August 2011 CE. Site code # E Pediatric Emergencies
|
|
|
- Barry Adams
- 5 years ago
- Views:
Transcription

1 August 2011 CE Site code # E-1211 Pediatric Emergencies Objectives by Mary Ann Zemla, RN Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit:
2 Date of CE presentation: August 2011 Topic: Pediatric Emergencies Behavioral Objectives: Upon successful completion of this module, the EMS provider will be able to: Describe components and purpose of the pediatric assessment triangle. Discuss pediatric vital signs. Describe the purpose of the Wong Baker Faces pain scale. Discuss airway assessment in the pediatric population Discuss use of the IO needle in the pediatric population. Identify possible causes of pediatric arrests. Describe defibrillator pad placement in the pediatric population. Describe the use of an AED in the pediatric population. Review a variety of EKG rhythms. Participate in medication calculation practice. Describe treatment per Region X SOP of the pediatric patient in a variety of rhythm disturbances. Describe the dosage and route for medications used in pediatric situations. Demonstrate use of a length based resuscitation tape (ie: Broselow Tape) to identify equipment and medication to use in a critical event. Demonstrate correct technique per AHA CPR guidelines for a neonate and infant. Actively participate in case scenarios for the pediatric population. Successfully complete the post quiz with a score of 80% or better. References: Aehlert, B. PALS Pediatric Advanced Life Support. Revised 2nd Edition. Elsevier American Academy of Pediatrics, 2nd Edition. Pediatric Education for Prehospital Professionals. Jones and Bartlett American Heart Association 2010 Guidelines for CPR and ECC Dietrich, A.M., Shaner, S., Campbell, J. Pediatric Trauma Life Support for Prehospital Care Providers 3rd Edition. ITLS Rahm, S. Pediatric Case Studies for the Paramedic. AAOS. Jones & Bartlett Region X SOP, March 2007, Revised May, 2008.
3 Pediatric Assessment Triangle The across the room assessment Appearance Work of breathing Group Practice #1 Circulation to skin 2 year old presents with shortness of breath. Mom states son has had a 3 day history of productive cough and runny nose. Child holding blanket & intently watching your movements while being held in mother s arms. RR appears to be within normal limits for age with no evidence of work of breathing. Chest expansion appears equal. Skin is pink Appearance - Work of breathing - Circulation - Is child sick/unstable? Or not sick/stable? Wong Baker Faces Pain Scale

4 Group Practice #2 An 8 month old infant presents with a cough, clear nasal discharge, and difficulty breathing. Mom states the infant has had a cold for the past 2 days. She is concerned because his breathing is different today and he has been feeding poorly. You note the infant appears tired & limp in mom s arms. Color is dusky. Respiratory rate is rapid & shallow. You note nasal flaring and intercostal & subcostal retractions. Appearance - Work of breathing Circulation Is child sick/unstable? Or not sick/stable? What action is necessary? Intraosseous Insertion 6 H s Hypovolemia give 20 ml/kg, repeat up to 60 ml/kg Hypoxia oxygenate Hydrogen ion acidosis ventilate Hyper/hypokalemia obtain history, check EKG for tall peaked T waves Hypothermia keep covered and warm Hypoglycemia most common metabolic problem in neonates 5 T s Tablets /drug overdose what has the child gotten in to? Tamponade, cardiac Tension pneumothorax check breath sounds, if bagging is there resistance? Equal rise and fall of chest wall? Thrombosis, coronary ACS Thrombosis, pulmonary embolism




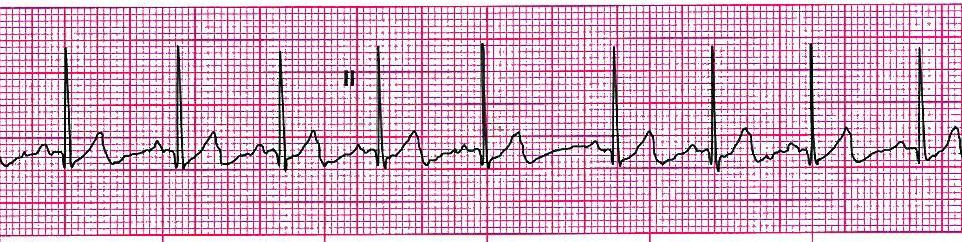
5 Rhythm Review Identify the following rhythm strips
6 Practice Calculating mg Problem #1 Pt weighs 44 pounds Administer 1:10,000 Epinephrine 0.01 mg/kg Problem #2 Pt weighs 56 pounds Administer Amiodarone 5 mg/kg Problem #3 Pt weighs 75 pounds Administer Benadryl 1 mg/kg How many mg does the calculation give to administer? Problem #4 Pt weighs 25 pounds Administer Versed 0.1 mg/kg
7 Drug Calculation Practice Formula #1 X ml = desired dose (mg) x vol on hand (ml) dose on hand (mg) Formula #2 mg on hand = mg ordered ml on hand x ml Practice Calculating Volume to Draw Up Use mg answers from previous problems Problem #1 Administer 0.2 mg. Epinephrine 1:10,000 packaged as 1 mg/10ml Problem #2 Administer 125 mg. Amiodarone packaged as 150mg/3ml Problem #3 Administer 34 mg. Benadryl packaged as 50mg/ml How much would you really administer to a patient per SOP? Problem #4 Administer 1.1mg.Versed packaged as 5mg/5ml
8 Group Practice #3 A 7 year-old girl is having difficulty breathing. You find the child sitting upright and leaning forward, supported by arms, mouth open. She is aware of your presence but unconcerned. You note nasal flaring, suprasternal retractions and use of intercostal muscles. You hear audible loud wheezes without a stethoscope. Color is pale. Caregiver states a history of asthma. A neighbor visited about 1 hour ago to show them a new cat. Respirations 38 and labored Pulse 140/minute B/P 94/62; capillary refill < 2 seconds Skin pale, warm & dry Speech limited to 2-3 word sentences Absent breath sounds bilaterally in bases, diminished throughout remaining lung fields Appearance - Work of breathing Circulation - Is child sick/unstable? Or not sick/stable? Case Scenario Small Group Practice Break into smaller groups. Each group to be assigned a scenario. Present your scenario to the group through discussion and role playing skills. All members need to take an active role and demonstrate at least one technique. You may use any available resources to answer your questions under the Instructions (texts, blackberries, SOP s, power point, websites, presenter, etc). Differentiating ST from SVT in the Pediatric Population Sinus Tachycardia SVT Rate Usually <220 infants; <180 children Usually >220 infants; >180 children Regularity Varies with activity Constant Onset/ termination Gradual Abrupt P waves Visible, normal Often indiscernible History Explanation can be given for rate Hx non-specific in absence of cardiac hx


9 Case Scenario #1 You receive a frantic 911 call from a mother screaming her 4 year-old is not breathing. Upon entering the home, the child is lying supine and motionless on the living room floor Child was electrocuted; is no longer in contact with the source Appearance unconscious, unresponsive Work of breathing none Circulation cyanotic S stuck a pin into an electrical outlet A none M vitamins P bilateral ear tubes 6 months ago L breakfast E playing in house, stuck a pin into the outlet First EKG Rhythm: EKG Rhythm after several rounds of CPR and medications: Instructions: Develop a general impression Determine your course of action Be prepared to role play the call to the group Demonstrate skills Performing CPR on a child Broselow tape Drawing up/preparing and administering medications Explain the rationale for medication used including dosing, and side effects/precautions

10 Case Scenario #2 911 call received for a 7 month-old infant with nausea and vomiting. Mother states child became ill earlier in the day and has had several episodes of vomiting and diarrhea. Child now refusing pedialyte and water. Appearance- Conscious, has weak cry, is listless Work of breathing - Airway open, respirations rapid and unlabored Circulation of skin - Pale S sudden onset this morning A- none M-vitamins; Motrin (last dose last night) P-none L-last night E-was fine yesterday afternoon. Started with fever last night (101.50F); Has vomited x3, diarrhea x5 episodes B/P not attempted P 190 R 50 SpO 2 97% room air Blood glucose - 90 Rhythm Strip Instructions: Develop a general impression Determine your course of action Be prepared to role play the call to the group Demonstrate skills Broselow tape Obtaining IV access Calculating and preparing fluid resuscitation Providing supportive ventilations via BVM Explain the rationale for interventions used and side effects/precautions

11 Case Scenario #3 You receive a 911 call from a mother stating her 6 month-old is having trouble breathing. Upon arrival you are met at the door with the mother holding the infant. The infant is in obvious respiratory distress, is coughing, and has a runny nose. Appearance -Conscious, decreased interactiveness Work of breathing - Nasal flaring; open mouth breathing, retractions evident Circulation - Pale, dry S Mother states the patient suddenly stopped breathing, turned blue; when she picked him up, the infant started to breathe A- none M- vitamins P- umbilical hernia repaired shortly after birth L-took half a bottle this morning; took longer than normal for intake E-cough and runny nose for 2 days; worsening today; low grade fever o F B/P not obtained (<3 years-old) P 200, regular R 50 SpO 2 93% Blood glucose 76 Rhythm strip: Instructions: Develop a general impression Determine your course of action Be prepared to role play the call to the group Demonstrate skills Broselow tape Securing the airway Regular Albuterol nebulizer and in-line delivery Supportive ventilations via BVM Explain the rationale for interventions used and side effects/precautions of interventions (airway, ventilating, med)
12 Case Scenario #4 You receive a 911 call for a 6 year old with an altered level of consciousness Child is sitting in mom s lap, conscious but not interactive Appears confused Appearance - Conscious but confused, sleepy Work of breathing - Respirations deep & rapid Circulation Skin pale, dry, poor turgor S Confused, tachycardic, tachypneic A- none M-none P- none L-last night E-Ill past few days. Mother thought it was the flu. Complained of stomach ache last night. Mother comments that the child has been very thirsty lately and going to the bathroom a lot. Mother states he may have lost weight recently. B/P 88/56 P 130 weak, regular R 40/minute and deep SpO2 97% Blood glucose high Instructions: Develop a general impression Determine your course of action Be prepared to role play the call to the group Demonstrate skills Obtaining a blood sugar sample on a child Broselow tape Drawing up/preparing and administering fluids List causes of altered mental status in the pediatric patient (ie: AEIOUTIPS) File: CE, EMS; CE Packets; 2011 ; August Handout Pediatric Emergencies
13 Pre-Quiz Paramedic And Basic Level From August 2011 CE Material Pediatric Emergencies Name Date 1. List the 3 components of the Pediatric Assessment Triangle. 2. What is the difference between respiratory distress and respiratory failure? Resp distress: Resp failure: 3. Is bradycardia an early or late sign of deterioration in a critically ill pediatric patient? 4. If a blood pressure cuff is too large for your patient, how will it affect your blood pressure results? 5. At what age is it appropriate to obtain blood pressures in the pediatric population in the field?
14 Aug 2011 Peds Pre-quiz 6. List at least 4 methods of non-pharmacological pain control measures. 7. List at least 4 signs or symptoms that a very young patient may be experiencing hypoglycemia. 8. Answer the questions in the columns for use of an AED in the following populations: Neonate Can an AED be used? Do you need a peds dose attenuator (special peds pads)? Can you use an adult AED? Infant Child Adult 9. Describe characteristics of sinus arrhythmia. When is it normally observed? 10. Describe neonatal ( not infant) CPR techniques. Compression depth: Ratio compressions to ventilations: Compression rate: If spontaneously breathing, rate to deliver ventilations via BVM: What is the goal heart rate to achieve when supporting ventilations? File: CE, EMS; CE Packets; Quizzes; 2011; August Pre-quiz
September 2013 CE. Site code # E Caring for the Pediatric Patient
 September 2013 CE Site code # 107200E-1213 Caring for the Pediatric Patient Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
September 2013 CE Site code # 107200E-1213 Caring for the Pediatric Patient Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
June 2009 CE. Site code # E-1209
 1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1
 POST-TEST: Module 1") Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
A silent chest is. Pediatrics II Asthma, seizures and cardiac arrest. Children are different. Cough variant asthma. Symptoms of severe distress
 Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
April 2011 CE. Site code # E The Patient With Heart Failure; CPAP as an Intervention
 April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
Quick review of Assessment. Pediatric Medical Assessment Review And Case Studies. Past Medical History. S.A.M.P.L.E. History is a great start.
 EMS Live at Night January 12 th, 2010 Pediatric Medical Assessment Review And Case Studies Brian Rogge RN Northwest Medstar Pediatric/Perinatal Team Quick review of Assessment S.A.M.P.L.E. History is a
EMS Live at Night January 12 th, 2010 Pediatric Medical Assessment Review And Case Studies Brian Rogge RN Northwest Medstar Pediatric/Perinatal Team Quick review of Assessment S.A.M.P.L.E. History is a
August 2012 CE. Site code # E Reading the Scene
 August 2012 CE Site code # 107200E-1212 Reading the Scene Prepared by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422 Date of
August 2012 CE Site code # 107200E-1212 Reading the Scene Prepared by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422 Date of
Naloxone Intranasal EMT OPTIONAL SKILL. Cell Phones and Pagers. Course Outline 09/2017
 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off.
 1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
Portage County EMS Patient Care Guidelines. Cardiac Arrest
 Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Pediatric Revised: 11/2013 (10 questions from this outline in the blue section) Emergency Medical
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
REGION 1 EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic, EMT Intermediate, EMT Paramedic. SMO: Pediatric Assessment Guidelines
 REGION 1 EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic, EMT Intermediate, EMT Paramedic SMO: Pediatric Assessment Guidelines Overview: Pediatric patients account for about 10% or less of
REGION 1 EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic, EMT Intermediate, EMT Paramedic SMO: Pediatric Assessment Guidelines Overview: Pediatric patients account for about 10% or less of
Pediatric. Pediatric Sick/Not Sick SICK... NOT SICK. The gift of a child. Pediatric Mike Helbock
 Pediatric Sick/Not Sick Developed and Authored by Mike Helbock M.I.C.P., NREMT-P Director EMS Associates Clinical Educator - Prehospital Medicine Seattle/King County EMS Division of Emergency Medicine
Pediatric Sick/Not Sick Developed and Authored by Mike Helbock M.I.C.P., NREMT-P Director EMS Associates Clinical Educator - Prehospital Medicine Seattle/King County EMS Division of Emergency Medicine
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
CETEP PRE-TEST For questions 1 through 3, consider the following scenario:
 CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
April 2009 Site Code #107200E-1209 The Patient with Dyspnea
 April 2009 Site Code #107200E-1209 The Patient with Dyspnea Prepared by: Bill Hoover, Medical Officer, Wauconda Fire Department Review/revisions by: Sharon Hopkins, RN, BSN, EMT-P To view on the website
April 2009 Site Code #107200E-1209 The Patient with Dyspnea Prepared by: Bill Hoover, Medical Officer, Wauconda Fire Department Review/revisions by: Sharon Hopkins, RN, BSN, EMT-P To view on the website
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies
 Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete The answers are
Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete The answers are
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
Chapter 11. Objectives. Objectives 01/09/2013. Baseline Vital Signs, Monitoring Devices, and History Taking
 Chapter 11 Baseline Vital Signs, Monitoring Devices, and History Taking Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 11 Baseline Vital Signs, Monitoring Devices, and History Taking Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL
 CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights
 Injection Administration EMT Optional Scope Highlights") Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights Nor-Cal EMS February 2018 version 1 Special Thank You To Seattle / King County EMS NY State Department of Health, Check
Epinephrine Intramuscular (IM) Injection Administration EMT Optional Scope Highlights Nor-Cal EMS February 2018 version 1 Special Thank You To Seattle / King County EMS NY State Department of Health, Check
Johnson County Emergency Medical Services Page 23
 Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
August 2013 CE. Site code # E-1213
 August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
August 2013 CE Site code # 107200E-1213 Caring for the Patient with CHF or COPD Objectives by Reviewed/revised by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
Bayfield-Ashland Counties EMS Council Pediatric Protocol PP-001 PREHOSPITAL CARE GUIDELINE
 INTRODUCTION: Pediatric emergencies may present a daunting challenge to prehospital care providers for a variety of reasons including: 1. The historical scarceness of primary training materials about the
INTRODUCTION: Pediatric emergencies may present a daunting challenge to prehospital care providers for a variety of reasons including: 1. The historical scarceness of primary training materials about the
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Beth Cetanyan, RN AHA RF Aka The GURU
 * Beth Cetanyan, RN AHA RF Aka The GURU *Discuss common causes of Pediatric CA *Review current PALS Guidelines *Through case presentations and discussion, become more comfortable and confident in providing
* Beth Cetanyan, RN AHA RF Aka The GURU *Discuss common causes of Pediatric CA *Review current PALS Guidelines *Through case presentations and discussion, become more comfortable and confident in providing
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Welcome to ACLS with Medical Education Angels!
 Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
PALS PRETEST. PALS Pretest
 PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
February 2009 CE. Site Code #107200E Revisions to the CMC EMS System CE Program and Determining ST Elevation on 12-Lead EKG s
 February 2009 CE Site Code #107200E-1209 Revisions to the CMC EMS System CE Program and Determining ST Elevation on 12-Lead EKG s Prepared by: Bill Glade, DC, Wauconda Fire Department Sharon Hopkins, RN,
February 2009 CE Site Code #107200E-1209 Revisions to the CMC EMS System CE Program and Determining ST Elevation on 12-Lead EKG s Prepared by: Bill Glade, DC, Wauconda Fire Department Sharon Hopkins, RN,
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Chapter 34. Objectives. Objectives 01/09/2013. Chest Trauma
 Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
PALS Study Guide 2016
 Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
Vital Signs. Vital Signs. Vital Signs
 Vital Signs Vital Signs Why do vital signs? Determine relative status of vital organs Establish baseline Monitor response to Rx, meds Observe trends Determine need for further evaluation, Rx, intervention
Vital Signs Vital Signs Why do vital signs? Determine relative status of vital organs Establish baseline Monitor response to Rx, meds Observe trends Determine need for further evaluation, Rx, intervention
Appendix (i) The ABCDE approach to the sick patient
 The ABCDE approach to the sick patient") Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Appendix (i) The ABCDE approach to the sick patient This appendix and the one following provide guidance on the initial approach and management of common medical emergencies which may arise in general
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Algorithm Focus. Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Perspective regarding the EMT- Intermediate algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Algorithms for the Conscious Patient Prehospital Medication Profiles Algorithm Focus Bradycardia Acute Pulmonary Edema and Shock Hypothermia
Pediatric Advanced E.M.T. Treatment Protocol
 Pediatric Advanced E.M.T. Treatment Protocol Important: Use Broselow tape for all pediatric and neonatal drug dosages and for equipment sizes. 06/12 Code 50 Emergency Childbirth Labor and Delivery Obtain
Pediatric Advanced E.M.T. Treatment Protocol Important: Use Broselow tape for all pediatric and neonatal drug dosages and for equipment sizes. 06/12 Code 50 Emergency Childbirth Labor and Delivery Obtain
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Pediatric Emergencies. September, 2018
 Pediatric Emergencies September, 2018 Introduction Children s bodies respond to significant injury and shock differently than adults. These differences may be subtle and difficult to recognize EMS providers
Pediatric Emergencies September, 2018 Introduction Children s bodies respond to significant injury and shock differently than adults. These differences may be subtle and difficult to recognize EMS providers
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Pediatric Resuscitation
 Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Advanced Life Support
 Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Paediatric Enhanced Life Support Scenarios
 Paediatric Enhanced Life Support Scenarios These scenarios should be used to assess staff undertaking the Paediatric Enhanced Life Support course within the Black Country Partnership NHS Foundation Trust.
Paediatric Enhanced Life Support Scenarios These scenarios should be used to assess staff undertaking the Paediatric Enhanced Life Support course within the Black Country Partnership NHS Foundation Trust.
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
PALS PROVIDER Course Study Guide/Pre-Test
 PALS PROVIDER Course Study Guide/Pre-Test *PLEASE COMPLETE AND BRING THIS DOCUMENT WITH YOU TO CLASS* Heartland CPR, llc 8101 NW 10 th St, Suite #C3 Oklahoma City, OK 73127 405-603-6666 contact@heartlandcpr.com
PALS PROVIDER Course Study Guide/Pre-Test *PLEASE COMPLETE AND BRING THIS DOCUMENT WITH YOU TO CLASS* Heartland CPR, llc 8101 NW 10 th St, Suite #C3 Oklahoma City, OK 73127 405-603-6666 contact@heartlandcpr.com
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
! Please rate by checking ( ): 5 = Highest, best or most.! 1 = Lowest, least, or worst
: 5 = Highest, best or most.! 1 = Lowest, least, or worst") Day 1 Evaluation Please rate by checking ( ): 5 = Highest, best or most. Please rate the extent to which your personal objectives were met 20 6 1 Please rate the appropriateness of the physical facilities
Day 1 Evaluation Please rate by checking ( ): 5 = Highest, best or most. Please rate the extent to which your personal objectives were met 20 6 1 Please rate the appropriateness of the physical facilities
March 2009 CE. Site code # E Carbon Monoxide, Smoke Inhalation, Cyanide Poisoning and Medical Rehab
 March 2009 CE Site code #107200-E-1209 Carbon Monoxide, Smoke Inhalation, Cyanide Poisoning and Medical Rehab Objectives and materials by: F/M Dan Ogurek Countryside Fire Protection Dist. Packet Prepared
March 2009 CE Site code #107200-E-1209 Carbon Monoxide, Smoke Inhalation, Cyanide Poisoning and Medical Rehab Objectives and materials by: F/M Dan Ogurek Countryside Fire Protection Dist. Packet Prepared
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Consider Treatable Underlying Causes Early
 Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS
 EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
EL DORADO COUNTY EMS AGENCY PREHOSPITAL PROTOCOLS Effective: July 1, 2017 Reviewed: November 9, 2016 Revised: November 9, 2016 EMS Agency Medical Director ALLERGIC REACTION/ANAPHYLAXIS ADULT BLS TREATMENT
Chapter 29. Objectives. Objectives 01/09/2013. Burns
 Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Baseline Vital Signs and SAMPLE History. Chapter 5
 Baseline Vital Signs and SAMPLE History Chapter 5 Baseline Vital Signs and SAMPLE History Assessment is the most complex skill EMT-Bs learn. During assessment you will: Gather key information. Evaluate
Baseline Vital Signs and SAMPLE History Chapter 5 Baseline Vital Signs and SAMPLE History Assessment is the most complex skill EMT-Bs learn. During assessment you will: Gather key information. Evaluate
Topic: Baseline Vitals and Sample History Company Drill
 Baseline Vitals and Sample History Company Drill Instructor Guide Session Reference: 1 Topic: Baseline Vitals and Sample History Company Drill Level of Instruction: 2 Time Required: Three Hours Materials
Baseline Vitals and Sample History Company Drill Instructor Guide Session Reference: 1 Topic: Baseline Vitals and Sample History Company Drill Level of Instruction: 2 Time Required: Three Hours Materials
A guide to writing clear, concise EMS reports using SIREN
 A guide to writing clear, concise EMS reports using SIREN OBJECTIVE: EMS narratives will document patient assessment findings, interventions, and patient response to interventions such that ED providers
A guide to writing clear, concise EMS reports using SIREN OBJECTIVE: EMS narratives will document patient assessment findings, interventions, and patient response to interventions such that ED providers
Airway and Breathing
 Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
EMT OPTIONAL SKILL. Cell Phones and Pagers. Epinephrine Auto-injector. Course Outline 9/2017
 EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
EMT OPTIONAL SKILL Epinephrine Auto-injector Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
Final FRCA Written PAEDIATRICS Past Paper Questions November March 2014
 Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010
 ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
ILCOR, ARC & NZRC PAEDIATRIC RESUSCITATION RECOMMENDATIONS 2010 Jim Tibballs Officer, RCH Convenor, Paediatric Sub-Committee, (ARC) ARC Paediatric Representative International Liaison Committee on (ILCOR)
Protocol Update 2019
 Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Chapter 12 - Vital_Signs_and_Monitoring_Devices
 Introduction to Emergency Medical Care 1 OBJECTIVES 12.1 Define key terms introduced in this chapter. Slides 13 15, 17, 21 22, 26, 28, 30, 32 33, 35, 44, 47 48, 50, 55, 60 12.2 Identify the vital signs
Introduction to Emergency Medical Care 1 OBJECTIVES 12.1 Define key terms introduced in this chapter. Slides 13 15, 17, 21 22, 26, 28, 30, 32 33, 35, 44, 47 48, 50, 55, 60 12.2 Identify the vital signs
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY. Administration of Naloxone for Opiate Overdose
 SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Naloxone for Opiate Overdose Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT) who
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Naloxone for Opiate Overdose Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT) who