS, FACSP, FFSEM (UK) Conditions that can be confused with hip pain 1. Referred pain lumbar spine Conditions that can be confused with hip pain 1. Referred pain lumbar
WHEN THE HIP IS NOT THE HIP M Cusí MBBS, FACSP, FFSEM (UK) Conditions that can be confused with hip pain 1. Referred pain lumbar spine Conditions that can be confused with hip pain 1. Referred pain lumbar
Precautions following Hip Arthroscopy/FAI: (Refixation/Osteochondroplasty)
") Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
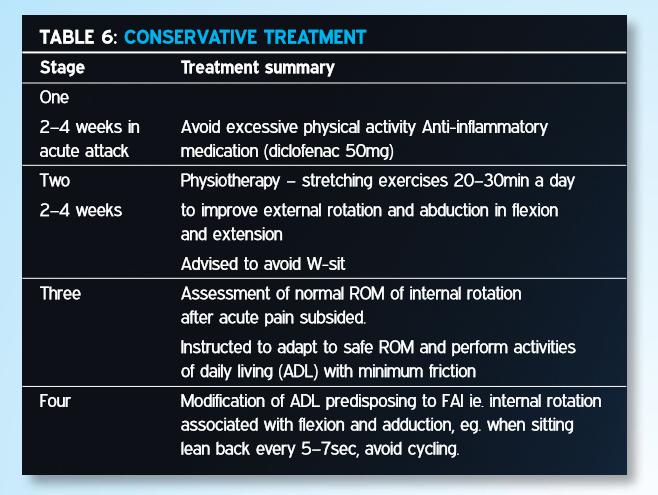
CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT
 SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
NETWORK FITNESS FACTS THE PELVIS
 NETWORK FITNESS FACTS THE PELVIS The Pelvis The pelvis has 3 joints connecting it together 2 sacro-iliac joints at the back (posterior) and the pubic symphysis joint which is at the front (anterior). A
NETWORK FITNESS FACTS THE PELVIS The Pelvis The pelvis has 3 joints connecting it together 2 sacro-iliac joints at the back (posterior) and the pubic symphysis joint which is at the front (anterior). A
Hip Arthroscopy Rehabilitation Protocol
 Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Human anatomy reference:
 Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Hip Arthroscopy Labral Repair Protocol
 Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Movement System Diagnoses. Movement System Impairment Syndromes of the Lumbar Spine. MSI Syndrome - Assumptions. Return From Forward Bending
 Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty. Faculty Disclosures. Objectives 11/17/2017
 Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking
 1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
Post Operative Total Hip Replacement Protocol Brian J. White, MD
 Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer. Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
BENJAMIN G. DOMB, MD
 Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Rehabilitation Considerations Following Surgical Arthroscopy of the Hip. Joy Anderson PT, ATC, CSCS
 Rehabilitation Considerations Following Surgical Arthroscopy of the Hip Joy Anderson PT, ATC, CSCS 1 Best Rehab Program? Review of the Evidence paucity of evidence surrounding post-operative rehabilitation
Rehabilitation Considerations Following Surgical Arthroscopy of the Hip Joy Anderson PT, ATC, CSCS 1 Best Rehab Program? Review of the Evidence paucity of evidence surrounding post-operative rehabilitation
DR. (PROF.) ANIL ARORA MS
 ANIL ARORA MS") Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Hip Examination DR. (PROF.) ANIL ARORA MS (Ortho) DNB (Ortho) Dip SIROT (USA) FAPOA (Korea), FIGOF (Germany), FJOA (Japan) Commonwealth Fellow Joint Replacement (Royal National Orthopaedic Hospital, London,
Pilates for the Endurance Runner With Special Focus on the Hip Joint
 Pilates for the Endurance Runner With Special Focus on the Hip Joint Kellie McGeoy April 11 th, 2014 Aptos, CA 2013 1 Abstract: Endurance running is defined as any distance over 5 kilometers (3.1 miles)
Pilates for the Endurance Runner With Special Focus on the Hip Joint Kellie McGeoy April 11 th, 2014 Aptos, CA 2013 1 Abstract: Endurance running is defined as any distance over 5 kilometers (3.1 miles)
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Evaluation of Posterior Hip Pain
 Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
7/14/18 OBJECTIVE WHAT IS LOWER CROSSED SYNDROME?
 LOWER CROSSED SYNDROME: A DIFFERENTIAL DIAGNOSIS FOR LOW BACK PAIN Kimberly Hansen ATC, LAT, CES Industrial Sports Medicine Professional with InSite Health Committee on Practice Advancement District 7
LOWER CROSSED SYNDROME: A DIFFERENTIAL DIAGNOSIS FOR LOW BACK PAIN Kimberly Hansen ATC, LAT, CES Industrial Sports Medicine Professional with InSite Health Committee on Practice Advancement District 7
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
CAPPAGH NATIONAL ORTHOPAEDIC HOSPITAL, FINGLAS, DUBLIN 11. The Sisters of Mercy. Hip Arthroscopy
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
Hip Conditioning Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER. Planes of Lumbar Pelvic Femoral (Back, Pelvic, Hip) Muscle Function
 Muscle Function") BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER Functional performance of the soccer player reflects functional capability of certain specific muscle and muscle groups of the back, pelvis and hip to work
BIOMECHANICAL INFLUENCES ON THE SOCCER PLAYER Functional performance of the soccer player reflects functional capability of certain specific muscle and muscle groups of the back, pelvis and hip to work
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component. Normalize gait pattern with brace and crutches
 Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair
 Repair") UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
7) True/False: Rigid motor strategies are the most effective way to handle high forces
 True/False: Rigid motor strategies are the most effective way to handle high forces") The Sacro-Iliac Joint 1) Which of the following make up part of the SIJ provocative physical examination? A. Gaenslen s, FABERS, stork, joint distraction B. Fortin finger test, joint compression, thigh
The Sacro-Iliac Joint 1) Which of the following make up part of the SIJ provocative physical examination? A. Gaenslen s, FABERS, stork, joint distraction B. Fortin finger test, joint compression, thigh
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals Precautions:
: Goals Precautions:") Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
DISTANCE RUNNER MECHANICS AMY BEGLEY
 DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
Young Adult Hip problems. Aresh Hashemi-Nejad FRCS(Orth)
") Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Hip Arthroscopy Protocol
 The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Exercises to Correct Muscular Imbalances. presented by: Darrell Barnes, LAT, ATC, CSCS
 Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Active-Assisted Stretches
 1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
1 Active-Assisted Stretches Adequate flexibility is fundamental to a functional musculoskeletal system which represents the foundation of movement efficiency. Therefore a commitment toward appropriate
The Hip Joint. Exercises and Injuries
 The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
The Hip Joint Exercises and Injuries Pelvis Abnormalities To appreciate the abnormalities that may occur, picture a box around the pelvis. The two most common situations are: 1.the pelvis is tilted forward
Rehabilitation. Friday, October 14, :00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA
 Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
What s Hip: Common Hip Problems and Kids and Adults
 What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip
 Of The Hip") UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket formed by
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket formed by
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Presentation Overview 8/8/12. Muscle Imbalances Revealed Assessment & Exercise for Personal Training
 Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Role Of The Fitness Professional. Causes of Fitness Related Injuries. The Assessments. Screening & Assessing: A Holistic Approach 2/9/2016
 Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
Screening & Assessing: A Holistic Approach Role Of The Fitness Professional Fitness professionals must assess clientele, but need to understand the difference between medical diagnosis vs fitness limitations.
JOHN M. REDMOND, M.D.
 Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Test-retest. The therapist can perform test: retest procedures throughout the treatment session as required.
 HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
A patient guide to Hip Impingement Non-Surgical Management. Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy
 A patient guide to Hip Impingement Non-Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Contents Page: 1 Cover 2 Contents 3 Hip impingement information 4 Conservative rehabilitation
A patient guide to Hip Impingement Non-Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Contents Page: 1 Cover 2 Contents 3 Hip impingement information 4 Conservative rehabilitation
Evaluating the Athlete Questionnaire
 Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Direct Anterior Total Hip Replacement Rehabilitation Program
 Direct Anterior Total Hip Replacement Rehabilitation Program The rehabilitation protocol following Direct Anterior Total Hip Replacement is an integral part of the recovery process. This document includes
Direct Anterior Total Hip Replacement Rehabilitation Program The rehabilitation protocol following Direct Anterior Total Hip Replacement is an integral part of the recovery process. This document includes
EXAMINATION OF HIP. A. Inspection Examination
 EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
EXAMINATION OF HIP History: What is your trouble? Pain, stiffness, limp Please tell me more about your problem?.listen Listen for at least one minute: Let patient do the talking Do not ask leading question
Hip Pain in the Athlete: A Diagnostic Challenge
 : A Diagnostic Challenge Matthew Gimre MD Sports Medicine 11 th Annual Sports Medicine Conference Presented June 17, 2017 on: Month day, Year Presented to: Insert relevant presenter information Calibri
: A Diagnostic Challenge Matthew Gimre MD Sports Medicine 11 th Annual Sports Medicine Conference Presented June 17, 2017 on: Month day, Year Presented to: Insert relevant presenter information Calibri
Initial Exercises (Weeks 1-3)
") Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Muscles of the Gluteal Region
 Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK. LPHC Homework Presented by Dr. Bruce Costello
 How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK LPHC Homework Presented by Dr. Bruce Costello Spinal Mobilization Reaching for the Stars Side-Bend Modified Karate Punch Session Objectives
How to GET RESULTS BETWEEN SESSIONS LumboPelvic Hip Complex HOMEWORK LPHC Homework Presented by Dr. Bruce Costello Spinal Mobilization Reaching for the Stars Side-Bend Modified Karate Punch Session Objectives
Hip Region. PHTY2020: Lecture
 Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
Knee Conditioning Program
 Knee Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Knee Conditioning Program Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Hip Arthroscopy Rehabilitation Protocol
 Hip Arthroscopy Rehabilitation Protocol This protocol is a generic outline of the postoperative management for patients undergoing hip arthroscopy. Depending on the exact diagnosis and the procedures performed,
Hip Arthroscopy Rehabilitation Protocol This protocol is a generic outline of the postoperative management for patients undergoing hip arthroscopy. Depending on the exact diagnosis and the procedures performed,
Knee Capsular Disorder. ICD-9-CM: Stiffness in joint of lower leg, not elsewhere classified
 1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
HOME EXERCISE PROGRAM FOR HIP CONDITIONING
 Exercise Program for: Prepared by: Seasons Family Medicine 37 South 2nd East Rexburg ID, 83440 (208) 356-9231 HOME EXERCISE PROGRAM FOR HIP CONDITIONING The stretching exercises below may be done in addition
Exercise Program for: Prepared by: Seasons Family Medicine 37 South 2nd East Rexburg ID, 83440 (208) 356-9231 HOME EXERCISE PROGRAM FOR HIP CONDITIONING The stretching exercises below may be done in addition
Femoroacetabular Impingement in the Throwing Athlete. Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute
 Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
Hip Arthroscopy. Labral Repair/Debridement with Femoroplasty
 Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Knee Conditioning Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Assessment of Lower Extremity Posture: Qualitative and Quantitative Clinical Skills
 CLINICAL EVALUATION & TESTING Darin A. Padua. PhD, ATC, Column Editor Assessment of Lower Extremity Posture: Qualitative and Quantitative Clinical Skills Marjorie A. King, PhD. ATC, PT Plymouth State University
CLINICAL EVALUATION & TESTING Darin A. Padua. PhD, ATC, Column Editor Assessment of Lower Extremity Posture: Qualitative and Quantitative Clinical Skills Marjorie A. King, PhD. ATC, PT Plymouth State University
BENJAMIN G. DOMB, M.D.
 Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Foot and Ankle Physical Exam. The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers
 Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Stretching Exercises for the Lower Body
 Stretching Exercises for the Lower Body Leg Muscles The leg has many muscles that allow us to walk, jump, run, and move. The main muscle groups are: Remember to: Warm-up your muscles first before stretching
Stretching Exercises for the Lower Body Leg Muscles The leg has many muscles that allow us to walk, jump, run, and move. The main muscle groups are: Remember to: Warm-up your muscles first before stretching