CHRONIC ANKLE INSTABILITY
|
|
|
- Poppy Baker
- 5 years ago
- Views:
Transcription


1 CHRONIC ANKLE INSTABILITY Eric M Magrum DPT OCS FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville ** Subjective Asterisks Signs/Symptoms ** 34 yo real estate agent; 5 months s/p misstep at construction site with ankle PF/INV injury. Goals: return to softball, coach kids soccer, walk uneven terrain work C/o: Anterolateral ankle pain, stiffness, feels vulnerable ; intermittent sharp pain laterally with lateral mvts, rotation. Intermittent effusion anterior TC, posterior to lateral malleolus. Denies mechanical, Neurovascular sxs. PMHx: Ankle sprain 5+; HS tear. Chronic Ankle Instability Development of repetitive ankle sprain Persistent post injury symptoms Giving Way Recurrent Inversion injury Differential List Peroneal Brevis Tearing - Longitudinal Peroneal Tenosynovitis Peroneal Tendon Subluxation OCD Lesion Talar Dome Ankle Impingement/Synovitis Retinacular Attenuation Syndesmosis Injury Medial/Deltoid Injury Lis Franc/Mid Foot Injury Reproduction Without Consent 1




2 ** Physical Exam Asterisks Signs/Symptoms ** Effusion anterior aspect TC Medial>lateral aspect Rearfoot Varus Limited DF ROM TC post glide; STJ EVR hypo mobility Functional Screen: Poor Single leg stance Increased sway, lateral LOB. Bilateral Squat: Limited TC DF with lateral ankle pain. Lateral Hop: Pain, loss of balance lateral (+) Talar Tilt Chronic Ankle Instability Arthrokinematic Restrictions Mechanical Insufficiencies Degenerative Changes Pathological Laxity Synovial Changes Recurrent Ankle Sprain Impaired Proprioception Impaired Neuromuscular Functional Insufficiencies Impaired Postural Control Control Strength Deficits Hertel, J Athletic Training, 2002 Reproduction Without Consent 2

 CAI Comprehensive Rehab Exercise Specificity Manual Therapy Proprioception")

3 Functional and/or Mechanical Deficits Functional Subjective report frequent giving way with normal activity Neuromuscular deficits Proprioceptive deficits Strength deficits Postural control deficits Mechanical Movement > physiological limit Pathologic laxity Arthrokinematic restrictions DJD Synovial changes Predictive of CAI 2 Weeks Inability to complete single drop landing and drop 6 months Lower FAAM ADLs Decreased SEBT (post reach directions) CAI Comprehensive Rehab Exercise Specificity Manual Therapy Proprioception - Specific Joint Neuromuscular control restrictions Strength Education Postural control Feedback Outcome Assessment Proprioception Neural input to the CNS Mechanoreceptors Articular Myofascial *Muscle afferents * Cutaneous Kinesthesia Joint Position Sense Reproduction Without Consent 3




4 Proprioception Deficits Decreased DF/EVR Clearance in swing Terminal Swing Increased PF/INV Bilateral Treatment Improve Joint Position Sense Multi station Balance Exercises Strengthening EVR/INV Frontal plane > Sagittal plane JPS deficits Reproduction Without Consent 4





5 Intrinsic Foot Muscle activation Short Foot - Drag Ball of big toe toward heel without toe flexion/clawing Activation - Lift 5 toes (passive tension arch muscles) relax toes maintain active tone in arch muscles Dissociation - Plant 1 st Ray, lift 4 lateral toes alternate <-> Lift 1 st Ray, keep 4 lateral toes stable CAI: Increased PF/INV at terminal swing Reproduction Without Consent 5






6 Results: Significant improvement in joint position sense and postural sway as well as significant changes in muscle reaction times Med Sci Sports Exerc Reproduction Without Consent 6




7 Neuromuscular Deficits Unconscious activation of dynamic restraints occurring in preparation for and in response to joint motion and loading for the purpose of maintaining and restoring functional stability Riemann BL J Athl Train 2002? Feed forward > Feed back Ligament mechanoreceptors do not facilitate a muscle reaction fast enough to protect from an inversion sprain Central Motor programming deficit Arthrogenic Muscular Inhibition Previous Ankle Sprain Impaired Peroneal Reaction Time Chronic Ankle Instability Delayed Peroneal Reaction time compared to uninvolved side Reproduction Without Consent 7









8 Neuromuscular Re-Education Unconscious Incompetence Conscious Incompetence Conscious Competence Unconscious Competence Neuromuscular Control Delayed/Inadequate Response Exercise Prescription Unexpected perturbations Landing mechanics Unstable surfaces Feedback Reproduction Without Consent 8


")






9 Strengthening -? Controversy Evertors (increased PF/INV terminal swing) Concentric Invertors = Improved JPS Co Contraction Closed Kinetic Chain Proximal Hip/Gluteals Foot Intrinsics Eccentric Invertors Displace COM laterally Functional Sport Specific Reproduction Without Consent 9








10 Reproduction Without Consent 10

 Resultant motor control deficit Progressive Balance Program Dynamic stabilization")

11 Star Excursion (Y) Balance Test Postural Control Involves Somatosensory, Visual, and Vestibular systems to remain upright Eyes Closed Unstable surfaces Progressive Dynamic Sport Specific CAI patients have altered sensory organization strategies Increased reliance on visual information (Up regulation) Decreased somatosensory information from ankle (Down regulation) Resultant motor control deficit Progressive Balance Program Dynamic stabilization Perturbations Unpredictable changes in direction Landing from Hop Dynamic reaching - SEBT Improved static stabilization: TTB eyes closed Improved dynamic stabilization : SEBT Improved self reported functional status : (FADI) Reproduction Without Consent 11
12 Single-Limb Stance Activities Participants performed three repetitions of single-limb stance activities. Each activity (eyes open and eyes closed) had seven levels of difficulty. 1. Arms out on hard floor for 30 s 2. Arms across chest on hard floor for 30 s 3. Arms across chest on hard floor for 60 s 4. Arms out on foam pad for 30 s 5. Arms across chest for 30 s on foam pad 6. Arms across chest for 60 s on foam pad 7. Arms across chest for 90 s on foam pad Single-Limb Hops to Stabilization 10 hops in each direction Hop from the starting position to the target position (18, 27, or 36 inches). After stabilizing balance in a single-limb stance, participants hopped in the exact opposite direction back to the starting position and stabilized in the single-limb stance. Four directions of hops: Anterior/Posterior Medial/Lateral Antero lateral/posterio medial Antero medial/posterio lateral Hop to Stabilization and Reach Hop After stabilization in the single-limb stance, participants had to reach back to the starting position Then they hopped back to the starting position and reached to the target position. Unanticipated Hop to Stabilization Numbers displayed to participants. Corresponding to a target position to which they would hop. Hop to stabilization - participants were allowed to use any combination of hops (AP, ML, AM/PL, or AL/PM) they desired to accomplish the goal of getting through the sequence error-free. Reproduction Without Consent 12




13 Arthrokinematic Restrictions Degenerative Changes Chronic Ankle Instability Pathological Laxity Mechanical Insufficiencies Synovial Changes Recurrent Ankle Sprain Impaired Proprioception Functional Insufficiencies Impaired Postural Control Impaired Neuromuscular Control Strength Deficits Changes at the Joint Increased laxity Altered joint alignment TC, Distal tib fib Impaired arthrokinematics Sensorimotor changes Increased load on the joint ARTHROKINEMATIC IMPAIRMENTS Hypo mobility Distal Tibia fibular Joint Positional Fault Talar Positional Fault Limited Posterior Talar Glide Reproduction Without Consent 13





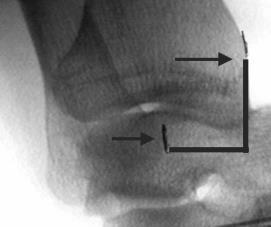

14 Anterior positional fault of the Talus may be present in individuals with CAI Reproduction Without Consent 14






15 Limited ankle dorsiflexion ROM during midstance Limited dorsiflexion ROM during gait among individuals with CAI may be a risk factor for recurrent ankle sprains Joint mobilization was associated with: - Greater DF ROM* -TTB anterior posterior direction* -Posterior Talar displacement -Mean of TTB medial-lateral This indicates that joint mobilization treatment has mechanical and functional benefits for addressing impairments in sensorimotor function and arthrokinematic restrictions commonly experienced by individuals with CAI Development of CPR to predict success with Manual Therapy + Exercise ¾ Variables predicted 95% likelihood for success Worse with standing Worse in the evening Navicular drop > 5mm Hypo mobile Distal Tib-Fib Reproduction Without Consent 15










16 Proximal Tibiofibular Joint Anterior Mob/Manipulation Grasp posterior aspect of fibular head with 2 nd MCP ER tibia, Flex knee to barrier with opposite hand on distal tibia High velocity, low amplitude thrust direction of force toward ipsilateral buttock Proximal TibFib Posterior Mobilization/Manipulation Decreased Post Medial glide Stabilize medially to prevent valgus Stabilize tibia medially Pisiform on fibular head Mob/Thrust down to table (Post Med) Reproduction Without Consent 16
 Individuals with CAI demonstrated changes in soleus H/M ratio without changes in fibularis longus activation following Distal Tibiofibular joint")


17 Proximal TibFib Anterior Mobilization/Manipulation Decreased Ant Lateral glide Opposite side so manipulating hand is in line with axis of joint Stabilize with inside hand Pisiform over fibular head Mob/Manip (Anteriolateral direction) Individuals with CAI demonstrated changes in soleus H/M ratio without changes in fibularis longus activation following Distal Tibiofibular joint manipulation Proximal tibiofibular joint manipulation did not have an effect on muscle activation J Electromyogr Kinesiol Distal Tib/Fib Posterior Mobilization/Manipulation Distal LE edge of table, stabilize foot at end ROM DF Stabilize distal Tibia with inside hand Thenar eminence contact lateral malleolus Anterior to Posterior force through weight shift Distal Tibiofibular Joint Functional Posterior Mobilization Clinician stabilizes the anterior aspect of the distal tibia. Opposite hand grasps the anterior aspect of the distal fibula with the Thenar eminence As the patient translates the knee forward, the distal fibula is translated in an anterior-toposterior direction Athletic Training & Sports Health Care Vol. 1 No Reproduction Without Consent 17






18 Mulligan Distal TibFib Taping Talocrural Distraction Mobilization/Manipulation Grasp dorsum of the foot with interlaced fingers, Stabilize plantar aspect with thumbs DF, pronate to barrier Long axis distraction Mob/Manipulation - Caudal Talocrural Posterior Mobilization/Manipulation Contact anterior talus with thumbs/web space DF, pronate/supinate to barrier; Stabilize with thigh Anterior to posterior force to talus Mob/Manipulation MWM Patient actively pulls into DF Reproduction Without Consent 18

 and force on talus angulation to engage specific")



19 Posterior Talar Mobilization With Movement Clinician contacts the anterior aspect of the talus with thumbs Anterior-to-posterior directed force is maintained while patient lunges forward Adjust lunge direction (medial, lateral) and force on talus angulation to engage specific barrier Athletic Training & Sports Health Care Vol. 1 No Contact anterior aspect talus with web space 1-2 nd digits Mobilization belt around posterior distal Tib-fib and clinicians buttocks Patient lunge to engage DF barrier Anterior Posterior mobilization at talus; Posterior Anterior mobilization distal tibia through clinician weight shift Functional Talocrural Posterior Mobilization STJ Distraction Reproduction Without Consent 19

; Outside hand navicular (thumb, calcaneus distally 2 nd MCP Stabilize Tibia medially with 2 nd MCP")

20 Medial Tilt Eversion Mobilization/Manipulation STJ Grasp calcaneus medially thumb/2 nd MCP (inside arm); Outside hand navicular (thumb, calcaneus distally 2 nd MCP Stabilize Fibula laterally with 2 nd MCP Popliteal region into clinician s iliac crest Distraction Lean back Ulnar deviation medial tilt (fulcrum with hypothenar on tibia) Lateral Tilt Inversion Mobilization/Manipulation STJ Grasp calcaneus medially thumb/2 nd MCP (inside arm); Outside hand navicular (thumb, calcaneus distally 2 nd MCP Stabilize Tibia medially with 2 nd MCP Popliteal region into clinician s iliac crest Distraction Lean back Radial deviation lateral tilt (fulcrum with hypothenar on tibia) STJ Medial/Lateral Glides Medial Column Mid foot Mobilization Navicular on Talus Medial Lateral Rotation Plantar-Dorsal Glide Reproduction Without Consent 20




21 Medial Column Mid foot Mobilization Medial Cuneiform on Navicular Medial Lateral Rotation Plantar-Dorsal Glide Medial Column Mid foot Mobilization First MT on Medial Cuneiform Medial Lateral Rotation Plantar-Dorsal Glide Plantar Mid Foot Mobilization/Manipulation Navicular Medial Cuneiform 1 st MTP Calcaneocuboid Joint Techniques Cuboid may present plantar positioned joint dysfunction and with medial rotation in inversion sprains Overactivation of PL pulling on a loose packed cuboid Cuboid dorsal glide hypomobility Less often will present dorsally positioned joint dysfunction Loss of plantar mobility and loss of Eversion Reproduction Without Consent 21







")

22 Plantar Cuboid Mobilization/Manipulation Dorsal Cuboid Whip Manipulation Prone Dorsiflexion Self Mobilization Summary Exercise Prescription Specificity Proprioception Multistation Balance Exercises DF/EVR at initial contact Neuromuscular Re education Feed forward > Feed back Strengthening Closed Kinetic Chain (Invertors, Evertors, Proximal) Postural Control Eyes closed, Dynamic Manual Therapy Specificity Restore TC DF Normal Arthrokinematics Reproduction Without Consent 22

23 ? Questions? Reproduction Without Consent 23
Module Three: Interventions of the Foot/Ankle
 Evidence-Based Treatment of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Three: Interventions of the Foot/Ankle (75 minutes) Skilled Process a rearfoot
Evidence-Based Treatment of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Three: Interventions of the Foot/Ankle (75 minutes) Skilled Process a rearfoot
Biokinesiology of the Ankle Complex
 Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs
 Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Outline. Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t
 Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Practical Applications of Manual Therapy for the Ankle and Foot
 Practical Applications of Manual Therapy for the Ankle and Foot PHATS Annual Meeting 2014 Orlando, Florida Outline! Objectives! Case Study! What is Manual Therapy?! Joint Mobilization! Joint Mobilization
Practical Applications of Manual Therapy for the Ankle and Foot PHATS Annual Meeting 2014 Orlando, Florida Outline! Objectives! Case Study! What is Manual Therapy?! Joint Mobilization! Joint Mobilization
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and
 Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Follow this and additional works at:
 The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2012 Effects of joint mobilization on ankle dorsiflexion range of motion, dynamic postural control and selfreported
The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2012 Effects of joint mobilization on ankle dorsiflexion range of motion, dynamic postural control and selfreported
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Main Menu. Ankle and Foot Joints click here. The Power is in Your Hands
 1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
Managing Tibialis Posterior Tendon Injuries
 Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
My Technique for Adjusting the Excessively Pronated Foot
 My Technique for Adjusting the Excessively Pronated Foot by Mark N. Charrette, DC One can think of Chiropractic in terms of science, art, and philosophy. The art or application of Chiropractic technique
My Technique for Adjusting the Excessively Pronated Foot by Mark N. Charrette, DC One can think of Chiropractic in terms of science, art, and philosophy. The art or application of Chiropractic technique
Re-establishing establishing Neuromuscular
 Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
Re-establishing establishing Neuromuscular Control Why is NMC Critical? What is NMC? Physiology of Mechanoreceptors Elements of NMC Lower-Extremity Techniques Upper-Extremity Techniques Readings Chapter
The Lower Limb VII: The Ankle & Foot. Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa
 The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Runner with Recurrent Achilles Tendon Pain 4/21/2017
 Young Runner with Recurrent Achilles Pain In alphabetical order: Kornelia Kulig PT, PhD, FAPTA Los Angeles, CA Lisa Meyer PT, DPT, OCS isports Physical Therapy Los Angeles, CA Liz Poppert MS, DPT, OCS
Young Runner with Recurrent Achilles Pain In alphabetical order: Kornelia Kulig PT, PhD, FAPTA Los Angeles, CA Lisa Meyer PT, DPT, OCS isports Physical Therapy Los Angeles, CA Liz Poppert MS, DPT, OCS
ANKLE JOINT ANATOMY 3. TALRSALS = (FOOT BONES) Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.
 Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.") ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle
 Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Manual Therapy for Patients with Knee OA Knee Manual Therapy Protocol
 Chapter SIX Manual Therapy for Patients with Knee OA Knee Manual Therapy Protocol Cathy Chapple Martin Kidd Jessica Smith Daniel Pinto J. Haxby Abbott 181 n n 182 General Guidelines Knee Manual Therapy
Chapter SIX Manual Therapy for Patients with Knee OA Knee Manual Therapy Protocol Cathy Chapple Martin Kidd Jessica Smith Daniel Pinto J. Haxby Abbott 181 n n 182 General Guidelines Knee Manual Therapy
Introduction. The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking.
 The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
THE EFFECT OF JOINT MOBILIZATION ON FUNCTIONAL OUTCOMES ASSOCIATED WITH CHRONIC ANKLE INSTABILITY
 University of Kentucky UKnowledge University of Kentucky Doctoral Dissertations Graduate School 2011 THE EFFECT OF JOINT MOBILIZATION ON FUNCTIONAL OUTCOMES ASSOCIATED WITH CHRONIC ANKLE INSTABILITY Matthew
University of Kentucky UKnowledge University of Kentucky Doctoral Dissertations Graduate School 2011 THE EFFECT OF JOINT MOBILIZATION ON FUNCTIONAL OUTCOMES ASSOCIATED WITH CHRONIC ANKLE INSTABILITY Matthew
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
Prevention and Treatment of Injuries. Anatomy. Anatomy. Tibia: the second longest bone in the body
 Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
USING FUNCTIONAL PERFORMANCE TESTS FOR PREDICTING CHRONIC ANKLE INSTABILITY JUPIL KO. (Under the Direction of DR. CATHLEEN BROWN CROWELL) ABSTRACT
 ABSTRACT") USING FUNCTIONAL PERFORMANCE TESTS FOR PREDICTING CHRONIC ANKLE INSTABILITY by JUPIL KO (Under the Direction of DR. CATHLEEN BROWN CROWELL) ABSTRACT Functional performance deficits may be present in a
USING FUNCTIONAL PERFORMANCE TESTS FOR PREDICTING CHRONIC ANKLE INSTABILITY by JUPIL KO (Under the Direction of DR. CATHLEEN BROWN CROWELL) ABSTRACT Functional performance deficits may be present in a
Feet First. Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention
 Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
AN OSTEOPTHIC APPROACH TO FOOT PAIN
 AN OSTEOPTHIC APPROACH TO FOOT PAIN rob truax, DO medical director, Osteopathic Sports Rehabilitation Clinic University Hospitals associate professor, Osteopathic Manipulative Medicine Department, Ohio
AN OSTEOPTHIC APPROACH TO FOOT PAIN rob truax, DO medical director, Osteopathic Sports Rehabilitation Clinic University Hospitals associate professor, Osteopathic Manipulative Medicine Department, Ohio
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems
 Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
The immediate effects of fibular repositioning tape on ankle kinematics and muscle activity. Megan East
 The immediate effects of fibular repositioning tape on ankle kinematics and muscle activity Megan East A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment
The immediate effects of fibular repositioning tape on ankle kinematics and muscle activity Megan East A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Arthrokinematics and Selected Joint Techniques
 The Foot and Ankle: An Overview of Arthrokinematics and Selected Joint Techniques Janice K. Loudon, PhD, PT, ATC, SCS; Stephania L. Bell, MS, PT ABSTRACT: Limited range of motion of the ankle is common
The Foot and Ankle: An Overview of Arthrokinematics and Selected Joint Techniques Janice K. Loudon, PhD, PT, ATC, SCS; Stephania L. Bell, MS, PT ABSTRACT: Limited range of motion of the ankle is common
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne
 What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
Posterior Tibialis Tendon Dysfunction & Repair
 1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005
 THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005 Unpublished Copyright Biomechanical Services, Inc. 2003 Biomechanical Services, Inc. 1050 Central Ave., Suite D
THE FOOT S CONNECTED TOO... Evaluation Procedures for Orthotic Therapy Prescription 2005 Unpublished Copyright Biomechanical Services, Inc. 2003 Biomechanical Services, Inc. 1050 Central Ave., Suite D
Key Points for Success:
 ANKLE & FOOT 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Keep your movements slow and precise. Breathe in before you move and breathe
ANKLE & FOOT 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Keep your movements slow and precise. Breathe in before you move and breathe
What is the most frequently sprained ligament with inversion ankle sprains? 1/30/2014
 What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
Ankle function alterations following acute ankle sprains over a 14 day period
 The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2014 Ankle function alterations following acute ankle sprains over a 14 day period Michael Sean Patrick Mayes
The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2014 Ankle function alterations following acute ankle sprains over a 14 day period Michael Sean Patrick Mayes
Ankle sprain. From acute to chronic. Dr Boris Gojanovic. Health & Performance Hôpital de La Tour, Meyrin, Switzerland
 Saas-Fee, March 9th 2016 Ankle sprain From acute to chronic Dr Boris Gojanovic Health & Performance Hôpital de La Tour, Meyrin, Switzerland Boris.Gojanovic@latour.ch @DrSportSante www.drsportsante.com
Saas-Fee, March 9th 2016 Ankle sprain From acute to chronic Dr Boris Gojanovic Health & Performance Hôpital de La Tour, Meyrin, Switzerland Boris.Gojanovic@latour.ch @DrSportSante www.drsportsante.com
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
SUBTLE CAVUS IN SPORTS INJURIES
 SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot. Objectives
 From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
From Childhood to Adulthood OMT for LOWER EXTREMITY Hip, Knee, Ankle, Foot Jan Hendryx, DO, FAAO Peek n Peak CME March 1, 2019 Objectives 1. Demonstrate knowledge of the anatomy of the lower extremity-
Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional Ankle Instability
 Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2009 Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2009 Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional
ChiroCredit.com Presents Biomechanics: Focus on
 ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity
 OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi
 Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Terms of Movements by Prof. Dr. Muhammad Imran Qureshi Three systems of the body work in coordination to perform various movements of the body. These are: A System of Bones (Osteology), A System of Muscles
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Functional biomechanics of the lower limb
 Functional biomechanics of the lower limb Ben and Matt. 24th July 2011 Principles of function Gravity Ground reaction Eco-concentric eccentric loading (preload) of a muscle (or group) is essential for
Functional biomechanics of the lower limb Ben and Matt. 24th July 2011 Principles of function Gravity Ground reaction Eco-concentric eccentric loading (preload) of a muscle (or group) is essential for
Ankle Rehabilitation with Wakefield Sports Clinic
 Ankle Rehabilitation with Wakefield Sports Clinic With Michael Woodcock Adelaide 36ERS & Wakefield Sports Clinic Physiotherapist The ankle joint is one of the major weight bearing structures in the body.
Ankle Rehabilitation with Wakefield Sports Clinic With Michael Woodcock Adelaide 36ERS & Wakefield Sports Clinic Physiotherapist The ankle joint is one of the major weight bearing structures in the body.
Everything. You Should Know. About Your Ankles
 Everything You Should Know About Your Ankles How Your Ankle Works The ankle joint is a hinge type joint that participates in movement and is involved in lower limb stability. There are 2 types of motions
Everything You Should Know About Your Ankles How Your Ankle Works The ankle joint is a hinge type joint that participates in movement and is involved in lower limb stability. There are 2 types of motions
31b Passive Stretches:! Technique Demo and Practice - Lower Body
 31b Passive Stretches:! Technique Demo and Practice - Lower Body 31b Passive Stretches:! Technique Demo and Practice - Lower Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
31b Passive Stretches:! Technique Demo and Practice - Lower Body 31b Passive Stretches:! Technique Demo and Practice - Lower Body! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
Why Train Your Calf Muscles
 Why Train Your Calf Muscles 1 Why Train Your Calf Muscles The muscles of the calf are often considered genetic muscles among fitness enthusiasts, suggesting that one is born with sizable and well developed
Why Train Your Calf Muscles 1 Why Train Your Calf Muscles The muscles of the calf are often considered genetic muscles among fitness enthusiasts, suggesting that one is born with sizable and well developed
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
Neurocognitive Ability in Individuals with Chronic Ankle Instability. A thesis presented to. the faculty of. In partial fulfillment
 Neurocognitive Ability in Individuals with Chronic Ankle Instability A thesis presented to the faculty of the College of Health Sciences and Professions of Ohio University In partial fulfillment of the
Neurocognitive Ability in Individuals with Chronic Ankle Instability A thesis presented to the faculty of the College of Health Sciences and Professions of Ohio University In partial fulfillment of the
HIP CASESTUDY 3. Body Chart-Initial Hypothesis: Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1
 Body Chart-Initial Hypothesis: HIP CASESTUDY 3 Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT OCS FAAOMPT Hamstring Strain HS Tendinopathy Lumbar Radiculopathy Lumbar
Body Chart-Initial Hypothesis: HIP CASESTUDY 3 Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 Eric Magrum DPT OCS FAAOMPT Hamstring Strain HS Tendinopathy Lumbar Radiculopathy Lumbar
Fibular Position in Individuals With Self-Reported Chronic Ankle Instability
 Fibular Position in Individuals With Self-Reported Chronic Instability Tricia J. Hubbard, PhD, ATC 1 Jay Hertel, PhD, ATC 2 Paul Sherbondy, MD 3 Study Design: Case control study. Objectives: The purpose
Fibular Position in Individuals With Self-Reported Chronic Instability Tricia J. Hubbard, PhD, ATC 1 Jay Hertel, PhD, ATC 2 Paul Sherbondy, MD 3 Study Design: Case control study. Objectives: The purpose
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
3/6/2012 STATE OF THE ART: FOOT AND ANKLE GENERAL KNOWLEDGE 1. TRASP REHABILITATION CONTENTS. General knowledge Trasp Prevention
 STATE OF THE ART: FOOT AND ANKLE ILITATION Fabienne Van De Steene. CONTENTS General knowledge Trasp Prevention Rehab Ankle sprain CAI Achilles tendon Plantar fasciitis Take home message 2 1. TRASP Ankle
STATE OF THE ART: FOOT AND ANKLE ILITATION Fabienne Van De Steene. CONTENTS General knowledge Trasp Prevention Rehab Ankle sprain CAI Achilles tendon Plantar fasciitis Take home message 2 1. TRASP Ankle
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Knee Injuries. PSK 4U Mr. S. Kelly North Grenville DHS. Medial Collateral Ligament Sprain
 Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
Knee Injuries PSK 4U Mr. S. Kelly North Grenville DHS Medial Collateral Ligament Sprain Result from either a direct blow from the lateral side in a medial direction or a severe outward twist Greater injury
BIOMECHANICS OF ANKLE FRACTURES
 BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
Functional Movement Screen (Cook, 2001)
") Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
What is Kinesiology? Basic Biomechanics. Mechanics
 What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
5 COMMON INJURIES IN THE FOOT & ANKLE
 5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic
 Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic ! Been running at a high level for 15 years.! 2012 Olympics Trials qualifier in the marathon and 6-time All-American in college! Owner of Ohio Sports
Leo Kormanik DC, MS, CCSP Ohio Sports Chiropractic ! Been running at a high level for 15 years.! 2012 Olympics Trials qualifier in the marathon and 6-time All-American in college! Owner of Ohio Sports
NEUROMOTOR FUNCTION FOLLOWING WHOLE-BODY VIBRATION IN INDIVIDUALS WITH CHRONIC ANKLE INSTABILITY
 NEUROMOTOR FUNCTION FOLLOWING WHOLE-BODY VIBRATION IN INDIVIDUALS WITH CHRONIC ANKLE INSTABILITY By DANA M. OTZEL A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL
NEUROMOTOR FUNCTION FOLLOWING WHOLE-BODY VIBRATION IN INDIVIDUALS WITH CHRONIC ANKLE INSTABILITY By DANA M. OTZEL A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL
Dr Nabil khouri MD. MSc. Ph.D
 Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
A comparison of strength, ROM, laxity, and dynamic and static postural control between those at-risk and healthy
 The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2013 A comparison of strength, ROM, laxity, and dynamic and static postural control between those at-risk and
The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2013 A comparison of strength, ROM, laxity, and dynamic and static postural control between those at-risk and
National Boards Part 4 Technique. Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical
. 2 setups per station (5 minutes) cervical") 1 National Boards Part 4 Technique Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical thoracic lumbar pelvic extremity Expect examiner interaction Graded on a Scantron
1 National Boards Part 4 Technique Exam Format 5 stations (1 doctor and 1 patient). 2 setups per station (5 minutes) cervical thoracic lumbar pelvic extremity Expect examiner interaction Graded on a Scantron
Importance of Topic 5/17/2013. Rethinking Proprioception Training & Ankle Instability. Dr Emily Splichal, DPM, MS, CES
 Rethinking Proprioception Training & Ankle Instability Dr Emily Splichal, DPM, MS, CES Evidence Based Fitness Academy Applying Research Achieving Results Importance of Topic JBJS 2010 study found average
Rethinking Proprioception Training & Ankle Instability Dr Emily Splichal, DPM, MS, CES Evidence Based Fitness Academy Applying Research Achieving Results Importance of Topic JBJS 2010 study found average
Dr Emily Splichal, DPM, MS, CES Evidence Based Fitness Academy Applying Research Achieving Results
 Rethinking Proprioception Training & Ankle Instability Dr Emily Splichal, DPM, MS, CES Evidence Based Fitness Academy Applying Research Achieving Results Importance of Topic JBJS 2010 study found average
Rethinking Proprioception Training & Ankle Instability Dr Emily Splichal, DPM, MS, CES Evidence Based Fitness Academy Applying Research Achieving Results Importance of Topic JBJS 2010 study found average
WEEKEND 2 Elbow. Elbow Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Manual and IASTM Treatment featuring the FAKTR Concept
 Manual and IASTM Treatment featuring the FAKTR Concept Tom Hyde, DC, DACBSP, FRCCSS (Hon), ICSSP, FAKTR, ART, GT, CRTP, CKTP, CSTI, FICC, Adjunct Faculty UWS Cyriax Friction Massage Simple yet effective
Manual and IASTM Treatment featuring the FAKTR Concept Tom Hyde, DC, DACBSP, FRCCSS (Hon), ICSSP, FAKTR, ART, GT, CRTP, CKTP, CSTI, FICC, Adjunct Faculty UWS Cyriax Friction Massage Simple yet effective
Running Athlete: Part C. Case Analysis Materials
 Running Athlete: Part C Case Analysis Materials Case 1 Subjective Examination (performed offcamera) Runs very sporadically, but generally 2-3 x per week around 2-4 miles Play recreational soccer Denies
Running Athlete: Part C Case Analysis Materials Case 1 Subjective Examination (performed offcamera) Runs very sporadically, but generally 2-3 x per week around 2-4 miles Play recreational soccer Denies
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Ankle Pain After a Sprain.
 Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
Fibular Malalignment in Subjects with Chronic Ankle Instability
 Fibular Malalignment in Subjects with Chronic Ankle Instability Takumi Kobayashi 1,2, Eiichi Suzuki 3, Naohito Yamazaki 3, Makoto Suzukawa 4, Atsushi Akaike 4, Kuniaki Shimizu 4, Kazuyoshi Gamada 1. 1
Fibular Malalignment in Subjects with Chronic Ankle Instability Takumi Kobayashi 1,2, Eiichi Suzuki 3, Naohito Yamazaki 3, Makoto Suzukawa 4, Atsushi Akaike 4, Kuniaki Shimizu 4, Kazuyoshi Gamada 1. 1
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612
 Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Lower Extremity Physical Performance Testing. Return to Function (Level I): Core Stability
: Core Stability") Physical performance testing is completed with patients in order to collect data and make observations regarding the overall function of the limb integrated into the entire functional unit of the body,
Physical performance testing is completed with patients in order to collect data and make observations regarding the overall function of the limb integrated into the entire functional unit of the body,
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle.
 Radiographic Evaluation of the Ankle.") X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
SMALL GROUP SESSION 16 January 8 th or 10 th. Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
ADVANCED MUSCULOSKELETAL TRAINING MUSMED
 ADVANCED MUSCULOSKELETAL TRAINING MUSMED Dr. Paul G. Conneely, Australia. www.musmed.com.au How to use a plum bob There are many types of plum bobs Examples of three different types. Procedure for using
ADVANCED MUSCULOSKELETAL TRAINING MUSMED Dr. Paul G. Conneely, Australia. www.musmed.com.au How to use a plum bob There are many types of plum bobs Examples of three different types. Procedure for using
Dorsal surface-the upper area or top of the foot. Terminology
 It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
It is important to learn the terminology as it relates to feet to properly communicate with referring physicians when necessary and to identify the relationship between the anatomical structure of the
Donald Stewart, MD. Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries
 Donald Stewart, MD Arlington Orthopedic Associates Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries Anatomy Mechanism of Injury Classification Diagnostic Tests Management
Donald Stewart, MD Arlington Orthopedic Associates Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries Anatomy Mechanism of Injury Classification Diagnostic Tests Management
Test-retest. The therapist can perform test: retest procedures throughout the treatment session as required.
 HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
HIP TREATMENT PROTOCOL Manual Therapy General Guidelines The goal of manual therapy: For this study, manipulative therapy includes specific manipulations (lowamplitude, high-velocity thrust techniques)
Arthritic history is similar to that of the hip. Add history of give way and locking, swelling
 KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity
KNEE VASU PAI Arthritic history is similar to that of the hip. Add history of give way and locking, swelling INJURY MECHANISM When How Sequence Progress Disability IKDC Activity I - Strenuous activity