JBI GRADE Research School Workshop. Presented by JBI Adelaide GRADE Centre Staff
|
|
|
- Anissa Carroll
- 5 years ago
- Views:
Transcription


1 JBI GRADE Research School Workshop Presented by JBI Adelaide GRADE Centre Staff
2 Declarations of Interest Presented by members of the GRADE Working Group The Joanna Briggs Institute and JBI methodological groups Members of the JBI Adelaide GRADE Centre Peer reviewers/editors for the JBI Database of Systematic Reviews and Implementation Reports
3 Objectives 1. To introduce participants to the work of the GRADE working group 2. To explain the rationale behind the GRADE approach 3. To explain the key factors to consider when assessing certainty of the evidence 4. To provide advice about additional resources for guidance following the workshop
4 Icebreaker: What do you know about GRADE? Examples: Read published papers on GRADE methods Have prepared a systematic review and a summary of findings table Have attended a GRADE meeting, workshop or talk Have said you will use GRADE in your protocol Have used GRADE methods for guideline devleopment...nothing yet! What do you want to know more about?
5 Session 1: Introduction to GRADE
6 Who are GRADE? Grading of Recommendations Assessment, Development and Evaluation (GRADE) International working group Endorsed by many EBHC organisations Website:
7 History of GRADE Began as an informal working group in 2000, largely out of McMaster University Informal collaboration of researchers/guideline developers with interest in methodology Purpose: to develop a common system for grading the quality (certainty) of evidence and the strength of recommendations that is transparent and sensible Workshops at Cochrane, WHO and GIN since 2000


8 Over 100 organisations From 19 countries


9 In Australia Systematic Reviewers JBI and Cochrane explicitly endorse the use of GRADE methods and require GRADE

10 In Australia Guideline Developers

11



12 1. Train, promote, disseminate and implement GRADE within ANZ and the JBC 2. Act as a central hub for GRADE in Oceania 3. Contribute to GRADE methods Pictured: JBI Adelaide GRADE Center Director Associate Professor Zachary Munn (centre) with GRADE Working Group co-chairs Professor Holger Schünemann (left) and Distinguished Professor Gordon Guyatt (right)
13 Session 2: Why GRADE?

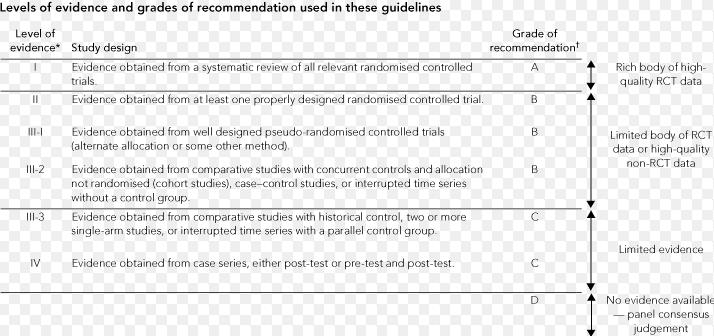
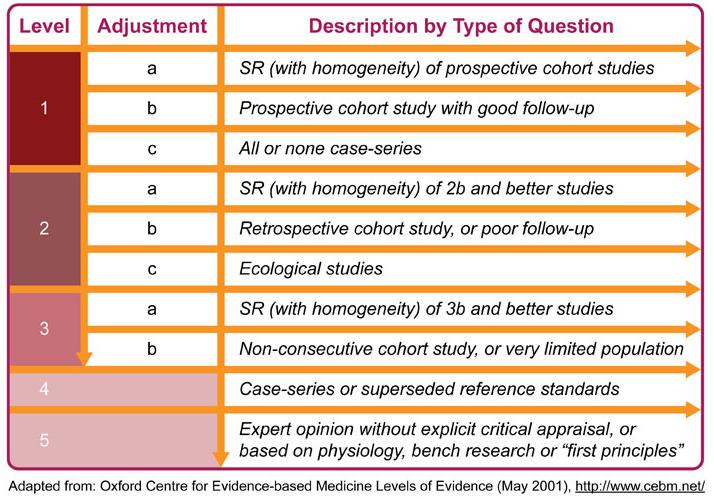
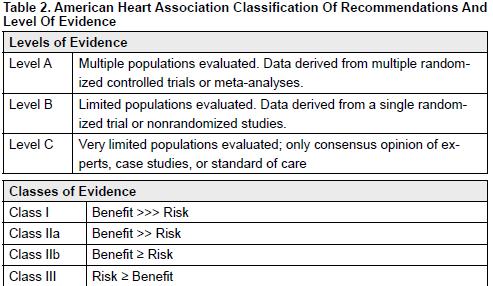
14 Levels of Evidence Grades of Recommendation Designate study types Better study designs, with greater methodological quality, are ranked higher Assigned to findings of research Assist in applying research into practice Recommendations assigned a Grade
15
16 Levels of Evidence The first hierarchy of evidence quality was created, where evidence of the highest quality would have to come from at least one randomized trial, and at the bottom of that hierarchy of evidence were opinions of respected experts without any empirical evidence. That seems really simple in retrospect, but, actually, it was an incredible breakthrough to address the way we dealt with the large amount of available research evidence. It made it feasible to sift through evidence in a meaningful way and apply the principles of using the best quality and least biased evidence. Paul Glasziou Guyatt, Gordon, Victor Montori, Holger Schünemann, and Paul Glasziou. "When Can We Be Confident about Estimates of Treatment Effects?." The Medical Roundtable General Medicine Edition (2015).
17 Eventually, the traditional hierarchies of evidence started to fall apart due to attempts to fit too many elements as well as a lack of standardization. Now, we have to move on to a new phase of trying to unify the principles Guyatt, Gordon, Victor Montori, Holger Schünemann, and Paul Glasziou. "When Can We Be Confident about Estimates of Treatment Effects?." The Medical Roundtable General Medicine Edition (2015).

18 Why GRADE? 18
19 GOBSAT Method Initial approach to development of recommendations within guidelines Based on expert opinion, powerful figures, eminence based medicine Good old boys sat around the table
20 clinical guidelines/clinical_guidelines/documents/ncg97.pdf

21
22
23 Forming recommendations with GRADE Patients values and preferences Equity Balance between benefits, harms and burdens Certainty of Evidence Resource use Feasibility How do we determine quality of the evidence? University of Adelaide 23
24 Quality of the evidence If not by study design: How can we ascertain the quality of the evidence? What impacts our confidence regarding the evidence?
25 Activity 1: Example meta-analysis discussion From the example provided, what information would increase or decrease your confidence in these results?
26 Discussion results Decrease Increase
27 GRADE Decrease Methodological limitations (risk of bias) Indirectness (i.e applicability, generalisability, transferability etc) Inconsistency (heterogeneity) Imprecision (uncertainty) Publication bias Increase Large, consistent, precise effect All plausible biases underestimate the effect Dose response effect
28 Summing up: So why GRADE? 1. Transparent approach to rating quality 2. Separation between quality of evidence and strength of recommendation 3. Considers issues other than study design 4. Focuses on outcomes, not studies 5. Clear guidance for developing and establishing recommendations 6. Supported and endorsed by the international systematic review and guideline development community
29 GRADE is much more than a rating system. It offers a transparent and structured process for developing and presenting evidence summaries for systematic reviews and guidelines in health care and for carrying out the steps involved in developing recommendations. GRADE specifies an approach to framing questions, choosing outcomes of interest and rating their importance, evaluating the evidence, and incorporating evidence with considerations of values and preferences of patients and society to arrive at recommendations. Furthermore, it provides clinicians and patients with a guide to using those recommendations in clinical practice and policy makers with a guide to their use in health policy. Guyatt et al 2011
30 Session 3: Introduction to the GRADE approach
31 Systematic review process 1. define the question 2. plan eligibility criteria Historically not a lot of 3. plan methods guidance for this 4. search for studies 5. apply eligibility criteria 6. collect data 7. assess studies for risk of bias 8. analyze and present results 9. interpret results and draw conclusions 10.improve and update review
32 Key principle Important to communicate Results Our certainty in these results?
33 Magnitude of Effect (results) Certainty/quality/ confidence in the evidence
34 Quality/certainty in the evidence varies from HIGH MODERATE LOW VERY LOW RCT Risk of bias Indirectness Inconsistency Imprecision Publication bias NRS Dose response Large effect Plausible confounding

35 Framing questions and selecting outcomes Use PICO for your SR or Guideline question/s Include a range of outcomes, addressing benefit and harms SRs often miss harms, guideline panels need to consider all outcomes for decision making Should include all potential patient important outcomes Classify outcomes regarding importance for decision making: Critical Important but not critical Of limited importance
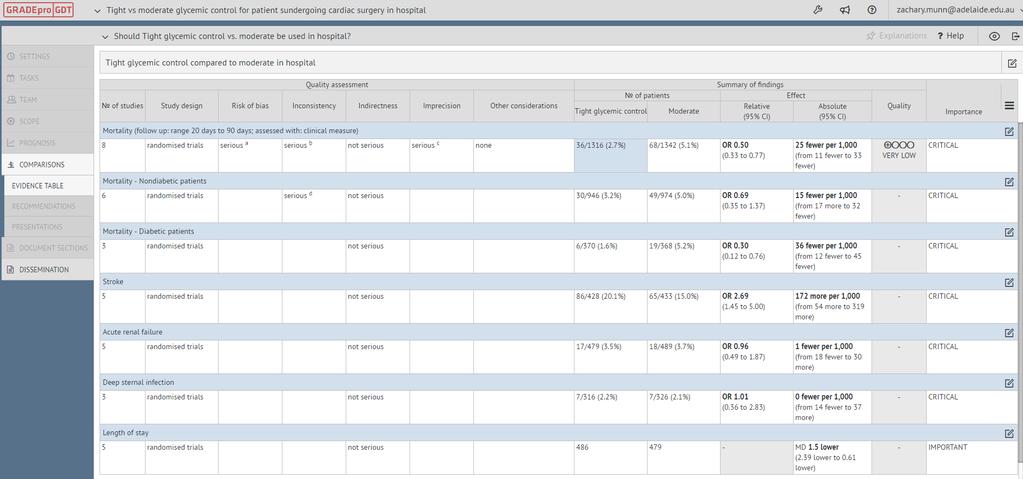
36 Activity 2: Example outcomes Hyperglycaemia is a common response to critical illness and metabolic stress during the perioperative period of cardiac surgery. The methods of glycemic control include bolus administration of subcutaneous insulin or directed continuous insulin infusion. However, there remains considerable controversy regarding the role of tight glycaemic control (aiming for 80 to 150 mg/dl, mmol/l) during and/or after cardiac surgery. The objective of this review was to identify the effectiveness of tight glycaemic (aiming for 80 to 150 mg/dl or mmol/l) control compared to conventional glycaemic control (160 to 250 mg/dl or mmol/l).
37 Activity 2: Classifying outcomes Turn to your workbook and begin activity 2. Have you thought about...? What would be important for someone making a decision? Have you considered benefits as well as harms? What outcomes are likely included in studies, and what may be missed? What outcomes should be included in a summary of findings table or evidence profile?
38 Activity 2: Example outcomes Outcomes Mortality (all cause) Infection (deep sternal or other) Length of stay Time on mechanical ventilation Acute renal failure Stroke Hypoglycaemic episode Health related quality of life Weight gain Ranking
39 Activity 2: Example outcomes Outcomes Mortality (all cause) Infection (deep sternal or other) Length of stay Time on mechanical ventilation Acute renal failure Stroke Hypoglycaemic episode Health related quality of life Weight gain Ranking 9 (critical) 7 (critical) 7 (critical) 6 (important) 7 (critical) 8 (critical) 7 (critical) 7 (critical) 3 (of limited importance)
40 Implications for HDR students Effectiveness reviews: in your protocol, you need to state what outcomes will be included in your summary of findings table and assessed using the GRADE criteria. This can be done in the Assessing Confidence section of the protocol. These should be the 7 most important outcomes, not necessarily only the primary outcomes. These should include both beneficial and harmful outcomes. These should not be surrogate outcomes where possible
41 Session 4: Determining quality (certainty) of the evidence
42 What does this mean? High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
43 GRADEing the evidence Pre ranking Evidence from RCTs start as high, Observational studies as low Quality of evidence ranges from High Moderate Low Very low Can be downgraded 1 or 2 points for each area of concern Maximum downgrade of 3 points overall
44 GRADE domains Risk of Bias Inconsistency Indirectness Imprecision Rating (circle one) No serious ( 1) very serious ( 2) No serious ( 1) very serious ( 2) No serious ( 1) very serious ( 2) No serious ( 1) very serious ( 2) Footnotes (explain judgements) Certainty of evidence (Circle one) High Moderate Low Publication Bias Undetected Strongly suspected ( 1) Very Low Other (upgrading factors, circle all that apply) Large effect (+1 or +2) Dose response (+1) No Plausible confounding (+1)
45 Session 5: Study limitations (Risk of bias)
46 Bias A bias is a systematic error, or deviation from the truth, in results or inferences (Higgins & Altman, 2008) Bias in research may lead to misleading estimates of effect Studies may be at risk of bias due to issues with the conceptualization, design, conduct or interpretation of the study There are many different types of bias that can arise in research
47 Type of bias Description Relevant domains in Cochrane s Risk of bias tool Selection bias. Performance bias. Detection bias. Attrition bias. Reporting bias. Other bias Systematic differences between baseline characteristics of the groups that are compared. Systematic differences between groups in the care that is provided, or in exposure to factors other than the interventions of interest. Systematic differences between groups in how outcomes are determined. Systematic differences between groups in withdrawals from a study. Systematic differences between reported and unreported findings. Stopping trial early Invalid outcome measures Cluster or crossover trial issues Sequence generation. Allocation concealment. Blinding of participants and personnel. Other potential threats to validity. Blinding of outcome assessment. Other potential threats to validity. Incomplete outcome data Selective outcome reporting Other types of bias
48 Overall Risk of Bias Use the risk of bias assessment from all studies to determine overall risk of bias This can be difficult!
49 So how should we do it? Can you simply count the number of yes compared to no s? Or high vs low risk? Rather than an average, consider judiciously the contribution of each study Consider whether a no answer on JBI checklist actually would result in a bias What about weighting? Risk of bias of studies providing more weight to the analysis should be considered more Should trials with high risk of bias be excluded? Potentially, although may be implications for imprecision
50 Key principles We suggest the following principles: In deciding on the overall quality of evidence, one does not average across studies (for instance if some studies have no serious limitations, some serious limitations, and some very serious limitations, one does not automatically rate quality down by one level because of an average rating of serious limitations). Rather, judicious consideration of the contribution of each study, with a general guide to focus on the high quality studies, is warranted. The judicious consideration requires evaluating the extent to which each trial contributes toward the estimate of magnitude of effect. This contribution will usually reflect study sample size and number of outcome events larger trials with many events will contribute more, much larger trials with many more events will contribute much more. One should be conservative in the judgment of rating down. That is, one should be confident that there is substantial risk of bias across most of the body of available evidence before one rates down for risk of bias. The risk of bias should be considered in the context of other limitations. If, for instance, reviewers find themselves in a close call situation with respect to two quality issues (risk of bias and, say, precision), we suggest rating down for at least one of the two. Reviewers will face close call situations. They should both acknowledge that they are in such a situation, make it explicit why they think this is the case, and make the reasons for their ultimate judgment apparent. (GRADE Handbook)
51 Final points You still need to assess risk of bias if only one study You still need to assess risk of bias if you cannot pool the results You still need to assess risk of bias is there is little information regarding the risk of bias
52 Session 6: Inconsistency
53 Inconsistency of results (unexplained heterogeneity) Widely differing estimates of treatment effect if inconsistency exists, look for explanation patients, intervention, comparator, outcome if unexplained inconsistency lower quality
54 Identifying heterogeneity Heterogeneity can be determined by: Wide variance of point estimates Minimal or no overlap of confidence intervals Statistical tests standard chi squared test (Cochran Q test) I square statistic (I2)
55 Interpreting I 2 Generally in regards to heterogeneity: < 40% may be low 30 60% may be moderate 50 90% may be substantial % may be considerable (GRADE Handbook)
56 Example Forest Plot: Activity 3
57 Forest Plot example: Continuous Data
58 Note: As we define quality of evidence for a guideline, inconsistency is important only when it reduces confidence in results in relation to a particular decision. Even when inconsistency is large, it may not reduce confidence in results regarding a particular decision. Guideline developers may or may not consider this degree of variability important. Systematic review authors, much less in a position to judge whether the apparent high heterogeneity can be dismissed on the grounds that it is unimportant, are more likely to rate down for inconsistency.
59 Caution: subgroups Although the issue is controversial, we recommend that metaanalyses include formal tests of whether a priori hypotheses explain inconsistency between important subgroups If inconsistency can be explained by differences in populations, interventions or outcomes, review authors should offer different estimates across patient groups, interventions, or outcomes. Guideline panelists are then likely to offer different recommendations for different patient groups and interventions. If study methods provide a compelling explanation for differences in results between studies, then authors should consider focusing on effect estimates from studies with a lower risk of bias.
60
61 Session 7: Imprecision
62 Imprecision Small sample size Small number of events Wide confidence intervals uncertainty about magnitude of effect Optimal information size Different for SRs vs Guidelines Guidelines contextualized for decision making and recommendations SRs free of this context
63 Optimal Information Size If the total number of patients included in a systematic review is less than the number of patients generated by a conventional sample size calculation for a single adequately powered trial, consider rating down for imprecision.
64 Total Number of Events Relative Risk Reduction Implications for meeting OIS threshold 100 or less < 30% Will almost never meet threshold whatever control event rate % Will meet threshold for control event rates for ~ 25% or greater % Will meet threshold for control event rates for ~ 50% or greater % Will meet threshold only for control event rates for ~ 80% or greater 300 > 30% Will meet threshold % Will meet threshold for control event rates ~ 25% or greater % Will meet threshold for control event rates ~ 60% or greater 400 or more > 25% Will meet threshold for any control event rate Guyatt or more 20% Will meet threshold for control event rates of ~ 40% or greater
65 OIS rule of thumb: dichotomous: 300 events continuous: 400 participants HOWEVER, carefully consider the OIS and event rate
66 Confidence intervals do not include null effect, and are all on one side of the decision threshold showing appreciable benefit: Do not downgrade
67 Confidence intervals do not include null effect, but do include appreciable benefit and cross the decision making threshold: May downgrade
68 Confidence intervals do include null effect, but do not reach appreciable harm or benefit: May not downgrade
69 Confidence intervals do include null effect, and appreciable benefit: Downgrade
70 Confidence intervals very wide, but all on one side of the decision threshold showing appreciable harm: May not downgrade
71 Discussion: would you rate down?
72 Forest Plot example: Continuous Data
73 Session 8: Indirectness
74 Directness of Evidence (generalizability, transferability, external validity, applicability) Confidence is increased when we have direct evidence Ask: is the evidence applicable to our relevant question? Population Intervention Comparisons Outcome
75 Population Ask: Is the population included in these studies similar to those in my question? Indirect evidence examples: Evidence from high income countries compared to LMIC All women as compared to pregnant women Sick (or sicker) people compared to all people (mild vs severe) Adults compared to children May be addressed in subgroups where appropriate and possible Can indicate different levels of risk for different groups Can create different SoF tables for different groups, therefore won t need to downgrade
76 Interventions Ask: Is the population included in these studies similar to those in my question? Older technology compared to newer technology Co interventions Different doses, different delivery, different providers
77 Outcomes Make sure to: Choose patient important outcomes Avoid surrogate outcomes If surrogate outcomes used, is there a strong association between the surrogate and patient important outcome?
78 Comparisons Are comparisons direct or indirect? Interested in A vs B A vs Control B vs Control May downgrade
79 Note: Authors of systematic reviews should answer the health care question they asked and, thus, they will rate the directness of evidence they found. The considerations made by the authors of systematic reviews may be different than those of guideline panels that use the systematic reviews. The more clearly and explicitly the health care question was formulated the easier it will be for the users to understand systematic review authors' judgments.
80 Session 9: Publication bias
81 Publication Bias Publication bias occurs when the published studies differ systematically from all conducted studies on a topic It is a serious threat to the validity of systematic reviews and metaanalyses Should always be suspected Only small positive studies For profit interest Various methods to evaluate none perfect, but clearly a problem
82 Funnel Plot Funnel plots are a method of investigating the retrieved studies in a meta analysis for publication bias A funnel plot is a scatter plot in which an effect estimate of each study is plotted against a measure of size or precision If no bias, expect symmetric and inverted funnel If bias, expect asymmetric or skewed shape Can also investigate small study effects
83 Funnel Plot A statistical test for funnel plot asymmetry investigates whether the association between effect estimate and measure of study size or precision is larger than what can be expected to have occurred by chance Egger test, Begg test, and Harbord test are the most popular statistical tests Due to low power a finding of no evidence of asymmetry does not serve to exclude bias Generally 10 studies are considered the minimum number to justify a funnel plot When there are less than 30 studies, the statistical power of all three tests is very low and results should be interpreted with caution
84 Figure 1 Figure 2 Figure 3 Taken from: Sterne et al 2005
85 What do we do? It is extremely difficult to be confident that publication bias is absent and almost as difficult to place a threshold on when to rate down quality of evidence due to the strong suspicion of publication bias. For this reason GRADE suggests rating down quality of evidence for publication bias by a maximum of one level. (GRADE Handbook) Consider: study size (small studies vs. large studies) lag bias (early publication of positive results) search strategy (was it comprehensive?) asymmetry in funnel plot.
86 Session 10: Factors that raise quality
87 Raising the quality Initially classified as low, a body of evidence from observational studies can be rated up Consideration of factors reducing quality of evidence must precede consideration of reasons for rating it up. 5 factors for rating down quality of evidence must be rated prior to the 3 factors for rating it up The decision to rate up quality of evidence should only be made when serious limitations in any of the 5 areas reducing the quality of evidence are absent. (GRADE Handbook)
88 What can raise quality? 1. Large magnitude of an effect 2. Dose response gradient 3. Effect of plausible residual confounding
89 Large magnitude of an effect Large, consistent, precise effect Although observational studies may overestimate the effect, bias is unlikely to explain or contribute all for a reported very large benefit (or harm) What is large? RR of 2 (large), 5 (very large) For example, odds ratio of babies sleeping on stomachs of 4.1 (95% CI of 3.1 to 5.5) for SIDS compared to sleeping on their back Parachutes to prevent death when jumping from airplanes May upgrade 1 level for large and 2 for very large
90 Dose-response gradient Dose response gradient Clear dose response indicative of a cause effect relationship Warfarin and bleeding (clear dose response) Delay in antibiotics for those presenting with sepsis (i.e. each hour delayed increases mortality)
91 Effect of plausible residual confounding Rigorous observational studies adjust/address confounding in their analysis for identified confounders Cannot control for unmeasured or unknown confounders (hence why observational studies are downgraded), and other plausible confounders may not be addressed This residual confounding may result in an underestimation of the true effect All plausible residual confounding may be working to reduce the demonstrated effect or increase the effect if no effect was observed Sicker patients doing better Not for profit vs for profit
92 Session 11: Summary of findings tables and evidence profiles
93 Summary of Findings tables Endpoint of the GRADE process for SRs Key milestone for Guideline developers on their way to make a recommendation SoF Tables profiles include outcomes, number of studies, assumed risk, corresponding risk, relative effect, overall rating, classification of outcome importance, footnotes
94 Summary of Findings tables Standard table format one for each comparison (may require more than one) Report all outcomes, even if no data Improve understanding Improve accessibility Created with GRADEpro GDT

95 Summary of findings table
96
97 GRADEPro GDT

98 What to do when you can t pool? Can report results from a single study Can report a range from multiple studies if can t pool
99 Considerations when ranking evidence While factors influencing the quality of evidence are additive such that the reduction or increase in each individual factor is added together with the other factors to reduce or increase the quality of evidence for an outcome grading the quality of evidence involves judgements which are not exclusive. Therefore, GRADE is not a quantitative system for grading the quality of evidence. Each factor for downgrading or upgrading reflects not discrete categories but a continuum within each category and among the categories. When the body of evidence is intermediate with respect to a particular factor, the decision about whether a study falls above or below the threshold for up or downgrading the quality (by one or more factors) depends on judgment. For example, if there was some uncertainty about the three factors: study limitations, inconsistency, and imprecision, but not serious enough to downgrade each of them, one could reasonably make the case for downgrading, or for not doing so. A reviewer might in each category give the studies the benefit of the doubt and would interpret the evidence as high quality. Another reviewer, deciding to rate down the evidence by one level, would judge the evidence as moderate quality. Reviewers should grade the quality of the evidence by considering both the individual factors in the context of other judgments they made about the quality of evidence for the same outcome. In such a case, you should pick one or two categories of limitations which you would offer as reasons for downgrading and explain your choice in the footnote. You should also provide a footnote next to the other factor, you decided not to downgrade, explaining that there was some uncertainty, but you already downgraded for the other factor and further lowering the quality of evidence for this outcome would seem inappropriate. GRADE strongly encourages review and guideline authors to be explicit and transparent when they find themselves in these situations by acknowledging borderline decisions. Despite the limitations of breaking continua into categories, treating each criterion for rating quality up or down as discrete categories enhances transparency. Indeed, the great merit of GRADE is not that it ensures reproducible judgments but that it requires explicit judgment that is made transparent to users.
100 Implications for HDR students Effectiveness reviews: you must include a SoF table underneath your executive summary You should discuss and interpret your results and certainty in those results in your discussion and this should impact the conclusions you make
101 Is this the end...or next steps? The endpoint for systematic reviews and for HTA restricted to evidence reports is a summary of the evidence the quality rating for each outcome and the estimate of effect. For guideline developers and HTA that provide advice to policymakers, a summary of the evidence represents a key milestone on the path to a recommendation. Guideline developers (but not systematic reviewers) then review all the information to make a final decision about which outcomes are critical and which are important and come to a final decision regarding the rating of overall quality of evidence, before considering making recommendations.
102 Session 12: Conclusion
103 Other resources/ Information Diagnostic test accuracy SoF tables Qualitative evidence synthesis GRADE Approach CerQual GRADE Handbook ( ) GIN McMaster Guidelines checklist ( MAGIC App Refer to workbook for additional resources University of Adelaide 103
104 GRADE project groups 1. Environmental and Occupational Health 19. Complex interventions 2. Prognosis 20. GRADE Dispute 3. Outcomes valuation 21. NRS Risk of bias 4. Technology 22. Certainty in evidence 5. GRADE CERQual 23. Philosophy of GRADE 6. Diagnosis 24. Modelling 7. Network Meta analysis 25. Genetic Epidemiology 9. Training and Credentialing 26. Performance measurement/quality improvement (QI) 10. Public Health 27. Standardised wording of results and interpretation 21. Rare diseases 28. Overview of rerviews 12. Communication 29. Implementation of guidelines 13. Evidence to Decisions 30. Time to event outcomes 14. Equity 31. Stakeholders involvment 15. Algorithms and pathways 32. Rapid guidelines 17. Biosimilars 18. GRADE for animal studies
105 Final questions?
106 Get involved! Sign up to the GRADE working group mailing list
107 Segue short presentation

108 Are levels of evidence..dead?
109 Disclosure Chair of JBI Levels of Evidence and Grades of Recommendation Working Party This presentation can be considered Level IV evidence, based on personal reflections and low quality philosophical musings...probably below Level IV, as it is dubious whether the speaker is actually an expert providing expert opinion Highly subjective and perhaps provocative opinions to keep you awake in the second day of research school pre lunch sleepiness



110 JBI Levels of Evidence and Grades of Recommendation Working Group
111
112
113 Eventually, the traditional hierarchies of evidence started to fall apart due to attempts to fit too many elements as well as a lack of standardization. Now, we have to move on to a new phase of trying to unify the principles Guyatt, Gordon, Victor Montori, Holger Schünemann, and Paul Glasziou. "When Can We Be Confident about Estimates of Treatment Effects?." The Medical Roundtable General Medicine Edition (2015).
114 Modified picture from Goldet et al 2013 (cropped)
115 What we know Much more than study design should be taken into account when judging the quality of the evidence Study design plays a role in pre ranking

116 So are they dead?

117 Still alive and breathing! Useful for: 1. Pre ranking in the GRADE approach 2. Educational purposes 3. Structuring searches 4. Rapid evidence synthesis/appraisal products

118 Educational purposes Introduction to study designs and epidemiology Provides a structure that can be referred to whilst learning the basics

119 Structuring searches Systematic review searching Manage and sort results Clear study inclusion/exclusion criteria
120 Rapid evidence products Various methodologies Applying levels of evidence as a quick screen and rapid assessment/indicator for quality Evidence summaries
121
122 JBI Levels Effectiveness Diagnostic test accuracy Prognosis Economic evaluations Meaningfulness approach.html#tabbed nav=levels of Evidence
Copyright GRADE ING THE QUALITY OF EVIDENCE AND STRENGTH OF RECOMMENDATIONS NANCY SANTESSO, RD, PHD
 GRADE ING THE QUALITY OF EVIDENCE AND STRENGTH OF RECOMMENDATIONS NANCY SANTESSO, RD, PHD ASSISTANT PROFESSOR DEPARTMENT OF CLINICAL EPIDEMIOLOGY AND BIOSTATISTICS, MCMASTER UNIVERSITY Nancy Santesso,
GRADE ING THE QUALITY OF EVIDENCE AND STRENGTH OF RECOMMENDATIONS NANCY SANTESSO, RD, PHD ASSISTANT PROFESSOR DEPARTMENT OF CLINICAL EPIDEMIOLOGY AND BIOSTATISTICS, MCMASTER UNIVERSITY Nancy Santesso,
GRADE. Grading of Recommendations Assessment, Development and Evaluation. British Association of Dermatologists April 2014
 GRADE Grading of Recommendations Assessment, Development and Evaluation British Association of Dermatologists April 2014 Previous grading system Level of evidence Strength of recommendation Level of evidence
GRADE Grading of Recommendations Assessment, Development and Evaluation British Association of Dermatologists April 2014 Previous grading system Level of evidence Strength of recommendation Level of evidence
GRADE, Summary of Findings and ConQual Workshop
 GRADE, Summary of Findings and ConQual Workshop To discuss Introduction New JBI Levels of Evidence and Grades of Recommendation Moving towards GRADE Summary of Findings tables Qualitative Levels Conclusion
GRADE, Summary of Findings and ConQual Workshop To discuss Introduction New JBI Levels of Evidence and Grades of Recommendation Moving towards GRADE Summary of Findings tables Qualitative Levels Conclusion
Determinants of quality: Factors that lower or increase the quality of evidence
 Determinants of quality: Factors that lower or increase the quality of evidence GRADE Workshop CBO, NHG and Dutch Cochrane Centre CBO, April 17th, 2013 Outline The GRADE approach: step by step Factors
Determinants of quality: Factors that lower or increase the quality of evidence GRADE Workshop CBO, NHG and Dutch Cochrane Centre CBO, April 17th, 2013 Outline The GRADE approach: step by step Factors
GRADE. Grading of Recommendations Assessment, Development and Evaluation. British Association of Dermatologists April 2018
 GRADE Grading of Recommendations Assessment, Development and Evaluation British Association of Dermatologists April 2018 Previous grading system Level of evidence Strength of recommendation Level of evidence
GRADE Grading of Recommendations Assessment, Development and Evaluation British Association of Dermatologists April 2018 Previous grading system Level of evidence Strength of recommendation Level of evidence
Cochrane-GRADE Workshop
 Cochrane-GRADE Workshop Modena, June 2017 Holger Schünemann, Elena Parmelli, Sara Balduzzi Jane Noyes, Heather Munthe-Kaas, Claire Glenton Background / history of GRADE and GRADE CERQual Deep vein thrombosis
Cochrane-GRADE Workshop Modena, June 2017 Holger Schünemann, Elena Parmelli, Sara Balduzzi Jane Noyes, Heather Munthe-Kaas, Claire Glenton Background / history of GRADE and GRADE CERQual Deep vein thrombosis
Cochrane Pregnancy and Childbirth Group Methodological Guidelines
 Cochrane Pregnancy and Childbirth Group Methodological Guidelines [Prepared by Simon Gates: July 2009, updated July 2012] These guidelines are intended to aid quality and consistency across the reviews
Cochrane Pregnancy and Childbirth Group Methodological Guidelines [Prepared by Simon Gates: July 2009, updated July 2012] These guidelines are intended to aid quality and consistency across the reviews
Controlled Trials. Spyros Kitsiou, PhD
 Assessing Risk of Bias in Randomized Controlled Trials Spyros Kitsiou, PhD Assistant Professor Department of Biomedical and Health Information Sciences College of Applied Health Sciences University of
Assessing Risk of Bias in Randomized Controlled Trials Spyros Kitsiou, PhD Assistant Professor Department of Biomedical and Health Information Sciences College of Applied Health Sciences University of
Washington, DC, November 9, 2009 Institute of Medicine
 Holger Schünemann, MD, PhD Chair, Department of Clinical Epidemiology & Biostatistics Michael Gent Chair in Healthcare Research McMaster University, Hamilton, Canada Washington, DC, November 9, 2009 Institute
Holger Schünemann, MD, PhD Chair, Department of Clinical Epidemiology & Biostatistics Michael Gent Chair in Healthcare Research McMaster University, Hamilton, Canada Washington, DC, November 9, 2009 Institute
Results. NeuRA Hypnosis June 2016
 Introduction may be experienced as an altered state of consciousness or as a state of relaxation. There is no agreed framework for administering hypnosis, but the procedure often involves induction (such
Introduction may be experienced as an altered state of consciousness or as a state of relaxation. There is no agreed framework for administering hypnosis, but the procedure often involves induction (such
The Joanna Briggs Institute Reviewers Manual 2014
 The Joanna Briggs Institute Reviewers Manual 2014 Summary of Findings Tables for Joanna Briggs Institute Systematic Reviews www.joannabriggs.org Joanna Briggs Institute Reviewers Manual: 2014 edition/supplement
The Joanna Briggs Institute Reviewers Manual 2014 Summary of Findings Tables for Joanna Briggs Institute Systematic Reviews www.joannabriggs.org Joanna Briggs Institute Reviewers Manual: 2014 edition/supplement
SOF: Summary of Findings tables. Negrar, 7 aprile 2018
 SOF: Summary of Findings tables Negrar, 7 aprile 2018 Grade up Grade down 2 3 Randomization raises initial quality RCTs: high Observational: low P I C O Outcome Outcome Outcome Outcome Evidence synthesis
SOF: Summary of Findings tables Negrar, 7 aprile 2018 Grade up Grade down 2 3 Randomization raises initial quality RCTs: high Observational: low P I C O Outcome Outcome Outcome Outcome Evidence synthesis
Systematic Reviews and Meta- Analysis in Kidney Transplantation
 Systematic Reviews and Meta- Analysis in Kidney Transplantation Greg Knoll MD MSc Associate Professor of Medicine Medical Director, Kidney Transplantation University of Ottawa and The Ottawa Hospital KRESCENT
Systematic Reviews and Meta- Analysis in Kidney Transplantation Greg Knoll MD MSc Associate Professor of Medicine Medical Director, Kidney Transplantation University of Ottawa and The Ottawa Hospital KRESCENT
Problem solving therapy
 Introduction People with severe mental illnesses such as schizophrenia may show impairments in problem-solving ability. Remediation interventions such as problem solving skills training can help people
Introduction People with severe mental illnesses such as schizophrenia may show impairments in problem-solving ability. Remediation interventions such as problem solving skills training can help people
Recent developments for combining evidence within evidence streams: bias-adjusted meta-analysis
 EFSA/EBTC Colloquium, 25 October 2017 Recent developments for combining evidence within evidence streams: bias-adjusted meta-analysis Julian Higgins University of Bristol 1 Introduction to concepts Standard
EFSA/EBTC Colloquium, 25 October 2017 Recent developments for combining evidence within evidence streams: bias-adjusted meta-analysis Julian Higgins University of Bristol 1 Introduction to concepts Standard
Introduzione al metodo GRADE
 Introduzione al metodo GRADE Atto Billio MD, MSc EBHC Ematologia e TMO-Bolzano Gruppo linee guida SIE Critique of EBM De-emphasizes patient values Doesn t account for individual variation Devalues clinical
Introduzione al metodo GRADE Atto Billio MD, MSc EBHC Ematologia e TMO-Bolzano Gruppo linee guida SIE Critique of EBM De-emphasizes patient values Doesn t account for individual variation Devalues clinical
Essential Skills for Evidence-based Practice Understanding and Using Systematic Reviews
 J Nurs Sci Vol.28 No.4 Oct - Dec 2010 Essential Skills for Evidence-based Practice Understanding and Using Systematic Reviews Jeanne Grace Corresponding author: J Grace E-mail: Jeanne_Grace@urmc.rochester.edu
J Nurs Sci Vol.28 No.4 Oct - Dec 2010 Essential Skills for Evidence-based Practice Understanding and Using Systematic Reviews Jeanne Grace Corresponding author: J Grace E-mail: Jeanne_Grace@urmc.rochester.edu
NeuRA Sleep disturbance April 2016
 Introduction People with schizophrenia may show disturbances in the amount, or the quality of sleep they generally receive. Typically sleep follows a characteristic pattern of four stages, where stage
Introduction People with schizophrenia may show disturbances in the amount, or the quality of sleep they generally receive. Typically sleep follows a characteristic pattern of four stages, where stage
Traumatic brain injury
 Introduction It is well established that traumatic brain injury increases the risk for a wide range of neuropsychiatric disturbances, however there is little consensus on whether it is a risk factor for
Introduction It is well established that traumatic brain injury increases the risk for a wide range of neuropsychiatric disturbances, however there is little consensus on whether it is a risk factor for
Alcohol interventions in secondary and further education
 National Institute for Health and Care Excellence Guideline version (Draft for Consultation) Alcohol interventions in secondary and further education NICE guideline: methods NICE guideline Methods
National Institute for Health and Care Excellence Guideline version (Draft for Consultation) Alcohol interventions in secondary and further education NICE guideline: methods NICE guideline Methods
Distraction techniques
 Introduction are a form of coping skills enhancement, taught during cognitive behavioural therapy. These techniques are used to distract and draw attention away from the auditory symptoms of schizophrenia,
Introduction are a form of coping skills enhancement, taught during cognitive behavioural therapy. These techniques are used to distract and draw attention away from the auditory symptoms of schizophrenia,
Clinical research in AKI Timing of initiation of dialysis in AKI
 Clinical research in AKI Timing of initiation of dialysis in AKI Josée Bouchard, MD Krescent Workshop December 10 th, 2011 1 Acute kidney injury in ICU 15 25% of critically ill patients experience AKI
Clinical research in AKI Timing of initiation of dialysis in AKI Josée Bouchard, MD Krescent Workshop December 10 th, 2011 1 Acute kidney injury in ICU 15 25% of critically ill patients experience AKI
Evidence-Based Medicine and Publication Bias Desmond Thompson Merck & Co.
 Evidence-Based Medicine and Publication Bias Desmond Thompson Merck & Co. Meta-Analysis Defined A meta-analysis is: the statistical combination of two or more separate studies In other words: overview,
Evidence-Based Medicine and Publication Bias Desmond Thompson Merck & Co. Meta-Analysis Defined A meta-analysis is: the statistical combination of two or more separate studies In other words: overview,
Results. NeuRA Treatments for internalised stigma December 2017
 Introduction Internalised stigma occurs within an individual, such that a person s attitude may reinforce a negative self-perception of mental disorders, resulting in reduced sense of selfworth, anticipation
Introduction Internalised stigma occurs within an individual, such that a person s attitude may reinforce a negative self-perception of mental disorders, resulting in reduced sense of selfworth, anticipation
Types of Data. Systematic Reviews: Data Synthesis Professor Jodie Dodd 4/12/2014. Acknowledgements: Emily Bain Australasian Cochrane Centre
 Early Nutrition Workshop, December 2014 Systematic Reviews: Data Synthesis Professor Jodie Dodd 1 Types of Data Acknowledgements: Emily Bain Australasian Cochrane Centre 2 1 What are dichotomous outcomes?
Early Nutrition Workshop, December 2014 Systematic Reviews: Data Synthesis Professor Jodie Dodd 1 Types of Data Acknowledgements: Emily Bain Australasian Cochrane Centre 2 1 What are dichotomous outcomes?
Animal-assisted therapy
 Introduction Animal-assisted interventions use trained animals to help improve physical, mental and social functions in people with schizophrenia. It is a goal-directed intervention in which an animal
Introduction Animal-assisted interventions use trained animals to help improve physical, mental and social functions in people with schizophrenia. It is a goal-directed intervention in which an animal
Outcomes and GRADE Summary of Findings Tables: old and new
 Holger Schünemann, MD, PhD Chair, Dept. of Clinical Epidemiology & Biostatistics Professor of Clinical Epidemiology & Biostatistics and of Medicine Michael Gent Chair in Healthcare Research McMaster University,
Holger Schünemann, MD, PhD Chair, Dept. of Clinical Epidemiology & Biostatistics Professor of Clinical Epidemiology & Biostatistics and of Medicine Michael Gent Chair in Healthcare Research McMaster University,
Results. NeuRA Mindfulness and acceptance therapies August 2018
 Introduction involve intentional and non-judgmental focus of one's attention on emotions, thoughts and sensations that are occurring in the present moment. The aim is to open awareness to present experiences,
Introduction involve intentional and non-judgmental focus of one's attention on emotions, thoughts and sensations that are occurring in the present moment. The aim is to open awareness to present experiences,
Results. NeuRA Worldwide incidence April 2016
 Introduction The incidence of schizophrenia refers to how many new cases there are per population in a specified time period. It is different from prevalence, which refers to how many existing cases there
Introduction The incidence of schizophrenia refers to how many new cases there are per population in a specified time period. It is different from prevalence, which refers to how many existing cases there
Meta Analysis. David R Urbach MD MSc Outcomes Research Course December 4, 2014
 Meta Analysis David R Urbach MD MSc Outcomes Research Course December 4, 2014 Overview Definitions Identifying studies Appraising studies Quantitative synthesis Presentation of results Examining heterogeneity
Meta Analysis David R Urbach MD MSc Outcomes Research Course December 4, 2014 Overview Definitions Identifying studies Appraising studies Quantitative synthesis Presentation of results Examining heterogeneity
Critical appraisal: Systematic Review & Meta-analysis
 Critical appraisal: Systematic Review & Meta-analysis Atiporn Ingsathit MD.PhD. Section for Clinical Epidemiology and biostatistics Faculty of Medicine Ramathibodi Hospital Mahidol University What is a
Critical appraisal: Systematic Review & Meta-analysis Atiporn Ingsathit MD.PhD. Section for Clinical Epidemiology and biostatistics Faculty of Medicine Ramathibodi Hospital Mahidol University What is a
Method. NeuRA Biofeedback May 2016
 Introduction is a technique in which information about the person s body is fed back to the person so that they may be trained to alter the body s conditions. Physical therapists use biofeedback to help
Introduction is a technique in which information about the person s body is fed back to the person so that they may be trained to alter the body s conditions. Physical therapists use biofeedback to help
Does the evidence directly answer my question?
 Does the evidence directly answer my question? " " " "! Domain!(original!question! asked)! Population:!All!patients! with!advanced!cancer! Intervention:!Heparins!! Comparator:!No! anticoagulation! Direct!comparison!
Does the evidence directly answer my question? " " " "! Domain!(original!question! asked)! Population:!All!patients! with!advanced!cancer! Intervention:!Heparins!! Comparator:!No! anticoagulation! Direct!comparison!
Results. NeuRA Forensic settings April 2016
 Introduction Prevalence quantifies the proportion of individuals in a population who have a disease during a specific time period. Many studies have reported a high prevalence of various health problems,
Introduction Prevalence quantifies the proportion of individuals in a population who have a disease during a specific time period. Many studies have reported a high prevalence of various health problems,
Meta-Analysis. Zifei Liu. Biological and Agricultural Engineering
 Meta-Analysis Zifei Liu What is a meta-analysis; why perform a metaanalysis? How a meta-analysis work some basic concepts and principles Steps of Meta-analysis Cautions on meta-analysis 2 What is Meta-analysis
Meta-Analysis Zifei Liu What is a meta-analysis; why perform a metaanalysis? How a meta-analysis work some basic concepts and principles Steps of Meta-analysis Cautions on meta-analysis 2 What is Meta-analysis
ACR OA Guideline Development Process Knee and Hip
 ACR OA Guideline Development Process Knee and Hip 1. Literature searching frame work Literature searches were developed based on the scenarios. A comprehensive search strategy was used to guide the process
ACR OA Guideline Development Process Knee and Hip 1. Literature searching frame work Literature searches were developed based on the scenarios. A comprehensive search strategy was used to guide the process
Authors face many challenges when summarising results in reviews.
 Describing results Authors face many challenges when summarising results in reviews. This document aims to help authors to develop clear, consistent messages about the effects of interventions in reviews,
Describing results Authors face many challenges when summarising results in reviews. This document aims to help authors to develop clear, consistent messages about the effects of interventions in reviews,
Fixed Effect Combining
 Meta-Analysis Workshop (part 2) Michael LaValley December 12 th 2014 Villanova University Fixed Effect Combining Each study i provides an effect size estimate d i of the population value For the inverse
Meta-Analysis Workshop (part 2) Michael LaValley December 12 th 2014 Villanova University Fixed Effect Combining Each study i provides an effect size estimate d i of the population value For the inverse
Live WebEx meeting agenda
 10:00am 10:30am Using OpenMeta[Analyst] to extract quantitative data from published literature Live WebEx meeting agenda August 25, 10:00am-12:00pm ET 10:30am 11:20am Lecture (this will be recorded) 11:20am
10:00am 10:30am Using OpenMeta[Analyst] to extract quantitative data from published literature Live WebEx meeting agenda August 25, 10:00am-12:00pm ET 10:30am 11:20am Lecture (this will be recorded) 11:20am
Component of CPG development ILAE Recommendation Document Identifying topic and developing clinical. S3 research question
 S1: Summary of recommendations for developing Clinical Practice Guidelines Minimum CPG development requirements (where resources are more limited) are bolded. When full resources are available, every recommendation
S1: Summary of recommendations for developing Clinical Practice Guidelines Minimum CPG development requirements (where resources are more limited) are bolded. When full resources are available, every recommendation
Results. NeuRA Motor dysfunction April 2016
 Introduction Subtle deviations in various developmental trajectories during childhood and adolescence may foreshadow the later development of schizophrenia. Studies exploring these deviations (antecedents)
Introduction Subtle deviations in various developmental trajectories during childhood and adolescence may foreshadow the later development of schizophrenia. Studies exploring these deviations (antecedents)
Post-traumatic stress disorder
 National Institute for Health and Care Excellence Final Post-traumatic stress disorder Methods NICE guideline NG116 Supplement 1 December 2018 Final These evidence reviews were developed by the National
National Institute for Health and Care Excellence Final Post-traumatic stress disorder Methods NICE guideline NG116 Supplement 1 December 2018 Final These evidence reviews were developed by the National
CHAMP: CHecklist for the Appraisal of Moderators and Predictors
 CHAMP - Page 1 of 13 CHAMP: CHecklist for the Appraisal of Moderators and Predictors About the checklist In this document, a CHecklist for the Appraisal of Moderators and Predictors (CHAMP) is presented.
CHAMP - Page 1 of 13 CHAMP: CHecklist for the Appraisal of Moderators and Predictors About the checklist In this document, a CHecklist for the Appraisal of Moderators and Predictors (CHAMP) is presented.
Incorporating Clinical Information into the Label
 ECC Population Health Group LLC expertise-driven consulting in global maternal-child health & pharmacoepidemiology Incorporating Clinical Information into the Label Labels without Categories: A Workshop
ECC Population Health Group LLC expertise-driven consulting in global maternal-child health & pharmacoepidemiology Incorporating Clinical Information into the Label Labels without Categories: A Workshop
Checklist for Randomized Controlled Trials. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews
 The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Randomized Controlled Trials http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Randomized Controlled Trials http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
Results. NeuRA Treatments for dual diagnosis August 2016
 Introduction Many treatments have been targeted to improving symptom severity for people suffering schizophrenia in combination with substance use problems. Studies of dual diagnosis often investigate
Introduction Many treatments have been targeted to improving symptom severity for people suffering schizophrenia in combination with substance use problems. Studies of dual diagnosis often investigate
CEU screening programme: Overview of common errors & good practice in Cochrane intervention reviews
 CEU screening programme: Overview of common errors & good practice in Cochrane intervention reviews Since September 2013, the CEU has been responsible for pre-publication screening of new intervention
CEU screening programme: Overview of common errors & good practice in Cochrane intervention reviews Since September 2013, the CEU has been responsible for pre-publication screening of new intervention
Evaluating the results of a Systematic Review/Meta- Analysis
 Open Access Publication Evaluating the results of a Systematic Review/Meta- Analysis by Michael Turlik, DPM 1 The Foot and Ankle Online Journal 2 (7): 5 This is the second of two articles discussing the
Open Access Publication Evaluating the results of a Systematic Review/Meta- Analysis by Michael Turlik, DPM 1 The Foot and Ankle Online Journal 2 (7): 5 This is the second of two articles discussing the
Results. NeuRA Family relationships May 2017
 Introduction Familial expressed emotion involving hostility, emotional over-involvement, and critical comments has been associated with increased psychotic relapse in people with schizophrenia, so these
Introduction Familial expressed emotion involving hostility, emotional over-involvement, and critical comments has been associated with increased psychotic relapse in people with schizophrenia, so these
In many healthcare situations, it is common to find
 Interpreting and Using Meta-Analysis in Clinical Practice Cheryl Holly Jason T. Slyer Systematic reviews, which can include a meta-analysis, are considered the gold standard for determination of best practice.
Interpreting and Using Meta-Analysis in Clinical Practice Cheryl Holly Jason T. Slyer Systematic reviews, which can include a meta-analysis, are considered the gold standard for determination of best practice.
Checklist for Randomized Controlled Trials. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews
 The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Randomized Controlled Trials http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Randomized Controlled Trials http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.3, 02 December 2013
 Methodological Expectations of Cochrane Intervention Reviews (MECIR) Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.3, 02 December 2013 Jackie Chandler, Rachel
Methodological Expectations of Cochrane Intervention Reviews (MECIR) Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.3, 02 December 2013 Jackie Chandler, Rachel
ISPOR Task Force Report: ITC & NMA Study Questionnaire
 INDIRECT TREATMENT COMPARISON / NETWORK META-ANALYSIS STUDY QUESTIONNAIRE TO ASSESS RELEVANCE AND CREDIBILITY TO INFORM HEALTHCARE DECISION-MAKING: AN ISPOR-AMCP-NPC GOOD PRACTICE TASK FORCE REPORT DRAFT
INDIRECT TREATMENT COMPARISON / NETWORK META-ANALYSIS STUDY QUESTIONNAIRE TO ASSESS RELEVANCE AND CREDIBILITY TO INFORM HEALTHCARE DECISION-MAKING: AN ISPOR-AMCP-NPC GOOD PRACTICE TASK FORCE REPORT DRAFT
School of Dentistry. What is a systematic review?
 School of Dentistry What is a systematic review? Screen Shot 2012-12-12 at 09.38.42 Where do I find the best evidence? The Literature Information overload 2 million articles published a year 20,000 biomedical
School of Dentistry What is a systematic review? Screen Shot 2012-12-12 at 09.38.42 Where do I find the best evidence? The Literature Information overload 2 million articles published a year 20,000 biomedical
GRADE Evidence Profiles on Long- and Rapid-Acting Insulin Analogues for the treatment of Diabetes Mellitus [DRAFT] October 2007
![GRADE Evidence Profiles on Long- and Rapid-Acting Insulin Analogues for the treatment of Diabetes Mellitus [DRAFT] October 2007](/thumbs/84/90988922.jpg "GRADE Evidence Profiles on Long- and Rapid-Acting Insulin Analogues for the treatment of Diabetes Mellitus [DRAFT] October 2007") GRADE Evidence Profiles on Long- and Rapid-Acting Insulin Analogues for the treatment of Diabetes Mellitus October 2007 Canadian Agency for Drugs and Technologies in Health Disclaimer This report is prepared
GRADE Evidence Profiles on Long- and Rapid-Acting Insulin Analogues for the treatment of Diabetes Mellitus October 2007 Canadian Agency for Drugs and Technologies in Health Disclaimer This report is prepared
Objectives. Information proliferation. Guidelines: Evidence or Expert opinion or???? 21/01/2017. Evidence-based clinical decisions
 Guidelines: Evidence or Expert opinion or???? Objectives Need for guidelines? Prakesh Shah Professor, Department of Pediatrics, Mount Sinai Hospital Institute of Health Policy Management and Evaluation
Guidelines: Evidence or Expert opinion or???? Objectives Need for guidelines? Prakesh Shah Professor, Department of Pediatrics, Mount Sinai Hospital Institute of Health Policy Management and Evaluation
Checklist for Diagnostic Test Accuracy Studies. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews
 The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Diagnostic Test Accuracy Studies http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Diagnostic Test Accuracy Studies http://joannabriggs.org/research/critical-appraisal-tools.html www.joannabriggs.org
Systematic reviews: From evidence to recommendation. Marcel Dijkers, PhD, FACRM Icahn School of Medicine at Mount Sinai
 Systematic reviews: From evidence to recommendation Session 2 - June 18, 2014 Going beyond design, going beyond intervention: The American Academy of Neurology (AAN) Clinical Practice Guideline process
Systematic reviews: From evidence to recommendation Session 2 - June 18, 2014 Going beyond design, going beyond intervention: The American Academy of Neurology (AAN) Clinical Practice Guideline process
NeuRA Obsessive-compulsive disorders October 2017
 Introduction (OCDs) involve persistent and intrusive thoughts (obsessions) and repetitive actions (compulsions). The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) defines
Introduction (OCDs) involve persistent and intrusive thoughts (obsessions) and repetitive actions (compulsions). The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) defines
Transcranial Direct-Current Stimulation
 Introduction (tdcs) is a non-invasive form of brain stimulation similar to transcranial magnetic stimulation, but instead of using magnets, it uses a lowintensity, constant current applied through scalp
Introduction (tdcs) is a non-invasive form of brain stimulation similar to transcranial magnetic stimulation, but instead of using magnets, it uses a lowintensity, constant current applied through scalp
Mapping the Informed Health Choices (IHC) Key Concepts (KC) to core concepts for the main steps of Evidence-Based Health Care (EBHC).
 Key Concepts (KC) to core concepts for the main steps of Evidence-Based Health Care (EBHC).") KC No KC Short Title KC Statement EBHC concept EBHC sub concept EBHC statement EBHC Step Reported 1.01 Treatments can harm Treatments may be harmful Explain the use of harm/aetiologies for (rare) adverse
KC No KC Short Title KC Statement EBHC concept EBHC sub concept EBHC statement EBHC Step Reported 1.01 Treatments can harm Treatments may be harmful Explain the use of harm/aetiologies for (rare) adverse
Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.1, 8 December 2011
 Methodological Expectations of Cochrane Intervention Reviews (MECIR) Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.1, 8 December 2011 Jackie Chandler, Rachel Churchill,
Methodological Expectations of Cochrane Intervention Reviews (MECIR) Methodological standards for the conduct of new Cochrane Intervention Reviews Version 2.1, 8 December 2011 Jackie Chandler, Rachel Churchill,
Implementing scientific evidence into clinical practice guidelines
 Evidence Based Dentistry Implementing scientific evidence into clinical practice guidelines Asbjørn Jokstad University of Oslo, Norway 15/07/2004 1 PRACTICE GUIDELINES IN DENTISTRY (Medline) 2100 1945
Evidence Based Dentistry Implementing scientific evidence into clinical practice guidelines Asbjørn Jokstad University of Oslo, Norway 15/07/2004 1 PRACTICE GUIDELINES IN DENTISTRY (Medline) 2100 1945
NeuRA Decision making April 2016
 Introduction requires an individual to use their knowledge and experience of a context in order to choose a course of action 1. A person s ability to autonomously make decisions is referred to as their
Introduction requires an individual to use their knowledge and experience of a context in order to choose a course of action 1. A person s ability to autonomously make decisions is referred to as their
Clinical Epidemiology for the uninitiated
 Clinical epidemiologist have one foot in clinical care and the other in clinical practice research. As clinical epidemiologists we apply a wide array of scientific principles, strategies and tactics to
Clinical epidemiologist have one foot in clinical care and the other in clinical practice research. As clinical epidemiologists we apply a wide array of scientific principles, strategies and tactics to
Meta-analyses: analyses:
 Meta-analyses: analyses: how do they help, and when can they not? Lee Hooper Senior Lecturer in research synthesis & nutrition l.hooper@uea.ac.uk 01603 591268 Aims Systematic Reviews Discuss the scientific
Meta-analyses: analyses: how do they help, and when can they not? Lee Hooper Senior Lecturer in research synthesis & nutrition l.hooper@uea.ac.uk 01603 591268 Aims Systematic Reviews Discuss the scientific
Standard Methods for Quality Assessment of Evidence
 Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503 947 1119 Standard Methods for Quality Assessment of Evidence
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503 947 1119 Standard Methods for Quality Assessment of Evidence
Introduction to meta-analysis
 Introduction to meta-analysis Steps of a Cochrane review 1. define the question 2. plan eligibility criteria 3. plan methods 4. search for studies 5. apply eligibility criteria 6. collect data 7. assess
Introduction to meta-analysis Steps of a Cochrane review 1. define the question 2. plan eligibility criteria 3. plan methods 4. search for studies 5. apply eligibility criteria 6. collect data 7. assess
Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods
 Jakobsen et al. BMC Medical Research Methodology 2014, 14:120 CORRESPONDENCE Open Access Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods Janus Christian
Jakobsen et al. BMC Medical Research Methodology 2014, 14:120 CORRESPONDENCE Open Access Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods Janus Christian
Evaluating the Quality of Evidence from a Network Meta- Analysis
 Evaluating the Quality of Evidence from a Network Meta- Analysis Georgia Salanti 1, Cinzia Del Giovane 2, Anna Chaimani 1, Deborah M. Caldwell 3, Julian P. T. Higgins 3,4 * 1 Department of Hygiene and
Evaluating the Quality of Evidence from a Network Meta- Analysis Georgia Salanti 1, Cinzia Del Giovane 2, Anna Chaimani 1, Deborah M. Caldwell 3, Julian P. T. Higgins 3,4 * 1 Department of Hygiene and
Results. NeuRA Herbal medicines August 2016
 Introduction have been suggested as a potential alternative treatment which may positively contribute to the treatment of schizophrenia. Herbal therapies can include traditional Chinese medicines and Indian
Introduction have been suggested as a potential alternative treatment which may positively contribute to the treatment of schizophrenia. Herbal therapies can include traditional Chinese medicines and Indian
Quality of Clinical Practice Guidelines
 Evidence Based Dentistry Quality of Clinical Practice Guidelines Asbjørn Jokstad University of Oslo, Norway 07/04/2005 1 Justification for developing guidelines Demand for effectiveness and efficacy studies
Evidence Based Dentistry Quality of Clinical Practice Guidelines Asbjørn Jokstad University of Oslo, Norway 07/04/2005 1 Justification for developing guidelines Demand for effectiveness and efficacy studies
Assessing risk of bias
 Assessing risk of bias Norwegian Research School for Global Health Atle Fretheim Research Director, Norwegian Institute of Public Health Professor II, Uiniversity of Oslo Goal for the day We all have an
Assessing risk of bias Norwegian Research School for Global Health Atle Fretheim Research Director, Norwegian Institute of Public Health Professor II, Uiniversity of Oslo Goal for the day We all have an
Confounding and Bias
 28 th International Conference on Pharmacoepidemiology and Therapeutic Risk Management Barcelona, Spain August 22, 2012 Confounding and Bias Tobias Gerhard, PhD Assistant Professor, Ernest Mario School
28 th International Conference on Pharmacoepidemiology and Therapeutic Risk Management Barcelona, Spain August 22, 2012 Confounding and Bias Tobias Gerhard, PhD Assistant Professor, Ernest Mario School
MINI SYMPOSIUM - EUMASS - UEMASS European Union of Medicine in Assurance and Social Security
 MINI SYMPOSIUM - EUMASS - UEMASS European Union of Medicine in Assurance and Social Security Quality of Evidence and Grades of Recommendations in guidelines A role for insurance medicine? Prof. Regina
MINI SYMPOSIUM - EUMASS - UEMASS European Union of Medicine in Assurance and Social Security Quality of Evidence and Grades of Recommendations in guidelines A role for insurance medicine? Prof. Regina
Robert M. Jacobson, M.D. Department of Pediatric and Adolescent Medicine Mayo Clinic, Rochester, Minnesota
 How to Conduct a Systematic Review: A Workshop 24 th Annual Primary Care Research Methods & Statistics Conference, San Antonio, Texas Saturday, December 3, 2011 Robert M. Jacobson, M.D. Department of Pediatric
How to Conduct a Systematic Review: A Workshop 24 th Annual Primary Care Research Methods & Statistics Conference, San Antonio, Texas Saturday, December 3, 2011 Robert M. Jacobson, M.D. Department of Pediatric
Introduction to systematic reviews/metaanalysis
 Introduction to systematic reviews/metaanalysis Hania Szajewska The Medical University of Warsaw Department of Paediatrics hania@ipgate.pl Do I needknowledgeon systematicreviews? Bastian H, Glasziou P,
Introduction to systematic reviews/metaanalysis Hania Szajewska The Medical University of Warsaw Department of Paediatrics hania@ipgate.pl Do I needknowledgeon systematicreviews? Bastian H, Glasziou P,
NeuRA Schizophrenia diagnosis May 2017
 Introduction Diagnostic scales are widely used within clinical practice and research settings to ensure consistency of illness ratings. These scales have been extensively validated and provide a set of
Introduction Diagnostic scales are widely used within clinical practice and research settings to ensure consistency of illness ratings. These scales have been extensively validated and provide a set of
Changes to NIH grant applications:
 Changes to NIH grant applications: Changes to application guide instructions for preparing the Research Strategy. Three new required sections have to be incorporated into the 12 page limit of the Research
Changes to NIH grant applications: Changes to application guide instructions for preparing the Research Strategy. Three new required sections have to be incorporated into the 12 page limit of the Research
CRITICAL APPRAISAL OF CLINICAL PRACTICE GUIDELINE (CPG)
") CRITICAL APPRAISAL OF CLINICAL PRACTICE GUIDELINE (CPG) Atiporn Ingsathit MD, PhD. 1 Rationale for Clinical Practice Guidelines Worldwide concerns about: Unexplained variations in clinical practice Rising
CRITICAL APPRAISAL OF CLINICAL PRACTICE GUIDELINE (CPG) Atiporn Ingsathit MD, PhD. 1 Rationale for Clinical Practice Guidelines Worldwide concerns about: Unexplained variations in clinical practice Rising
Standards for the reporting of new Cochrane Intervention Reviews
 Methodological Expectations of Cochrane Intervention Reviews (MECIR) Standards for the reporting of new Cochrane Intervention Reviews 24 September 2012 Preface The standards below summarize proposed attributes
Methodological Expectations of Cochrane Intervention Reviews (MECIR) Standards for the reporting of new Cochrane Intervention Reviews 24 September 2012 Preface The standards below summarize proposed attributes
Why is ILCOR moving to GRADE?
 1 Why is ILCOR moving to GRADE? Associate Professor Peter Morley Director Medical Education Royal Melbourne Hospital University of Melbourne 10 min 2 3 4 5 6 7 Apart from international consensus Allows
1 Why is ILCOR moving to GRADE? Associate Professor Peter Morley Director Medical Education Royal Melbourne Hospital University of Melbourne 10 min 2 3 4 5 6 7 Apart from international consensus Allows
Workshop: Cochrane Rehabilitation 05th May Trusted evidence. Informed decisions. Better health.
 Workshop: Cochrane Rehabilitation 05th May 2018 Trusted evidence. Informed decisions. Better health. Disclosure I have no conflicts of interest with anything in this presentation How to read a systematic
Workshop: Cochrane Rehabilitation 05th May 2018 Trusted evidence. Informed decisions. Better health. Disclosure I have no conflicts of interest with anything in this presentation How to read a systematic
Systematic Reviews in healthcare and the Joanna Briggs Institute /Cochrane Collaboration. Fiona Bath-Hextall
 Systematic Reviews in healthcare and the Joanna Briggs Institute /Cochrane Collaboration Fiona Bath-Hextall Fiona.bath-hextall@nottingham.ac.uk Remit The importance of Systematic Reviews Who uses systematic
Systematic Reviews in healthcare and the Joanna Briggs Institute /Cochrane Collaboration Fiona Bath-Hextall Fiona.bath-hextall@nottingham.ac.uk Remit The importance of Systematic Reviews Who uses systematic
Attention deficit hyperactivity disorder: diagnosis and management (update)
") National Institute for Health and Care Excellence Final Attention deficit hyperactivity disorder: diagnosis and management (update) NICE guideline: methods NICE guideline NG87 March 2018 Final Developed
National Institute for Health and Care Excellence Final Attention deficit hyperactivity disorder: diagnosis and management (update) NICE guideline: methods NICE guideline NG87 March 2018 Final Developed
How to interpret results of metaanalysis
 How to interpret results of metaanalysis Tony Hak, Henk van Rhee, & Robert Suurmond Version 1.0, March 2016 Version 1.3, Updated June 2018 Meta-analysis is a systematic method for synthesizing quantitative
How to interpret results of metaanalysis Tony Hak, Henk van Rhee, & Robert Suurmond Version 1.0, March 2016 Version 1.3, Updated June 2018 Meta-analysis is a systematic method for synthesizing quantitative
GLOSSARY OF GENERAL TERMS
 GLOSSARY OF GENERAL TERMS Absolute risk reduction Absolute risk reduction (ARR) is the difference between the event rate in the control group (CER) and the event rate in the treated group (EER). ARR =
GLOSSARY OF GENERAL TERMS Absolute risk reduction Absolute risk reduction (ARR) is the difference between the event rate in the control group (CER) and the event rate in the treated group (EER). ARR =
Evidence-based Laboratory Medicine: Finding and Assessing the Evidence
 Find Assess Decide Evidence-based Laboratory Medicine: Finding and Assessing the Evidence Pieter Vermeersch, M.D. Ph.D. Laboratory Medicine, UZ Leuven November 18th 2008 Introduction Archie Cochrane (1908-1988)
Find Assess Decide Evidence-based Laboratory Medicine: Finding and Assessing the Evidence Pieter Vermeersch, M.D. Ph.D. Laboratory Medicine, UZ Leuven November 18th 2008 Introduction Archie Cochrane (1908-1988)
LIHS Mini Master Class
 Alexandru Nicusor Matei 2013 CC BY-NC-ND 2.0 Grading the evidence Liz Mitchell Liz Mitchell University of Leeds 2015. This work is made available for reuse under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike
Alexandru Nicusor Matei 2013 CC BY-NC-ND 2.0 Grading the evidence Liz Mitchell Liz Mitchell University of Leeds 2015. This work is made available for reuse under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike
Tiago Villanueva MD Associate Editor, The BMJ. 9 January Dear Dr. Villanueva,
 Tiago Villanueva MD Associate Editor, The BMJ 9 January 2018 Dear Dr. Villanueva, Thank you for your thoughtful re-review of our Manuscript (BMJ.2017.041528) entitled "Immune-related Toxicities in PD-1
Tiago Villanueva MD Associate Editor, The BMJ 9 January 2018 Dear Dr. Villanueva, Thank you for your thoughtful re-review of our Manuscript (BMJ.2017.041528) entitled "Immune-related Toxicities in PD-1
Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist.
: Checklist.") Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist. MOOSE Checklist Infliximab reduces hospitalizations and surgery interventions in patients with inflammatory bowel disease:
Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist. MOOSE Checklist Infliximab reduces hospitalizations and surgery interventions in patients with inflammatory bowel disease:
Mapping from SORT to GRADE. Brian S. Alper, MD, MSPH, FAAFP Editor-in-Chief, DynaMed October 31, 2013
 Mapping from SORT to GRADE Brian S. Alper, MD, MSPH, FAAFP Editor-in-Chief, DynaMed October 31, 2013 Disclosures Brian S. Alper MD, MSPH, FAAFP is editor-in-chief for DynaMed (published by EBSCO) and medical
Mapping from SORT to GRADE Brian S. Alper, MD, MSPH, FAAFP Editor-in-Chief, DynaMed October 31, 2013 Disclosures Brian S. Alper MD, MSPH, FAAFP is editor-in-chief for DynaMed (published by EBSCO) and medical
Evidence Based Medicine
 Course Goals Goals 1. Understand basic concepts of evidence based medicine (EBM) and how EBM facilitates optimal patient care. 2. Develop a basic understanding of how clinical research studies are designed
Course Goals Goals 1. Understand basic concepts of evidence based medicine (EBM) and how EBM facilitates optimal patient care. 2. Develop a basic understanding of how clinical research studies are designed
Cochrane Breast Cancer Group
 Cochrane Breast Cancer Group Version and date: V3.2, September 2013 Intervention Cochrane Protocol checklist for authors This checklist is designed to help you (the authors) complete your Cochrane Protocol.
Cochrane Breast Cancer Group Version and date: V3.2, September 2013 Intervention Cochrane Protocol checklist for authors This checklist is designed to help you (the authors) complete your Cochrane Protocol.
Reporting the effects of an intervention in EPOC reviews. Version: 21 June 2018 Cochrane Effective Practice and Organisation of Care Group
 Reporting the effects of an intervention in EPOC reviews Version: 21 June 2018 Cochrane Effective Practice and Organisation of Care Group Feedback on how to improve this resource is welcome and should
Reporting the effects of an intervention in EPOC reviews Version: 21 June 2018 Cochrane Effective Practice and Organisation of Care Group Feedback on how to improve this resource is welcome and should
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Principles of meta-analysis
 Principles of meta-analysis 1 The popularity of meta-analyses Search on 22 October 2015 10000 9000 8156 8875 8000 7000 6554 6000 5000 4852 4000 3000 2000 1000 0 1 1 1 272 334 371 323 386 429 482 596 639
Principles of meta-analysis 1 The popularity of meta-analyses Search on 22 October 2015 10000 9000 8156 8875 8000 7000 6554 6000 5000 4852 4000 3000 2000 1000 0 1 1 1 272 334 371 323 386 429 482 596 639
PHO MetaQAT Guide. Critical appraisal in public health. PHO Meta-tool for quality appraisal
 PHO MetaQAT Guide Critical appraisal in public health Critical appraisal is a necessary part of evidence-based practice and decision-making, allowing us to understand the strengths and weaknesses of evidence,
PHO MetaQAT Guide Critical appraisal in public health Critical appraisal is a necessary part of evidence-based practice and decision-making, allowing us to understand the strengths and weaknesses of evidence,
Establishing confidence in qualitative evidence. The ConQual Approach
 Establishing confidence in qualitative evidence The ConQual Approach Objectives To review the JBI conceptualisation of what constitutes evidence for decision making To provide an overview of the JBI approach
Establishing confidence in qualitative evidence The ConQual Approach Objectives To review the JBI conceptualisation of what constitutes evidence for decision making To provide an overview of the JBI approach
Glossary of Practical Epidemiology Concepts
 Glossary of Practical Epidemiology Concepts - 2009 Adapted from the McMaster EBCP Workshop 2003, McMaster University, Hamilton, Ont. Note that open access to the much of the materials used in the Epi-546
Glossary of Practical Epidemiology Concepts - 2009 Adapted from the McMaster EBCP Workshop 2003, McMaster University, Hamilton, Ont. Note that open access to the much of the materials used in the Epi-546