Baby Basics - Common Concerns of the Infant Years Jennifer W. Swoyer, DO
|
|
|
- Barnard Mason
- 5 years ago
- Views:
Transcription

1 Baby Basics - Common Concerns of the Infant Years Jennifer W. Swoyer, DO

2



3 Baby Basics- Common Health Concerns of the Infant Years Jennifer W. Swoyer, DO Photos posted by permission of Danielle Campbell, DO Overview Cases representative of common health concerns of the neonate and infant Diagnosis Pathophysiology Management Answer boards style question **Key words/clues in bold throughout** Case #1 You are reviewing the lab work of a neonate at 24 hours of life. The total serum bilirubin is 15 mg/dl with a direct bilirubin of 0.2 mg/dl. The child was born at 40 weeks gestation with apgars of 9/9 and is doing well. On exam the child s sclera, face, and chest appear yellow and there is a one centimeter cephalohematoma on the R parietal region. The child is being exclusively breast fed and is feeding well. What is the appropriate management for this child? 1


4 Neonatal Jaundice Caused by: increased bilirubin production decreased bilirubin clearance increased enterohepatic circulation of bilirubin Kernicterus Term used to describe the chronic and permanent sequela of bilirubin toxicity Severe hyperbilirubinemia- TB >25 to 30 mg/dl At this level unconjugated bilirubin can cross the blood-brain barrier and cause cell death Hyperbilirubinemia Defined as TB >95th percentile on the hourspecific Bhutani nomogram in infants 35 weeks gestation Treatment Options Phototherapy Intensive Home Sunlight Exchange Transfusion IVIG, Phenobarb, Ursodeoxycholic acid, Metalloporphyrins 2


5 Risk Factors for the Development of Severe Hyperbilirubinemia Pre-discharge TB >95th percentile for age Jaundice within the first 24 hours of life Cephalohematoma or significant bruising from birth trauma Exclusive breastfeeding nursing is not going well and weight loss is excessive (>12 percent of birth weight) Hemolytic disease Gestational age 35 to 36 weeks or less Previous sibling who received phototherapy East Asian race Albumin < 3 g/dl 3
6 Indications for Phototherapy For infants at low risk ( 38 weeks gestation and without risk factors), intensive phototherapy is started at the following TB values: 24 hours of age: >12 mg/dl 48 hours of age: >15 mg/dl 72 hours of age: >18 mg/dl Infants in this category who have TB levels 2 to 3 mg/dl below the recommended levels may be treated with fiber optic or conventional phototherapy at home Indications for Phototherapy For infants at medium risk ( 38 weeks gestation with risk factors or 35 to 38 weeks gestation without risk factors), intensive phototherapy is started at the following TB values: 24 hours of age: >10 mg/dl 48 hours of age: >13 mg/dl 72 hours of age: >15 mg/dl The threshold for intervention may be lowered for infants closer to 35 weeks and raised for those closer to 37 6/7 weeks. Indications for Phototherapy For infants at high risk (35 to 38 weeks gestation with risk factors), phototherapy is initiated at the following TB values: 24 hours of age: > 8 mg/dl 48 hours of age: >11 mg/dl 72 hours of age: >13.5 mg/dl 4



7 Red Flag JAUNDICE IN THE FIRST 24 HOURS OF LIFE! Most likely due to hemolysis and will most likely need phototherapy or other interventions 5
8 Case #1 You are reviewing the lab work of a neonate at 24 hours of life. The total serum bilirubin is 15 mg/dl with a direct bilirubin of 0.2 mg/dl. The child was born at 40 weeks gestation with apgars of 9/9 and is doing well. On exam the child s sclera, face, and chest appear yellow and there is a one centimeter cephalohematoma on the R parietal region. What is the appropriate management for this child? Answer Choices A. IVIG B. initiate phototherapy C. exchange transfusion D. re-check TB in 48 hours E. do nothing Answer Choices A. IVIG B. initiate phototherapy C. exchange transfusion D. re-check TB in 48 hours E. do nothing 6

9 Case #2 During a well baby exam on a six month old infant that is new to your practice you assess for the red reflex. You are unable to illicit a red reflex in the infant s L eye and the reflex actually seems to be white. What is your initial step in management? Leukocoria Differential Retinoblastoma- 47 percent of cases in one series Persistent fetal vasculature Retinopathy of prematurity Cataract Coloboma (fissure or cleft) of choroid or optic disc Uveitis Toxocariasis Coats' disease Vitreous hemorrhage Retinal dysplasia 7
10 Retinoblastoma most common intraocular malignancy of childhood approximately 300 new cases per year usually diagnosed in children < 2 y/o sporadic and heritable forms If bilateral then always inherited Unilateral is usually sporadic Pathophysiology mutational inactivation of both alleles of the retinoblastoma (RB1) gene untreated retinoblastoma grows to fill the eye and destroys the internal architecture of the globe metastasizes after six months death occurs within years Case #2 During a well baby exam on a six month old infant that is new to your practice you assess for the red reflex. You are unable to illicit a red reflex in the infant s L eye and the reflex actually seems to be white. What is your initial step in management? 8
11 Answer Choices A. re check at 9 month well check B. dilate the eye in the office to better assess the retina C. send for ophthalmology evaluation D. start antibiotic drops and re check in one week E. do nothing Answer Choices A. re check at 9 month well check B. dilate the eye in the office to better assess the retina C. send for ophthalmology evaluation D. start antibiotic drops and re check in one week E. do nothing Case #3 At a routine two week well check you are examining an otherwise healthy full term female and notice a +Galeazzi test on the R and feel a clunk of entry with the Ortolani maneuver on the R. What is your first step in management? 9
12 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) abnormal development of the hip with respect to instability of the hip joint and dysplasia of the acetabulum Pathophysiology Ligamentous laxity predisposes the developing hip to mechanical forces that cause the femoral head to move outside of the acetabulum (dislocation) dysplasia appears to be the result of dislocation Risk Factors Female predominate- 4:1 F:M Breech positioning Family history of DDH Limited fetal mobility oligohydramnios firstborn infants 10
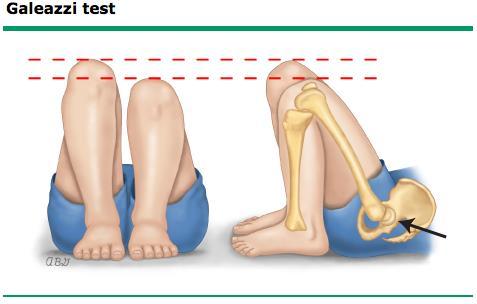
13 Screening Guidelines USPSTF evidence is insufficient to recommend routine screening for DDH as a means to prevent adverse outcomes newborn screening leads to over diagnosis of hips that do not benefit and may be harmed by treatment Screening Guidelines Pediatric Orthopaedic Society of North America (POSNA) Responds to USPSTF by pointing to the value of early diagnosis Recommends following the AAP Clinical Practice Guidelines assessment for DDH at every well-child visit until the child is walking normally Physical Exam Findings Asymmetry Apparent shortening of one femur + Galeazzi test Asymmetry of inguinal, thigh, or gluteal skin folds gait asymmetry Hip instability + Ortolani and Barlow maneuvers > 3 mos old: limitation of abduction (<45º) is the most reliable sign of DDH 11



14 Barlow Ortolani 12
15 Appropriate Management Definite signs of instability two weeks: directly to orthopedics without imaging > two weeks: age specific imaging or ortho AAP recommends US < 3 mos and XR > 3 mos Subtle or nonspecific findings Newborn: re-examine in two weeks Two-weeks old: re-examine in two weeks or US or refer to ortho > two weeks: age specific imaging Case #3 At a routine two week well check you are examining an otherwise healthy full term female and notice a +Galeazzi test on the R and feel a clunk of entry with the Ortolani maneuver on the R. What is your first step in management? Answer Options A. refer to ortho B. CT R hip C. US L hip D. Xray R hip E. Xray L hip 13
16 Answer Options A. refer to ortho B. CT R hip C. US L hip D. Xray R hip E. Xray L hip Case #4 You receive a call from a worried mom about her 4 month old son vomiting after feeds. The patient is exclusively breastfed and mom reports he spits up approximately one ounce of non-bloody, non-bilious vomitus after each feed. The infant is at the 50 th percentile for both height and weight, which has been consistent since birth. He is not excessively irritable, and has no other complaints or medical problems. What is the most appropriate treatment at this point? GERD Extremely common in healthy infants gastric fluids reflux into the esophagus 30 or more times daily normally Often results in regurgitation into the oral cavity Frequency decreases with increasing age Very uncommon in children > 18 mos 14

 Other chronic disorders (eg, HIV) Fever, Lethargy, Failure to thrive Uncomplicated GERD happy spitter Warning signs of complication")

17 GERD- Diagnostic Approach Uncomplicated Good weight gain feeds well not unusually irritable happy spitter Complicated Failure to thrive GI blood loss Recurrent PNA Warning Signs Bilious vomiting GI bleeding: hematemesis, hematochezia Consistently forceful vomiting Onset of vomiting after six months of life Constipation, Diarrhea Abdominal tenderness, distension Hepatosplenomegaly Bulging fontanelle Macro/microcephaly Seizures Genetic disorders (eg, Trisomy 21) Other chronic disorders (eg, HIV) Fever, Lethargy, Failure to thrive Uncomplicated GERD happy spitter Warning signs of complication absent No intervention is required If the reflux is causing significant adverse effects on quality of life trial of a milk-free diet thickening of feeds Acid suppression and prokinetic agents not valuable in treating children < 1 y/o with uncomplicated GERD Trial only if above measures fail and QOL an issue 15
18 Indications for Pharmacotherapy Esophagitis documented by endoscopic biopsies PPI most effective Eosinophilic esophagitis PPI + leukotriene inhibitor Case #4 You receive a call from a worried mom about her 4 month old son vomiting after feeds. The patient is exclusively breastfed and mom reports he spits up approximately one ounce of non-bloody, non-bilious vomitus after each feed. The infant is at the 50 th percentile for both height and weight, which has been consistent since birth, he is not excessively irritable, and has no other complaints or medical problems. What is the most appropriate treatment at this point? Answer Choices A. Stop breastfeeding and start soy formula immediately B. Order an upper GI series C. Reassure and follow D. Refer to GI E. Start PPI 16
19 Answer A. Stop breastfeeding and start soy formula immediately B. Order an upper GI series C. Reassure and follow D. Refer to GI E. Start PPI Case #5 You are evaluating a 3 week old male neonate in the office due to slow weight gain and vomiting. He has not yet reached birth weight. Mom says she is feeding him every one to two hours, but he vomits after each feeding and is still hungry afterwards. The vomitus is non-bloody and non-bilious. Mom describes the episodes of vomiting to be projectile. On exam you can palpate a small mass in the RUQ. What is the most appropriate treatment for this child? Pyloric Stenosis Hypertrophy of the pylorus eventually progressing to near-complete obstruction of the gastric outlet Male predominant- M:F = 4:1 to 6:1 Peak incidence of dx: 3-5 weeks of age 30% occur in firstborn children 17

20 Pyloric Stenosis Etiology Unknown May have a genetic predisposition Classic presentation 3- to 6-week-old male baby immediate postprandial, non-bilious, often projectile vomiting demands to be re-fed soon afterwards "hungry vomiter" Plyoric Stenosis Physical exam findings emaciated and dehydrated palpable "olive-like" mass at the lateral edge of the rectus abdominus in the RUQ Lab findings hypochloremic metabolic alkalosis hypokalemia may develop after 3 weeks of vomiting Pyloric Stenosis Diagnosis US vs upper GI Recommendation of which modality to chose varies from center to center and case to case Treatment Definitive treatment for pyloric stenosis is surgery Pyloromyotomy 18
21 Case #5 You are evaluating a 3 week old male neonate in the office due to slow weight gain and vomiting. He has not yet reached birth weight. Mom says she is feeding him every one to two hours, but he vomits after each feeding and is still hungry afterwards. The vomitus is non-bloody and non-bilious. Mom describes the episodes of vomiting to be projectile. On exam you can palpate a small mass in the RUQ. What is the most appropriate treatment for this child? Answer Choices A. increase frequency of feeds and decrease amount of each feed B. fundoplication C. start PPI D. re evaluate in two weeks E. pyloromyotomy Answer Choices A. increase frequency of feeds and decrease amount of each feed B. fundoplication C. start PPI D. re evaluate in two weeks E. pyloromyotomy 19
22 Case #6 A two year old male without significant past medical history taking no medications presents to your office c/o abdominal pain which began three hours ago. Pain is described as intermittent and crampy. Episodes are becoming more frequent and the patient tends to pull his legs up to his chest during the episodes. No n/v/d but his last stool did have some blood and mucous in it. On exam vital signs are stable, the abdomen is soft, mildly distended, and without peritoneal signs. You notice a sausage shaped mass on palpation of the RLQ. What is your diagnosis and treatment? Intussusception Invagination of a part of the intestine into itself Most common abdominal emergency in early childhood particularly in children younger than two years of age Most common cause of intestinal obstruction in infants between 6 and 36 months of age 60% before one y/o 80% before two y/o Male predominant- M:F = 3:2 Intussusception Occurs most often near the ileocecal junction Proximal segment of bowel, telescopes into a distal segment dragging the associated mesentery with it Leads to intestinal edema Can ultimately lead to ischemia, perforation, and peritonitis Etiology- most cases thought to be idiopathic but some increased incidence post-viral illness 20


 and sometimes mucous")
23 Intussusception Concept of lead point lesion or variation in the intestine that is trapped by peristalsis and dragged into a distal segment of the intestine meckel diverticulum polyp tumor hematoma- HSP vascular malformation thick inspisssated stool- CF Must be vigilant for pathological lead points Intussusception Presentation sudden onset- intermittent, severe, crampy, progressive abdominal pain inconsolable crying drawing up of the legs toward the abdomen Episodes occur at minute intervals Become more frequent Vomiting may follow episode Pain free between episodes Intussusception Physical Exam +/- abdominal distention sausage-shaped abdominal mass may be felt in the right side of the abdomen Stool contains blood (70%) and sometimes mucous Resembles currant jelly 21

24 Intussusception Classic triad Abdominal pain Sausage-shaped palpable mass Currant jelly stool Only seen in 15% of patients at presentation, so high index of suspicion necessary Intussusception Patients with classic presentation and no suspicion for perforation may proceed directly to contrast enema for dx and tx If diagnosis in question: Radiological studies US- modality of choice in most institutions Approaches 100% sensitivity/specificity Will see a bull's eye" or "coiled spring" lesion Plain film Less sensitive/specific than US signs of intestinal obstruction target sign- two concentric radiolucent circles superimposed on the right kidney crescent sign- soft tissue density projecting into the gas of the large bowel 22


25 Intussusception Treatment No perforation Nonoperative reduction using hydrostatic or pneumatic pressure by enema Water soluble contrast enema under fluoroscopic guidance Perforation suspected Laparotomy Recurrence recurs in approximately 10 percent of children after successful nonoperative reduction Should prompt search for pathological lead point 23
26 Case #6 A two year old male without significant past medical history taking no medications presents to your office c/o abdominal pain which began three hours ago. Pain is described as intermittent and crampy. Episodes are becoming closer together and the patient tends to pull his legs up to his chest during the episodes. No n/v/d but his last stool did have some blood and mucous in it. On exam vital signs are stable, the abdomen is soft, mildly distended, and without peritoneal signs. You notice a sausage shaped mass on palpation of the RLQ. What is your diagnosis and treatment? Answer Choices A. Mekels Diverticulum- watchful waiting B. Intussusception- laparotomy C. Mekels Diverticulum- laparatomy D. Intussusception- contrast enema E. Volvulus- laparotomy Answer Choices A. Mekels Diverticulum- watchful waiting B. Intussusception- laparotomy C. Mekels Diverticulum- laparatomy D. Intussusception- contrast enema E. Volvulus- laparotomy 24
27 Questions??? References Hay, Current Diagnosis and Treatment: Pediatrics, 19 th edition, 2009 Le, First Aid for the Family Medicine Boards, 2008 Rakel, Textbook of Family Medicine, 8 th edition, 2011 Sotirios, Transcutaneous Bilirubin Levels for the First 120 Postnatal Hours in Healthy Neonates, Pedaitrics, Vol. 125 No. 1, 1/1/2010. Waickus, Family Medicine Board Review, 4 th edition,
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
Objectives: Resources:
 Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Bowel Obstruction
 Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Safe and Healthy Beginnings. M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI
 Safe and Healthy Beginnings M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI jmaisels@beaumont.edu Risk Factors There are 2 kinds Those that increase the risk of subsequently developing a
Safe and Healthy Beginnings M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI jmaisels@beaumont.edu Risk Factors There are 2 kinds Those that increase the risk of subsequently developing a
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip
 Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Emergent Pediatric Ultrasound. Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound
 Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
GI POTPOURRI. What is the best diagnostic test? Presentation #1: Vomiting. I have no disclosures
 I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
I have no disclosures GI POTPOURRI Andi Marmor, MD Associate Professor, Pediatrics UCSF, San Francisco General Hospital Presentation #1: Vomiting Caraway, a 3 week old boy, is brought to your walk-in clinic
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Early detection of Retinoblastoma in children. Max Mantik
 Early detection of Retinoblastoma in children Max Mantik Introduction The most common primary intraocular malignancy of childhood 10 to 15 % of cancers that occur within the first year of life Typical
Early detection of Retinoblastoma in children Max Mantik Introduction The most common primary intraocular malignancy of childhood 10 to 15 % of cancers that occur within the first year of life Typical
11/8/12. KERNICTERUS: The reason we have to care about bilirubin. MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice
 MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice November 16, 2012 Orange County Lawrence M. Gartner, M.D. University of Chicago and Valley Center, California KERNICTERUS:
MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice November 16, 2012 Orange County Lawrence M. Gartner, M.D. University of Chicago and Valley Center, California KERNICTERUS:
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS
 Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Pediatric abdominal emergencies In the first year of life
 Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS
 DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Nothing
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Nothing
Clinical evaluation Jaundice skin and mucous membranes
 JAUNDICE Framework The definition of Neonatal Jaundice Billirubin Metabolism Special characteristic in neonates Dangerous of the Hyperbillirubinemia The diseases in relation with Neonatal Jaundice Objectives:
JAUNDICE Framework The definition of Neonatal Jaundice Billirubin Metabolism Special characteristic in neonates Dangerous of the Hyperbillirubinemia The diseases in relation with Neonatal Jaundice Objectives:
Adult Intussusception
 Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Gastroesophageal Reflux in Infants
 Gastroesophageal Reflux in Infants Lindsey Albenberg, DO Andrew Grossman, MD The Children s Hospital of Philadelphia 2013 Resident Education Series Reviewed by Jyoti Ramakrishna, MD of the Professional
Gastroesophageal Reflux in Infants Lindsey Albenberg, DO Andrew Grossman, MD The Children s Hospital of Philadelphia 2013 Resident Education Series Reviewed by Jyoti Ramakrishna, MD of the Professional
Pediatric Radiology Update
 Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Pediatric Imaging Studies: Congenital and Acquired Diagnoses
 Pediatric Imaging Studies: Congenital and Acquired Diagnoses Robin Foster MD FAAP FACEP Division Chief Pediatric Emergency Medicine Children s Hospital of Richmond at Virginia Commonwealth University Health
Pediatric Imaging Studies: Congenital and Acquired Diagnoses Robin Foster MD FAAP FACEP Division Chief Pediatric Emergency Medicine Children s Hospital of Richmond at Virginia Commonwealth University Health
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Gastroenterology
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Gastroenterology 1. GOAL: Understand the role of the general pediatrician in the assessment and management of patients with
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Gastroenterology 1. GOAL: Understand the role of the general pediatrician in the assessment and management of patients with
Differentiate IgE-mediated food allergy from non-ige mediated food allergy. List the foods and formulas most commonly associated with food allergy.
 Gastroenterology Description: The resident will be exposed to various clinical symptoms and diseases of the gastrointestinal tract which are commonly seen by the gastroenterologist. The resident will be
Gastroenterology Description: The resident will be exposed to various clinical symptoms and diseases of the gastrointestinal tract which are commonly seen by the gastroenterologist. The resident will be
Approach to the management of Hyperbilirubinemia in Term Newborn Infant
 Approach to the management of Hyperbilirubinemia in Term Newborn Infant Mohammad Bagher Hosseini MD Neonatologist Assosiated professor of Tabriz University of Medical science May 2011 Case1 You are called
Approach to the management of Hyperbilirubinemia in Term Newborn Infant Mohammad Bagher Hosseini MD Neonatologist Assosiated professor of Tabriz University of Medical science May 2011 Case1 You are called
Crash Cart therapy for Severe Jaundice. Dr Sandeep Kadam Neonatologist Pune
 Crash Cart therapy for Severe Jaundice Dr Sandeep Kadam Neonatologist Pune Objectives Assessment & stabilization Role of Investigations Management principles Steps for a crash-cart approach Assess Risk
Crash Cart therapy for Severe Jaundice Dr Sandeep Kadam Neonatologist Pune Objectives Assessment & stabilization Role of Investigations Management principles Steps for a crash-cart approach Assess Risk
Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
 Case Reports in Medicine Volume 2012, Article ID 340947, 4 pages doi:10.1155/2012/340947 Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
Case Reports in Medicine Volume 2012, Article ID 340947, 4 pages doi:10.1155/2012/340947 Case Report A Rare Case of Mucinous Adenocarcinoma of the Colon Presenting as Ileoileal Intussusception in an Adult
Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy?
 January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
Management of Common Paediatric Surgical G.I. Problems
 Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
Management of Common Paediatric Surgical G.I. Problems Dr. Loh Ser Kheng Dale Lincoln Senior Consultant Department of Paediatric Surgery National University Hospital National University Health System Tongue
The Hip Baby?? Baby Hippie??
 In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Chapter Outline. Structural defects. Obstructive disorders. Preview from Notesale.co.uk Page 3 of 98. Cleft lip and cleft palate
 Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
Structural defects Chapter Outline Cleft lip and cleft palate Page 3 of 98 Esophageal atresia and tracheoesophageal fistula Hernias Obstructive disorders Hypertrophic pyloric stenosis Intussusception Anorectal
OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General
![OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General](/thumbs/85/91909911.jpg "OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General") OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG
 7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
7 INTESTINAL OBSTRUCTION ESCAPED SURGERY: MECONIUM PLUG Oluwayemi IO 1 *, Ade-Ojo IP 2, Olofinbiyi BA 2 1. Department of Paediatrics, Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria
Background OVER 30 ISSUES IDENTIFIED! Key opportunities. What we ve done. October 31, 2012
 Background Hyperbilirubinemia: Developed by CMNRP s Jaundice Working Group Strategic planning meeting of CMNRP and its committees Multiple tables identified jaundice as a problem/priority Opportunity to
Background Hyperbilirubinemia: Developed by CMNRP s Jaundice Working Group Strategic planning meeting of CMNRP and its committees Multiple tables identified jaundice as a problem/priority Opportunity to
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier
 Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier GASTROENTERITIS History: Common diagnosis but may hide sinister pathology, so consider it a diagnosis of exclusion In cases of
Episode 19 part 2 Pediatric Abdominal Pain Prepared by Dr. Lucas Chartier GASTROENTERITIS History: Common diagnosis but may hide sinister pathology, so consider it a diagnosis of exclusion In cases of
SWISS SOCIETY OF NEONATOLOGY. Prenatal diagnosis and postnatal management of meconium pseudocysts
 SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
SWISS SOCIETY OF NEONATOLOGY Prenatal diagnosis and postnatal management of meconium pseudocysts September 2007 2 Burch E, Caduff JH, Hodel M, Berger TM, Neonatal and Pediatric Intensive Care Unit (BE,
A Crash Course in Failure to Thrive April 5, Kelly E. Wood, MD Clinical Assistant Professor Stead Family Department of Pediatrics
 A Crash Course in Failure to Thrive April 5, 2016 Kelly E. Wood, MD Clinical Assistant Professor Stead Family Department of Pediatrics Disclosures I have nothing to disclose Educational Objectives Define
A Crash Course in Failure to Thrive April 5, 2016 Kelly E. Wood, MD Clinical Assistant Professor Stead Family Department of Pediatrics Disclosures I have nothing to disclose Educational Objectives Define
SWISS SOCIETY OF NEONATOLOGY. Hypertrophic pyloric stenosis in a preterm infant
 SWISS SOCIETY OF NEONATOLOGY Hypertrophic pyloric stenosis in a preterm infant February 2014 2 Georgi R, Berger M, Schnyder I, Berger S, McDougall J, Division of Neonatology (GR, BM, McDJ), Department
SWISS SOCIETY OF NEONATOLOGY Hypertrophic pyloric stenosis in a preterm infant February 2014 2 Georgi R, Berger M, Schnyder I, Berger S, McDougall J, Division of Neonatology (GR, BM, McDJ), Department
Gastro Intestinal pg 1 of 6
 Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
Gastro Intestinal pg 1 of 6 Diabetic Ketoacidosis -Treatment differences True Na: adjust upward 1.6 mleq/l for every 100 mg/dl increase in blood glucose Potential serious CNS effects; 2-5% mortality rate
PEDIATRIC GI EMERGENCIES. AGE-RELATED DIAGNOSIS Early Infancy EXAMINATION TIPS PEDIATRIC ABDOMINAL PAIN. How Common Is It?
 PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
History taking in paediatrics PROF. DR STANISŁAW POPOWSKI REGIONAL SPECIALIZED CHILDREN S HOSPITAL IN OLSZTYN
 History taking in paediatrics PROF. DR STANISŁAW POPOWSKI REGIONAL SPECIALIZED CHILDREN S HOSPITAL IN OLSZTYN Paediatric history taking- Introduction Obtaining an accurate history is the critical first
History taking in paediatrics PROF. DR STANISŁAW POPOWSKI REGIONAL SPECIALIZED CHILDREN S HOSPITAL IN OLSZTYN Paediatric history taking- Introduction Obtaining an accurate history is the critical first
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Infantile Hypertrophic Pyloric Stenosis
 A Sonographic walk-through: Infantile Hypertrophic Pyloric Stenosis Tara K. Cielma, RDMS, RDCS, RVT, RT(S) Anjum N. Bandarkar, MD, Adebunmi O. Adeyiga, MD, Diagnostic Imaging and Radiology, Children s
A Sonographic walk-through: Infantile Hypertrophic Pyloric Stenosis Tara K. Cielma, RDMS, RDCS, RVT, RT(S) Anjum N. Bandarkar, MD, Adebunmi O. Adeyiga, MD, Diagnostic Imaging and Radiology, Children s
What is Your Diagnosis?
 What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
What is a Hip Dysplasia?
 What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
FACE THE EXAMINER. Hirschsprung s Disease in Newborns. (This section is meant for residents to check their understanding regarding a particular topic)
") Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
Journal of Neonatal Surgery 2013;2(4):51 FACE THE EXAMINER Hirschsprung s Disease in Newborns (This section is meant for residents to check their understanding regarding a particular topic) QUESTIONS 1.
CRACKCast Episode 172: Pediatric Gastrointestinal Disorders
 CRACKCast Episode 172: Pediatric Gastrointestinal Disorders Episode Overview Key concepts: Physiologic jaundice of the newborn and breast milk jaundice are the most common causes of jaundice in the neonatal
CRACKCast Episode 172: Pediatric Gastrointestinal Disorders Episode Overview Key concepts: Physiologic jaundice of the newborn and breast milk jaundice are the most common causes of jaundice in the neonatal
Common Pediatric Surgical Emergencies
 Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
The Case Begins. The case continued. Necrotizing Enterocolitis
 Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
Bugs, Drugs and Things that go Bump in the Night From ghoulies to ghosties and long leggety beasties & things that go bump in the night, good lord deliver us Old Cornish Prayer Caring for premature infant
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
WHAT IT MEANS or WHY YOU DO IT
 WHAT IT MEANS or WHY YOU DO IT Dr. Patrick Sauer Billings Clinic Pediatrics Objective Increase understanding of prenatal tests Increase understanding of routine newborn procedures Increase knowledge to
WHAT IT MEANS or WHY YOU DO IT Dr. Patrick Sauer Billings Clinic Pediatrics Objective Increase understanding of prenatal tests Increase understanding of routine newborn procedures Increase knowledge to
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Childhood hip conditions. Belen Carsi Paediatric Orthopaedic Consultant
 Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Developmental Dysplasia of the Hip
 Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Anal Atresia FACTS: There is no known cause for anal atresia. Children with anal atresia can lead very happy lives post surgery!
 Anal Atresia FACTS: Anal atresia affects 1 in 5,000 births and is slightly more common in boys. There is no known cause for this condition. With anal atresia, any of the following can occur: The anal passage
Anal Atresia FACTS: Anal atresia affects 1 in 5,000 births and is slightly more common in boys. There is no known cause for this condition. With anal atresia, any of the following can occur: The anal passage
Low temperature < 96.8 F (36.0 C) rectally that doesn't respond to warming
 rectally that doesn't respond to warming") Jaundice - Newborn Office Hours Telephone Triage Protocols Pediatric 2018 DEFINITION The skin has turned a yellow color At higher bilirubin levels, the whites of the eyes also turn yellow Included: Home
Jaundice - Newborn Office Hours Telephone Triage Protocols Pediatric 2018 DEFINITION The skin has turned a yellow color At higher bilirubin levels, the whites of the eyes also turn yellow Included: Home
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability
 Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST
 CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Ocular warning signs in GP practice: Paediatric Eye Pointers
 Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Defining incidence of intussusception (IS) in Bangladesh in preparation for a phase III trial of a new Rotavirus vaccine
 in Bangladesh in preparation for a phase III trial of a new Rotavirus vaccine") Defining incidence of intussusception (IS) in Bangladesh in preparation for a phase III trial of a new Rotavirus vaccine Principal Investigator: Dr. K. Zaman Final Report June 1, 2007 1 This study was
Defining incidence of intussusception (IS) in Bangladesh in preparation for a phase III trial of a new Rotavirus vaccine Principal Investigator: Dr. K. Zaman Final Report June 1, 2007 1 This study was
Gastro- Intestinal Bleeding in Children
 Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
Severe neonatal hyperbilirubinemia leading to exchange transfusion
 Original Article Medical Journal of the Islamic Republic of Iran (MJIRI) Iran University of Medical Sciences Severe neonatal hyperbilirubinemia leading to exchange transfusion Downloaded from mjiri.iums.ac.ir
Original Article Medical Journal of the Islamic Republic of Iran (MJIRI) Iran University of Medical Sciences Severe neonatal hyperbilirubinemia leading to exchange transfusion Downloaded from mjiri.iums.ac.ir
So Much More Than The PKU Test
 Newborn Metabolic Screening So Much More Than The PKU Test Sarah Viall, MSN, PPCNP BC Newborn Screening Program Coordinator Division of Genetics & Metabolism Conflicts of Interest I have no conflicts of
Newborn Metabolic Screening So Much More Than The PKU Test Sarah Viall, MSN, PPCNP BC Newborn Screening Program Coordinator Division of Genetics & Metabolism Conflicts of Interest I have no conflicts of
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR
 Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Four weeks of Intrauterine life
 Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
GUIDELINE FOR THE MANAGEMENT OF PROLONGED JAUNDICE IN BABIES. All babies admitted to hospital with prolonged jaundice
 GUIDELINE FOR THE MANAGEMENT OF PROLONGED JAUNDICE IN BABIES Reference No: Prolonged Jaundice Version No: 1 Applicable to All babies admitted to hospital with prolonged jaundice Classification of document:
GUIDELINE FOR THE MANAGEMENT OF PROLONGED JAUNDICE IN BABIES Reference No: Prolonged Jaundice Version No: 1 Applicable to All babies admitted to hospital with prolonged jaundice Classification of document:
Intussusception Secondary to a Meckel Diverticulum in an Adolescent
 48) Intussusception Secondary to a Meckel Diverticulum in an Adolescent Yener O., Demir M., Yigitbaşı R. Department of Surgery, Göztepe Training and Research Hospital, Istanbul, Turkey Received March 28,
48) Intussusception Secondary to a Meckel Diverticulum in an Adolescent Yener O., Demir M., Yigitbaşı R. Department of Surgery, Göztepe Training and Research Hospital, Istanbul, Turkey Received March 28,
Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff. Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012
 Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012 Objectives for Presentation At the end of this talk; the
Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012 Objectives for Presentation At the end of this talk; the
: Abdominal Emergencies
 INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
INTRODUCTION Abdominal complaints are very common in emergency medicine. The specific cause of the abdominal pain can very rarely be determined in the pre-hospital environment, however performing a good
CASE-BASED SESSION 1
 YLLSOM SENIORS TEACHING INITIATIVE M3 PROGRAMMES AY14/15 CONTENT PAGE CASE-BASED SESSION 1 Case 1: 40 year old man with abdominal pain 2 Case 2: 55 year old man with blood in her stool 4 Case 3: 45 year
YLLSOM SENIORS TEACHING INITIATIVE M3 PROGRAMMES AY14/15 CONTENT PAGE CASE-BASED SESSION 1 Case 1: 40 year old man with abdominal pain 2 Case 2: 55 year old man with blood in her stool 4 Case 3: 45 year
An Approach to Vomiting Block 10
 An Approach to Vomiting Block 10 Dr A Meyer Department of Pediatrics and Child Health Children vomit! Common Anxiety Need to find serious life-threatening disorders 1 The magnitude of the problem. To illustrate
An Approach to Vomiting Block 10 Dr A Meyer Department of Pediatrics and Child Health Children vomit! Common Anxiety Need to find serious life-threatening disorders 1 The magnitude of the problem. To illustrate
Developmental Dysplasia of the Hip
 1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP
 Severe Hyperbilirubinemia Prevention (SHP Toolkit) Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP Original Authors: Richard Bell, MD, Lisa Bollman, RN, CPHQ, Courtney Nisbet, RN,
Severe Hyperbilirubinemia Prevention (SHP Toolkit) Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP Original Authors: Richard Bell, MD, Lisa Bollman, RN, CPHQ, Courtney Nisbet, RN,
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST
 COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST Paediatric Gastroenterology : Referral Base Common problems Feeding difficulties in infancy Recurrent
COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST Paediatric Gastroenterology : Referral Base Common problems Feeding difficulties in infancy Recurrent
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Rectal Bleeding in Infancy
 Rectal Bleeding in Infancy Bittoo Kanwar, MD Assistant Professor of Pediatrics Division of Gastroenterology UCSF Objectives To understand the common and uncommon causes of rectal bleeding in infancy To
Rectal Bleeding in Infancy Bittoo Kanwar, MD Assistant Professor of Pediatrics Division of Gastroenterology UCSF Objectives To understand the common and uncommon causes of rectal bleeding in infancy To