Neurologic Localization for M3s. Kevin Chan Teo Ting Wei Edited from Dr Eugene Gan s slides (Batch of 2016)
|
|
|
- Solomon Morris
- 5 years ago
- Views:
Transcription
1 Neurologic Localization for M3s Kevin Chan Teo Ting Wei Edited from Dr Eugene Gan s slides (Batch of 2016)
2 #1: Where is the lesion?
3 Where Upper/ Lower Symmetrical/ Asymmetrical Unilateral/ Bilateral Sensory Hallmarks Cortex Subcortical Brainstem Spinal Cord Anterior Horn Cell Plexus, Roots Peripheral nerves NMJ Muscles
4 Where Upper/ Lower Symmetrical/ Asymmetrical Unilateral/ Bilateral Sensory Hallmarks Cortex Upper Asymmetrical Unilateral +/- Crossed Cortical Signs Subcortical Upper Asymmetrical Unilateral +/- Lacunar Syndromes Brainstem Upper Asymmetrical Unilateral +/- Crossed Hemiparesis Spinal Cord Upper Symmetrical Bilateral - (SS lvl) Anterior Horn Cell Plexus, Roots Peripheral nerves Mixed Symmetrical Bilateral/ Unilateral Cord syndromes, ARU + Fasciculations, CNs affected Lower Asymmetrical Unilateral - Dependent on levels affected Lower Symmetrical Bilateral +/- Length-dep distal weakness NMJ Lower Symmetrical Bilateral + Prox weakness, fluctuating fatig Muscles Lower Symmetrical Bilateral + Prox weakness, check CN
5
6
7
8
9
10
11
12
13
14
15
16
17


18
19 General Inspection (chronicity) UMN lesion LMN lesion Mixed lesion Minimal wasting, unless chronic Wasting, contractures Tone /- Reflexes /- Wasting, contractures, fasciculations Plantars Power Up-going plantars Clonus UL: flexors > extensors LL: extensors > flexors Down-going plantars +/- Dependent on site of lesion Globally reduced
20 #2: What is the etiology?
21 Differential Diagnoses (supporting risk factors) Sudden onset Vascular (stroke) Trauma Epilepsy (Todd s paralysis) Subacute onset Infection (TB abscess, meningitis) Inflammation (lupus, MS) Gradual onset Degeneration (PD) Demyelination (MS) SOL (hydrocephalus, neoplasm) Variable onset Metabolic (hypoglycemia great mimicker of neuro conditions) Toxic/paraneoplastic
22 Now, back to basics
23 Reflexes 1. Afferent (Sensory) 2. Efferent (AHC + Peripheral nerve) 3. Modulation (UMN)
24 Examples of Reflex Arcs Spinal -Biceps & Brachioradialis (C5-6) -Triceps (C7-8) -Hoffman s (C8) -Cremasteric Reflex (L1) -Knee Jerk (L3-4) -Babinski, Ankle Jerk (S1) -Anal Sphinctor Tone (S2-S4) Cranial -Pupilliary Light Reflex (CN II-III) -Corneal Reflex (CN V1 VII) -Jaw Jerk Reflex (CN V3 V3) -Gag Reflex (CN IX-X)
25 Teaching points about reflexes 1)An hyper-reflexic jerk (Nuclear) should prompt you to think upwards (Supra-nuclear) 2) A hypo-reflexic jerk should prompt you to think of - Afferent - Efferent
26 The neuro limbs exam 1. Inspection 2. Tone Hyper Normal Hypo 3. Reflexes Hyper Normal Hypo/Absent 4. Power Proximal vs Distal vs Other patterns 5. Sensation Pattern of loss (Glove and stocking vs Dermatomal vs Nerve Distribution) Modalities lost Pain + Temperature Fine Touch + Vibration 6. Cerebellar Involved/uninvolved
27 Important features of weakness 1. UMN vs LMN UMN: Spinal cord and above LMN: AHC and below 2. Proximal vs Distal Proximal: Myopathy, NMJ or MND Distal: Wide range of differentials. MND and myotonia dystrophica may present with distal weakness. 3. Unilateral vs Bilateral Unilateral: Peripheral nerve/plexus compression, spinal cord, strokes Bilateral: Myopathies, NMJ, MND, Cord syndromes, Cord transections 4. Sensory involvement If sensory involved, unlikely to be myopathy/nmj Glove and stocking: Peripheral neuropathy, cervical myelopathy Peripheral nerve distribution: nerve compression, mononeuropathy, mononeuritis multiplex Dermatomal: Radiculopathy 5. Specific distinguishing features Muscular pain/skin involvement points to myositis Fatigability and ocular involvement suggests MG 6. Misc. GBS can present with almost any pattern of LMN weakness, with or without sensory involvement
28 Weakness Bilateral upper motor neuron weakness with sensory level at L2 With a history of RTA? With signs of raised ICP? In an immunocompromised patient with fever? In a known cancer patient with back pain?
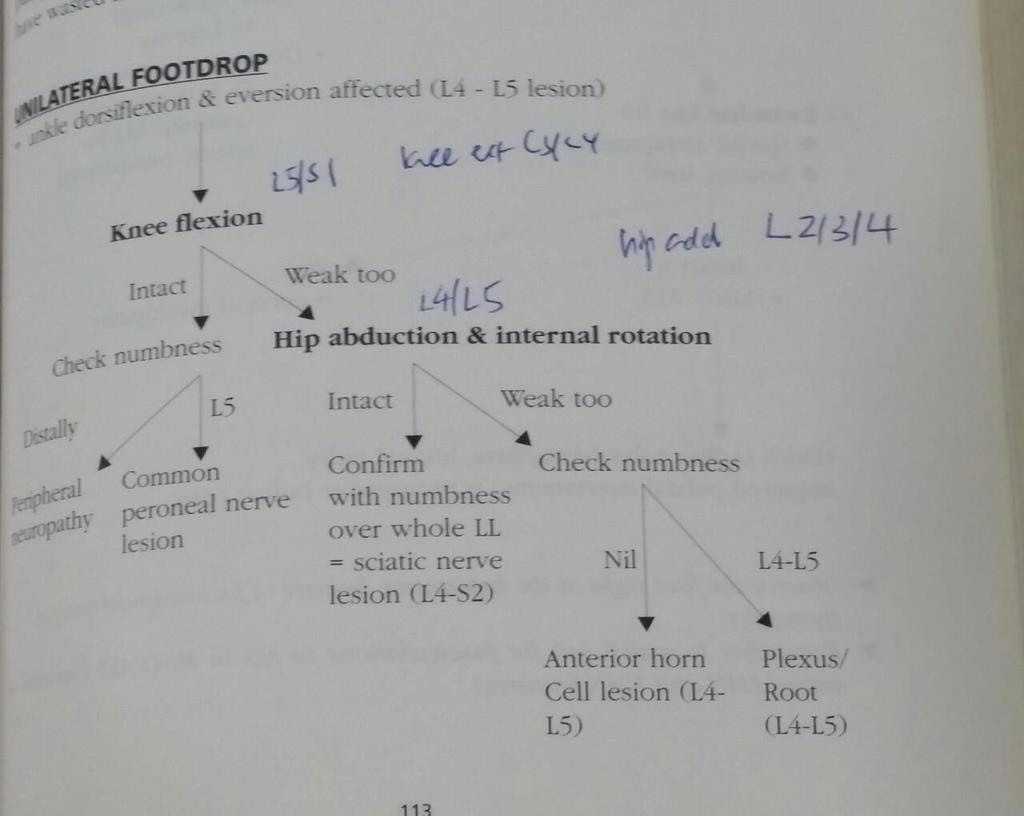
29 Weakness Weakness of left lower limb, power 5/5 on hip flexion and extension. Power 5/5 on knee flexion and extension. Power 3/5 on ankle dorsiflexion and 5/5 on plantarflexion. Knee jerk reflex 2+, ankle jerk 2+, plantar reflex downgoing. Sensory loss of pain and temperature to lateral aspect of leg and dorsum of foot Translation: Unilateral distal weakness with sensory loss Upper limb examination normal Likely levels Peripheral Nerve Common peroneal nerve Radiculopathy L4-L5 Plexus? How to differentiate? Hip Abduction
30
31 Weakness Weakness of both lower limbs, power 3/5 on hip flexion and extension. Power 3/5 on knee flexion and extension. Power 4+/5 on ankle dorsiflexion and plantarflexion. Knee jerk reflex 1+, ankle jerk 2+, plantar reflex downgoing. No sensory loss of pain/temperature or vibration/proprioception Translation: Bilateral proximal weakness with hyporeflexia and no sensory loss (LMN proximal weakness, no sensory involvement) Similar upper limb pattern of weakness Likely levels Muscle NMJ
32 Weakness Bilateral proximal weakness with hyporeflexia and no sensory loss (LMN proximal weakness, no sensory involvement) In a 15 year old boy with a family history? In a 40 year old woman with a rash? In a 65 year old man with diplopia and whose weakness is worse at night? In a 70 year old man taking statins with muscle pain?
33 Weakness Weakness of both lower limbs, power 5/5 on hip flexion and extension. Power 5/5 on knee flexion and extension. Power 4/5 on ankle dorsiflexion and plantarflexion. Power 3+/5 on big toe extension. Knee jerk reflex 1+, ankle jerk 1+, plantar reflex absent. Sensory loss of pain and temperature in dorsal and plantar aspects of the feet. Similar findings in the upper limb Translation: Bilateral distal weakness with hyporeflexia and sensory loss involving both upper and lower limbs (LMN distal weakness with sensory involvment) Likely level Peripheral nerve (peripheral neuropathy)
34 Differentials for peripheral neuropathies Alcohol, AIDP B12 CIDP, carcinoma Diabetes, drugs Familial (HMSN, CMT)
35 The neuro cranial nerves exam 1. Smell 2. Pupils (CN 2 afferent, CN 3 efferent) Big/Small Reactive/Nonreactive 3. Visual Field (Somewhat cortical) Complete monocular blindness Bitemporal hemianopia Homonymous hemianopia (more vs less congruent) Homonymous hemianopia with macular sparing 4. EOMs (CN 3, 4 and 6) Simple vs Complex ophthalmoplegia Medical vs surgical third nerve 5. Sensation (CN V) Intact vs lost 6. Hearing (CN 8) Rinee and Webers 7. Motor (CN V 3, 7, 10, 11, 12) CN 7 UMN vs LMN
36 4 Cranial Nerve Rules 1. All cranial nerves except CN 1 and 2 arise from the brainstem 3, 4 from midbrain 5, 6, 7, 8 from pons 9, 10, 11, 12 from medulla 2. Cranial nerves group at several locations 3. Cranial nerves are in contact with the meninges and skull base CN 6 is particularly affected by meningitis, NPC and raised ICP due to its long intracranial course 4. Cranial nerves behave as peripheral nerves and are thus affected in peripheral neuropathies Most peripheral neuropathies affect limbs, but GBS/MFS can affect cranial nerves first
37 Approach Unilateral vs Bilateral UMN vs LMN 7 Isolated vs group vs random Long tract signs
38 Cranial nerve groups Cavernous sinus: 3, 4, V 1, 6 (sometimes V 2 ) Orbital apex: Cavernous sinus + CN 2 Cerebello-pontine angle: 5, 6, 7, 8 (Vestibular schwannoma/meningiomas) Jugular foramen: 9, 10, 11, 12
39 Cranial Nerve Innervation Besides Facial Nerve (lower half of motor nucleus) and Hypoglossal nerve, all other cranial nerve nuclei have bilateral innervation.
40 DDx for eye movement problems Isolated 3 Medical: Usually DM Surgical: Usually PCA aneurysm Isolated 4 Usually congenital, unmasked when the squint decompensates Isolated 6 Usually DM, but look for skull base, cavernous sinus, meningeal and ICP causes first Complex ophthalmoplegia Consider MG and thyroid eye disease among other ddx
41 Tips CN 3 carries parasympathetic fibres on the outside, leading to a blown pupil when compressed but a normal pupil when ischemic (surgical vs medical 3 rd ) CN 6 has a long intracranial course and is compressed by raised ICP
42 Visual Fields
43 Brainstem rules of 4 4 Medial structures Medial lemniscus (DCML) Motor pathway (pyramidal pathway) Motor nuclei of 3, 4, 6 and 12 Medial Longitduinal Fasciculus (MLF) 4 Side structures Spinothalamic Sensory nucleus of 5 Sympathetic nerves Spinocerebellar tract
44 Misc. Radiation to the neck for NPC is a cause for cranial neuropathies, especially bilateral cranial neuropathies. Consider it when the deficits fit individual nerves but don t localise well anatomically

45 Eye movements

46 Eyes
47 Eyes 6 th nerve palsy Recent onset with early morning headache and vomiting? Tinnitus, sensorineural hearing loss and vertiginous giddiness? With contralateral limb weakness?

48 Eyes
49 Eye Complete left sided eye paralysis (3, 4, 6) with? Failure of depression of right eye With numbness over left side of face? Patient is NPL?


50 Eye
51 Eye 3rd nerve palsy With a longstanding history of DM and a normal pupil? With a blown pupil? With contralateral hemiplegia?
52 Cortical signs Dominant Cortex Language (Aphasia) Apraxia Gerstmann Syndrome (Dominant inferior parietal lobe) Writing (Dysgraphia) Calculation (Dyscalculia) Finger agnosia Left-right disorientation Nondominant Cortex Neglect Dressing (Dressing Apraxia) Construction/Drawing (Constructional Apraxia) Stereognosis Frontal Lobe Personality changes Failure to plan Contralateral gaze preference Primitive reflexes Disinhibition

53 Sensory System
54 Sensory System

55 Sensory System
56 Important features of numbness 1. If there is weakness, approach as a weak patient with sensory symptoms 2. Modalities affected Different modalities between limbs: Brown Sequard Dorsal columnar loss: bear in mind SCDC and syphilis 3. Distribution of loss 4. Symmetry of loss Peripheral neuropathies tend to be more symmetrical
57 Constellations Pattern Distal Nerve distribution Nerve distribution Limbs - Upper Both Ddx 1. Peripheral Neuropathy (Sensory PN, Pure SFSN etc.) 2. Cervical myelopathy 3. SCDC 4. Demyelinating diseases 1. Median/Radial/Ul nar neuropathy 2.? Brachial Plexopathy 1. Mononeuritis multiplex 2. Sensory neuronopathy
58 Constellations Pattern Dermatomal Dermatomal Limbs Upper Lower Ddx 1. Cervical radiculopathy 2. Cervical myelopathy 1. Acute Myelopathies 2. Cord transection/transverse myelitis
59 Case 1 Mr Darren Tan
60 Stem Mr Darren Tan is a 62 year old gentleman who presents with a 3 week history of leg weakness. Please examine the patient s lower limbs.
61 Physical examination: Inspection Patient appears alert and comfortable at rest No signs of muscle wasting, muscle bulk in both legs appears symmetrical No fasciculations
62 Physical examination: Tone Increased tone bilaterally Presence of clonus bilaterally
63 Physical examination: Reflexes Bilateral brisk knee-jerk reflexes Bilateral brisk ankle-jerk reflexes Bilateral upgoing plantar reflexes
64 Physical examination: Power R+L Hip flexion 2/5 R+L Hip extension 2/5 R+L Knee flexion 2/5 R+L Knee extension 2/5 R+L Ankle dorsiflexion 2/5 R+L Ankle plantarflexion 2/5 R+L Big toe extension 2/5 R+L Big toe flexion 2/5
65 Physical examination: Sensation Widespread loss of pin-prick, fine touch and vibration sensation below the hips Loss of proprioception bilaterally
66 Physical Examination: Summary Bilateral increased tone and clonus Bilateral brisk knee-jerk, ankle-jerk reflexes and upgoing plantar reflexes Bilateral weakness of all lower limb muscles with power of 2/5 Bilateral loss of pain, fine touch, vibration and proprioception
67 Gait + UL Examination Unable to ambulate Absence of pronator drift Biceps reflex normal Triceps reflex normal Brachioradialis reflex normal Shoulder abduction 5/5 Finger flexion 5/5 Finger abduction 5/5 Gross sensation intact
68 Where is the lesion? Cortex? Subcortex? Brainstem? Spinal cord? Anterior Horn Cell? Plexus? Peripheral nerves? Neuromuscular junction? Muscles?
69 Spinal Cord!!!!!! Lesion likely between T1 L1 Complete examination by requesting to perform abdominal reflexes, digital rectal examination.
70 Case 2 Mr Ming Shan
71 Stem Mr Ming Shan is a 40 year old male who presents with weakness of the arms. Please examine the patient s upper limbs.
72 Physical examination: Inspection Patient appears alert and comfortable at rest No signs of muscle wasting, muscle bulk in both legs appears symmetrical No fasciculations
73 Physical examination: Tone Pronator drift present Normal tone bilaterally, no spasticity/rigidity
74 Physical examination: Reflexes Biceps reflex normal Triceps reflex normal Brachioradialis reflex normal
75 Physical examination: Power R Shoulder abduction 3/5 L Shoulder abduction 4/5 R+L Shoulder adduction 5/5 R+L Elbow flexion 4/5 R+L Elbow extension 5/5 R+L Wrist flexion 5/5 R+L Wrist extension 5/5 R+L Finger flexion 5/5 R+L Finger abduction 5/5
76 Physical examination: Sensation Normal pin-prick, fine touch, vibration and proprioception sensation
77 Physical Examination: Summary Normal tone, reflexes, sensation R Shoulder abduction 3/5 L Shoulder abduction 4/5 R+L Shoulder adduction 5/5 R+L Elbow flexion 4/5
78 Cerebellar + Cranial Nerve + LL Examination Dysmetria? PEARL Presence of diplopia in all gaze-directions Patient unable to give a wide smile LL reflexes all normal 3/5 weakness in hip flexion, knee extension Gross sensation of LL intact
79 Where is the lesion? Cortex? Subcortex? Brainstem? Spinal cord? Anterior Horn Cell? Plexus? Peripheral nerves? Neuromuscular junction? Muscles?

80

81 Characteristics of MG Weakness in muscles is more marked in the evening. Muscle weakness which increases with exercises and is painless Associated with other autoimmune conditions such as thyrotoxicosis, diabetes mellitus, rheumatoid arthritis etc. Can sometimes be caused by D- penicillamine
82 Unilateral ptosis Myasthenia gravis Horner s syndrome Lung apex (pancoast tumour) Neck (carotid artery dissection) T1 pathology Lateral medullary/pontine syndrome CN III palsy Single nerve lesion Cavernous sinus / superior orbital fissure / orbital apex syndrome Midbrain lesions Myotonic dystrophy Congenital
83 Bilateral ptosis Myasthenia gravis CN III nuclear lesions Myotonic dystrophy Congenital
84 Case 3
85 STEM This is your pediatrics short-case station. Jennifer, 15y/o Chinese adolescent, has had multiple hospital admissions for urinary tract infections. Please perform a neurological examination of her lower limbs.
86 Physical Examination: Inspection Cheerful, alert and comfortable No signs of dysmorphism, appropriate growth No physical abnormalities Left BKA, Right AFO No fasciculations noted Customized motorized wheelchair by bedside
87 Physical Examination: Tone Decreased tone; floppiness
88 Physical Examination: Reflexes Absent knee-jerk reflex Absent ankle-jerk reflex Down-going plantars
89 Physical Examination: Power Bilateral hip extension: 0/5 Bilateral hip flexion: 5/5 Bilateral knee extension: 0/5 Bilateral knee flexion: 0/5 Right ankle dorsiflexion: 0/5 Right ankle plantarflexion: 0/5 Right big toe extension: 0/5 Right big toe flexion: 0/5
90 Physical Examination: Sensation Intact sensation of all modalities when tested over bilateral mid-thighs Loss of sensation of all modalities when tested over bilateral medial knees, right medial malleolus, right interdigital web-space of big and second toe and right lateral sole of foot
91 Physical Examination: Summary Left BKA, Right AFO Decreased tone; floppiness Absent knee-jerk and ankle-jerk reflexes, down-going plantars Bilateral weakness of all LL muscles from knee distally + hip extension with power of 0/5 Bilateral loss of sensation of all modalities from medial knees distally
92 Physical Examination: Back & Abdomen Midline scar Oblique scar along left flank No vertebral abnormalities No pressure sores
93 Physical Examination: Others Upper limbs? Cerebellar examination? Cranial nerves? Head examination? Developmental assessment?
94 Case 4
95 STEM This is your IM short-case station. Mr Chander, 45y/o Chinese, presents to the A&E with complaint of difficulty eating. Please perform a cranial nerve examination.

96
97 Physical Examination: Inspection Alert and comfortable, communicable Vitals stable Presence of left facial droop with loss of left nasolabial fold and smoothening of left forehead creases
98 Physical Examination: CN V, VII, VIII Facial sensation fully intact Inability to raise left eyebrow, inability to bury left eyelashes, drooping of left angle of mouth when asked to smile, asymmetrical appearance when asked to puff up cheeks Hearing intact
99 Physical Examination: CN I, II, III, IV, VI PEARL (direct and consensual) Full extra-ocular movements, no RAPD
100 Physical Examination: CN IX, X, XI, XII No dysarthria/dysphonia, uvula central No tongue deviation Power of SCM and trapezius full
101 Physical Examination: Summary Presence of left facial droop with loss of left nasolabial fold and smoothening of left forehead creases Inability to raise left eyebrow, inability to bury left eyelashes, drooping of left angle of mouth when asked to smile, asymmetrical appearance when asked to puff up cheeks Other CN intact
102 Physical Examination: Others Upper limbs? Lower limbs? Head and neck examination? Acoustic reflex? Taste and oral examination? Assessing complications?
103 Review: Approach to CN palsies CN pathologies can happen in: Isolated Together as a group (rules of 4) No pattern Together with signs in UL and LL
104 Rules of 4 Level of brainstem Midbrain/diencephalon Pons Medulla Cranial nerves I, II, III, IV V, VI, VII, VIII IX, X, XI, XII Cranial nerves involved III, IV, V1, V2 III, IV, V1, VI Pathology/lesion Cavernous Sinus Syndrome Superior Orbital Fissure Syndrome V, VII, VIII, cerebellum Cerebellopontine angle lesion IX, X, XI, XII Lesions in the posterior fossa

105 Review: Approach to CNVII
106 Review: Approach to CNVII Intracranial (intratemporal vs extratemporal) vs extracranial 5 P s (pons, posterior fossa, petrous bone, parotid, peripheries)
107 Case 5
108 STEM This is your IM short-case station. Mr Lim was brought to the A&E by NH staff for?weakness. He has background dementia with BPSD and is uncommunicative. Please perform a neurological examination of his lower limbs
109 Physical Examination: Inspection Resting in bed, comfortable, smiling inappropriately, stable vitals Symmetrical; no fasciculations
110 Physical Examination: Tone Increased tone/rigidity over right lower limb with presence of clonus Normal tone of left lower limb
111 Physical Examination: Reflexes Brisk knee-jerk and ankle-jerk reflexes and upgoing plantars for right lower limb Normal reflexes and down-going plantars for left lower limb
112 Physical Examination: Power Right/left hip extension 3/5; 5/5 Right/left hip flexion 3/5; 5/5 Right/left knee extension 3/5; 5/5 Right/left knee flexion 3/5; 5/5 Right/left ankle dorsiflexion 3/5; 5/5 Right/left ankle plantarflexion 3/5; 5/5 Right/left big toe extension 3/5; 5/5 Right/left big toe flexion 3/5; 5/5
113 Physical Examination: Sensation Intact sensation of all modalities of lower limbs
114 Physical Examination: Cerebellum Heel-shin test positive Patient not keen to ambulate
115 Physical Examination: Summary Increased tone/rigidity over right lower limb with presence of clonus Brisk knee-jerk and ankle-jerk reflexes and upgoing plantars for right lower limb Diminished power of 3/5 of right lower limb Intact sensation of all modalities of both LLs
116 Physical Examination: Others Upper limbs? Cranial nerves? Cardiovascular examination?
117 Discussion What if he presented with headache, nausea and vomiting with weakness? What if he presented with right-sided facial weakness with left-sided hemiparesis? What if he presented with right-sided hemiparesis and expressive aphasia?
118 #1: Where is the lesion?
119 Where Upper/ Lower Symmetrical/ Asymmetrical Unilateral/ Bilateral Sensory Hallmarks Cortex Upper Asymmetrical Unilateral +/- Crossed Cortical Signs Subcortical Upper Asymmetrical Unilateral +/- Lacunar Syndromes Brainstem Upper Asymmetrical Unilateral +/- Crossed Hemiparesis Spinal Cord Upper Symmetrical Bilateral - (SS lvl) Anterior Horn Cell Plexus, Roots Peripheral nerves Mixed Symmetrical Bilateral/ Unilateral Cord syndromes, ARU + Fasciculations, CNs affected Lower Asymmetrical Unilateral - Dependent on levels affected Lower Symmetrical Bilateral +/- Length-dep distal weakness NMJ Lower Symmetrical Bilateral + Prox weakness, fluctuating fatig Muscles Lower Symmetrical Bilateral + Prox weakness, check CN
120 #2: What is the etiology?
121 Differential Diagnoses (supporting risk factors) Sudden onset Vascular (stroke) Trauma Epilepsy (Todd s paralysis) Subacute onset Infection (TB abscess, meningitis) Inflammation (lupus, MS) Gradual onset Degeneration (PD) Demyelination (MS) SOL (hydrocephalus, neoplasm) Variable onset Metabolic (hypoglycemia great mimicker of neuro conditions) Toxic/paraneoplastic
122 #3: What are the complications?
123 Complications Medical Contractures, neuropathic ulcers Complications of prolonged immobilization Functional Body function, activity, participation Social Patient, family, community Psychological Depression, mania Financial
124 Neuro Approaches Approach to weakness/numbness Approach to hemiparesis Approach to spastic/flaccid paraparesis Approach to foot drop Approach to CN lesions Approach to ophthalmoplegia Approach to ptosis Approach to movement disorders

125
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The High-Yield Neurologic Examination
 The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
Year 2 MBChB Clinical Skills Session Examination of the Motor System
 Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Physical Assessment Class 3
 Physical Assessment Class 3 Daily Tasks **Spot Test and assessment 1 (Class materials from1 2)** Goals: Understand significant features of a neurological history Know the complete sequence of cranial nerve
Physical Assessment Class 3 Daily Tasks **Spot Test and assessment 1 (Class materials from1 2)** Goals: Understand significant features of a neurological history Know the complete sequence of cranial nerve
Lecturer. Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014
 Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Examination Approach. Examination Approach. Case 1: Mental Status. The Neurological Exam In the ICU: High Yield Techniques 5/8/2015
 The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
The Neurological Exam In the ICU: High Yield Techniques Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests and techniques S.
Upper and Lower Motoneurons for the Head Objectives
 Upper and Lower Motoneurons for the Head Objectives Know the locations of cranial nerve motor nuclei Describe the effects of motor cranial nerve lesions Describe how the corticobulbar tract innervates
Upper and Lower Motoneurons for the Head Objectives Know the locations of cranial nerve motor nuclei Describe the effects of motor cranial nerve lesions Describe how the corticobulbar tract innervates
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
Neurological Assessment
 Neurological Assessment Name: Age: Gender: Date: History Review of history related to neurological system YES/NO If YES, provide details: General Neurological Mental Illness Neurological disease Severe
Neurological Assessment Name: Age: Gender: Date: History Review of history related to neurological system YES/NO If YES, provide details: General Neurological Mental Illness Neurological disease Severe
5.1 Alex.
 5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
PHYSIOLOGY OF THE BRAIN STEM
 PHYSIOLOGY OF THE BRAIN STEM Dr Syed Shahid Habib Professor & Consultant Clinical Neurophysiology Dept. of Physiology College of Medicine & KKUH King Saud University OBJECTIVES At the end of this lecture
PHYSIOLOGY OF THE BRAIN STEM Dr Syed Shahid Habib Professor & Consultant Clinical Neurophysiology Dept. of Physiology College of Medicine & KKUH King Saud University OBJECTIVES At the end of this lecture
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Course: Physical Assessment II Date: October 17, 2008 Doc: Practice Quiz 1
 Course: Physical Assessment II Date: October 17, 2008 Doc: Practice Quiz 1 This is the practice quiz we did in Class 4. The answers are at the end of the quiz should you wish to test yourself. Complete
Course: Physical Assessment II Date: October 17, 2008 Doc: Practice Quiz 1 This is the practice quiz we did in Class 4. The answers are at the end of the quiz should you wish to test yourself. Complete
Cranial Nerves and Spinal Cord Flashcards
 1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
PERIPHERAL NERVOUS SYSTEM
 CHAPTER 13 PERIPHERAL NERVOUS SYSTEM Functional division of nervous system = afferent info to the CNS ascending spinal cord = efferent info from CNS descending spinal cord somatic skin, muscles visceral
CHAPTER 13 PERIPHERAL NERVOUS SYSTEM Functional division of nervous system = afferent info to the CNS ascending spinal cord = efferent info from CNS descending spinal cord somatic skin, muscles visceral
An Illustrated Guide For Peripheral Nerve Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Neuro Exam Explained
 Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
PHYSIOLOHY OF BRAIN STEM
 PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
GENERAL PRINCIPLES OF NEUROLOGY- John W. Day, M.D., Ph.D.
 I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES
 NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
NEUROLOGY CLERKSHIP CORE CURRICULUM GUIDELINES Endorsed by the following organizations - October 2000: American Academy of Neurology Association of University Professors of Neurology American Neurological
Initial symptom or syndrome: (1) FOCAL WEAKNESS OR NUMBNESS
 FOCAL WEAKNESS OR NUMBNESS") View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
View the referenced DVD patient cases, especially if few hospital or clinic patients are encountered for any one symptom or syndrome. The DVD patient cases are referenced by initial symptom or syndrome
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Lab 16: PNS: Nerves and Autonomic NS Hamilton Answers to Pre- Lab Assignments
 Lab 16: PNS: Nerves and Autonomic NS Hamilton Answers to Pre- Lab Assignments Pre-Lab Activity 1: 1. a. olfactory nerve b. optic nerve c. oculomotor nerve d. abducens nerve e. trochlear nerve f. trigeminal
Lab 16: PNS: Nerves and Autonomic NS Hamilton Answers to Pre- Lab Assignments Pre-Lab Activity 1: 1. a. olfactory nerve b. optic nerve c. oculomotor nerve d. abducens nerve e. trochlear nerve f. trigeminal
Structure, function and assessments of cranial nerves: Part 1 (CN 1-7) MSTN121 - Neurophysiology Session 12 Department of Myotherapy
 MSTN121 - Neurophysiology Session 12 Department of Myotherapy") Structure, function and assessments of cranial nerves: Part 1 (CN 1-7) MSTN121 - Neurophysiology Session 12 Department of Myotherapy Session objectives List the four functions of the cranial nerves (CNs).
Structure, function and assessments of cranial nerves: Part 1 (CN 1-7) MSTN121 - Neurophysiology Session 12 Department of Myotherapy Session objectives List the four functions of the cranial nerves (CNs).
Neurological examinations made easy. Dr. H. A. M. Nazmul Ahasan Professor Department of Medicine Dhaka Medical College Hospital
 Neurological examinations made easy Dr. H. A. M. Nazmul Ahasan Professor Department of Medicine Dhaka Medical College Hospital Introduction The aim of the neurological examination is to delineate the patient
Neurological examinations made easy Dr. H. A. M. Nazmul Ahasan Professor Department of Medicine Dhaka Medical College Hospital Introduction The aim of the neurological examination is to delineate the patient
Neurological Examination
 Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Neurological Assessment. Lecture 8
 Neurological Assessment Lecture 8 Nervous System Central Nervous System Brain Spinal cord Peripheral Nervous System Cranial nerves Spinal nerves Central Nervous System-Brain Central Nervous System-Spinal
Neurological Assessment Lecture 8 Nervous System Central Nervous System Brain Spinal cord Peripheral Nervous System Cranial nerves Spinal nerves Central Nervous System-Brain Central Nervous System-Spinal
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
The Neurological System. Neurological Exam 5 Components. Mental Status Examination
 The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
The Neurological System 1 Neurological Exam 5 Components Mental status Cranial nerves Reflexes Motor- includes Cerebellar function Sensory 2 Mental Status Examination Examination - ABCT Appearance Behavior
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions
 Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
Unit VIII Problem 4 Physiology lab: Brain Stem Lesions - Motor and sensory somatotopy: Pre-central gyrus: is the motor area. Post-central gyrus: is the sensory area. Somatotopy: there is a map of thee
Unit VIII Problem 3 Neuroanatomy: Brain Stem, Cranial Nerves and Scalp
 Unit VIII Problem 3 Neuroanatomy: Brain Stem, Cranial Nerves and Scalp - Brain stem: It is connected to the cerebellum and cerebral hemispheres. Rostral end of brain stem: diencephalon is the area which
Unit VIII Problem 3 Neuroanatomy: Brain Stem, Cranial Nerves and Scalp - Brain stem: It is connected to the cerebellum and cerebral hemispheres. Rostral end of brain stem: diencephalon is the area which
Cancer Rehabilitation New Patient Intake Form
 _ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
_ I. Personal Information Date of Birth Age: Home Address: Home Phone: Cell Phone: Office Phone: Fax: E-Mail: II. Chief Complaint Please describe the major problem that brings you in today: Who referred
THE BRAINSTEM. Raymond S. Price, MD University of Pennsylvania
 THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
THE BRAINSTEM Raymond S. Price, MD University of Pennsylvania Overview of Brainstem Functions The brainstem serves numerous crucial neurologic functions. The most clinically relevant functions include:
Functional components
 Facial Nerve VII cranial nerve Emerges from Pons Two roots Functional components: 1. GSA (general somatic afferent) 2. SA (Somatic afferent) 3. GVE (general visceral efferent) 4. BE (Special visceral/branchial
Facial Nerve VII cranial nerve Emerges from Pons Two roots Functional components: 1. GSA (general somatic afferent) 2. SA (Somatic afferent) 3. GVE (general visceral efferent) 4. BE (Special visceral/branchial
Spinal nerves. Aygul Shafigullina. Department of Morphology and General Pathology
 Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
The Nervous System: Sensory and Motor Tracts of the Spinal Cord
 15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
15 The Nervous System: Sensory and Motor Tracts of the Spinal Cord PowerPoint Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska Introduction Millions of sensory
HEAD AND NECK PART 2
 HEAD AND NECK PART 2 INTEGRATED CURRICULUM = Integrate Basic Science and Clinical Training 1- ENT PATIENT EXAM IN ICS COURSE - Today and next week - Review/Preview Anatomy underlying ENT exam 2- NEUROANATOMY/NEUROLOGY
HEAD AND NECK PART 2 INTEGRATED CURRICULUM = Integrate Basic Science and Clinical Training 1- ENT PATIENT EXAM IN ICS COURSE - Today and next week - Review/Preview Anatomy underlying ENT exam 2- NEUROANATOMY/NEUROLOGY
Neurologic Examination
 John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST
 BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
Differential Diagnosis of Neuropathies and Compression. Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre
 Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Neurological Assessment Part 1
 Neurological Assessment Part 1 MOTOR EXAMINATION: Look at bulk, contour and symmetry of individual muscles: muscles of face upper arm arm thigh lower leg Look for atrophy--may help to localize the site
Neurological Assessment Part 1 MOTOR EXAMINATION: Look at bulk, contour and symmetry of individual muscles: muscles of face upper arm arm thigh lower leg Look for atrophy--may help to localize the site
Cranial Nerve VII & VIII
 Cranial Nerve VII & VIII Lecture Objectives Follow up the course of facial nerve from its point of central connections, exit and down to its target areas. Follow up the central connections of the facial
Cranial Nerve VII & VIII Lecture Objectives Follow up the course of facial nerve from its point of central connections, exit and down to its target areas. Follow up the central connections of the facial
3) Approach to Ataxia - Dr. Zana
 Approach to Ataxia - Dr. Zana") 3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
MOTOR NEURONE DISEASE
 MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7. Some PGY1
 Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Cranial Nerves Exam. 1. To learn how to examine the functions of the 12 pairs of cranial nerves.
 Cranial Nerves Exam [Purpose] 1. To learn how to examine the functions of the 12 pairs of cranial nerves. 2. To understand the function of the 12 pairs of cranial nerves. [Principle] The cranial nerves
Cranial Nerves Exam [Purpose] 1. To learn how to examine the functions of the 12 pairs of cranial nerves. 2. To understand the function of the 12 pairs of cranial nerves. [Principle] The cranial nerves
Anatomy of Nervous System. Neurological Assessment. Brain. Brain. Spinal Cord. Spinal Cord 03/23/2010. Central. Peripheral
 Anatomy of Nervous System Neurological Assessment Central Brain Spinal cord Peripheral Spinal Nerves Brain Cerebral cortex ( rind ) gray matter Frontal Parietal Temporal Occipital Wernicke s area receptive
Anatomy of Nervous System Neurological Assessment Central Brain Spinal cord Peripheral Spinal Nerves Brain Cerebral cortex ( rind ) gray matter Frontal Parietal Temporal Occipital Wernicke s area receptive
By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi
 By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi OBJECTIVES By the end of the lecture, students shouldbe able to: List the nuclei of the deep origin of the trigeminal and facial nerves in the brain
By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi OBJECTIVES By the end of the lecture, students shouldbe able to: List the nuclei of the deep origin of the trigeminal and facial nerves in the brain
e) None of the above e) None of the above
 None of the above e) None of the above") Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Neurology 1) For the management of an acute delirium acquired in the hospital, which one of the following options would be least appropriate? a) Treating the underlying cause b) Promptly increasing antibiotic
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Motor, Reflex, Coordination and Sensory Screening Examination
 Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES
 UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. Vol. 18: Nervous System: Sensory System and Reflexes
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION Vol. 18: Nervous System: Sensory System and Reflexes Your learning objectives for mastering the examination of the sensory system and reflexes are: to assess
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION Vol. 18: Nervous System: Sensory System and Reflexes Your learning objectives for mastering the examination of the sensory system and reflexes are: to assess
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Spinal cord. We have extension of the pia mater below L1-L2 called filum terminale
 Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal:
 Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
Motor tracts Both pyramidal tracts and extrapyramidal both starts from cortex: Area 4 Area 6 Area 312 Pyramidal: mainly from area 4 Extrapyramidal: mainly from area 6 area 6 Premotorarea: uses external
I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts.
 Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
Descending Tracts I: To describe the pyramidal and extrapyramidal tracts. II: To discuss the functions of the descending tracts. III: To define the upper and the lower motor neurons. 1. The corticonuclear
CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST
 CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST Hannah Shinoda, OD Caroline Ooley, OD, FAAO Assistant Professors Pacific University College of Optometry The authors have no financial interest in
CRANIAL NERVE TESTING FOR THE PRIMARY CARE OPTOMETRIST Hannah Shinoda, OD Caroline Ooley, OD, FAAO Assistant Professors Pacific University College of Optometry The authors have no financial interest in
 Spinal Cord Tracts DESCENDING SPINAL TRACTS: Are concerned with somatic motor function, modification of ms. tone, visceral innervation, segmental reflexes. Main tracts arise form cerebral cortex and others
Spinal Cord Tracts DESCENDING SPINAL TRACTS: Are concerned with somatic motor function, modification of ms. tone, visceral innervation, segmental reflexes. Main tracts arise form cerebral cortex and others
NS201C Anatomy 1: Sensory and Motor Systems
 NS201C Anatomy 1: Sensory and Motor Systems 25th January 2017 Peter Ohara Department of Anatomy peter.ohara@ucsf.edu The Subdivisions and Components of the Central Nervous System Axes and Anatomical Planes
NS201C Anatomy 1: Sensory and Motor Systems 25th January 2017 Peter Ohara Department of Anatomy peter.ohara@ucsf.edu The Subdivisions and Components of the Central Nervous System Axes and Anatomical Planes
LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP
 LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP 1 EPISODE IV2012 EYE MOVEMENT LOCALIZATION NEUROLOGY DEPARTMENT of MEDICINE MAHARAT NAKORNRAJSIMA HOSPITAL PAWUT MEKAWICHAI MD 2 ABNORMAL EYE
LOCALIZATION NEUROLOGY EPISODE IV EYE MOVEMENT AND FOOT DROP 1 EPISODE IV2012 EYE MOVEMENT LOCALIZATION NEUROLOGY DEPARTMENT of MEDICINE MAHARAT NAKORNRAJSIMA HOSPITAL PAWUT MEKAWICHAI MD 2 ABNORMAL EYE
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Cranial Nerves. Steven McLoon Department of Neuroscience University of Minnesota
 Cranial Nerves Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Sensory and Motor Systems Sensory Systems:
Cranial Nerves Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Sensory and Motor Systems Sensory Systems:
Neurology. Hollie Wilson
 Neurology Hollie Wilson Objectives Anatomy Physiology: Functional centres of brain UMN lesion vs. LMN lesion Spinal cord Main tracts ascending and descending Nerve roots and peripheral nerves action potentials
Neurology Hollie Wilson Objectives Anatomy Physiology: Functional centres of brain UMN lesion vs. LMN lesion Spinal cord Main tracts ascending and descending Nerve roots and peripheral nerves action potentials
Brainstem. Steven McLoon Department of Neuroscience University of Minnesota
 Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Brainstem Steven McLoon Department of Neuroscience University of Minnesota 1 Course News Change in Lab Sequence Week of Oct 2 Lab 5 Week of Oct 9 Lab 4 2 Goal Today Know the regions of the brainstem. Know
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Arterial Blood Supply
 Arterial Blood Supply Brain is supplied by pairs of internal carotid artery and vertebral artery. The four arteries lie within the subarachnoid space Their branches anastomose on the inferior surface of
Arterial Blood Supply Brain is supplied by pairs of internal carotid artery and vertebral artery. The four arteries lie within the subarachnoid space Their branches anastomose on the inferior surface of
Peripheral Nervous System Dr. Gary Mumaugh
 Peripheral Nervous System Dr. Gary Mumaugh Spinal Nerves Overview Thirty-one pairs of spinal nerves are connected to the spinal cord No special names; numbered by level of vertebral column at which they
Peripheral Nervous System Dr. Gary Mumaugh Spinal Nerves Overview Thirty-one pairs of spinal nerves are connected to the spinal cord No special names; numbered by level of vertebral column at which they
Peripheral Nervous System
 Peripheral Nervous System Sensory Receptors Motor Endings Cranial Nerves The Four Plexuses Extremities Review of Reflexes Fast, preprogrammed, inborn, automatic responses Occur in the CNS at the spinal
Peripheral Nervous System Sensory Receptors Motor Endings Cranial Nerves The Four Plexuses Extremities Review of Reflexes Fast, preprogrammed, inborn, automatic responses Occur in the CNS at the spinal
Doctor Osama Asa ad Khader. Mohammad Alsalem
 6 Doctor 2015 Osama Asa ad Khader Mohammad Alsalem A quick revision for the spinal cord blood supply: Arterial Blood supply of spinal cord The spinal cord got its arterial supply by two ways: Longitudinal
6 Doctor 2015 Osama Asa ad Khader Mohammad Alsalem A quick revision for the spinal cord blood supply: Arterial Blood supply of spinal cord The spinal cord got its arterial supply by two ways: Longitudinal
Name Date Period. Human Reflexes Lab
 Name Date Period Introduction: Human Reflexes Lab Neurons communicate in many ways, but much of what the body must do every day is programmed as reflexes. Reflexes are rapid, predictable, involuntary motor
Name Date Period Introduction: Human Reflexes Lab Neurons communicate in many ways, but much of what the body must do every day is programmed as reflexes. Reflexes are rapid, predictable, involuntary motor
General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways
 General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways Lecture Objectives Describe pathways for general sensations (pain, temperature, touch and proprioception) from the face area.
General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways Lecture Objectives Describe pathways for general sensations (pain, temperature, touch and proprioception) from the face area.
Done By: manar aljebreen Abdulrahman alsharidah
 Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Female Side Male side Done By: manar aljebreen Abdulrahman alsharidah Revised By: Nour Al-Khawajah Mohammed Asiri 2 Slide No.( 1 ) Slide No.( 2 ) 3 Slide No.( 3 ) Slide No.( 4 ) Upper motor neurons are
Sheet lab 3. Page 8B Section1 of medulla at pyramidal {motor} decussation:
 Sheet lab 3 Page 8B Section1 of medulla at pyramidal {motor} decussation: This section is at lower third of medulla and is the most close part to spinal cord and it has some characteristic of spinal cord
Sheet lab 3 Page 8B Section1 of medulla at pyramidal {motor} decussation: This section is at lower third of medulla and is the most close part to spinal cord and it has some characteristic of spinal cord
Arielle Bokhour, class of 2017
 Arielle Bokhour, class of 2017 Objectives 1. Understand the actions and innervation of the extrinsic and intrinsic eye muscles 2. Describe the pathways for pupillary constriction and dilation 3. Understand
Arielle Bokhour, class of 2017 Objectives 1. Understand the actions and innervation of the extrinsic and intrinsic eye muscles 2. Describe the pathways for pupillary constriction and dilation 3. Understand
Internal Organisation of the Brainstem
 Internal Organisation of the Brainstem Major tracts and nuclei of the brainstem (Notes) The brainstem is the major pathway for tracts and houses major nuclei, that contain sensory, motor and autonomics
Internal Organisation of the Brainstem Major tracts and nuclei of the brainstem (Notes) The brainstem is the major pathway for tracts and houses major nuclei, that contain sensory, motor and autonomics
Brain and spinal nerve. By: shirin Kashfi
 Brain and spinal nerve By: shirin Kashfi Nervous system: central nervous system (CNS) peripheral nervous system (PNS) Brain (cranial) nerves Spinal nerves Ganglions (dorsal root ganglions, sympathetic
Brain and spinal nerve By: shirin Kashfi Nervous system: central nervous system (CNS) peripheral nervous system (PNS) Brain (cranial) nerves Spinal nerves Ganglions (dorsal root ganglions, sympathetic
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
THE BACK. Dr. Ali Mohsin. Spinal Cord
 Spinal Cord THE BACK Dr. Ali Mohsin The spinal cord is the elongated caudal part of the CNS. It starts as the inferior continuation of the medulla oblongata at the level of foramen magnum, & ends as an
Spinal Cord THE BACK Dr. Ali Mohsin The spinal cord is the elongated caudal part of the CNS. It starts as the inferior continuation of the medulla oblongata at the level of foramen magnum, & ends as an
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy
 By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
By Dr. Saeed Vohra & Dr. Sanaa Alshaarawy 1 By the end of the lecture, students will be able to : Distinguish the internal structure of the components of the brain stem in different levels and the specific
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES
 INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases
 Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology
 Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of
 Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes
Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes