Hip pain: A comparison of Osteoarthritis and Femoroacetabular Impingement Kristine Flais, PT, DPT
|
|
|
- Sherilyn Ferguson
- 5 years ago
- Views:
Transcription
1 Hip pain: A comparison of Osteoarthritis and Femoroacetabular Impingement Kristine Flais, PT, DPT

2 Most common cause of hip pain in older adults Prevalence of Hip OA
3 Age Gender Race Developmental disorders Genetics Occupation Sports exposure Previous injury Body mass index Leg length discrepancy Risk Factors

4 Entire joint structure is affected: Joint capsule shortening thickening& lengthening Osteophytes/spur development Sclerosis of subchondral bone Muscle weakness Pathoanatomical Features of OA

5 Joint space narrowing Osteophytes/spurs Subchondral sclerosis Imaging Findings
6 4 out of the 5 indicates a strong prediction of OA + LR 24.3: Probability of OA 91% Squatting increased symptoms Lateral hip pain with active hip FLEX Scour test with ADD causes lateral hip/groin pain Pain with active hip EXT PROM IR < to 25º Clinical prediction rule for OA

7 Patient profile: Greater than 60 y/o Pain description, location, behavior: Morning stiffness hip & groin Improves in less than an hour Lateral hip pain hip flexion weight bearing Posterior hip pain with squatting Aggravating factors: Walking Standing Squatting Stairs Kneeling Patient Profile
8 Assess hip ROM and joint mobility Limited passive hip joint motion in at least 3 of 6 motions Hip flexion < 115 Hip IR < 25º Examination

9 Assess hip strength SLR x 4 Hip IR/ER MMT Examination

10 Trendelenburg sign/ lurch om/watch?v=iueekzqs fmk&feature=player_d etailpage Examination

11 Patrick s test + if reproduces pt s sx om/watch?v=wpzbow KG7lc&feature=player _detailpage Examination

12 Scour test + scour test with adduction causes lateral hip or groin pain om/watch?v=wob2es GaPLM&feature=play er_detailpage Examination

13 OA progresses slowly with THR/THA the primary clinical endpoint Dependent upon the severity and progression of OA Prognosis

14 Patient Education Gait & Balance training Manual treatment Hip joint mobilizations Caudal glide with hip flexion Lateral glide with IR FABER mob Long Axis Distraction Interventions




15 Caudal glide with hip FL Lateral glide w/hip IR FABER mobilization Long-axis distraction Hip mobilizations
16 Exercise Stretching techniques of shortened muscles Aerobic conditioning Strengthening hip abductors Interventions

17 Single Knee to chest self mobilization technique

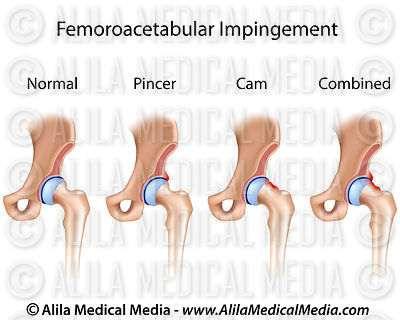
18 Abnormal contact between the femoral head/neck and the acetabular margin Femoroacetabular Impingement

19 Pincer impingement: Acetabular abnormalities Cam impingement: Femoral head/neck abnormalities Combination: Most common Categories of Impingement
20

21 Genetics Sex Pincer lesions y/o active women Cam impingement y/o athletic men Sports Hockey players Goalies Butterfly style Risk Factors

22 Pincer Impingement: Increase acetabular depth Coxa Profunda Acetabular Protrusion Decreased acetabular depth Acetabular retroversion Radiographic Findings

23 Cam Impingement: Increased femoral neck diameter Increased thickness of femoral head-neck junction Radiographic Findings

24 Patient profile: Healthy active y/o Involved in athletics Pain description, location, behavior: Anterior groin pain Sharp, catching, pinching C sign Aggravating factors: Running Excessive hip flexion Worst after/with sitting Squatting Twisting maneuvers Recumbent bike Patient Profile

25 Swayback posture Lengthened external oblique & iliopsoas Shortened rectus femoris and tensor fascia latae Disuse atrophy Gluteal musculature: Examination: Posture

26 Limited hip flexion, IR, &/or adduction compared to opposite side Insufficient posterior glide/joint play during hip flexion Examination: ROM

27 MMT: Iliopsoas, Gluteus medius, Gluteus maximus, Hamstrings, TFL Commonly iliopsoas long & weak TFL short Glut max short & weak Examination: Muscle Length/Strength

28 FADIR impingement test: Hip & knee flexion 90º combine with hip adduction and IR + sign sudden, sharp pain which replicates sx m/watch?feature=player_ detailpage&v=zde_0vn Pjkw Examination: Special Tests

29 Thomas test om/watch?v=nbrxinzvjs Ober s test om/watch?v=3iz57sm 17-M Examination: Special Tests

30 Forward Bending Single leg stance Single leg step down SLR hip extension Quadruped rock back Gait Analysis Walking & running Examination: Movement analysis

31 FAI is proposed to contribute to OA Surgical management Arthroscopic procedures Labral tear resection or repair Clinical Course

32 Physical Therapy Manual therapy Stretching Strengthening Neuromuscular Re-ed Activity modification: Avoid activities that place the hip joint in positions that create impingement End range flexion, internal rotation, and adduction Interventions

33 Improve ROM Hip mobs Strengthen hip musculature Prone hip extension with knee flexion Side-lying hip lateral rotation Side -lying hip abduction with ER Ckc: lunges, standing hip hikes, single leg squats, forward step ups Correct faulty movement patterns Increasing step rate Decreased hip extension at terminal Use softer surfaces Avoid treadmill or narrow trail Dynamic warm-up Do NOT run consecutive days for 1st month Cross train Conservation Treatment Goals
34 Hip OA Greater than 60 y/o Morning stiffness hip & groin Lateral hip pain with WB and/or hip flexion (Trendelenburg gait) Squatting increased symptoms Lateral hip pain with active hip FLEX Scour test with ADD causes lateral hip/groin pain Pain with active hip EXT PROM IR < or = to 25º FAI y/o Involved in athletics Anterior groin pain Sharp, catching, pinching No lateral thigh pain Worst after/with sitting Pinching Limited hip flexion, IR &/or adduction compared to opposite side +Impingement test (FADIR) Final Comparison
35 Questions?
36 1.Cibulka M, White D, Woehrle J, Harris-Hayes M, Enseki K, Fagerson T. Hip Pain and Mobility Deficits- Hip Osteoarthritis: Clinical Guidelines Linked to the International classification of Functioning, Disability and Health From the Orthopaedic Section of the American Physical Therapy Association. J Ortho Sports Phys Ther. 2009;A1-A25. 2.Cleland J, Koppenhaver S. Netter s Orthopaedic Clinical Examination:An Evidence- Based Approach. 2nd Edition. Elsevier, Inc Dooley, P. Femoroacetabular impingement syndrome. Canadian Family Physician. 2008;54: Enseki K, Harris-Hayes M, White D, Cibulka M, Woehrle J, Fagerson T. Nonarthritic Hip Joint:Clinical Guidelines Linked to the International classification of Functioning, Disability and Health From the Orthopaedic Section of the American Physical Therapy Association. J Ortho Sports Phys Ther. 2014;A1- A32. 5.Maslowski E, Sullivan W, Harwood J, Gonzalez P, Kaufman M, Vidal A. The Diagnostic Validity of Hi Provocation Maneuvers to Detect Intra-Articular Hip Pathology. PM R. 2010; 2: Sutlive T, Lopez H, Schnitker D, Yawn S, Halle R, Mansfield L. Development of a Clinical Prediction Rule for Diagnosing Hip Osteoarthritis in Individuals with Unilateral Hip Pain. J Ortho Sports Phys Ther. 2008; 38(9): Tibor L, Sekiya J. Differential Diagnosis of Pain Around the Hip Joint. Arthroscopy:The Journal of Arthroscopic and related Surgery. 2008; 24(12): MedBridge Education: Hip Osteoarthritis: An Evidence-Based Approach Ben Hando, PT, DSc, FAAOMPT References
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
HIP_CASE 2_OA. Hip Forces. Function of the Hip. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1
 HIP_CASE 2_OA Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT, OCS, FAAOMPT 62 yo female AM stiffness Hip pain diffuse, variable ant>lateral>post Gradual onset Tennis
HIP_CASE 2_OA Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT, OCS, FAAOMPT 62 yo female AM stiffness Hip pain diffuse, variable ant>lateral>post Gradual onset Tennis
CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT
 SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
SPORTS REHABILITATION CONSERVATIVE MANAGEMENT OF FEMOROACETABULAR IMPINGEMENT A case study and rationale for treatment Written by Joanne Kemp and Kay Crossley, Australia BACKGROUND The hip joint and FAI
Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Gluteus Medius Tear, Labral Tear, CAM / Pincer Procedure: Gluteus Medius Repair, CAM / Pincer Decompression, Labral refixation / Capsular Shift
The Focused Hip Examination of the Pre-arthritic, Athletic Patient. Adam Anz, MD Andrews Institute Gulf Breeze, Florida
 The Focused Hip Examination of the Pre-arthritic, Athletic Patient Adam Anz, MD Andrews Institute Gulf Breeze, Florida Correct Diagnosis: - 35% History - 30 % Physical Exam - 30% Plain X-rays - 5% MRI
The Focused Hip Examination of the Pre-arthritic, Athletic Patient Adam Anz, MD Andrews Institute Gulf Breeze, Florida Correct Diagnosis: - 35% History - 30 % Physical Exam - 30% Plain X-rays - 5% MRI
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies
 Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
Non-arthritic anterior hip pain in the younger patient: examination and intervention strategies Melodie Kondratek, PT, DScPT, OMPT Bryan Kuhlman, PT, DPT, OMPT Oakland University Orthopedic Spine and Sports
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
General Guidelines: Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic or Open Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace and crutches Weight-bearing:
A patient guide to Hip Impingement Non-Surgical Management. Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy
 A patient guide to Hip Impingement Non-Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Contents Page: 1 Cover 2 Contents 3 Hip impingement information 4 Conservative rehabilitation
A patient guide to Hip Impingement Non-Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Contents Page: 1 Cover 2 Contents 3 Hip impingement information 4 Conservative rehabilitation
Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement
 Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement Michael Newsome PT, OCS, SCS, CSCS Hip injuries account for 3.1% of all injuries in the NFL from 1997-2006 (Feeley 2008) 59% strains
Rehabilitation of Hip Labral Tears and Femoroacetabular Impingement Michael Newsome PT, OCS, SCS, CSCS Hip injuries account for 3.1% of all injuries in the NFL from 1997-2006 (Feeley 2008) 59% strains
Conservative Interventions for the Hip Region
 Anatomical Considerations Conservative Interventions for the Hip Region Shoulder vs. Hip RobRoy Martin, PhD PT Associate Professor Duquesne University Staff Physical Therapist UPMC/CRS Center for Sports
Anatomical Considerations Conservative Interventions for the Hip Region Shoulder vs. Hip RobRoy Martin, PhD PT Associate Professor Duquesne University Staff Physical Therapist UPMC/CRS Center for Sports
Travis G. - 1 Maak, - MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
Travis G. - 1 Maak, - MD Rehabilitation for Arthroscopic Osteochondroplasty with or without Labral Repair/Debridement General Guidelines: Normalize gait pattern with brace and crutches Continuous Passive
Hip Arthroscopy. Labral Repair/Debridement with Femoroplasty
 Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Precautions for weeks 1 4 post-op: Hip Arthroscopy Labral Repair/Debridement with Femoroplasty Patient Education o For 1 week, Assist the involved LE during all transfers o For 2 weeks, Do not sit with
Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement. Normalize gait pattern with brace (if indicated) and crutches
 and crutches") General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Effectiveness of Gluteal Muscle Strengthening in Patients with Hip Osteoarthritis: Review of the Literature. Patrick Idowu
 Effectiveness of Gluteal Muscle Strengthening in Patients with Hip Osteoarthritis: Review of the Literature Patrick Idowu Northern Illinois University Dr. Dawn Brown, PT, DPT, OCS December 8, 2017 ABSTRACT
Effectiveness of Gluteal Muscle Strengthening in Patients with Hip Osteoarthritis: Review of the Literature Patrick Idowu Northern Illinois University Dr. Dawn Brown, PT, DPT, OCS December 8, 2017 ABSTRACT
APTA Intro to Identity. The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee THE HUMAN MOVEMENT SYSTEM
 The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
Precautions following Hip Arthroscopy/FAI: (Refixation/Osteochondroplasty)
") Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, CAM / Pincer Procedure: Labral Repair / Capsular Shift, CAM / Pincer Decompression RX: Evaluate / Treat, and follow attached protocol
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Hip Arthroscopy Protocol
 The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
The intent of this protocol is to provide guidelines for progression of rehabilitation, it is not intended to serve as a substitute for clinical decision making. Progression through each phase of rehabilitation
Hip Cases from Clinic: Refining your history and physical
 Hip Cases from Clinic: Refining your history and physical Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery 11/20/2017 Case #1 Healthy 21 M College
Hip Cases from Clinic: Refining your history and physical Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery 11/20/2017 Case #1 Healthy 21 M College
What s Hip: Common Hip Problems and Kids and Adults
 What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
Labral Tears / Femoro- Acetabular Impingement / Hip Arthroscopy/THA. Dr Allen Turnbull Hip and Knee Surgery
 Labral Tears / Femoro- Acetabular Impingement / Hip Arthroscopy/THA Hip Anatomy Labrum Fovea Femoral Head Articular Cartilage Ligamentum Teres Labral Tears Function of Labrum Deepens acetabulum by 20%
Labral Tears / Femoro- Acetabular Impingement / Hip Arthroscopy/THA Hip Anatomy Labrum Fovea Femoral Head Articular Cartilage Ligamentum Teres Labral Tears Function of Labrum Deepens acetabulum by 20%
Overview. Overview. Introduction. Introduction Anatomy History Examination Common Disorders. Introduction Anatomy History Examination Common Disorders
 Common Hip Disorders in Figure Skaters 14 th Annual Meeting of Sports Medicine and Science in Figure Skating January 25, 2009 8:15-8:45am Robert J. Dimeff, MD Medical Director of Sports Medicine Overview
Common Hip Disorders in Figure Skaters 14 th Annual Meeting of Sports Medicine and Science in Figure Skating January 25, 2009 8:15-8:45am Robert J. Dimeff, MD Medical Director of Sports Medicine Overview
CLINICS IN SPORTS MEDICINE
 Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
Clin Sports Med 25 (2006) 365 369 CLINICS IN SPORTS MEDICINE A Acetabular labrum, tears of, hip arthroscopy in, 264 Acetabular rim, trimming of, and labral repair, new method for, 293 297 Acetabulum, femoral
Travis G. Maak, MD Sports Medicine University of Utah Orthopaedics 590 Wakara Way Salt Lake City, UT Tel: Fax:
 General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
General Guidelines: Hip Arthroscopy Rehabilitation Capsular Shift with or without FAI Labral Components No external rotation greater than 30 degrees for 4 weeks No hyperextension for 4 weeks Normalize
Hip Injuries & Arthroscopy in Athletes
 Hip Injuries & Arthroscopy in Athletes John P Salvo, MD Sports Medicine Rothman Institute Philadelphia, PA EATA Annual Meeting January, 2011 Hip Injuries & Arthroscopy in Anatomy History Physical Exam
Hip Injuries & Arthroscopy in Athletes John P Salvo, MD Sports Medicine Rothman Institute Philadelphia, PA EATA Annual Meeting January, 2011 Hip Injuries & Arthroscopy in Anatomy History Physical Exam
The Young Adult Hip: FAI. Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California
 The Young Adult Hip: FAI Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California Introduction Femoroacetabular Impingment(FAI) Presentation and Exam Imaging Surgical Management
The Young Adult Hip: FAI Jason Snibbe, M.D. Snibbe Orthopedics Team Physician, University of Southern California Introduction Femoroacetabular Impingment(FAI) Presentation and Exam Imaging Surgical Management
STAIRS. What s Hip: Top 5 Hip Problems in Primary Care. I have no relevant disclosures. Top 5 (or 6) Pathologies. Big 3- Questions to Ask
 Pathologies. Big 3- Questions to Ask") I have no relevant disclosures. What s Hip: Top 5 Hip Problems in Primary Care Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery December, 2015
I have no relevant disclosures. What s Hip: Top 5 Hip Problems in Primary Care Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery December, 2015
Young Adult Hip problems. Aresh Hashemi-Nejad FRCS(Orth)
") Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair
 Repair") UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Open Hip Abductor (Gluteus Medius) Repair The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket which is from
Hip Arthroscopy Labral Repair Protocol
 Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Hip Arthroscopy Labral Repair Protocol Applicability: Physician Practices Date Effective: 09/2013 Department: Rehabilitation Services Date Last Reviewed: 1/2018 Supersedes: n/a Administration Approval:
Bryan T. Kelly, MD Center for Hip Pain and Preservation Hospital for Special Surgery
 Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Hip Arthroscopy Rehabilitation Labral refixation with or without FAI Component General Guidelines: Limited external rotation to 20 degrees (2 weeks) No hyperextension (4 weeks) Normalize gait pattern with
Objectives. Objectives 9/26/2017. Evaluation and Rehab Management of the Patient with Hip Pain
 Evaluation and Rehab Management of the Patient with Hip Pain Joe Tupta, PT, OCS WPTA Fall Conference October 13 th, 2017 jtupta@uwhealth.org Objectives Screen the hip and adjacent regions for dysfunction
Evaluation and Rehab Management of the Patient with Hip Pain Joe Tupta, PT, OCS WPTA Fall Conference October 13 th, 2017 jtupta@uwhealth.org Objectives Screen the hip and adjacent regions for dysfunction
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit. Evaluation and Diagnosis of Osteoarthritis in Primary Care
 Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer. Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement
 Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
Physical Therapy Prescription: Hip Arthroscopy Diagnosis: Labral Tear, Internal Snapping Hip, CAM / Pincer Procedure: Partial Psoas Release with CAM / Pincer Decompression and Labral Debridement RX: Evaluate
Rehabilitation. Friday, October 14, :00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA
 Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
Rehabilitation Friday, October 14, 2011 11:00 11:45am General Session Rehabilitation following FAI Surgery Mark Ryan, MS, ATC, CSCS USA Best Tip Srino Bharam, MD USA Best Tip Robroy Martin, PhD, PT USA
Alejandro Verdugo, M.D.
 Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Alejandro Verdugo, M.D. Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016
 Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Hip Pain in Adults: Evaluation 67th Annual McGill Refresher Course for Family Physicians Dec6/2016 David J Zukor MD FRCSC Chief Department of Orthopedic Surgery SMBD-Jewish General Hospital Associate Professor
Bone Bangalore
 Dr Suresh Annamalai MBBS, MRCS(Edn), FRCS( Tr & Orth)(Edn), FEBOT(European Board), Young Hip and Knee Fellowship(Harrogate, UK) HOD & Consultant Arthroplasty and Arthroscopic Surgeon Manipal Hospital,
Dr Suresh Annamalai MBBS, MRCS(Edn), FRCS( Tr & Orth)(Edn), FEBOT(European Board), Young Hip and Knee Fellowship(Harrogate, UK) HOD & Consultant Arthroplasty and Arthroscopic Surgeon Manipal Hospital,
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals Precautions:
: Goals Precautions:") Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
Phase 1- Immediate Rehabilitation (1-3 weeks): Goals: Protection of the repaired tissue Prevent muscular inhibition and gait abnormalities Diminish pain and inflammation Precautions: 20 lb. flat-foot weight-bearing
BENJAMIN G. DOMB, MD
 Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
Physical Therapy Protocol Partial or full thickness gluteus medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is
BENJAMIN G. DOMB, M.D.
 Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Arthroscopic Hip Surgery Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment. We
Femoroacetabular Impingement in the Throwing Athlete. Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute
 Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
Femoroacetabular Impingement in the Throwing Athlete Michael Banffy, MD Sports Medicine, Hip Preservation Kerlan Jobe Institute Disclosures None Baseball Hip Injuries - Background Abdominal/groin injuries
Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component. Limited external rotation to 20 degrees (2 weeks)
") General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
General Guidelines: 4140 Centennial Hills Boulevard Casper, WY 82609 (307) 265-7205 Hip Arthroscopy Rehabilitation Labral Refixation with or without FAI Component Limited external rotation to 20 degrees
The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the
, obesity, and previous knee trauma or surgery. OA affects usually the") The Arthritic Knee The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the medial compartment of the knee, and
The Arthritic Knee The causes of OA of the knee are multiple and include aging (wear and tear), obesity, and previous knee trauma or surgery. OA affects usually the medial compartment of the knee, and
Rehabilitation Considerations Following Surgical Arthroscopy of the Hip. Joy Anderson PT, ATC, CSCS
 Rehabilitation Considerations Following Surgical Arthroscopy of the Hip Joy Anderson PT, ATC, CSCS 1 Best Rehab Program? Review of the Evidence paucity of evidence surrounding post-operative rehabilitation
Rehabilitation Considerations Following Surgical Arthroscopy of the Hip Joy Anderson PT, ATC, CSCS 1 Best Rehab Program? Review of the Evidence paucity of evidence surrounding post-operative rehabilitation
A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report
 58 Case Report A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report Jun-hyeok Jang, Ph.D., PT, Professor 1 ; In-cheol Jeon,
58 Case Report A Movement-System-Impairment Approach to the Evaluation and Treatment of a Patient with Femoral Anterior Glide Syndrome: A Case Report Jun-hyeok Jang, Ph.D., PT, Professor 1 ; In-cheol Jeon,
Initial Exercises (Weeks 1-3)
") Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Labral Repair This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Partial weight bearing (50%) (4 weeks). Encourage, but limit hip
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty. Faculty Disclosures. Objectives 11/17/2017
 Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Impingement and Arthritis: Preservation vs. Total Hip Arthroplasty Jonathan R. Schiller, MD Assistant Professor of Orthopedics Warren Alpert Medical School of Brown University Director, Adolescent
Hip Region. PHTY2020: Lecture
 Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Post Operative Hip Arthroscopy Rehabilitation Protocol Dr. David Hergan Labral Repair with or without FAI Component Initial Joint Protection Guidelines- (P.O. Day 1-4 wks): Joint Protection Patient education
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 Hip Arthroscopy - FAI/Labral Repair Protocol The hip is a ball and
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 Hip Arthroscopy - FAI/Labral Repair Protocol The hip is a ball and
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component
 Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
Post Operative Hip Arthroscopy Rehabilitation Protocol Labral Repair With or Without FAI Component ROM Restrictions: -Perform PROM in patient s PAIN FREE Range FLEXION EXTENSION EXTERNAL ROTATION 90 degrees
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
ARTHROSCOPIC GLUTEUS MEDIUS REPAIR PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use appropriate clinical
11/11/2016. Hip FAI & Core Muscle Deficiency: Diagnosis and Treatment. Disclosures. Differential Diagnosis. Consultant, Smith and Nephew
 Hip FAI & Core Muscle Deficiency: Diagnosis and Treatment FORE Baseball Sports Medicine Game-Changing Concepts November 4, 2016 T. Sean Lynch, MD Assistant Professor New York-Presbyterian/ Columbia University
Hip FAI & Core Muscle Deficiency: Diagnosis and Treatment FORE Baseball Sports Medicine Game-Changing Concepts November 4, 2016 T. Sean Lynch, MD Assistant Professor New York-Presbyterian/ Columbia University
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Tears/FAI. Andrew Parker, MD
 Labral Tears/FAI Andrew Parker, MD Athletic Hip Injuries Incidence of hip injuries has increased dramatically over the last decade In part due to better recognition with improved imaging and arthroscopy,
Labral Tears/FAI Andrew Parker, MD Athletic Hip Injuries Incidence of hip injuries has increased dramatically over the last decade In part due to better recognition with improved imaging and arthroscopy,
The Evaluation of Hip pain in the Athlete
 The Evaluation of Hip pain in the Athlete DREW ROGERS,MD The Evaluation of Hip pain in the Athlete Andrew Rogers, MD (Drew) Orthopedic Care Physician Network Chief of Orthopedics Morton Hospital Team Physician
The Evaluation of Hip pain in the Athlete DREW ROGERS,MD The Evaluation of Hip pain in the Athlete Andrew Rogers, MD (Drew) Orthopedic Care Physician Network Chief of Orthopedics Morton Hospital Team Physician
Rehabilitation Guidelines for Hip Arthroscopy Procedures
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Hip Arthroscopy Procedures The hip joint is composed of the femur (the thigh bone), and the acetabulum (the socket which is from the three
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Hip Arthroscopy Procedures The hip joint is composed of the femur (the thigh bone), and the acetabulum (the socket which is from the three
Movement System Diagnoses. Movement System Impairment Syndromes of the Lumbar Spine. MSI Syndrome - Assumptions. Return From Forward Bending
 Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
Movement System Diagnoses Kinesiopathologic Pathokinesiologic Movement System Impairment Syndromes of the Lumbar Spine Shirley Sahrmann, PT, PhD, FAPTA Washington University St. Louis School of Medicine
JOHN M. REDMOND, M.D.
 Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Physical Therapy Protocol Gluteus Medius repair with or without labral repair The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip
 of the Hip") A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Femoroacetabular Impingement (FAI) of the Hip 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
Diagnostic Approach to Hip Pain. Zoë J. Foster, MD October 3, 2018
 Diagnostic Approach to Hip Pain Zoë J. Foster, MD October 3, 2018 Disclosures I have nothing to disclose. Objectives Review examination of the hip, including special tests Discuss differential diagnosis
Diagnostic Approach to Hip Pain Zoë J. Foster, MD October 3, 2018 Disclosures I have nothing to disclose. Objectives Review examination of the hip, including special tests Discuss differential diagnosis
Hip Conditioning Program
 Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
Prepared for: Prepared by: Purpose of Program After an injury or surgery, an exercise conditioning program will help you return to daily activities and enjoy a more active, healthy lifestyle. Following
7/14/18 OBJECTIVE WHAT IS LOWER CROSSED SYNDROME?
 LOWER CROSSED SYNDROME: A DIFFERENTIAL DIAGNOSIS FOR LOW BACK PAIN Kimberly Hansen ATC, LAT, CES Industrial Sports Medicine Professional with InSite Health Committee on Practice Advancement District 7
LOWER CROSSED SYNDROME: A DIFFERENTIAL DIAGNOSIS FOR LOW BACK PAIN Kimberly Hansen ATC, LAT, CES Industrial Sports Medicine Professional with InSite Health Committee on Practice Advancement District 7
Evaluation of the Hip
 Evaluation of the Hip Adam Lewno, DO PCSM Fellow, University of Michigan Primary Care Sports Update 2017 Disclosures Financial: None Images: I would like to acknowledge the work of the original owners
Evaluation of the Hip Adam Lewno, DO PCSM Fellow, University of Michigan Primary Care Sports Update 2017 Disclosures Financial: None Images: I would like to acknowledge the work of the original owners
Hip Arthroscopy. Christopher J. Utz, MD. Assistant Professor of Orthopaedic Surgery University of Cincinnati
 Hip Arthroscopy Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. Brief History 2. Review of
Hip Arthroscopy Christopher J. Utz, MD Assistant Professor of Orthopaedic Surgery University of Cincinnati Disclosures I have no disclosures relevant to this topic. Outline 1. Brief History 2. Review of
HIP ARTHROSCOPY CLINICAL PRACTICE GUIDELINE
 HIP ARTHROSCOPY CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio State Sports Medicine
HIP ARTHROSCOPY CLINICAL PRACTICE GUIDELINE Progression is time and criterion-based, dependent on soft tissue healing, patient demographics and clinician evaluation. Contact Ohio State Sports Medicine
HIP EVALUATION. LBP_Cancer Rules. Differential Diagnosis non MSK. Property of VOMPTI, LLC
 HIP EVALUATION Eric Magrum DPT OCS FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History Initial Hypothesis from Body chart/intake info Symptom onset Pain description
HIP EVALUATION Eric Magrum DPT OCS FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Subjective History Initial Hypothesis from Body chart/intake info Symptom onset Pain description
Rehabilitation Guidelines for Hip Arthroscopy Procedures
 UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Hip Arthroscopy Procedures The hip joint is composed of the femur (the thigh bone), and the acetabulum (the socket which is from the three
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines for Hip Arthroscopy Procedures The hip joint is composed of the femur (the thigh bone), and the acetabulum (the socket which is from the three
Hip Arthroscopy: State of the Art
 Hip Arthroscopy: State of the Art Seung J. Yi Florida Orthopaedic Institute Orthopaedics for Primary Care and Therapists ER HPI 24 yo F R hip pain x 4 months after twisting injury in flag football C sign
Hip Arthroscopy: State of the Art Seung J. Yi Florida Orthopaedic Institute Orthopaedics for Primary Care and Therapists ER HPI 24 yo F R hip pain x 4 months after twisting injury in flag football C sign
CENTER FOR ORTHOPAEDICS AND SPINE CARE PHYSICAL THERAPY PROTOCOL ACUTE PROXIMAL HAMSTRING TENDON REPAIR BENJAMIN J. DAVIS, MD
 Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
Weeks 0-6 Goal: 1) Protection of the surgical repair Precautions: 1) Non-weight bearing with crutches for 6 weeks with foot flat or with knee Knee flexed to 90 degrees with sitting 2) No active hamstring
CAPPAGH NATIONAL ORTHOPAEDIC HOSPITAL, FINGLAS, DUBLIN 11. The Sisters of Mercy. Hip Arthroscopy
 1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
1.0 Policy Statement... 2 2.0 Purpose... 2 3.0 Scope... 2 4.0 Health & Safety... 2 5.0 Responsibilities... 2 6.0 Definitions and Abbreviations... 3 7.0 Guideline... 3 7.1 Rehabilitation Phase 1 (Day 1
Knee Capsular Disorder. ICD-9-CM: Stiffness in joint of lower leg, not elsewhere classified
 1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
Disclosures. Objectives. Overview. Patellofemoral Syndrome. Etiology. Management of Patellofemoral Pain
 Management of Patellofemoral Pain Implications of Top Down Mechanics Disclosures I have no actual or potential conflict of interest in relation to this presentation David Nolan, PT, DPT, MS, OCS, SCS,
Management of Patellofemoral Pain Implications of Top Down Mechanics Disclosures I have no actual or potential conflict of interest in relation to this presentation David Nolan, PT, DPT, MS, OCS, SCS,
FAI syndrome with or without labral tear.
 Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Case This 16-year-old female, soccer athlete was treated for pain in the right groin previously. Now has acute onset of pain in the left hip. The pain was in the groin that was worse with activities. Diagnosis
Sports Medicine and Radiology
 Sports Medicine and Radiology The judicious utilization of a thorough history and physical examination and appropriately applied imaging studies will allow for accurate diagnosis and treatment of athletic
Sports Medicine and Radiology The judicious utilization of a thorough history and physical examination and appropriately applied imaging studies will allow for accurate diagnosis and treatment of athletic
Post Operative Hip Arthroscopy Procedure Form
 Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Post Operative Hip Arthroscopy Procedure Form Femoracetabular Impingement (FAI) Femoral Osteochondroplasty Acetabular Rim Trimming Acetabular Labrum Repair Location: o clock to o clock Debridement Articular
Internal Rotation (turning toes/knee toward other leg) 30 degree limit. limit
 30 degree limit. limit") Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component. Normalize gait pattern with brace and crutches
 Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Hip Arthroscopy Rehabilitation Labral Debridement with or without FAI Component General Guidelines: Normalize gait pattern with brace and crutches Weightbearing as per procedure performed Continuous Passive
Presented by : Frank Filice (PT) London Health Sciences Centre
 London Health Sciences Centre") Total Hip Arthroplasty Presented by : Frank Filice (PT) London Health Sciences Centre June 20, 2008 Purpose Provide information that explains the rationale for the post-op precautions. Provide some general
Total Hip Arthroplasty Presented by : Frank Filice (PT) London Health Sciences Centre June 20, 2008 Purpose Provide information that explains the rationale for the post-op precautions. Provide some general
Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip
 Of The Hip") UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket formed by
UW HEALTH SPORTS REHABILITATION Rehabilitation Guidelines For Periacetabular Osteotomy (PAO) Of The Hip The hip joint is composed of the femur (the thigh bone) and the acetabulum (the socket formed by
Specialists in Joint Replacement, Spinal Surgery, Orthopaedics and Sport Injuries. The Hip.
 Specialists in Joint Replacement, Spinal Surgery, Orthopaedics and Sport Injuries The Hip INTRODUCTION THE HIP The hip is a ball-and-socket joint. The socket is formed by the acetabulum, which is part
Specialists in Joint Replacement, Spinal Surgery, Orthopaedics and Sport Injuries The Hip INTRODUCTION THE HIP The hip is a ball-and-socket joint. The socket is formed by the acetabulum, which is part
Hip Labrum and FAI Post-Surgical Rehabilitation Guideline
 Hip Labrum and FAI Post-Surgical Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Hip Labrum and FAI Post-Surgical Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for rehabilitation
Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme
 Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
Chapter FOUR Exercise Therapy for Patients with Knee OA Knee Exercise Protocol Knee Home Exercise Programme Chris Higgs Cathy Chapple Daniel Pinto J. Haxby Abbott 99 n n 100 General Guidelines Knee Exercise
Total Hip Replacement Rehabilitation: Progression and Restrictions
 Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular rim during normal hip range of motion.
 RIM SYNDROME [femoroacetabular impingement] It has been suggested to be a preosteoarthritic mechanism. The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular
RIM SYNDROME [femoroacetabular impingement] It has been suggested to be a preosteoarthritic mechanism. The condition occurs when the proximal femur repeatedly comes into contact with the native acetabular
Gluteal Strengthening Exercises: A Review of the Literature
 Common Imbalances Female Athlete Hip Injuries: Exploring the CORE of Patterns and Prevention Kelly McInnis, DO Irene Davis, PhD, PT, FAPTA, FACSM, FASB David Nolan, PT, DPT, MS, OCS, SCS, CSCS Gluteal
Common Imbalances Female Athlete Hip Injuries: Exploring the CORE of Patterns and Prevention Kelly McInnis, DO Irene Davis, PhD, PT, FAPTA, FACSM, FASB David Nolan, PT, DPT, MS, OCS, SCS, CSCS Gluteal
Test-retest. The therapist can perform test: retest procedures throughout the treatment session as required.
 HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
A patient guide to Hip Impingement Surgical Management
 A patient guide to Hip Impingement Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Patient Name: Occupation: Operation / Restrictions: Work/Sport: Contents Page: 1 Cover 2 Contents
A patient guide to Hip Impingement Surgical Management Mr Sanjeev Patil Miss Louise Duncan Mr Frank Gilroy Patient Name: Occupation: Operation / Restrictions: Work/Sport: Contents Page: 1 Cover 2 Contents
DISTANCE RUNNER MECHANICS AMY BEGLEY
 DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
Presentation Overview 8/8/12. Muscle Imbalances Revealed Assessment & Exercise for Personal Training
 Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Presentation Overview Common issues seen in many athletes from different sports Some important assessments that can be used for many varieties of athletes Exercise progressions that can fix imbalances
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
A Patient s Guide to Labral Tears of the Hip
 A Patient s Guide to Labral Tears of the Hip 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Labral Tears of the Hip 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled from a variety