AMERICAN BOARD OF FOOT AND ANKLE SURGERY
|
|
|
- Erica Stevens
- 6 years ago
- Views:
Transcription


1 Board Certification (October 2017) American Board of Foot and Ankle Surgery AMERICAN BOARD OF FOOT AND ANKLE SURGERY Information and Requirements For Board Certification American Board of Foot and Ankle Surgery 445 Fillmore Street San Francisco, CA (415) This document contains information specific to the 2018 examinations only October 2017
2 Board Certification (October 2017) American Board of Foot and Ankle Surgery Table of Contents The Board Certification Process... 3 What does it mean to be Board Certified?... 3 Board Certification in Foot Surgery... 3 Board Certification in Reconstructive Rearfoot/Ankle (RRA) Surgery... 3 Board Certification is a Two-Part Process... 3 Case Review Podiatry Logging Service (PLS) Case Logging... 3 PLS Checklist Required Procedures Documentation of Facility, Procedures, and Hospital Privileges Case Documentation & Case Review... 6 Case Documentation Instructions... 6 Image Submission Requirements... 7 Computer-based Patient Simulation Examination Register Test Components Instructions and Practice Cases Testing Sites Failure to Appear Scoring Test Results Appeals Confidentiality Calendar Fees Appendix A. List of Categories for Foot Case Review...13 Appendix B. List of Categories for RRA Case Review Appendix C. Table of ABFAS Procedure Categories Appendix D. Uploading Images into PLS...20 Appendix E. Sample Case Documentation Copyright 2017 ABFAS. Any unauthorized use, modification, reproduction, display, publication, performance, or distribution of this work without the prior written consent of ABFAS is prohibited and may violate the Copyright Act, 17 U.S.C. 101 et seq. Such prohibited actions may result in legal action or the loss of privileges, benefits, qualifications, or certifications granted by the ABFAS. Nondiscrimination Policy. In accordance with applicable federal laws, the American Board of Foot and Ankle Surgery does not discriminate in any of its policies, procedures, or practices based on race, color, national origin, sex, sexual orientation, age, or disability. Americans with Disabilities Act. In compliance with the Americans With Disabilities Act, the American Board of Foot and Ankle Surgery will make reasonable accommodations for individuals with disabilities provided the candidate submits a written request and all required documentation no later than thirty (30) days prior to the date(s) of the examination. Candidates will find additional information including how to apply on the ABFAS website. Page 2
3 Board Certification (October 2017) American Board of Foot and Ankle Surgery The Board Certification Process After attaining Board Qualified status, you can begin the Board Certification process. Board Certification must be achieved within 7 years of Board Qualification. What does it mean to be Board Certified? Board Certification in Foot Surgery Board certification in Foot Surgery indicates that you have demonstrated a cognitive knowledge of foot surgery, including the diagnosis of general medical problems and surgical management of pathologic foot conditions, deformities, and/or trauma, and related structures that affect the foot and ankle. Board Certification in Reconstructive Rearfoot/Ankle (RRA) Surgery Board certification in RRA Surgery indicates that you have demonstrated a cognitive knowledge of foot and ankle surgery, including the diagnosis of general medical problems and surgical management of pathologic foot and ankle conditions, deformities, and/or trauma, and related structures that affect the foot, ankle, and leg. Board Certification in Foot Surgery is a prerequisite for Board Certification in RRA. Board Certification is a Two-Part Process There are two parts to the Board Certification process: (1) Case Review and (2) the Computer-based Patient Simulation Board Certification (CBPS) Examination. The Case Review process has four components: (1) PLS case logging, (2) completion of diverse procedures, (3) facility documentation, and (4) case documentation and review. Summary of Changes Those holding ABFAS Board Qualification status are eligible to take the Part II CBPS exam any time after becoming board qualified. They cannot register for Case Review until they have met the procedure diversity requirements (listed below). Case Review Documentation 1. Podiatry Logging Service (PLS) Case Logging Log all post-residency procedures performed in accredited facilities for which you were the surgeon of record, into the Podiatry Logging Service (PLS) for Surgery. ABFAS will request complete documentation for the required number of foot and RRA surgery cases from the PLS log. All surgical procedures must be logged into PLS to obtain ABFAS certification. Procedures you performed during residency are not acceptable for logging in PLS or for case submission. You may log cases performed while in a fellowship program provided you were surgeon of record. ABFAS recommends that you enter into PLS all post-residency surgical procedures that you performed in accredited facilities. The PLS system will inform you when you have met the quantity and diversity requirements, but you must continue logging all cases until you complete the case review application process. If you are certified in Foot Surgery and seeking only RRA certification, you may log only post-residency RRA procedures performed. The PLS system will inform you when you have met the quantity and diversity requirements. ABFAS will lock Page 3
4 Board Certification (October 2017) American Board of Foot and Ankle Surgery cases selected for case review (see below), however please continue logging procedures on PLS until you became board certified. If you do not pass case review, ABFAS will need to select different cases when you reapply. It is therefore necessary that you continue to log all required cases until you pass case review. PLS Checklist Ensure that cases are logged with the correct procedure code in PLS. Note: Failure to correctly log procedure type is a common error. Ensure that you are listed as Surgeon (not Co-surgeon, Assistant Surgeon, or any other designation) on all operative reports and all chart materials for every procedure on the list. Ensure that you are listed as the surgeon of record (not co-surgeon) in the intraoperative anesthesia record or circulating nurse notes. List every procedure performed and documented in the operative report. 2. Required Procedures Candidates must log a minimum of 65 cases in PLS for eligibility to submit cases for review for Foot Surgery certification and/or Reconstructive Rearfoot/Ankle Surgery (RRA) certification (see Appendix C). For Foot Surgery certification, a minimum of 30 cases must include surgery from the First Ray, Other Osseous and Reconstructive Rearfoot/Ankle categories listed in Appendix A. For RRA Surgery certification, a minimum of 30 RRA cases must be logged. Additionally, the RRA cases must include a minimum of 12 procedures from Appendix B. Candidates repeating the Case Review portion of the examination must ensure they have an adequate volume of cases to meet the requirement. Cases selected for Case Review in previous years will not be used for Case Review in subsequent years. RRA procedures consisting of diagnostic operative arthroscopy, subtalar joint arthroereisis, foreign body/hardware removal, or ostectomy are not counted toward the required 30 total. Open management of fractures must include some type of internal or external fixation. Unproven or experimental procedures are not counted toward the required 65 total. Removal of internal or external fixation devices or implants is not counted. Extracorporeal shock wave therapy (ESWT) procedures and application of biological dressings are not acceptable. Required Cases for Access to Board Certification FOOT SURGERY CERTIFICATION 65 First Ray, Other Osseous, RRA Cases a 30 b c RRA SURGERY CERTIFICATION RRA - Elective Osseous RRA - Nonelective Osseous 30 d, e 10 e 2 e a. See Appendix A for more details. b. Of these 30 cases, 27 (90 percent) must have been performed in an accredited healthcare facility. Page 4
5 Board Certification (October 2017) American Board of Foot and Ankle Surgery c. List procedures involving only the hallux as digital procedures. d. All 30 cases must have been performed in an accredited healthcare facility. e. See Appendix B for more details. The procedures within each major category must demonstrate the candidate s range of surgical experience. Inappropriate use or overuse of one procedure type (e.g., chevron bunionectomy) may result in failing scores. Important to know: Follow all instructions carefully to optimize your chances of successfully passing Case Review. Mislogging Mislogging is one of the major reasons why candidates fail case review. Pay close attention to ensure each case is logged accurately. Below is a list of common logging errors that resulted in candidates failing case review: 1) A Lisfranc fracture ORIF or arthrodesis is not considered a rearfoot procedure. A lisfranc fracture ORIF should be logged as 4.13 (Open management of tarsometatarsal fracture/dislocation) and a lisfranc joint arthrodesis is logged as 4.15 (tarsometatarsal fusion). Please note: "Midfoot" joint(s) refers to any joint proximal to, and not including, tarsometatarsal/lisfranc joint. 2) A Lapidus bunionectomy is a first ray procedure and should only be logged as (bunionectomy with first metatarsocuneiform fusion) or (joint salvage with first metatarsocuneiform fusion) or (metatarsocuneiform fusion, other than for hallux valgus or hallux limitus) 3) A Haglund's deformity where the posterior heel exostosis is shaved (without detaching and reattaching a major portion of the Achilles tendon) should be logged as 4.1 (partial ostectomy). Such cases are never used for case review. If logged incorrectly, and the case is pulled for review, a failing score will occur 4) Plastic surgery does not include simple wound debridement and synthetic/biological graft application. A synthetic/biological graft application and/or simple double elliptical lesion excision does not meet the criteria for case review and if submitted will result in a failing score. 5) A Kidner procedure should be logged either as (ligament or tendon augmentation/supplementation/restoration) or 3.1 (excision of ossicle). Removal of any ossicle such as os peroneum, os navicularis, os trigonum should only be logged as 3.1. Do not take the risk and log incorrectly as a simple ossicle removal with/without tendon debridement is not a qualified procedure for case review and will result in a failing score. 6.) If a joint salvage procedure with cheilectomy only is logged as a joint salvage procedure with distal metatarsal osteotomy, the candidate will receive a low or failing score for that case. 7.) Open management of fracture or metatarsophalangeal joint (MTPJ) dislocation cases must include internal or external fixation. 3. Documentation of Facility, Procedures, and Hospital Privileges Facility Verification Letter This is advance notice of a new requirement that will start in September ABFAS will require you to confirm the accreditation status of the facility(ies) in which you performed your cases. ABFAS will notify you of additional details in early Page 5
6 Board Certification (October 2017) American Board of Foot and Ankle Surgery Accredited healthcare facilities include facilities accredited by The Joint Commission, Joint Commission International, the Accreditation Association for Ambulatory Health Care (AAAHC), the American Osteopathic Association (AOA), or the American Association for Accreditation of Ambulatory Surgery Facilities, Inc. (AAAASF). Hospital/Surgery Center Audit ABFAS will select one of the facilities in which you performed surgery to ensure that you have logged all procedures that you performed at that facility into PLS. On December 12, 2017, ABFAS will you detailed instructions on obtaining and submitting the notarized facility letter to verify the list of procedures that you performed at that facility for a given period. You will have until January 5, 2018 to upload the letter into PLS. Verification of Surgical Privileges ABFAS requires official documentation of surgical privileges consistent with the area of certification desired (Foot Surgery and/or RRA). Please submit proof via at privileges@abfas.org, or fax to Do NOT upload proof of surgical privileges into PLS. 4. Case Documentation & Case Review ABFAS will randomly select 13 Foot Surgery and/or 13 RRA cases from your PLS log for detailed documentation of the case. By January 22, 2018, ABFAS will notify you via that the list of selected cases is available on your PLS site. You will then submit complete documentation, including all images, to ABFAS for review no later than March 9, After you submit all required documentation (detailed instructions below), a team of case reviewers (ABFAS board certified foot and ankle surgeons) will evaluate all aspects of the surgical procedures that you submitted. This includes evaluation of preoperative clinical assessment, preoperative radiographic assessment and postoperative care as well as performance of the procedures(s) including technical skills assessment, and outcomes analysis. Case Documentation Instructions ABFAS evaluates and scores all procedures based on materials provided by candidates. Provision of incomplete documentation is a common error that may result in a lower score. All documents must be legible. All typed/handwritten materials must be submitted in PDF format. 1. Podiatric History and Physical (H&P) This is the record of your initial assessment (not that of another physician) when the patient first presented for the condition leading to the surgical procedure performed. Include all pertinent supportive medical assessments generated by another physician. If the records are handwritten, please submit H&P records electronically as both (1) scanned copies of all handwritten material; and (2) typed copies of all handwritten materials. Please convert typed copies to PDF format. Alternatively, you can submit copies of electronic medical records. 2. Operative Report (OP Report) Submit a copy of the typed operative report upon which you are listed as Surgeon (not Co-Surgeon, Assistant Surgeon, or any other designation). Procedures listing more than one surgeon of record are not acceptable. Common error: Another physician listed as surgeon or co-surgeon. Page 6
7 Board Certification (October 2017) American Board of Foot and Ankle Surgery 3. Progress Notes Submit typed progress notes from the time of first presentation for the condition leading to the procedure(s) performed through final outcome. If a patient undergoes multiple procedures on separate dates, all progress notes must be presented, including any notes related to complications, prior surgery, or surgical revisions. For procedures involving hospital admissions of greater than 24 hours, include: Typed copies of progress notes from the first 3 inpatient days Copies of all inpatient progress notes (including those of consultants) Typed versions of all outpatient follow-up visit progress notes through final outcome Submit progress note records electronically converted to PDF format and in chronological order from oldest to most recent. If you performed a surgery on a patient that you saw at a required free clinic/resident clinic/emergency facility, but were unable to follow the patient postoperatively, please address the reason for the inability for follow-up in the progress notes. Note: Preprinted or standardized operative reports with blank spaces filled in or using standardized language from a word processor or computer are not acceptable. ABFAS Policy for Potential Misrepresentation Any incomplete, questionable, modified or falsified case materials submitted 4. Pathology Report may be evaluated further by ABFAS. (Path Report) If case review uncovers any suspicion or evidence of falsified records, including Submit copies of altered labeling of medical imaging studies, if substantiated, this may result in, any pathology at minimum, forfeiture of the right to sit for the examination and all fees paid, report for softtissue lesions, ABFAS may require that you help verify submitted documents. and at maximum, your disqualification for Board Qualification or Certification. infections, and ABFAS reserves the right to pursue further investigation including, but not other limited to, sending an ABFAS-appointed representative to the hospital/surgery procedures for center to further review documentation. which a Failure to comply with the process and/or discovery of falsified records will specimen was result in disqualification and such other action as ABFAS deems appropriate sent because including revocation of Board Qualified status, disqualification for abnormal certification, and forfeiture of fees paid. pathology was present. 5. Laboratory Reports (Labs)/Diagnostic Reports Submit copies of any relevant report of preoperative tests ordered, including laboratory studies, MRI, nuclear medicine, electrodiagnostic studies, etc. 6. Intraoperative Anesthesia Record/Circulating Nurse s Notes Submit copies of the intraoperative anesthesia record or circulating nurse s notes from the facility listing the candidate as the surgeon of record (not the anesthesiology consultation notes). Appendix E provides examples of proper documentation Page 7
8 Board Certification (October 2017) American Board of Foot and Ankle Surgery Image Submission Requirements General Requirements The following general requirements apply to every image presented as part of complete case documentation. Noncompliance with image requirements and instructions may result in rejection of case documentation, with no opportunity to resubmit missing materials. Appendix D provides further information 1. JPG Format Submit all images, regardless of original format, in JPG, JPEG or PNG format. ABFAS reserves the right to examine, on site, images stored on the imaging equipment hard drive to determine that submitted images have not been altered. If it is determined that images have been altered, you will forfeit, at minimum, the right to sit for the examination and all fees paid. 2. Image Clarity All images must be clearly readable. Ensure that that the reviewer will be able to clearly identify all pathology, fixation, and bone healing within the image. Note: Unreadable images may lead to rejection of procedures and/or failing the case. 3. Three Views For MRIs and computerized tomographic (CT) images, submit individual images of a minimum of three views (see below) clearly demonstrating pathology or findings. Required Radiographic Images Select appropriate views for each procedure, listed below. Identify each image, and label each image with patient s name and date of imaging. Best two views must demonstrate appropriate surgical pathology and outcome. Preoperative images (weight- bearing not required for trauma) First Ray Surgery Weightbearing AP, Lateral Infection/ Other Osseous Foot Surgery Foot and Ankle Trauma RRA Surgery Best two views Best two views Weightbearing Best two views Initial postoperative images Within 1 week of surgery Demonstrate operative alignment and fixation, if used (intraoperative images acceptable) Final outcome images At least 4 weeks postoperative Demonstrate removal of provisional/ temporary hardware and radiographic osseous union of osteotomies, fusions, and fractures AP, Lateral Best two views Best two views Best two views Weightbearing AP, Lateral Best two views Best two views Weightbearing Best two views When appropriate, an MRI may substitute for an x-ray. Page 8
9 Board Certification (October 2017) American Board of Foot and Ankle Surgery Common Errors Lack of preoperative weight-bearing radiographs where required. Lack of postoperative weight-bearing radiographs demonstrating reduction of deformity, bone healing, or consolidation. Final radiographs demonstrating provisional/temporary hardware. Failure to upload each image in the appropriate category represented by the image (preoperative, immediate postoperative, and final). Board Certification Examination The Board Certification Computer-based Patient Simulation (CBPS) examination evaluates knowledge and skills in obtaining and interpreting clinical information as well as the ability to reason logically and to arrive at a diagnosis or treatment plan for a specific patient presentation. 1. Register To register for an ABFAS examination, log into the ABFAS website Click Register for an Exam under exam quick links. If you are taking both the Foot Surgery and RRA Surgery CBPS examinations, you may sit for both examinations on the same day. 2. Test Components The CBPS Examination consists of 12 CBPS questions for the Foot Surgery CBPS and 16 for RRA Surgery CBPS. Similar to the Board Qualification CBPS Examination, the Board Certification CBPS Examination uses case scenarios to evaluate clinical reasoning skills, content knowledge, problem-solving ability, and clinical decision making, i.e., ability to reason logically and arrive at a diagnosis or treatment plan for a specific patient presentation. It measures the clinical knowledge, skills, and judgment associated with your ability to integrate academics with surgical experience. The case questions cover diagnostic, intraoperative, and perioperative care of the podiatric surgical patient via clinical scenarios, problem-solving in a case-based format, surgical outcomes assessment, perioperative management, and decision-making. The examination represents commonly accepted standards of care (i.e., regionally and individually unbiased). The examination questions encompass the diagnostic, intraoperative, and perioperative care of the presented patient. The intraoperative content of the Foot examination may include surgical procedures of the entire foot and ankle, except for RRA procedures. The subject areas covered in the Foot Surgery and RRA Surgery examinations are shown in Table 2. The subject area subcategories are listed in Table Instructions and Practice Examination Instructions Access the CBPS Practice Exam instructions Page 9
10 Board Certification (October 2017) American Board of Foot and Ankle Surgery Practice Exam Access the CBPS practice exam. During the exam, do not press the [F5] key or the browser back button. This will log you out of the exam. 4. Testing Sites ABFAS contracts with Pearson VUE to administer examinations. Pearson VUE offers 200 testing sites in the United States and abroad (see ABFAS strongly encourages early registration to ensure availability of a convenient testing site. Failure to Appear Candidates who fail to appear for their examination(s) without completing the formal withdrawal process forfeit all fees. 5. Scoring Test Results ABFAS will you a notification when your test results have been posted (log in to see your results) to your ABFAS profile page. If you fail an exam, you will be able to download a score report that provides an analysis of your performance. Copies of the test items are not available. If you pass only one component of the Board Certification exams, you will receive credit for that component but will not achieve Board Certification status. CBPS or Case Review credit is valid for 7 years or until your eligibility for ABFAS certification expires, whichever occurs first. Statute of Limitations If your Board Qualified status in Foot Surgery expires before your Board Qualified status in RRA Surgery, ABFAS will suspend your RRA status until you have successfully reestablished the required status in Foot Surgery (provided that your RRA status has not expired prior to the reestablishment of Foot Surgery status). If you do not achieve Board Certification by the close of the seventh year after you achieve Board Qualification status, you will no longer be eligible for ABFAS certification, unless you finished a PMSR or PMSR/RRA residency program prior to Appeals ABFAS does not have an appeal process for its examinations. An independent psychometric consultant rescores and reviews all failed examinations. Candidates may write to examconcerns@abfas.org if they have questions about their exam score reports. 7. Confidentiality ABFAS considers the status of an individual's participation in and the stage of completion of all Certification components, including an individual's certification status and certification history, to be public information. ABFAS reserves the right to publish and share public information in any and all public forums determined by ABFAS to be reasonable, including the posting of public information on the ABFAS website, sharing the public information with medical licensure boards, managed care organizations, third party payers, or others. While ABFAS generally regards all other information about individuals as private and confidential, there are times that ABFAS must release certain information to fulfill its responsibilities as a medical specialty board. Page 10
11 Board Certification (October 2017) American Board of Foot and Ankle Surgery ABFAS specifically regards the results of an individual's Qualification, Certification, or Recertification examination (score and whether the individual passed or failed) as private and confidential. Diplomate Certificates After you meet all Board Certification requirements and pass the Board Certification examination, ABFAS will issue you a certificate confirming that you are a: Diplomate of the American Board of Foot and Ankle Surgery with Certification in Foot Surgery and (if applicable) Diplomate of the American Board of Foot and Ankle Surgery with Certification in Reconstructive Rearfoot/Ankle Surgery Period of Certification Initial certification is for a period of 10 years. Board Certified surgeons may promote their status on ABFAS letterhead, publications, and other advertisements following ABFAS advertising guidelines. Page 11
12 Board Certification (October 2017) American Board of Foot and Ankle Surgery Calendar A full calendar for all ABFAS examinations and deadlines is at Exam Calendar. The dates that pertain to the Board Certification Examination and Case Documentation are repeated below for convenience. Board Certification Examination (CBPS) Spring Registration opens November 1, 2017 Registration closes April 25, 2018 Last day to withdraw without penalty May 2, 2018 Examination May 9, 2018 Case Review Registration opens November 1, 2017 Registration closes December 8, 2017 ABFAS notifies candidates of hospital December 12, 2017 audit/surgical privileges needs Deadline for ABFAS to receive hospital audit documentation January 5, 2018 ABFAS notifies candidate of case selection January 22, 2018 Deadline for candidate to upload all case March 9, 2018 documentation Case Reviewers meet April 12-14, 2018 Examination Fees You can find a full list of all ABFAS application, examination, and other fees at Exam Fees. The fees that pertain to the Board Certification Examinations are also repeated below for your convenience. Application Fee (NON-REFUNDABLE). Paid once per calendar year, regardless $225 of number of exams. Examination Board Certification Examination (CBPS) $425 Case Review $475 Withdrawal* On-time 0 Late fees One Part $150 Two Parts $250 * Candidates who do not appear for an examination and have not withdrawn before the examination date will forfeit all fees paid. Page 12
13 Board Certification (October 2017) American Board of Foot and Ankle Surgery APPENDIX A Expanded List of Categories for Foot Certification Case Review Procedures must be logged correctly on PLS by the candidate. Procedures are evaluated and scored based on the category under which it is categorized. For example, if a joint salvage procedure with cheilectomy only is logged as a joint salvage procedure with distal metatarsal osteotomy, the candidate will receive a low or failing score for that case. Open management of fracture or MTPJ dislocation cases must include internal or external fixation. Procedures are evaluated based on surgical decision-making, preoperative clinical assessment, preoperative radiographic assessment, technical skills assessment, and outcomes analysis. Each category in italics has an allowable maximum of 2 of the 30 required cases. Each category in non-italics has an allowable maximum of 15 of the 30 required cases. Hallux Valgus Surgery bunionectomy with phalangeal osteotomy bunionectomy with distal first metatarsal osteotomy bunionectomy with first metatarsal base or shaft osteotomy bunionectomy with first metatarsocuneiform fusion MTPJ fusion MTPJ implant Hallux Limitus Surgery cheilectomy joint salvage with phalangeal osteotomy (Kessel- Bonney, enclavement) joint salvage with distal metatarsal osteotomy joint salvage with first metatarsal shaft or base osteotomy joint salvage with first metatarsocuneiform fusion MTPJ fusion MTPJ implant Other First Ray Surgery osteotomy (e.g., dorsiflexory) metatarsocuneiform fusion (other than for hallux valgus or hallux limitus) amputation management of osseous tumor/neoplasm (with or without bone graft) management of bone/joint infection (with or without bone graft) open management of fracture or MTPJ dislocation with fixation corticotomy with callus distraction revision/repair of surgical outcome (e.g., nonunion, hallux varus) Osseous Foot Surgery 4.5 lesser MTPJ implant 4.6 central metatarsal osteotomy 4.7 bunionectomy of the fifth metatarsal with osteotomy Page 13
14 Board Certification (October 2017) American Board of Foot and Ankle Surgery 4.8 open management of lesser metatarsal fracture(s) 4.10 amputation (lesser ray, transmetatarsal amputation (TMA) 4.11 management of bone/joint infection distal to the tarsometatarsal joints (with or without bone graft) 4.12 management of bone tumor/neoplasm distal to the tarsometatarsal joints (with or without bone graft) 4.13 open management of tarsometatarsal fracture/dislocation 4.14 multiple osteotomy management of metatarsus adductus 4.15 tarsometatarsal fusion 4.16 corticotomy/callus distraction of lesser metatarsal Elective Soft-tissue plastic surgery techniques involving the midfoot, rearfoot or ankle tendon transfer involving the midfoot, rearfoot, ankle, or leg soft-tissue repair of complex congenital foot/ankle deformity (clubfoot, vertical talus) delayed repair of ligamentous structures ligament or tendon augmentation/supplementation/restoration Elective - Osseous detachment/reattachment of Achilles tendon with partial ostectomy midfoot, rearfoot, or ankle fusion midfoot, rearfoot, or tibial osteotomy coalition resection open management of talar dome pathology (with or without osteotomy) ankle arthrotomy with removal of loose body or other osteochondral debridement ankle implant corticotomy or osteotomy with callus distraction/ correction of complex deformity of the midfoot, rearfoot, ankle, or tibia Nonelective Soft tissue repair of acute tendon injury repair of acute ligament injury microscopic nerve/vascular repair of the midfoot, rearfoot, or ankle excision of soft-tissue tumor/mass of the foot (with reconstructive surgery) open repair of dislocation (proximal to tarsometatarsal joints) Nonelective Osseous open repair of adult midfoot fracture open repair of adult rearfoot fracture open repair of adult ankle fracture open repair of pediatric rearfoot/ankle fracture or dislocation management of bone tumor/neoplasm (with or without bone graft) management of bone/joint infection (with or without bone graft) amputation proximal to the tarsometatarsal joints Page 14
15 Board Certification (October 2017) American Board of Foot and Ankle Surgery APPENDIX B RRA Surgery Certification requires logging a minimum of 30 RRA procedures. ABFAS requires a minimum of 12 procedures from the following list. RRA Elective Osseous (minimum 10) midfoot, rearfoot, or ankle fusion midfoot, rearfoot, or tibial osteotomy ankle implant corticotomy or osteotomy with callus distraction/correction of complex deformity of the midfoot, rearfoot, ankle, or tibia RRA Nonelective Osseous (minimum 2) open repair of adult rearfoot fracture open repair of adult ankle fracture open repair of pediatric rearfoot/ankle fracture or dislocation management of bone tumor/neoplasm (with or without bone graft) Procedures must be logged correctly on PLS by the candidate. Procedures are evaluated and scored based on the category under which it is categorized. For example, if excision of a fracture fragment is logged as open reduction and internal fixation of a fracture, the candidate will receive a low or failing score for that case. Open management of fracture or dislocation cases must include internal or external fixation. Foot Surgery cases logged as Reconstructive Rearfoot/Ankle surgery cases will not be scored and no credit will be given for that case. Procedures are evaluated based on surgical decision-making, preoperative clinical assessment, preoperative radiographic assessment, technical skills assessment, and outcomes analysis. Page 15
16 Board Certification (October 2017) American Board of Foot and Ankle Surgery APPENDIX C Table of ABFAS Procedure Categories 1. Digital Surgery category (lesser digit or hallux) 1.1 partial ostectomy 1.8 amputation 1.2 phalangectomy 1.9 management of osseous tumor/neoplasm 1.3 arthroplasty (interphalangeal joint [IPJ]) 1.10 management of bone/joint infection 1.4 implant (IPJ) 1.11 open management of digital 1.5 diaphysectomy fracture/dislocation 1.6 phalangeal osteotomy 1.12 revision/repair of surgical outcome 1.7 fusion (IPJ) 1.13 other osseous digital procedure not listed above 2. First Ray Surgery (30 procedures). Hallux Valgus Surgery bunionectomy (partial ostectomy/silver procedure) bunionectomy with capsulotendon balancing procedure bunionectomy with phalangeal osteotomy bunionectomy with distal first metatarsal osteotomy bunionectomy with first metatarsal base or shaft osteotomy bunionectomy with first metatarsocuneiform fusion MTPJ fusion MTPJ implant MTPJ arthroplasty Hallux Limitus Surgery cheilectomy joint salvage with phalangeal osteotomy (Kessel- Bonney, enclavement) joint salvage with distal metatarsal osteotomy joint salvage with first metatarsal shaft or base osteotomy joint salvage with first metatarsocuneiform fusion MTPJ fusion MTPJ implant MTPJ arthroplasty Other First Ray Surgery tendon transfer/lengthening/ capsulotendon balancing procedure osteotomy (e.g., dorsiflexory) metatarsocuneiform fusion (other than for hallux valgus or hallux limitus) amputation management of osseous tumor/neoplasm (with or without bone graft) management of bone/joint infection (with or without bone graft) open management of fracture or MTPJ dislocation with fixation corticotomy with callus distraction revision/repair of surgical outcome (e.g., nonunion, hallux varus) other first ray procedure not listed above Page 16
17 Board Certification (October 2017) American Board of Foot and Ankle Surgery 3. Other Soft-tissue Foot Surgery 3.1 excision of ossicle/sesamoid 3.9 plantar fasciectomy 3.2 excision of neuroma 3.10 excision of soft-tissue tumor/mass of the 3.3 removal of deep foreign body (excluding hardware removal) foot (without reconstructive surgery) 3.11 external neurolysis/decompression 3.4 plantar fasciotomy (including tarsal tunnel) 3.5 lesser MTPJ capsulotendon balancing 3.12 plastic surgery techniques (including skin 3.6 tendon repair, lengthening, or transfer involving the forefoot (including digital FDL transfer) 3.7 open management of dislocation (MTPJ/tarsometatarsal) graft, skin plasty, flaps, syndactylization, desyndactylization, and debulking procedures limited to the forefoot) 3.13 microscopic nerve/vascular repair (forefoot only) 3.8 incision and drainage/wide debridement of soft-tissue infection (including plantar space) 3.14 other soft-tissue procedures not listed above (limited to the foot). 1. Osseous Foot Surgery 4.1 partial ostectomy (metatarsocuneiform exostosis or exostectomy) 4.11 management of bone/joint infection distal to the tarsometatarsal joints (with or without bone graft) 4.2 lesser MTPJ arthroplasty 4.12 management of bone 4.3 bunionectomy of the fifth metatarsal without osteotomy tumor/neoplasm distal to the tarsometatarsal joints (with or without 4.4 metatarsal head resection (single or multiple) bone graft) 4.13 open management of tarsometatarsal 4.5 lesser MTPJ implant fracture/dislocation 4.6 central metatarsal osteotomy 4.14 multiple osteotomy management of 4.7 bunionectomy of the fifth metatarsal with osteotomy metatarsus adductus 4.15 tarsometatarsal fusion 4.8 open management of lesser metatarsal fracture(s) 4.16 corticotomy/callus distraction of lesser metatarsal 4.9 harvesting of bone graft distal to the ankle 4.17 revision/repair of surgical outcome in the forefoot 4.10 amputation (lesser ray, transmetatarsal amputation (TMA]) 4.18 other osseous procedures not listed above (distal to the tarsometatarsal joint) Page 17
18 Board Certification (October 2017) American Board of Foot and Ankle Surgery 5. Reconstructive Rearfoot/Ankle Surgery (30 procedures) Elective Soft-tissue plastic surgery techniques involving the midfoot, rearfoot or ankle tendon transfer involving the midfoot, rearfoot, ankle, or leg tendon lengthening involving the midfoot, rearfoot, ankle, or leg soft-tissue repair of complex congenital foot/ankle deformity (clubfoot, vertical talus) delayed repair of ligamentous structures ligament or tendon augmentation/supplementation/restorati on open synovectomy of the rearfoot/ankle other elective reconstructive rearfoot /ankle soft-tissue surgery not listed above Elective Osseous operative arthroscopy detachment/reattachment of Achilles tendon with partial ostectomy ankle arthrotomy with removal of loose body or other osteochondral debridement subtalar arthroereisis ankle implant midfoot, rearfoot, or ankle fusion midfoot, rearfoot, or tibial osteotomy coalition resection open management of talar dome pathology (with or without osteotomy) corticotomy or osteotomy with callus distraction/ correction of complex deformity of the midfoot, rearfoot, ankle, or tibia other elective reconstructive rearfoot /ankle osseous surgery not listed above Nonelective Soft tissue repair of acute tendon injury repair of acute ligament injury microscopic nerve/vascular repair of the midfoot, rearfoot, or ankle excision of soft-tissue tumor/mass of the foot (with reconstructive surgery) excision of soft-tissue tumor/mass of the ankle (with or without reconstructive surgery) open repair of dislocation (proximal to tarsometatarsal joints) other nonelective reconstructive rearfoot /ankle soft-tissue surgery not listed above. Page 18
19 Board Certification American Board of Foot and Ankle Surgery Nonelective Osseous open repair of adult midfoot fracture open repair of adult rearfoot fracture open repair of adult ankle fracture open repair of pediatric rearfoot/ankle fracture or dislocation management of bone tumor/neoplasm (with or without bone graft) management of bone/joint infection (with or without bone graft) amputation proximal to the tarsometatarsal joints other nonelective reconstructive rearfoot/ankle osseous surgery not listed above Page 19
20 Board Certification American Board of Foot and Ankle Surgery Appendix D Uploading Images into PLS One of the major areas of concern for candidates preparing their board certification case documentation is images. Indeed, unreadable or inappropriately uploaded images are frequently cited in the case review process. The following information can assist you in the preparation of suitable images for uploading with your case documentation. Hard Copy Images (including MRI and CT) - Use a light box to photograph the image. - Capture the entire image; do not crop or zoom in. Include patient identifying information if possible. - Pictures can be taken with a digital camera or good mobile phone camera. Do not scan the x-ray. - Check the picture carefully. It should be as clear as the original. If it is not, retake until satisfied (a few attempts with different exposures may be necessary). - Save the pictures to your computer. The preferred format for saving is jpg. If you do not have that option, you may save it as jpeg or png. Digital Images - Download the image from your system to your computer or a flash drive. Save it in jpg format. If jpg is not an available option, then save it in jpeg or png format. - Do not take a picture of the image from a monitor or computer screen. General Upload instructions - Follow ABFAS instructions carefully. - Be sure all images are labeled with the patient name and date taken on the image. If your EMR deletes this information or it is unreadable on your picture, place a text box in the image and type in the patient name and date the image was taken. - How do I place a text box? o To do this in Microsoft Paint: Click Open With from the menu bar, hit the text button A to insert a text box. Save. o To do this in Preview on a Mac: Go to the View menu, select Show Edit Toolbar then select the text tool to insert a text box. Save. - Be sure all uploaded images are of the correct patient and procedure. - Be sure to upload images into the correct section on PLS (pre-op/immediate post-op/final) - First ray and RRA cases are to include weight-bearing pre-op and weight-bearing final images. - Trauma cases are not required to have weight-bearing pre-op images. Page 20
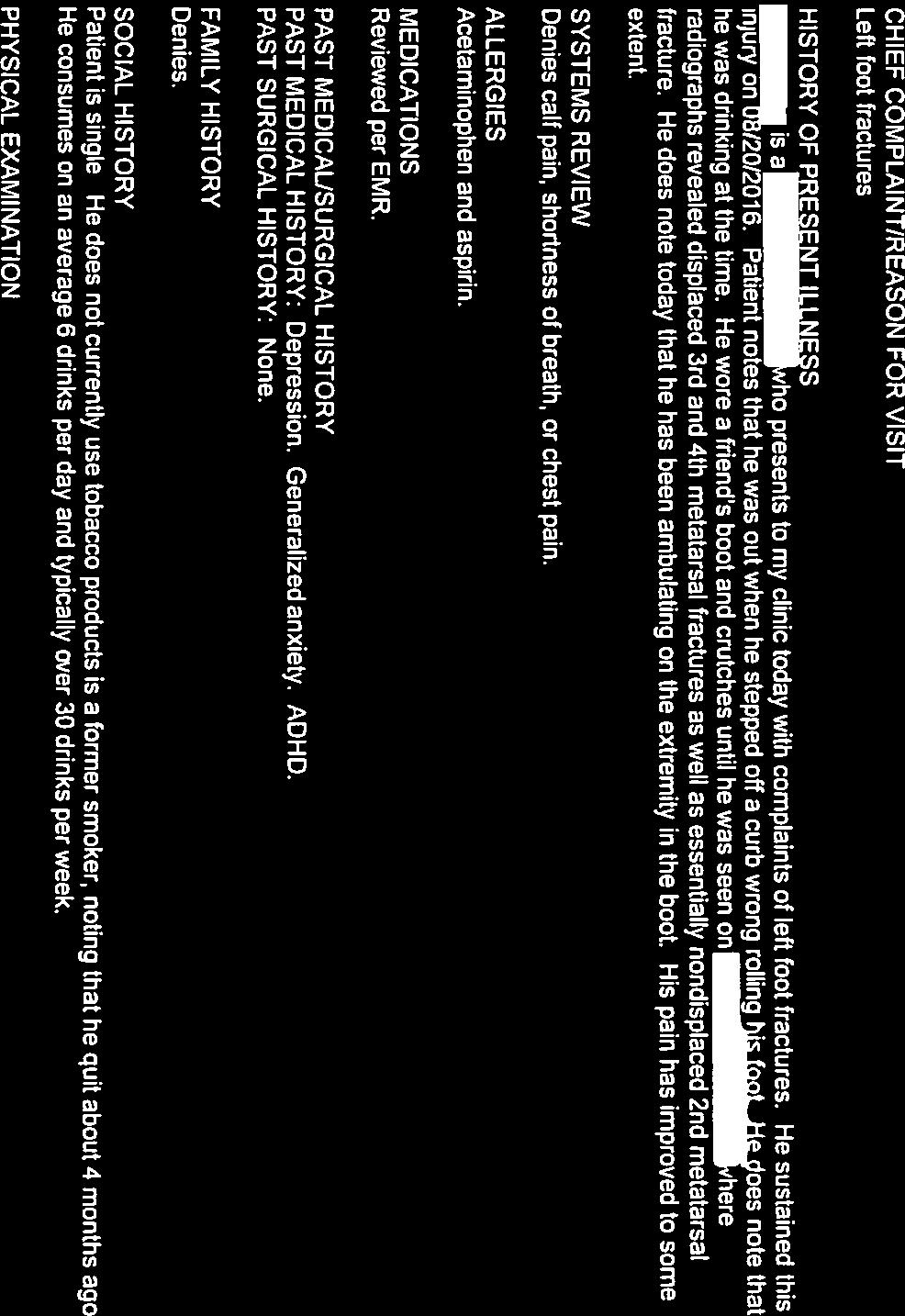
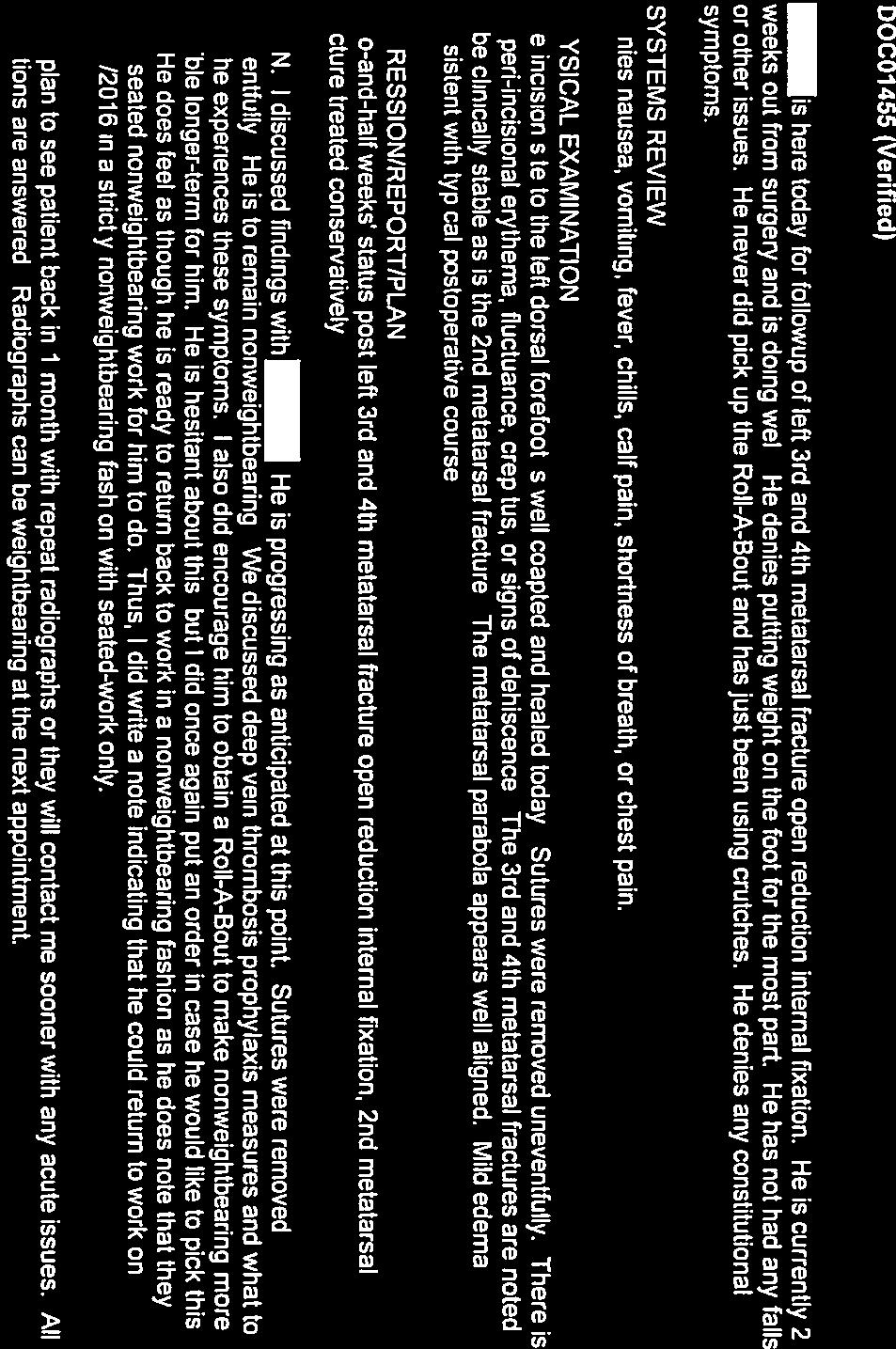
21 Board Certification American Board of Foot and Ankle Surgery Appendix E Sample of Case Documentation to Upload into PLS Page 21

22
23


24

25
26


27

28
29
30

31

32
33

34
35

36
37


38
39

40


41

42
43

44

45

46

47
48


49
50


51


52
53


54

55





56


57
American Board of Foot and Ankle Surgery
 American Board of Foot and Ankle Surgery Logging Guidelines Revisions ABFAS Task Force Mindy Benton, DPM Randall Dei, DPM Charles Lombardi, DPM John Thomas Marcoux, DPM Roya Mirmiran, DPM Michael Vaardahl,
American Board of Foot and Ankle Surgery Logging Guidelines Revisions ABFAS Task Force Mindy Benton, DPM Randall Dei, DPM Charles Lombardi, DPM John Thomas Marcoux, DPM Roya Mirmiran, DPM Michael Vaardahl,
Proper Logging of Surgical Procedures (Effective July 1, 2018)
") Proper Logging of Surgical Procedures (Effective July 1, 2018) GENERAL GUIDELINES: 1) For the procedure codes listed below, the program director must review each entry to determine proper usage. The following
Proper Logging of Surgical Procedures (Effective July 1, 2018) GENERAL GUIDELINES: 1) For the procedure codes listed below, the program director must review each entry to determine proper usage. The following
An Independent, Specialized Accrediting Agency
 9312 Old Georgetown Road Bethesda, Mar yland 20814 P 301.581.9200 I F 301.571.4903 www.cpme.org MEMORANDUM March 20, 2018 TO: FROM: SUBJECT: Program Directors and Residents Council on Podiatric Medical
9312 Old Georgetown Road Bethesda, Mar yland 20814 P 301.581.9200 I F 301.571.4903 www.cpme.org MEMORANDUM March 20, 2018 TO: FROM: SUBJECT: Program Directors and Residents Council on Podiatric Medical
Proper Logging of Podiatric Medical / Surgical Residency Experiences
 Proper Logging of Podiatric Medical / Surgical Residency Experiences Revisions effective July 1, 2018 John T. Marcoux, DPM, FACFAS ABFAS Proper Logging Task Force Mindy Benton, DPM Randall Dei, DPM Charles
Proper Logging of Podiatric Medical / Surgical Residency Experiences Revisions effective July 1, 2018 John T. Marcoux, DPM, FACFAS ABFAS Proper Logging Task Force Mindy Benton, DPM Randall Dei, DPM Charles
CLAD Error Key. Error Levels: Definite, Possible. Error Procedure Scope. Validation Scope. Location Scope. Violation/Information Text
 CLAD Key s: Definite, Possible Procedure 1 2 3 4 5 6 7 8 9 10 Two or more category 1 procedures Digit Definite 1.6 plus one or more of the following: 2.1.3, 2.1.7, 2.2.2, 2.2.6, and 2.3.4 Side Definite
CLAD Key s: Definite, Possible Procedure 1 2 3 4 5 6 7 8 9 10 Two or more category 1 procedures Digit Definite 1.6 plus one or more of the following: 2.1.3, 2.1.7, 2.2.2, 2.2.6, and 2.3.4 Side Definite
ABPS 500. Examination Blueprints (Revised Classification) American Board of Podiatric Surgery 445 Fillmore Street San Francisco, CA
 American Board of Podiatric Surgery 445 Fillmore Street San Francisco, CA") ABPS 500 Examination Blueprints () American Board of Podiatric Surgery 445 Fillmore Street San Francisco, CA 94117-3404 (415) 553-7800 (415) 553-7801 (FAX) info@abps.org November 2012 Purpose, Test Specification,
ABPS 500 Examination Blueprints () American Board of Podiatric Surgery 445 Fillmore Street San Francisco, CA 94117-3404 (415) 553-7800 (415) 553-7801 (FAX) info@abps.org November 2012 Purpose, Test Specification,
DEPARTMENT OF SURGERY PODIATRIC SURGERY
 NAME: DEPARTMENT OF SURGERY PODIATRIC SURGERY Applicant: Check the Requested box for each privilege requested. Applicants have the burden of producing information deemed adequate by the hospital for a
NAME: DEPARTMENT OF SURGERY PODIATRIC SURGERY Applicant: Check the Requested box for each privilege requested. Applicants have the burden of producing information deemed adequate by the hospital for a
Alberta Health Care Insurance Plan. Schedule Of Anaesthetic Rates Applicable To Podiatry. Procedure List. As Of. 01 April Government of Alberta
 Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
AMERICAN BOARD OF FOOT AND ANKLE SURGERY
 AMERICAN BOARD OF FOOT AND ANKLE SURGERY In-training Examination Guide for Residency Directors 445 Fillmore Street San Francisco, CA 94117 (415) 553-7800 www.abfas.org This document contains information
AMERICAN BOARD OF FOOT AND ANKLE SURGERY In-training Examination Guide for Residency Directors 445 Fillmore Street San Francisco, CA 94117 (415) 553-7800 www.abfas.org This document contains information
Alberta Health Care Insurance Plan. Schedule Of Anaesthetic Rates Applicable To Podiatric Surgery. Procedure List. As Of.
 Alberta Health Care Insurance Plan Procedure List As Of 01 April 2016 Alberta Health Care Insurance Plan Page i Generated 2016/03/22 TABLE OF CONTENTS As of 2016/04/01 07 PHYSICAL MEDICINE, REHABILITATION,
Alberta Health Care Insurance Plan Procedure List As Of 01 April 2016 Alberta Health Care Insurance Plan Page i Generated 2016/03/22 TABLE OF CONTENTS As of 2016/04/01 07 PHYSICAL MEDICINE, REHABILITATION,
Didactic activities will be provided in a variety of formats, including faculty participation, which shall include:
 Didactic Training Didactic activities that complement and supplement the curriculum shall be available at least weekly. The formal schedule will be developed and distributed prior to the beginning of each
Didactic Training Didactic activities that complement and supplement the curriculum shall be available at least weekly. The formal schedule will be developed and distributed prior to the beginning of each
Cpt code for exostectomy medial cuneiform
 Cpt code for exostectomy medial cuneiform The Borg System is 100 % Cpt code for exostectomy medial cuneiform 9-11-2011 Exostectomy left third and fourth cuboid and lateral cun. Exostectomy cuneiforms and
Cpt code for exostectomy medial cuneiform The Borg System is 100 % Cpt code for exostectomy medial cuneiform 9-11-2011 Exostectomy left third and fourth cuboid and lateral cun. Exostectomy cuneiforms and
MINIMALLY INVASIVE FOOT AND ANKLE SURGERY CERTIFICATION CASE REQUIREMENTS AND GUIDELINES
 MINIMALLY INVASIVE FOOT AND ANKLE SURGERY CERTIFICATION CASE REQUIREMENTS AND GUIDELINES Document number: 61714.10142017 Originated 10.14.2017 555 8 th Ave Suite 1902 New York, NY 10018 (888) 852-1442
MINIMALLY INVASIVE FOOT AND ANKLE SURGERY CERTIFICATION CASE REQUIREMENTS AND GUIDELINES Document number: 61714.10142017 Originated 10.14.2017 555 8 th Ave Suite 1902 New York, NY 10018 (888) 852-1442
Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES
 Updated 2/8/10 Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES INTERPERSONAL AND COMMUNICATION SKILLS Resident will at all times demonstrate behavior that is beyond reproach. Residents must be
Updated 2/8/10 Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES INTERPERSONAL AND COMMUNICATION SKILLS Resident will at all times demonstrate behavior that is beyond reproach. Residents must be
Department of Orthopedic Surgery
 Department of Orthopedic Surgery CT 1 asic Privileges: Patient management, including H & Ps and diagnostic and therapeutic treatments, procedures and interventions encompassing the areas described under
Department of Orthopedic Surgery CT 1 asic Privileges: Patient management, including H & Ps and diagnostic and therapeutic treatments, procedures and interventions encompassing the areas described under
Certification in Lower Extremity Geriatric Medicine Handbook
 Certification in Lower Extremity Geriatric Medicine Handbook 555 8 th Ave, Ste 1902, New York, NY 10018 888 852 1442 1 Mission Statement We exist to protect and improve the podiatric health and welfare
Certification in Lower Extremity Geriatric Medicine Handbook 555 8 th Ave, Ste 1902, New York, NY 10018 888 852 1442 1 Mission Statement We exist to protect and improve the podiatric health and welfare
Index. Clin Podiatr Med Surg 22 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Clin Podiatr Med Surg 22 (2005) 309 314 Index Note: Page numbers of article titles are in boldface type. A Abductor digiti minimi muscle, myectomy of, for tailor s bunionette, 243 Achilles tendon, lengthening
Foot and Ankle Systems Coding Reference Guide
 Foot and Ankle Systems Coding Reference Guide Physician Arthrodesis 27870 Arthrodesis, ankle, open 27871 Arthrodesis, tibiofibular joint, proximal or distal 28705 Arthrodesis; pantalar 28715 Arthrodesis;
Foot and Ankle Systems Coding Reference Guide Physician Arthrodesis 27870 Arthrodesis, ankle, open 27871 Arthrodesis, tibiofibular joint, proximal or distal 28705 Arthrodesis; pantalar 28715 Arthrodesis;
Section 6: Preoperative Planning
 Clinical Relevance of the PedCat Study: In many ways the PedCat study confirmed radiographic findings. With the measuring tools embedded in the DICOM viewing software it was possible to gauge the thickness
Clinical Relevance of the PedCat Study: In many ways the PedCat study confirmed radiographic findings. With the measuring tools embedded in the DICOM viewing software it was possible to gauge the thickness
SAN ANTONIO, TEXAS DECEMBER 9-11, 2010 Hyatt Regency Hill Country Resort & Spa Resort, San Antonio, TX USA. Program Agenda
 6 th ANNUAL INTERNATIONAL EXTERNAL FIXATION SYMPOSIUM The Diabetic Charcot Foot SAN ANTONIO, TEXAS DECEMBER 9-11, 2010 Hyatt Regency Hill Country Resort & Spa Resort, San Antonio, TX USA Program Agenda
6 th ANNUAL INTERNATIONAL EXTERNAL FIXATION SYMPOSIUM The Diabetic Charcot Foot SAN ANTONIO, TEXAS DECEMBER 9-11, 2010 Hyatt Regency Hill Country Resort & Spa Resort, San Antonio, TX USA Program Agenda
3. The prescribed fee shall be accepted as payment in full for the podiatry services.
 WorkSafeBC Schedule for Podiatry Services 1. The Payment Schedule includes the services of podiatrists who are registered members in good standing of the College of Podiatric Surgeons of British Columbia,
WorkSafeBC Schedule for Podiatry Services 1. The Payment Schedule includes the services of podiatrists who are registered members in good standing of the College of Podiatric Surgeons of British Columbia,
2017 SAFSA CONGRESS PROGRAMME
 2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,
2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,
MULTIPLE APPLICATIONS OF THE MINIRAIL
 C H A P T E R 2 1 MULTIPLE APPLICATIONS OF THE MINIRAIL Thomas J. Merrill, DPM James M. Losito, DPM Mario Cala, DPM Victor Herrera, DPM Alan E. Sotelo, DPM INTRODUCTION The unilateral MiniRail External
C H A P T E R 2 1 MULTIPLE APPLICATIONS OF THE MINIRAIL Thomas J. Merrill, DPM James M. Losito, DPM Mario Cala, DPM Victor Herrera, DPM Alan E. Sotelo, DPM INTRODUCTION The unilateral MiniRail External
*Rippstein, Trnka, Saragas, Hoffman
 THURS 25th MAY 07:00 07:10 Welcome and Introductions Paulo Ferrao Lecture 1: 07:10 09:45 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 40 mins 07:10 07:50 Surgical Management of Hallux Valgus 30
THURS 25th MAY 07:00 07:10 Welcome and Introductions Paulo Ferrao Lecture 1: 07:10 09:45 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 40 mins 07:10 07:50 Surgical Management of Hallux Valgus 30
Rippstein, Trnka, Saragas, Narramore
 THURS 25th MAY 07:45 07:55 Welcome and Introductions Paulo Ferrao Lecture 1: 08:00 10:20 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 30 mins 08:00 08:30 Surgical Management of Hallux Valgus Saragas,
THURS 25th MAY 07:45 07:55 Welcome and Introductions Paulo Ferrao Lecture 1: 08:00 10:20 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 30 mins 08:00 08:30 Surgical Management of Hallux Valgus Saragas,
Curriculum Vitae Charles M. Lombardi, DPM
 Curriculum Vitae Charles M. Lombardi, DPM General A Date of Preparation: April 24, 2009 General Information: Birth date: March 8, 1956 Birth Place: New York, NY Citizenship: USA Licensure: Family: Date
Curriculum Vitae Charles M. Lombardi, DPM General A Date of Preparation: April 24, 2009 General Information: Birth date: March 8, 1956 Birth Place: New York, NY Citizenship: USA Licensure: Family: Date
code it PRO-TOE C2 HCPCS Device Codes CPT Codes Physician Coding Hammertoe Implant HCPCS Code Description C1713 CPT CODE Description RVUs
 code it HCPCS Device Codes 2015 Reimbursement Codes The following codes contained within this document are representative of possible services or diagnoses that may be associated with use of Wright products.
code it HCPCS Device Codes 2015 Reimbursement Codes The following codes contained within this document are representative of possible services or diagnoses that may be associated with use of Wright products.
CURRICULUM VITAE. East Lansing, Michigan B.S. Biochemistry. Michigan State University
 NAME: EDUCATION: Michigan State University East Lansing, Michigan 1979-1983 B.S. Biochemistry Michigan State University College of Osteopathic Medicine East Lansing, Michigan Top 20% Class Standing 1983-1987
NAME: EDUCATION: Michigan State University East Lansing, Michigan 1979-1983 B.S. Biochemistry Michigan State University College of Osteopathic Medicine East Lansing, Michigan Top 20% Class Standing 1983-1987
Foot & Ankle Disorders
 Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective: 03/21/ 2012
 [ ] Initial appointment [ ] Reappointment Instructions All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective: 03/21/ 2012 Applicant: Check off
[ ] Initial appointment [ ] Reappointment Instructions All new applicants must meet the following requirements as approved by the UNM SRMC Board of Directors effective: 03/21/ 2012 Applicant: Check off
Orthopedic Surgery Goals and Objectives FOOT AND ANKLE ROTATION. Preamble
 Orthopedic Surgery Goals and Objectives FOOT AND ANKLE ROTATION Preamble Residents will complete a junior and a senior foot & ankle rotation during their training. The expectations, goals and objectives
Orthopedic Surgery Goals and Objectives FOOT AND ANKLE ROTATION Preamble Residents will complete a junior and a senior foot & ankle rotation during their training. The expectations, goals and objectives
Technique Guide. 6.5 mm Midfoot Fusion Bolt. For intramedullary fixation of the medial column of the foot.
 Technique Guide 6.5 mm Midfoot Fusion Bolt. For intramedullary fixation of the medial column of the foot. Table of Contents Introduction 6.5 mm Midfoot Fusion Bolt 2 AO Principles 4 Indications 5 Surgical
Technique Guide 6.5 mm Midfoot Fusion Bolt. For intramedullary fixation of the medial column of the foot. Table of Contents Introduction 6.5 mm Midfoot Fusion Bolt 2 AO Principles 4 Indications 5 Surgical
Total Number Programs Evaluated: 382 January 1, 2000 through October 31, 2017
 Page 1 Oral and Maxillofacial Surgery -Residency INFORMATIONAL REPORT ON FREQUENCY OF CITINGS OF ACCREDITATION STANDARDS FOR ADVANCED SPECIALTY EDUCATION PROGRAMS IN ORAL AND MAXILLOFACIAL SURGERY Frequency
Page 1 Oral and Maxillofacial Surgery -Residency INFORMATIONAL REPORT ON FREQUENCY OF CITINGS OF ACCREDITATION STANDARDS FOR ADVANCED SPECIALTY EDUCATION PROGRAMS IN ORAL AND MAXILLOFACIAL SURGERY Frequency
POSTOP FOLLOW-UP & REHABILITATION FOLLOWING FOOT & ANKLE SURGERY
 1 POSTOP FOLLOW-UP & REHABILITATION FOLLOWING FOOT & ANKLE SURGERY The following instructions are general guidelines, but surgeon post-op instructions will dictate the individual patient's post-op management
1 POSTOP FOLLOW-UP & REHABILITATION FOLLOWING FOOT & ANKLE SURGERY The following instructions are general guidelines, but surgeon post-op instructions will dictate the individual patient's post-op management
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abscesses, 27 30 Acellular products, for bone healing, 55 56 Acetaminophen, 79 80 Achilles tendon lengthening, for pediatric flatfoot,
Index Note: Page numbers of article titles are in boldface type. A Abscesses, 27 30 Acellular products, for bone healing, 55 56 Acetaminophen, 79 80 Achilles tendon lengthening, for pediatric flatfoot,
Delineation of Privileges Department of Internal Medicine Division of Metabolism, Endocrinology and Diabetes PODIATRY
 University of Michigan Hospitals and Health Centers Delineation of Privileges Department of Internal Medicine Division of Metabolism, Endocrinology and Diabetes PODIATRY Name: Please Print or Type LEVEL
University of Michigan Hospitals and Health Centers Delineation of Privileges Department of Internal Medicine Division of Metabolism, Endocrinology and Diabetes PODIATRY Name: Please Print or Type LEVEL
Loma Linda University Children s Hospital Loma Linda, CA ORTHOPAEDIC SURGERY PRIVILEGE FORM
 Name: Page 1 of 6 REQUEST CATEGORY MEMBERSHIP CATEGORY Provisional (Bylaws 4.3) Administrative (Bylaws 4.7) Affiliate (Bylaws(4.9) Active (Bylaws 4.2) Courtesy (Bylaws 4.4) Consulting (Bylaws 4.5) All
Name: Page 1 of 6 REQUEST CATEGORY MEMBERSHIP CATEGORY Provisional (Bylaws 4.3) Administrative (Bylaws 4.7) Affiliate (Bylaws(4.9) Active (Bylaws 4.2) Courtesy (Bylaws 4.4) Consulting (Bylaws 4.5) All
IBCSOMS Certificate of Added Qualification Handbook
 IBCSOMS Certificate of Added Qualification Handbook TABLE OF CONTENTS IMPORTANT: The enclosed Rules and Procedures are specific to initial Subspecialty Certification in Head and Neck Oncologic and Reconstructive
IBCSOMS Certificate of Added Qualification Handbook TABLE OF CONTENTS IMPORTANT: The enclosed Rules and Procedures are specific to initial Subspecialty Certification in Head and Neck Oncologic and Reconstructive
Foot and ankle update
 Foot and ankle update Mr Ian Garnham Consultant Foot and Ankle Surgeon Whipps Cross University Hospital Hallux Rigidus Symptoms first ray and 1st MTP pain and swelling worse with push off or forced dorsiflexion
Foot and ankle update Mr Ian Garnham Consultant Foot and Ankle Surgeon Whipps Cross University Hospital Hallux Rigidus Symptoms first ray and 1st MTP pain and swelling worse with push off or forced dorsiflexion
2018 BOARD CERTIFICATION HANDBOOK
 Page 1 Mission Objectives Organization 2018 BOARD CERTIFICATION HANDBOOK ABOMS 625 North Michigan Avenue Suite 1820 Chicago IL, 60611 Page 2 Examinations & Examination Applications Page 4 2017 Examination
Page 1 Mission Objectives Organization 2018 BOARD CERTIFICATION HANDBOOK ABOMS 625 North Michigan Avenue Suite 1820 Chicago IL, 60611 Page 2 Examinations & Examination Applications Page 4 2017 Examination
Index. Note: Page numbers of article titles are in bold face type.
 Index Note: Page numbers of article titles are in bold face type. A Achilles tendon, Zadek osteotomy effects on, 430 Adult acquired flatfoot disorder, 387 403 calcaneal Z osteotomy for, 397 399 historical
Index Note: Page numbers of article titles are in bold face type. A Achilles tendon, Zadek osteotomy effects on, 430 Adult acquired flatfoot disorder, 387 403 calcaneal Z osteotomy for, 397 399 historical
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium
 MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
MiniRail System. Part B: Foot Applications. By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito
 Q U I C K R E F E R E N C E G U I D E 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ORDERING INFORMATION MiniRail System Kit, M190C Contents: M 101 Standard
Q U I C K R E F E R E N C E G U I D E 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ORDERING INFORMATION MiniRail System Kit, M190C Contents: M 101 Standard
pedcat Clinical Case Studies
 pedcat Clinical Case Studies C u r v e B e a m 1 7 5 T i t u s A v e, S u i t e 3 0 0 W a r r i n g t o n, P A 1 8 9 7 6 267-4 8 3-8081 w w w. c u r v e b e a m. c o m PedCAT: Clinical Evidence of diagnostic
pedcat Clinical Case Studies C u r v e B e a m 1 7 5 T i t u s A v e, S u i t e 3 0 0 W a r r i n g t o n, P A 1 8 9 7 6 267-4 8 3-8081 w w w. c u r v e b e a m. c o m PedCAT: Clinical Evidence of diagnostic
Page 1 of 6. Appendix 1
 Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
Page 1 Appendix 1 Rotation Objectives and Schedule 1. Introductory Month 4 weeks 2. Total Joints 4 weeks a. Diagnosis and management of hip and knee arthritis b. Indications for surgery c. Implant selection;
Midfoot - Reduction & Fixation - ORIF - screw fixation - AO Surgery Reference. ORIF - screw fixation
 Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
PROGRAM AGREEMENT (for 2018 Fellowship Match for fellowship positions) RECITALS
 RECITALS") 2017-2018 PROGRAM AGREEMENT (for 2018 Fellowship Match for 2019-2020 fellowship positions) This Agreement is made and entered into as of the day of, 201 by and between the American Orthopaedic Foot & Ankle
2017-2018 PROGRAM AGREEMENT (for 2018 Fellowship Match for 2019-2020 fellowship positions) This Agreement is made and entered into as of the day of, 201 by and between the American Orthopaedic Foot & Ankle
Introduction. October 2018 Page 1
 Requirements for Recognition of Dental Specialties and National Certifying Boards for Dental Specialists Adopted as Amended by the ADA House of Delegates, October 2018 Introduction A specialty is an area
Requirements for Recognition of Dental Specialties and National Certifying Boards for Dental Specialists Adopted as Amended by the ADA House of Delegates, October 2018 Introduction A specialty is an area
AMERICAN BOARD OF CRANIOFACIAL DENTAL SLEEP MEDICINE
 AMERICAN BOARD OF CRANIOFACIAL DENTAL SLEEP MEDICINE Requirements for ABCDSM Craniofacial Dental Sleep Medicine Credentialing I. Background Craniofacial Dental Sleep Medicine is the area of dentistry that
AMERICAN BOARD OF CRANIOFACIAL DENTAL SLEEP MEDICINE Requirements for ABCDSM Craniofacial Dental Sleep Medicine Credentialing I. Background Craniofacial Dental Sleep Medicine is the area of dentistry that
Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow.
 Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow. Berezhnoy Sergey. Percutaneous First Metatarsocuneiform Joint Arthrodesis in a Treatment of Metatarsus Primus Varus: a Prospective
Medincenter GlavUpDK by the Ministry of Foreign Affairs of Russia, Moscow. Berezhnoy Sergey. Percutaneous First Metatarsocuneiform Joint Arthrodesis in a Treatment of Metatarsus Primus Varus: a Prospective
The American Academy of Foot & Ankle Osteosynthesis. presents
 The American Academy of Foot & Ankle Osteosynthesis presents Comprehensive Course of Internal Fixation for Reconstructive Surgery and Trauma of the Foot & Ankle September 4-6, 2014 Goodlett Farms Innovation
The American Academy of Foot & Ankle Osteosynthesis presents Comprehensive Course of Internal Fixation for Reconstructive Surgery and Trauma of the Foot & Ankle September 4-6, 2014 Goodlett Farms Innovation
QUICK REFERENCE GUIDE. MiniRail System. Part B: Foot Applications. By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING
 14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING ORDERING INFORMATION Sterilization box, empty M190 Can accommodate: M101 Standard MiniRail
14 MiniRail System Part B: Foot Applications By Dr. B. Magnan, Dr. E. Rodriguez and Dr. G. Vito ALWAYS INNOVATING ORDERING INFORMATION Sterilization box, empty M190 Can accommodate: M101 Standard MiniRail
CERTIFICATION IN LOWER EXTREMITY GERIATRIC MEDICINE CASE REQUIREMENTS AND GUIDELINES
 CERTIFICATION IN LOWER EXTREMITY GERIATRIC MEDICINE CASE REQUIREMENTS AND GUIDELINES 555 8 th Ave Suite 1902 New York, NY 10018 (888) 852-1442 Document number: 61714.10142017 Originated 10.14.2017 ABMSP
CERTIFICATION IN LOWER EXTREMITY GERIATRIC MEDICINE CASE REQUIREMENTS AND GUIDELINES 555 8 th Ave Suite 1902 New York, NY 10018 (888) 852-1442 Document number: 61714.10142017 Originated 10.14.2017 ABMSP
6.5 mm midfoot fusion bolt
 6.5 mm midfoot fusion bolt For intramedullary fixation of the medial column of the foot SurgIcal technique Table of Contents Introduction 6.5 mm Midfoot Fusion Bolt 2 AO Principles 4 Indications 5 Surgical
6.5 mm midfoot fusion bolt For intramedullary fixation of the medial column of the foot SurgIcal technique Table of Contents Introduction 6.5 mm Midfoot Fusion Bolt 2 AO Principles 4 Indications 5 Surgical
Regions Hospital Delineation of Privileges Orthopaedic Surgery
 Regions Hospital Delineation of Orthopaedic Surgery Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic formal
Regions Hospital Delineation of Orthopaedic Surgery Applicant s Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting. Review education and basic formal
5 COMMON CONDITIONS IN THE FOOT & ANKLE
 5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
Wet Lab. Elective Foot and Ankle Surgery. Orthopedic-Trauma Instructional Courses, University Hospital Basel.
 Wet Lab. Elective Foot and Ankle Surgery. Orthopedic-Trauma Instructional Courses,. Program April 26 27, 2012 08.00 18.30 h 08.00 13.30 h Institute of Anatomy Variable Angle LCP Forefoot/Midfoot System
Wet Lab. Elective Foot and Ankle Surgery. Orthopedic-Trauma Instructional Courses,. Program April 26 27, 2012 08.00 18.30 h 08.00 13.30 h Institute of Anatomy Variable Angle LCP Forefoot/Midfoot System
Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot
 168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
168 Forefoot Reconstruction Use of the 20 Memory Staple in Osteotomies of Fusions of the Forefoot Definition, History, Generalities This staple first provides a permanent compression both in the prongs
SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT
 C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
CHAPTER Section 3 of P.L.1983, c.296 (C.45: ) is amended to read as follows:
 is amended to read as follows:") CHAPTER 121 AN ACT concerning the practice of physical therapy, amending P.L.2003, c.18, and amending and supplementing P.L.1983, c.296. BE IT ENACTED by the Senate and General Assembly of the State of
CHAPTER 121 AN ACT concerning the practice of physical therapy, amending P.L.2003, c.18, and amending and supplementing P.L.1983, c.296. BE IT ENACTED by the Senate and General Assembly of the State of
Increased pressures at
 Surgical Off-loading of Plantar Hallux Ulcerations These approaches can be used to treat DFUs. By Adam R. Johnson, DPM Increased pressures at the plantar aspect of the hallux leading to chronic hyperkeratosis
Surgical Off-loading of Plantar Hallux Ulcerations These approaches can be used to treat DFUs. By Adam R. Johnson, DPM Increased pressures at the plantar aspect of the hallux leading to chronic hyperkeratosis
CASE REPORT. Antegrade tibia lengthening with the PRECICE Limb Lengthening technology
 CASE REPORT Antegrade tibia lengthening with the PRECICE Limb Lengthening technology Austin T. Fragomen, M.D. Hospital for Special Surgery New York, NY 1 1 PR O D U CTS CONDITION Nonunion of an attempted
CASE REPORT Antegrade tibia lengthening with the PRECICE Limb Lengthening technology Austin T. Fragomen, M.D. Hospital for Special Surgery New York, NY 1 1 PR O D U CTS CONDITION Nonunion of an attempted
Amputation is the removal of a limb by trauma, medical illness, or surgery. As a surgical measure, it is used to control pain or a disease process in
 Amputation is the removal of a limb by trauma, medical illness, or surgery. As a surgical measure, it is used to control pain or a disease process in the affected limb, such as malignancy or gangrene.
Amputation is the removal of a limb by trauma, medical illness, or surgery. As a surgical measure, it is used to control pain or a disease process in the affected limb, such as malignancy or gangrene.
DAY 1: FRIDAY, 31 st AUGUST Operative Sessions: 8.00 am to 3.30 pm
 DAY 1: FRIDAY, 31 st AUGUST Operative Sessions: 8.00 am to 3.30 pm SURGICAL PROCEDURES / CASES (PROPOSED) 1. Haglund with Tendoachilles Tendinopathy 2. ORIF Calcaneus Fracture 3. OCD talus: Arthroscopic
DAY 1: FRIDAY, 31 st AUGUST Operative Sessions: 8.00 am to 3.30 pm SURGICAL PROCEDURES / CASES (PROPOSED) 1. Haglund with Tendoachilles Tendinopathy 2. ORIF Calcaneus Fracture 3. OCD talus: Arthroscopic
The American Academy of Foot & Ankle Osteosynthesis. presents
 The American Academy of Foot & Ankle Osteosynthesis presents Comprehensive Course of Internal Fixation for Reconstructive Surgery and Trauma of the Foot & Ankle Hyatt DFW Airport Dallas, Texas SCIENTIFIC
The American Academy of Foot & Ankle Osteosynthesis presents Comprehensive Course of Internal Fixation for Reconstructive Surgery and Trauma of the Foot & Ankle Hyatt DFW Airport Dallas, Texas SCIENTIFIC
Surgical Off-loading. Reiber et al Goals of Diabetic Foot Surgery 4/28/2012. The most common causal pathway to a diabetic foot ulceration
 Reiber et al. 1999 Surgical Off-loading The most common causal pathway to a diabetic foot ulceration Alex Reyzelman DPM Associate Professor California School of Podiatric Medicine at Samuel Merritt University
Reiber et al. 1999 Surgical Off-loading The most common causal pathway to a diabetic foot ulceration Alex Reyzelman DPM Associate Professor California School of Podiatric Medicine at Samuel Merritt University
PATH Intl. Interactive Vaulting Instructor Application Booklet
 PATH Intl. Interactive Vaulting Instructor Application Booklet Updated 1/2019 Page 1 PATH Intl. Interactive Vaulting Instructor Application Booklet Table of Contents THE PATH INTL. INTERACTIVE VAULTING
PATH Intl. Interactive Vaulting Instructor Application Booklet Updated 1/2019 Page 1 PATH Intl. Interactive Vaulting Instructor Application Booklet Table of Contents THE PATH INTL. INTERACTIVE VAULTING
19 Arthrodesis of the First Metatarsocuneiform Joint
 19 Arthrodesis of the First Metatarsocuneiform Joint CHARLES GUDAS Abduction of the first metatarsal to correct metatarsus primus varus and hallux valgus was first described by Albrecht in 1911. 1 Lapidus
19 Arthrodesis of the First Metatarsocuneiform Joint CHARLES GUDAS Abduction of the first metatarsal to correct metatarsus primus varus and hallux valgus was first described by Albrecht in 1911. 1 Lapidus
Cpt code removal of metatarsal stump
 Cpt code removal of metatarsal stump This article will focus on the definitions of three root operations:. 2018 by The American Health Information Management Association. All Rights Reserved. Osteotomy
Cpt code removal of metatarsal stump This article will focus on the definitions of three root operations:. 2018 by The American Health Information Management Association. All Rights Reserved. Osteotomy
HEMI IMPLANT ARTHROPLASTY FOR THE SECOND METATARSOPHALANGEAL JOINT
 C H A P T E R 1 5 HEMI IMPLANT ARTHROPLASTY FOR THE SECOND METATARSOPHALANGEAL JOINT Joe T. Southerland, DPM Mickey D. Stapp, DPM INTRODUCTION Hemi-implant arthroplasty of the first metatarsophalangeal
C H A P T E R 1 5 HEMI IMPLANT ARTHROPLASTY FOR THE SECOND METATARSOPHALANGEAL JOINT Joe T. Southerland, DPM Mickey D. Stapp, DPM INTRODUCTION Hemi-implant arthroplasty of the first metatarsophalangeal
New York Certified Peer Specialist
 New York Certified Peer Specialist PROVISIONAL Application New York Peer Specialist Certification Board 11 North Pearl Street, Suite 801 Albany New York 12207 Phone: 518.426.0945 Fax: 518.426.1046 www.nypeerspecialist.org
New York Certified Peer Specialist PROVISIONAL Application New York Peer Specialist Certification Board 11 North Pearl Street, Suite 801 Albany New York 12207 Phone: 518.426.0945 Fax: 518.426.1046 www.nypeerspecialist.org
Foot Disorders, from the cradle to the grave
 Foot Disorders, from the cradle to the grave A O ADEDAPO MBBS, FRCS, FRCS(Tr/Orth) Consultant Orthopaedic Surgeon James Cook University Hospital Middlesbrough, U.K. General Overview. General Orthopaedic
Foot Disorders, from the cradle to the grave A O ADEDAPO MBBS, FRCS, FRCS(Tr/Orth) Consultant Orthopaedic Surgeon James Cook University Hospital Middlesbrough, U.K. General Overview. General Orthopaedic
Is Distraction Histiogenesis a Reliable Method to Reconstruct Segmental Bone and Acquired Leg Length Discrepancy in Tibia Fractures and Non Unions?
 Is Distraction Histiogenesis a Reliable Method to Reconstruct Segmental Bone and Acquired Leg Length Discrepancy in Tibia Fractures and Non Unions? James J Hutson Jr MD Professor Orthopedic Trauma Ryder
Is Distraction Histiogenesis a Reliable Method to Reconstruct Segmental Bone and Acquired Leg Length Discrepancy in Tibia Fractures and Non Unions? James J Hutson Jr MD Professor Orthopedic Trauma Ryder
Mr. Siva Chandrasekaran Orthopaedic Surgeon MBBS MSpMed MPhil (surg) FRACS
 FRACS") Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
Bunion Surgery Most people with bunions find pain relief with simple treatments to reduce pressure on the big toe, such as wearing wider shoes or using pads in their shoes. However, if these measures do
RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS
 C H A P T E R 1 7 RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS Michelle L. Butterworth, DPM Michael S. Downey, DPM Digital deformities are one of the most common entities we face as foot and
C H A P T E R 1 7 RETROSPECTIVE ANALYSIS OF END-TO-END DIGITAL ARTHRODESIS Michelle L. Butterworth, DPM Michael S. Downey, DPM Digital deformities are one of the most common entities we face as foot and
APPLICATION FELLOWSHIP IN IMPLANT DENTISTRY PROGRAM
 : Application Date Month Day Year University of Rochester University of Rochester Medical Center Eastman Institute for Oral Health 625 Elmwood Avenue Rochester, New York 14620-2989 USA (585) 275-8315 Paste
: Application Date Month Day Year University of Rochester University of Rochester Medical Center Eastman Institute for Oral Health 625 Elmwood Avenue Rochester, New York 14620-2989 USA (585) 275-8315 Paste
DARCO. Bow 2 Plate SURGIC AL TECHNIQUE
 DARCO Bow 2 Plate SURGIC AL TECHNIQUE Contents 2 Preface 3 Chapter 1 4 Chapter 2 5 6 7 8 9 Appendix 10 10 11 Intended Use Indications/Contraindications Design Rationale Preoperative Planning Surgical Technique
DARCO Bow 2 Plate SURGIC AL TECHNIQUE Contents 2 Preface 3 Chapter 1 4 Chapter 2 5 6 7 8 9 Appendix 10 10 11 Intended Use Indications/Contraindications Design Rationale Preoperative Planning Surgical Technique
Anesthesia Cross Coder. Essential links from CPT codes to ICD-9-CM and HCPCS codes
 Anesthesia Cross Coder Essential links from CPT codes to ICD-9-CM and HCPCS codes 2015 Contents Introduction... i CPT Anesthesia to Procedure Crosswalk...i Format...i Icon Key...ii CPT Codes...ii Resequenced
Anesthesia Cross Coder Essential links from CPT codes to ICD-9-CM and HCPCS codes 2015 Contents Introduction... i CPT Anesthesia to Procedure Crosswalk...i Format...i Icon Key...ii CPT Codes...ii Resequenced
Division of Registrations Gregory Ferland Interim Division Director. Corrected Notice of Proposed Rulemaking and Rulemaking Hearing
 Division of Registrations Gregory Ferland Interim Division Director State Physical Therapy Board Deann Conroy Program Director John W. H1ckenlooper Governor Barbara J. Kelley Executive Director Corrected
Division of Registrations Gregory Ferland Interim Division Director State Physical Therapy Board Deann Conroy Program Director John W. H1ckenlooper Governor Barbara J. Kelley Executive Director Corrected
Preservation of the First Ray in Patients with Diabetes
 Preservation of the First Ray in Patients with Diabetes Surgical approaches are often necessary to off-load excessive pressure. By Derek Ley, DPM, and Barry Rosenblum, DPM Introduction In approaching diabetic
Preservation of the First Ray in Patients with Diabetes Surgical approaches are often necessary to off-load excessive pressure. By Derek Ley, DPM, and Barry Rosenblum, DPM Introduction In approaching diabetic
Orthopedic Surgery Clinical Privilege List
 Description of Service Alberta Health Services (AHS) Medical Staff who are specialists in Orthopedic Surgery (or its associated subspecialties) and have privileges in the Section of Orthopedic Surgery
Description of Service Alberta Health Services (AHS) Medical Staff who are specialists in Orthopedic Surgery (or its associated subspecialties) and have privileges in the Section of Orthopedic Surgery
Bunionectomy-Forefoot Surgery
 Richard M. Marks, MD Professor and Director Division of Foot and Ankle Department of Orthopaedic Surgery Medical College of Wisconsin Explanation: Bunionectomy-Forefoot Surgery A bunion (also called hallux
Richard M. Marks, MD Professor and Director Division of Foot and Ankle Department of Orthopaedic Surgery Medical College of Wisconsin Explanation: Bunionectomy-Forefoot Surgery A bunion (also called hallux
Certification Guidelines: Credential Standards and Requirements Table
 Certification Guidelines: Credential Standards and Requirements Table Certified Recovery Peer Specialist (CRPS) Define Yourself as a Professional through Certification. 1715 S. Gadsden St. Tallahassee,
Certification Guidelines: Credential Standards and Requirements Table Certified Recovery Peer Specialist (CRPS) Define Yourself as a Professional through Certification. 1715 S. Gadsden St. Tallahassee,
Index. Clin Sports Med 23 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Lesser Toe Correction
 Richard M. Marks, MD Professor and Director Division of Foot and Ankle Department of Orthopaedic Surgery Medical College of Wisconsin Explanation: Lesser Toe Correction Lesser toe deformities are classified
Richard M. Marks, MD Professor and Director Division of Foot and Ankle Department of Orthopaedic Surgery Medical College of Wisconsin Explanation: Lesser Toe Correction Lesser toe deformities are classified
Instructions for Applicants. Successful completion of this examination is required as one of the conditions for licensure in the State of Vermont.
 Board of Dental Examiners Page 1 - Rev. 12/1/2010 Instructions for Applicants Successful completion of this examination is required as one of the conditions for licensure in the State of Vermont. 1. Use
Board of Dental Examiners Page 1 - Rev. 12/1/2010 Instructions for Applicants Successful completion of this examination is required as one of the conditions for licensure in the State of Vermont. 1. Use
Amputations of the digit, ray and midfoot
 Amputations of the digit, ray and midfoot Dane K. Wukich M.D. Chief, Division of Foot and Ankle Surgery Medical Director, UPMC Foot and Ankle Center University of Pittsburgh School of Medicine Disclosure
Amputations of the digit, ray and midfoot Dane K. Wukich M.D. Chief, Division of Foot and Ankle Surgery Medical Director, UPMC Foot and Ankle Center University of Pittsburgh School of Medicine Disclosure
Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy
 TheZenith's Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy Application: Zenith Insurance Company and Wholly Owned Subsidiaries Policy
TheZenith's Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy Application: Zenith Insurance Company and Wholly Owned Subsidiaries Policy
ABOS/CORD Surgical Skills Assessment Program
 American Board of Orthopaedic Surgery Establishing Education & Performance Standards for Orthopaedic Surgeons ABOS/CORD Surgical Skills Assessment Program ABOS Essential Knowledge, Skills, and Behaviors
American Board of Orthopaedic Surgery Establishing Education & Performance Standards for Orthopaedic Surgeons ABOS/CORD Surgical Skills Assessment Program ABOS Essential Knowledge, Skills, and Behaviors
CHARLOTTE Lisfranc. Recontruction System SURGICAL TECHNIQUE
 CHARLOTTE Lisfranc Recontruction System SURGICAL TECHNIQUE Contents Preface 3 Chapter 1 4 Chapter 2 4 4 4 4 4 Chapter 3 5 5 5 6 6 6 7 7 8 Chapter 4 8 8 9 10 Appendix 10 Introduction Indications and Contraindications
CHARLOTTE Lisfranc Recontruction System SURGICAL TECHNIQUE Contents Preface 3 Chapter 1 4 Chapter 2 4 4 4 4 4 Chapter 3 5 5 5 6 6 6 7 7 8 Chapter 4 8 8 9 10 Appendix 10 Introduction Indications and Contraindications
CHARLOTTE. 3.0 and 4.3 Multi-Use Compression Screws SURGIC A L T ECHNIQUE
 CHARLOTTE 3.0 and 4.3 Multi-Use Compression Screws SURGIC A L T ECHNIQUE CHARLOTTE 3.0 and 4.3 Multi-Use Compression Screws SURGICAL TECHNIQUE Surgical Technique as described by: Robert Anderson, MD Bruce
CHARLOTTE 3.0 and 4.3 Multi-Use Compression Screws SURGIC A L T ECHNIQUE CHARLOTTE 3.0 and 4.3 Multi-Use Compression Screws SURGICAL TECHNIQUE Surgical Technique as described by: Robert Anderson, MD Bruce
REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY
 C H A P T E R 2 1 REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY John V. Vanore, DPM INTRODUCTION Bunion surgery is frequently performed by foot and ankle surgeons. Generally, bunion surgery is quite predictable,
C H A P T E R 2 1 REPAIR OF THE DISPLACED AUSTIN OSTEOTOMY John V. Vanore, DPM INTRODUCTION Bunion surgery is frequently performed by foot and ankle surgeons. Generally, bunion surgery is quite predictable,
OTRF Athletic Trainer Residency Program Description and Curriculum
 OTRF Athletic Trainer Residency Program Description and Curriculum The Orthopaedic Surgery and Sports Medicine Teaching and Research Foundation (OTRF) residency program for athletic trainers is an educational
OTRF Athletic Trainer Residency Program Description and Curriculum The Orthopaedic Surgery and Sports Medicine Teaching and Research Foundation (OTRF) residency program for athletic trainers is an educational
Subcutaneous Tissues
 Podiatry Fee Schedule Effective January 1, 2013 The Base Fee listed below for each code is reimbursement for services rendered to adult recipients age 21 and over. To calculate the fee for children under
Podiatry Fee Schedule Effective January 1, 2013 The Base Fee listed below for each code is reimbursement for services rendered to adult recipients age 21 and over. To calculate the fee for children under
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abscess, in puncture wounds, 531 Absorbable fixation, for Lisfranc joint injuries, 556 Advanced glycosylation end products, complications due
Note: Page numbers of article titles are in boldface type. A Abscess, in puncture wounds, 531 Absorbable fixation, for Lisfranc joint injuries, 556 Advanced glycosylation end products, complications due
Legislative Counsel s Digest:
 Senate Bill No. 250 Senator Carlton (by request) CHAPTER... AN ACT relating to dentistry and dental hygiene; revising various provisions governing the qualifications, examination and licensure of dentists
Senate Bill No. 250 Senator Carlton (by request) CHAPTER... AN ACT relating to dentistry and dental hygiene; revising various provisions governing the qualifications, examination and licensure of dentists
AN ACT. The General Assembly of the Commonwealth of Pennsylvania hereby enacts as follows:
 Pennsylvania General Assembly http://www.legis.state.pa.us/cfdocs/legis/li/uconscheck.cfm?txttype=htm&yr=2014&sessind=0&smthlwind=0&act=89 07/17/2014 12:54 PM Home / Statutes of Pennsylvania / Unconsolidated
Pennsylvania General Assembly http://www.legis.state.pa.us/cfdocs/legis/li/uconscheck.cfm?txttype=htm&yr=2014&sessind=0&smthlwind=0&act=89 07/17/2014 12:54 PM Home / Statutes of Pennsylvania / Unconsolidated