Early treatment of birth palsy
|
|
|
- Theresa Davis
- 5 years ago
- Views:
Transcription

1 Early treatment of birth palsy The Hong King Society for Surgery of the Hand Dr. W.L.TSE Department of Orthopaedics & Traumatology Prince of Wales Hospital WL Tse

2 Early management how?
3 Early management: crucial points Detail Documentation Appropriate Investigation Start Therapy ASAP
4 Documentation Assessment tools Mallet score Active Movement Scale Gilbert & Tassin grading Paediatric Outcome Data Collection Instrument
5 DDX Pseudo paralysis of fracture clavicle/humerus Infection CNS injury Neuromuscular disorders Congenital anomalies of upper limb
6 Muscle grading Gilbert & Tassin 1987 Observation No contraction Contraction without movement Movement with weight eliminated Complete movement Muscle grade M0 M1 M2 M3

7 Mallet Score Gilbert modification 1993
8 Active Movement Scale Clarke & Cutis, Hospital for Sick Children 1995 Gravity eliminated No contraction 0 Contraction, no motion Score 1 <50% motion 2 >50% motion 3 Full 4 Against gravity <50% motion 5 >50% motion 6 Shoulder Elbow Forearm Wrist Finger Thumb Abd Add Flexion ER IR Flexion Extension Flexion Extension Pronation Supination Flexion Extension Flexion Extension Flexion Extension
9 Sensory grading Narakas 1987 Observation No reaction to pain stimuli Reaction to pain but not touch Reaction to touch but not light touch Apparently normal sensation Sensory Grade S0 S1 S2 S3
10 Candidate for Surgery? Nature /pattern of palsy Expected Time of recovery

11 Types of injury and prognosis Avulsion Rupture Traction
12 Clinical categories (Narakas & Slooff 1987, 1993) Group lesion Clinical Incidence Prognosis I C5C6 Erb s 46% 90% spontaneous recover II C5C6C7 Waiter s tip posture 29% Less predictable, Poorer III C5 T1 Fail limb 25% Poor IV C5 T1 + Horner Fail limb with Horner s sign Very poor

13 Pre- ganglionic Horner s Elevated diaphragm Winged scapula Absent rhomboid Absent supraspinatus Absent LD Sympathetic ganglion Phrenic n Long thoracic n Dorsal scapular n Suprascapula n Throacodorsal n

14 Investigation Plain radiograph of CXR, humerus High resolution MRI Electrophysiological studies
15 Physical therapy Goals To educate caregiver in handling, positioning & ADL To improve & maintain ROM To improve & maintain muscle strength To improve sensation To gain milestones and age appropiate skills To prevent joint contracture & Deformities


16 Physical Therapy should start ASAP Advice on positioning


17 Passive joint motion with scapula stablized Strengthening & stimulating sensation


18 Joint compression & loading Bimanual task & play
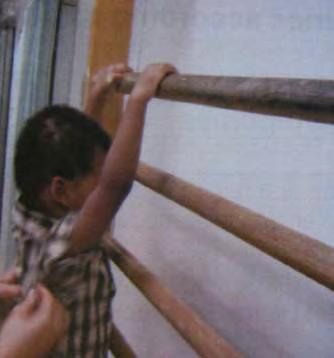
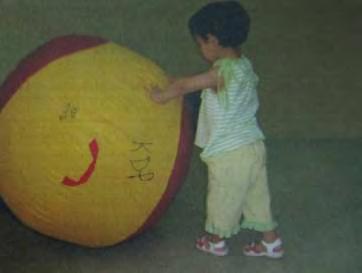
19 Age appropriate skills

20 Hand, wrist, elbow splints
21 Timing & Indication for early surgery Time Clinical examine 2 3 months Total plexus palsy with Horner s syndrome 3 6 months Upper trunk lesion with no antigravity elbow flexion 9 months Cookie s test positive


22 Cookie test at 9 months old Clarke & Cutis

23 Surgery: Microsurgery Neurolysis with nerve grafting Nerve Transfer
24 Microsurgery General stragerty: Nerve graft for intact roots Nerve Transfer if not enough healthy roots Priority: Hand>wrist >elbow>shoulder ( XI, ICN2 6, contralateral C7, hypoglossal, branch of UN, RN )


25 Neurolysis No role in avulsion injury May be useful if >50% muscle action potential across a neuroma in continuity Upper trunk SCN C 5 Upper trunk

26 Neuroma resection and nerve grafting
 anterior division /")

27 Upper trunk C5C6+/-C7 rupture: neuroma resection with sural nerve graft C5 6 >SNG > Upper trunk (UT) anterior division / Lateral cord / MCN elbow flexion SCN shoulder ER UT posterior division / posteror cord / axillary / RN elbow & wrist extension






28 Upper trunk C5C6 rupture: nerve transfer XI branch > SCN shoulder ER ICNs/UN branch to MCN elbow flexion Triceps LH branch >axillary n elbow extension

29 Partial / Total plexus avulsion: multiple transfers from: XI ICN 2 6 Contralateral C7 Hypoglossal nerve
30 How often is operations for OBPI performed? NTEC data ( only PWH has PICU support ) Between 1988 to April 2011 (23 years) 23 children operated 45 major/ultra major operations performed 6 children received operation before 1 year old at PWH
31 8 patients received > 1 operations No. of patients 1 operation 13 2 operations 4 3 operations 4 4 operations 1 6 operations 1 TOTAL 23
32 Dermographics ( n=23 ) M: F=11:12 Right 15 / Left 8 Erb s ( C5C6 +/ C7): 16 Whole plexus: 7 Exploration performed in 9 patients and document 4 patients with root avulsions
33 Microsurgical procedures performed: Nerve grafting alone in 2 patients Nerve transfer in 5 patients with 2 of them require grafting Free muscle (gracilis )transfer: 4
34 Donar No. of patients Recipient XI 2 UT(x2), SCN ICNs 5 MCN (x4), TDN, MN Cervical plexus Contralateral C7 VUNG 1 C5 1 MN
35 Other reconstructive procedures Muscle /tendon transfer : 14 patients De rotational osteotomy of radius: 2 Arthroscopic shoulder release: 3 Arthroscopic elbow release: 1
36 Case examples Ching Ching, girl FTNSD BW 7.31 lb No record of shoulder dystocia Apgar score 1(8),5(10) Failed right upper limb at birth


37 5 month old No Horner M1 shoulder abduction M2 biceps Flickering of middle finger flexion MRI: normal

38 Exploration at 5 months old Grossly swollen Upper, middle trunk with thick swollen Lower trunk Neurolysis reveal healthy fascicles in continuity within LT

39 32 months old
40 Ka Lok Boy FTNSD Shoulder dystocia Left Erb s palsy Exploration at 2 year old noted rupture C5, C6 Sural nerve grafting C5C6 to Upper trunk done



41



42 16 years post grafting


43 M/18 Total plexus injury with contralateral C7 transfer done at Huashan Hospital, Shanghai Chi ming Elbow flexion 5/5 Floppy wrist and fingers with no active control

44 Surgical procedure 2 team approach Donor site Recipient site



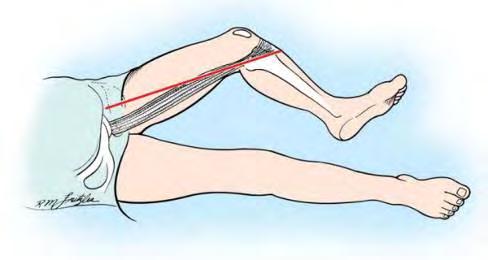
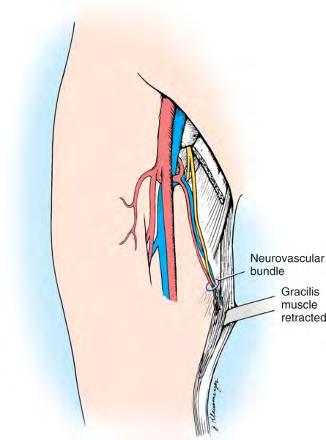
45 DONOR Site


46 Recipient site Identify 2 branches from MCN to brachialis muscle Nerve stimulator to confirm motor f(x)


47 Anastomosis - Brachial artery - Deep brachial vein/cutaneous vein - Nerve Vein Artery Nerve Vein



48 Muscle anchored with mitek at supracondylar region Gracilis tendon splitted and transferred to FDPs and FPL with Pulvertaft technique




49 Results Re innervation of graft Finger flexion +ve in all 3 cases 6 months




50 Results Hook Grip holding briefcase and shopping bag

51 Most Important point in early management of Birth Palsy Establish Rapport

52 Rapport Child Parents Family PRO?!
53 See consultation & referral ASAP Close FU Multi Disciplinary Approach Emphasis the role & participation of the Family Medical and psychological support throughout children s development
54 Bring home message Birth palsy is a potential devastating condition that give profound impact to the patient and the family Early establishment of good rapport form the foundation for the family to comply with the rehabilitation Early surgical intervention achieve better outcome for those with delayed neurological recovery
55 Thank you
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH
 Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
BPBP. Brachial Plexus Birth Palsy BPBP BPBP 11/2/2015. Traction or compression injury during birth. ~ 1 : 1000 live births R > L (LAO presentation)
") Brachial Plexus Birth Palsy Donald S. Bae, MD Boston Children s Hospital BPBP Traction or compression injury during birth ~ 1 : 1000 live births R > L (LAO presentation) Risk factors: macrosomia, difficult
Brachial Plexus Birth Palsy Donald S. Bae, MD Boston Children s Hospital BPBP Traction or compression injury during birth ~ 1 : 1000 live births R > L (LAO presentation) Risk factors: macrosomia, difficult
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Yorkshire and Humber Neonatal ODN (South) Clinical Guideline
 Clinical Guideline") Yorkshire and Humber Neonatal ODN (South) Clinical Guideline Title: Author: NEONATAL BRACHIAL PLEXUS INJURY Rebecca Musson Date written: January 2011, reviewed January 2016 Review date: January 2019 This
Yorkshire and Humber Neonatal ODN (South) Clinical Guideline Title: Author: NEONATAL BRACHIAL PLEXUS INJURY Rebecca Musson Date written: January 2011, reviewed January 2016 Review date: January 2019 This
Brachial Plexopathy in a Division I Football Player
 www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery
 Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
 Nerve Compression Syndromes Median Nerve Carpal Tunnel Syndrome Pronator Syndrome Ulnar Nerve Cubital Tunnel Syndrome Ulnar Tunnel Syndrome TOS www.fisiokinesiterapia.biz Carpal Tunnel Syndrome (CTS) Definition
Nerve Compression Syndromes Median Nerve Carpal Tunnel Syndrome Pronator Syndrome Ulnar Nerve Cubital Tunnel Syndrome Ulnar Tunnel Syndrome TOS www.fisiokinesiterapia.biz Carpal Tunnel Syndrome (CTS) Definition
If head is rapidly forced away from shoulder the injury is generally at C5,C6. If arm is rapidly abducted the lesion is generally at C8-T1.
 BRACHIAL PLEXUS Etiology Generally caused by MVA in adults. Generally males aged 15 to 25 years old. Naracas: Rule of seven seventies. 70% occur secondary to MVA; 70% involve motorcycles or bicycles. 70%
BRACHIAL PLEXUS Etiology Generally caused by MVA in adults. Generally males aged 15 to 25 years old. Naracas: Rule of seven seventies. 70% occur secondary to MVA; 70% involve motorcycles or bicycles. 70%
Repair of Severe Traction Lesions of the Brachial Plexus
 Repair of Severe Traction Lesions of the Brachial Plexus LAURENT SEDEL, M.D. Since 1972, the author has performed 259 brachial plexus repairs and various associated secondary procedures. The best results
Repair of Severe Traction Lesions of the Brachial Plexus LAURENT SEDEL, M.D. Since 1972, the author has performed 259 brachial plexus repairs and various associated secondary procedures. The best results
Management of Brachial Plexus & Peripheral Nerves Blast Injuries. First Global Conflict Medicine Congress
 Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Neonatal brachial plexus palsy: From conservative management to nerve reconstruction
 Current Practice Neonatal brachial plexus palsy: From conservative management to nerve reconstruction K A Nihal Gunatillaka 1 Sri Lanka Journal of Child Health, 2005; 34: 52-5 (Key words: brachial plexus
Current Practice Neonatal brachial plexus palsy: From conservative management to nerve reconstruction K A Nihal Gunatillaka 1 Sri Lanka Journal of Child Health, 2005; 34: 52-5 (Key words: brachial plexus
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES
 PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES Introduction As such, protocols in the management of brachial plexus injuries (BPI) are a bit of a misnomer. This
PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES Introduction As such, protocols in the management of brachial plexus injuries (BPI) are a bit of a misnomer. This
Gross Anatomy Questions That Should be Answerable After October 27, 2017
 Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Plastic Surgery - Cyber Lectures. Brachial Plexus Injuries Dr. Ashok K. Gupta
 Plastic Surgery - Cyber Lectures Brachial Plexus Injuries Dr. Ashok K. Gupta Projecting for a useful rehabilitation following Brachial Plexus Injury is one of the most demanding surgical designs. Advent
Plastic Surgery - Cyber Lectures Brachial Plexus Injuries Dr. Ashok K. Gupta Projecting for a useful rehabilitation following Brachial Plexus Injury is one of the most demanding surgical designs. Advent
Obstetric Brachial Plexus Injuries: Evaluation and Management
 Obstetric Brachial Plexus Injuries: Evaluation and Management Peter M. Waters, MD Abstract Most infants with brachial plexus birth palsy who show signs of recovery in the first 2 months of life will subsequently
Obstetric Brachial Plexus Injuries: Evaluation and Management Peter M. Waters, MD Abstract Most infants with brachial plexus birth palsy who show signs of recovery in the first 2 months of life will subsequently
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Slide 1. Slide 2. Slide 3. The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach. Peripheral Nerve Surgery
 Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
BRACHIAL PLEXUS. DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae
 supraclavicular branch innervates rhomboids (major and minor) and levator scapulae") THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy. Dr Grace Ng Department of Paed PMH
 Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Brachial plexus lesions
 Brachial plexus lesions SGH Course 11.01.18 Esther Vögelin and Team Handchirurgie und Chirurgie der peripheren Nerven, Universitätsspital Bern Surgical anatomy of the brachial plexus 5-3-6-3-5 5 Roots:
Brachial plexus lesions SGH Course 11.01.18 Esther Vögelin and Team Handchirurgie und Chirurgie der peripheren Nerven, Universitätsspital Bern Surgical anatomy of the brachial plexus 5-3-6-3-5 5 Roots:
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms.
 THE BRACHIAL The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms. CONTENTS Brachial plexus Brachial plexus anatomy MRI of brachial plexus Dermatome(C8-T1)
THE BRACHIAL The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms. CONTENTS Brachial plexus Brachial plexus anatomy MRI of brachial plexus Dermatome(C8-T1)
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
The arm: *For images refer back to the slides
 The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
BRACHIAL PLEXUS INJURY INVESTIGATION, LOCALIZATION AND TREATMENT. Presented By : Dr.Pankaj Jain
 BRACHIAL PLEXUS INJURY INVESTIGATION, LOCALIZATION AND TREATMENT Presented By : Dr.Pankaj Jain EMBRYOLOGY l Brachial plexus (BP) is developed at 5 weeks of gestation l Afferent fibers develop from neuroblast
BRACHIAL PLEXUS INJURY INVESTIGATION, LOCALIZATION AND TREATMENT Presented By : Dr.Pankaj Jain EMBRYOLOGY l Brachial plexus (BP) is developed at 5 weeks of gestation l Afferent fibers develop from neuroblast
MUSCLES. Anconeus Muscle
 LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
Biceps Brachii. Muscles of the Arm and Hand 4/4/2017 MR. S. KELLY
 Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Clinical Study Extending the Indications for Primary Nerve Surgery in Obstetrical Brachial Plexus Palsy
 BioMed Research International, Article ID 627067, 5 pages http://dx.doi.org/10.1155/2014/627067 Clinical Study Extending the Indications for Primary Nerve Surgery in Obstetrical Brachial Plexus Palsy Stuart
BioMed Research International, Article ID 627067, 5 pages http://dx.doi.org/10.1155/2014/627067 Clinical Study Extending the Indications for Primary Nerve Surgery in Obstetrical Brachial Plexus Palsy Stuart
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
The Elbow and Radioulnar Joints Kinesiology. Dr Cüneyt Mirzanli Istanbul Gelisim University
 The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
Neurolysis of the conducting neuroma-in-continuity in perinatal brachial plexus palsy evaluation of the results of surgical treatment
 Original article Neurolysis of the conducting neuroma-in-continuity in perinatal brachial plexus palsy evaluation of the results of surgical treatment Jerzy Gosk 1, Roman Rutowski 1, 2, Maciej Urban 1,
Original article Neurolysis of the conducting neuroma-in-continuity in perinatal brachial plexus palsy evaluation of the results of surgical treatment Jerzy Gosk 1, Roman Rutowski 1, 2, Maciej Urban 1,
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Clinical Guidance. Neonatal Manual Chapter 10: Musculoskeletal problems
 Clinical Guidance Neonatal Manual Chapter 10: Musculoskeletal problems Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter
Clinical Guidance Neonatal Manual Chapter 10: Musculoskeletal problems Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter
Assessment of the Brachial Plexus EMG Course CNSF Halifax Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University
 Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone
, to the elbow joint (distal) - it has one bone ; the humerus which is a long bone") *the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
Faculty of Dental Medicine and Surgery. Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla
 Faculty of Dental Medicine and Surgery Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla PNS Terminology Ganglia neuron cell bodies Peripheral nerves neuronal axons PNS neuroglia Satellite
Faculty of Dental Medicine and Surgery Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla PNS Terminology Ganglia neuron cell bodies Peripheral nerves neuronal axons PNS neuroglia Satellite
Upper limb Arm & Cubital region 黃敏銓
 Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Peripheral Nerve Injuries of the Upper Limb.
 Peripheral Nerve Injuries of the Upper Limb www.fisiokinesiterapia.biz Definitions Radiculopathy Process affecting the nerve root, most commonly by a herniated disc Weakness in muscles supplied by the
Peripheral Nerve Injuries of the Upper Limb www.fisiokinesiterapia.biz Definitions Radiculopathy Process affecting the nerve root, most commonly by a herniated disc Weakness in muscles supplied by the
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus.
 *Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
G24: Shoulder and Axilla
 G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
Anatomy of the Musculoskeletal System
 Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Management of Hand Palsies in Isolated C7 to T1 or C8, T1 Root Avulsions
 12(3):156 160, 2008 T E C H N I Q U E Management of Hand Palsies in Isolated C7 to T1 or C8, T1 Root Avulsions Jean-Noel Goubier, PhD and Frédéric Teboul, MD Centre International de Chirurgie de la Main
12(3):156 160, 2008 T E C H N I Q U E Management of Hand Palsies in Isolated C7 to T1 or C8, T1 Root Avulsions Jean-Noel Goubier, PhD and Frédéric Teboul, MD Centre International de Chirurgie de la Main
Upper Limb Muscles Muscles of Axilla & Arm
 Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
Treating a child with a brachial plexus birth injury
 J Neurosurg Pediatrics 13:229 237, 2014 AANS, 2014 Neurolysis alone as the treatment for neuroma-in-continuity with more than 50% conduction in infants with upper trunk brachial plexus birth palsy Clinical
J Neurosurg Pediatrics 13:229 237, 2014 AANS, 2014 Neurolysis alone as the treatment for neuroma-in-continuity with more than 50% conduction in infants with upper trunk brachial plexus birth palsy Clinical
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Inspection. Physical Examination of the Elbow. Anterior Elbow 2/14/2017. Inspection. Carrying angle. Lateral dimple. Physical Exam of the Elbow
 of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
Electrical stimulation of the upper limb. Paul Taylor
 Electrical stimulation of the upper limb Paul Taylor Three upper limb Pathways Shoulder subluxation Upper Limb Active Function Upper limb Passive All differ in aims but follow a similar 6 month protocol
Electrical stimulation of the upper limb Paul Taylor Three upper limb Pathways Shoulder subluxation Upper Limb Active Function Upper limb Passive All differ in aims but follow a similar 6 month protocol
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
Scientific paper session 4: Brachial plexus adults/ nerve general
 Scientific paper session 4: Brachial plexus adults/ nerve general Introduced and moderated by Mariano Socolovsky and Willem Pondaag Grafting versus transfer Mariano Socolovsky, Buenos Aires How to improve
Scientific paper session 4: Brachial plexus adults/ nerve general Introduced and moderated by Mariano Socolovsky and Willem Pondaag Grafting versus transfer Mariano Socolovsky, Buenos Aires How to improve
Al Hess MD NERVE REPAIR
 Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report
 SHORT REPORT Eur J Anat, 10 (3): 61-66 (2006) Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report K. Ramachandran, I. Kanakasabapathy and
SHORT REPORT Eur J Anat, 10 (3): 61-66 (2006) Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report K. Ramachandran, I. Kanakasabapathy and
Type II SLAP lesions are created when the biceps anchor has pulled away from the glenoid attachment.
 Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Arthroscopic Superior Labral (SLAP) Repair Protocol-Type II, IV, and Complex Tears The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation course of
Intra-operative neurophysiological prediction of upper trunk recovery in obstetric brachial plexus palsy with neuroma in continuity
 CHILDREN S ORTHOPAEDICS Intra-operative neurophysiological prediction of upper trunk recovery in obstetric brachial plexus palsy with neuroma in continuity K. F. Chin, V. P. Misra, G. M. Sicuri, M. Fox,
CHILDREN S ORTHOPAEDICS Intra-operative neurophysiological prediction of upper trunk recovery in obstetric brachial plexus palsy with neuroma in continuity K. F. Chin, V. P. Misra, G. M. Sicuri, M. Fox,
Slides of Anatomy. Spring Dr. Maher Hadidi, University of Jordan
 Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited by the Premed Academic Team to fit the slides of spring 2019. Spring 2019 Dr. Maher Hadidi, University
Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited by the Premed Academic Team to fit the slides of spring 2019. Spring 2019 Dr. Maher Hadidi, University
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Hemiplegic Shoulder. Incidence & Rationale. Shoulder Pain Assessment & Treatment
 Hemiplegic Shoulder Jeane Davis Fyfe OT, Senior Therapist Incidence & Rationale Up to 72% of stroke survivors will experience shoulder pain Shoulder pain may inhibit patient participation in rehabilitation
Hemiplegic Shoulder Jeane Davis Fyfe OT, Senior Therapist Incidence & Rationale Up to 72% of stroke survivors will experience shoulder pain Shoulder pain may inhibit patient participation in rehabilitation
Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation
 Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation Sheelah Cochran OTR/L, CPAM, CKTP Objectives Perform an initial evaluation of post-surgical conditions Identify appropriate splinting
Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation Sheelah Cochran OTR/L, CPAM, CKTP Objectives Perform an initial evaluation of post-surgical conditions Identify appropriate splinting
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader. Lab Leaders: STATION I BRACHIAL PLEXUS
 Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Anatomy Workshop Upper Extremity David Ebaugh, PT, PhD Workshop Leader Lab Leaders: STATION I BRACHIAL PLEXUS A. Posterior cervical triangle and axilla B. Formation of plexus 1. Ventral rami C5-T1 2. Trunks
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
We reviewed a consecutive series of 33 infants who
 Function of the upper limb after surgery for obstetric brachial plexus palsy C. E. Dumont, V. Forin, H. Asfazadourian, C. Romana From Hôpital d Enfants Armand Trousseau, Paris, France We reviewed a consecutive
Function of the upper limb after surgery for obstetric brachial plexus palsy C. E. Dumont, V. Forin, H. Asfazadourian, C. Romana From Hôpital d Enfants Armand Trousseau, Paris, France We reviewed a consecutive
Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient with Multiple Previous Operations
 Case Reports in Surgery, Article ID 715389, 4 pages http://dx.doi.org/10.1155/2014/715389 Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient
Case Reports in Surgery, Article ID 715389, 4 pages http://dx.doi.org/10.1155/2014/715389 Case Report Successful Outcome of Triangle Tilt as Revision Surgery in a Pediatric Obstetric Brachial Plexus Patient
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/267 holds various files of this Leiden University dissertation. Author: Duijnisveld, B.J. Title: Muscle and joint sequelae in brachial plexus injury Issue
Cover Page The handle http://hdl.handle.net/887/267 holds various files of this Leiden University dissertation. Author: Duijnisveld, B.J. Title: Muscle and joint sequelae in brachial plexus injury Issue
Spinal nerves. Aygul Shafigullina. Department of Morphology and General Pathology
 Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions
 British Journal of Plastic Surgery (2005) 58, 541 546 The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions M.M. Samardzic*, D.M. Grujicic, L.G. Rasulic,
British Journal of Plastic Surgery (2005) 58, 541 546 The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions M.M. Samardzic*, D.M. Grujicic, L.G. Rasulic,
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5. September 30, 2011
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
Chapter 14. Summary and Discussion
 Chapter 14 Summary and Discussion Key Findings 1) The severity of the nerve lesion increases with birthweight. 2) The natural history has not been appropriately investigated. 3) Spontaneous recovery is
Chapter 14 Summary and Discussion Key Findings 1) The severity of the nerve lesion increases with birthweight. 2) The natural history has not been appropriately investigated. 3) Spontaneous recovery is
A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course
 2014 Annual Breast Cancer Rehabilitation Healthcare Provider Event A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course November 7 th and 8 th, 2014 Mercer University, Atlanta,
2014 Annual Breast Cancer Rehabilitation Healthcare Provider Event A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course November 7 th and 8 th, 2014 Mercer University, Atlanta,
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Brachial plexuses and axillary lymph nodes
 Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi. E. mail:
 Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain
 Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
Physical examination protocol in the study of VPT and nerve conduction in working women with and without chronic pain ID number General health OK Affected Height cm Weight kg Heart OK Arrhythmia Murmurs
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
IFSSH Scientific Committee on Neonatal Brachial Plexus Palsy
 IFSSH Scientific Committee on Neonatal Brachial Plexus Palsy Chair: Howard Clarke (Canada) Committee: Raymond Tse (USA) Martijn Malessy (The Netherlands) Scott Kozin (USA) Report submitted August 2014
IFSSH Scientific Committee on Neonatal Brachial Plexus Palsy Chair: Howard Clarke (Canada) Committee: Raymond Tse (USA) Martijn Malessy (The Netherlands) Scott Kozin (USA) Report submitted August 2014
Outcome Following Spinal Accessory to Suprascapular (Spinoscapular) Nerve Transfer in Infants with Brachial Plexus Birth Injuries
 Nerve Transfer in Infants with Brachial Plexus Birth Injuries") HAND (2010) 5:190 194 DOI 10.1007/s11552-009-9236-1 ORIGINAL ARTICLE Outcome Following Spinal Accessory to Suprascapular (Spinoscapular) Nerve Transfer in Infants with Brachial Plexus Birth Injuries David
HAND (2010) 5:190 194 DOI 10.1007/s11552-009-9236-1 ORIGINAL ARTICLE Outcome Following Spinal Accessory to Suprascapular (Spinoscapular) Nerve Transfer in Infants with Brachial Plexus Birth Injuries David
Witold Wnukiewicz 1, Piotr Mazurek 1
 POLSKI PRZEGLĄD CHIRURGICZNY 2010, 82, 11, 610 614 10.2478/v10035-010-0092-z The results of surgical treatment of the forearm deformity in perinatal brachial plexus palsy Jerzy Gosk 1, Roman Rutowski 1,2,
POLSKI PRZEGLĄD CHIRURGICZNY 2010, 82, 11, 610 614 10.2478/v10035-010-0092-z The results of surgical treatment of the forearm deformity in perinatal brachial plexus palsy Jerzy Gosk 1, Roman Rutowski 1,2,
Trapezius transfer in brachial plexus palsy
 Upper limb Trapezius transfer in brachial plexus palsy CORRELATION OF THE OUTCOME WITH MUSCLE POWER AND OPERATIVE TECHNIQUE O. Rühmann, S. Schmolke, M. Bohnsack, J. Carls, C. J. Wirth From Hannover Medical
Upper limb Trapezius transfer in brachial plexus palsy CORRELATION OF THE OUTCOME WITH MUSCLE POWER AND OPERATIVE TECHNIQUE O. Rühmann, S. Schmolke, M. Bohnsack, J. Carls, C. J. Wirth From Hannover Medical
Fascial Compartments of the Upper Arm
 Fascial Compartments of the Upper Arm The upper arm is enclosed in a sheath of deep fascia and has two fascial septa: 1- Medial fascial septum (medial intermuscular septum): attached to the medial supracondylar
Fascial Compartments of the Upper Arm The upper arm is enclosed in a sheath of deep fascia and has two fascial septa: 1- Medial fascial septum (medial intermuscular septum): attached to the medial supracondylar
Rahul K Nath * and Chandra Somasundaram
 Nath and Somasundaram Journal of Orthopaedic Surgery and Research (2015) 10:51 DOI 10.1186/s13018-015-0191-y RESEARCH ARTICLE Open Access Significant improvement in nerve conduction, arm length, and upper
Nath and Somasundaram Journal of Orthopaedic Surgery and Research (2015) 10:51 DOI 10.1186/s13018-015-0191-y RESEARCH ARTICLE Open Access Significant improvement in nerve conduction, arm length, and upper
Human Anatomy Biology 351
 1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy
 An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy") A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete brachial plexus palsy
 Int J Clin Exp Med 2016;9(11):22880-22885 www.ijcem.com /ISSN:1940-5901/IJCEM0032455 Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete
Int J Clin Exp Med 2016;9(11):22880-22885 www.ijcem.com /ISSN:1940-5901/IJCEM0032455 Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete
BRACHIAL PLEXUS 11/12/2014 كيف تتكون الضفيرة FORMATION ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD. Grey matter. Cervical intumescence - C 6 - T 2
 OF THE SPINAL CORD. Grey matter. Cervical intumescence - C 6 - T 2") BRACHIAL PLEXUS Prof. Fawzy Elnady ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD Grey matter Cervical intumescence - C 6 - T 2 Lumbar intumescence - L 4 S 2 كيف تتكون الضفيرة FORMATION The ventral rami
BRACHIAL PLEXUS Prof. Fawzy Elnady ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD Grey matter Cervical intumescence - C 6 - T 2 Lumbar intumescence - L 4 S 2 كيف تتكون الضفيرة FORMATION The ventral rami
Brachial Plexus Injury in the Newborn Trenna L. Sutcliffe. DOI: /neo.8-6-e239
 Brachial Plexus Injury in the Newborn Trenna L. Sutcliffe NeoReviews 2007;8;e239-e246 DOI: 10.1542/neo.8-6-e239 The online version of this article, along with updated information and services, is located
Brachial Plexus Injury in the Newborn Trenna L. Sutcliffe NeoReviews 2007;8;e239-e246 DOI: 10.1542/neo.8-6-e239 The online version of this article, along with updated information and services, is located
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Rehabilitation Guidelines for Labral/Bankert Repair
 Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Rehabilitation Guidelines for Labral/Bankert Repair The true shoulder joint is called the glenohumeral joint and consists humeral head and the glenoid. It is a ball and socket joint. Anatomy of the Shoulder
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Peripheral Nervous Sytem: Upper Body
 Peripheral Nervous Sytem: Upper Body MSTN121 - Neurophysiology Session 10 Department of Myotherapy Cervical Plexus Accessory nerve (CN11 + C1-5) Motor: trapezius and sternocleidomastoid Greater auricular
Peripheral Nervous Sytem: Upper Body MSTN121 - Neurophysiology Session 10 Department of Myotherapy Cervical Plexus Accessory nerve (CN11 + C1-5) Motor: trapezius and sternocleidomastoid Greater auricular
ARM Brachium Musculature
 ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches
ARM Brachium Musculature Coracobrachialis coracoid process of the scapula medial shaft of the humerus at about its middle 1. flexes the humerus 2. assists to adduct the humerus Blood: muscular branches