Radiology Update: Balancing Diagnostic Needs with Cost Effectiveness
|
|
|
- Muriel Palmer
- 5 years ago
- Views:
Transcription
1 Radiology Update: Balancing Diagnostic Needs with Cost Effectiveness October 2018 Ramin Khorasani, MD, MPH Professor of Radiology, Harvard Medical School Director, Center for Evidence-Based Imaging Vice Chair, Department of Radiology Brigham and Women s Hospital
2 Disclosure Nothing to disclose
3 Objective I. Discuss factors that may contribute to the inappropriate use of radiological studies II. Discuss the imaging workup of some commonly encountered clinical problems III. Key points and next best steps to reduce inappropriate use of imaging studies
4 Background Excessive number of tests with? Impact on patients outcome concern of radiation risk; Increasing concern of costs Patient experience Steady growth of imaging costs Pre-authorization programs by payers CMS program on Imaging CDS Proper selection of imaging tests Clinical problem, test characteristics, local expertise Increasing complexity of imaging technology Use of contrast-e.g. gadolinium induced NSF Impossible to present all guidelines
5 I. Main causes of inappropriate use of imaging studies Test results are unlikely to affect patient management short interval follow-up studies Repeating studies which have already been performed (including elsewhere) Patient demand Not requesting the best test Access to technology Inadequate clinical information provided on the requisition
6 II. Imaging Guidelines American College of Radiology (ACR) Appropriateness criteria ; 1995, 1999, 2002, updates through 2008, 2010, 2013, 2014, 2015 The British royal College of Radiologists (BRCR): Making the best use of a department of clinical radiology: guidelines for doctors ; 1995
7 II. Imaging Guidelines 80-90% of recommendations based on consensus opinion Take a long time to develop These are not algorithms: do not account of local expertise do not account for patient to patient variations Role of a Radiology Consultation Service?
8 Radiology Consultation Service- Peer to peer consultation Designed like other consultation services in medicine Allows for on-the-ward, or outpatient clinic consultation Comprehensive imaging consultation Many advantages and disadvantages Expect expansion of concept with value-based contracts
9 Imaging Modalities Ultrasound: adv: ionizing radiation, relatively cheap and accessible. Exam of choice in OB, excellent in the female pelvis disadv: operator dependent, interference from bone, air, fat, difficult in the very obese
10 Imaging Modalities Computed Tomography (CT): adv: no interference from bone, air or fat, easy in the obese, non-operator dependent, rapid exam, easily accessible at most sites disadv: more expensive than US, ionizing radiation, intravenous contrasts with associated costs and risks
11 Imaging Modalities Magnetic Resonance Imaging (MRI): adv. No ionizing radiation, exquisite soft tissue contrast (similar spatial resolution to CT), multiplanar imaging disadv: more expensive than CT, less accessible than US/CT, rapidly changing technology, length of exam longer than CT, patient contraindications
12 Clinical Problem: Imaging Strategy Neuroradiology: acute and chronic headache, low back pain Thoracic Radiology: pulmonary embolism Abdominal Radiology: bowel obstruction, appendicitis, renal colic, hematuria, common incidental lesions Musculoskeletal radiology hip fracture
13 Case 1 40 year old female with acute onset of severe headache and loss of consciousness Best study to do first: If the first study is normal, the next test:

14 Best study to do first: CT


15 Next imaging study: cerebral arteriogram

16

17 Clinical Decision Support for iterative Data Collectione.g. Head CT Minor Head Trauma

18 Clinical Decision Support Output for Imaging Study Requests Deviating from Evidence
19 Head and Neck Clinical Problem: headache Acute, severe: CT excellent for intracranial hemorrhage, Chronic imaging not routinely indicated in the absence of focal signs or symptoms, unless evidence of raised intracranial pressure, posterior fossa signs MRI is superior to CT in the posterior fossa, sellar and juxta-sellar regions
20 Case 6 24 year old male with 6 wk history of low back pain not improving despite conservative treatment, right S-I radiculopathy Best study to do first: If first study is normal, the next test:

21

22


23 Best study to do first: MRI
24 Spine- Clinical Problem: low back pain 4-6 weeks of conservative treatment if no red flag E.g. Malignancy, infection, bladder/bowel symptoms Remember that normal patients can have abnormal MRIs Need to continue to develop better decision rules and guidelines- ACP October 2007, ACR Embed as decision support in order entry systems

25

26

27

28
29 National Ambulatory Medical Care Survey Reference: Ip IK, Schneider LI, Gershanik EF, Raja AS, Mar W, Seltzer S, Khorasani R. Promoting primary care physician guideline adherence for MRI use among patients with low back pain: Impact of clinical decision support and accountability tools. Am. J. Med
30 Ip IK, Schneider LI, Gershanik EF, Raja AS, Mar W, Seltzer S, Khorasani R. Promoting primary care physician guideline adherence for MRI use among patients with low back pain: Impact of clinical decision support and accountability tools. AM. J. Med

31 epublished February 2015
32 epublished February 2015
33 Protecting Access To Medicare Act (PAMA; 2014) Section 218b: Promoting Evidence Based Care Through the use of Imaging CDS The imaging CDS requirement is not in MACRA

34
35 Protecting Access to Medicare Act (HR 4302; 2014)- Section 218b Promoting Evidence-Based Care New Requirement: Ordering professionals for ambulatory and ED applicable advanced imaging services must be exposed to specified Appropriate Use Criteria (AUC) via a certified CDS mechanism Consequence for failure imaging provider (pro to tech) will not be paid Implementation date January 1, 2020 *AUC: evidence-based criteria linking a clinical condition to an imaging service with an assessment of appropriateness
36 PAMA rules: Key provisions Specified AUC will be developed and published by qualified provider-led entities (qple) qple must have rigorous processes to assess, grade the evidence and publish evidence-based criteria on web-site Excludes RBMs Enables accommodation for local best practices First application cycle January 1, 2016, then annually Implication: Providers can meet PAMA by implementing a certified CDS mechanism with an AUC set from any qple CDS mechanism applications March 2017; certifications expected summer 2017
37 Key provisions under PAMA 218(b) Priority clinical areas Coronary artery disease (suspected or diagnosed) Suspected pulmonary embolism Headache (traumatic and non-traumatic) Hip pain Low back pain. Shoulder pain (to include suspected rotator cuff injury) Cancer of the lung (primary or metastatic, suspected or diagnosed) Cervical or neck pain Outlier ordering professionals after 2020 to be potentially exposed to pre-authorization

38 Harvard Medical School elibrary of Evidence
39 Case 9 32 Y.O. Female with Braca1 gene mutation. Need to screen for breast cancer. Best study to do first: If the first study is normal, the next test:
 No")


40 42 y/o BRCA 1 ER/PR Her2/Neu Negative High Grade Invasive Ductal Carcinoma (IDC) No Ductal Carcinoma In situ (DCIS) MR post contrast shows round rim enhancing mass Axial delayed MR shows washout delayed kinetics Ultrasound shows an oval mass with irregular margins


41 56 y/o, Strong Family History; BRCA Negative ER/PR Her2/neu Negative High Grade IDC High grade DCIS Contrast enhanced MRI shows an oval mass with irregular margins and rim enhancement. Around the mass is non-masslike enhancement worrisome Ramin for Khorasani, DCIS MD, MPH, 2016
42 Breast MRI and breast cancer Established yearly screening tool adjunct to mammography in high risk population- e.g. Braca1 gene mutation It is being used [with large variation in practice] in staging of newly diagnosed breast cancer primarily to look for multi-centric disease Need to develop evidence on use of MRI in this context to improve patient outcomes Other screening use not supported by current evidence dense breast legislation adjunct screening with ultrasound or MRI
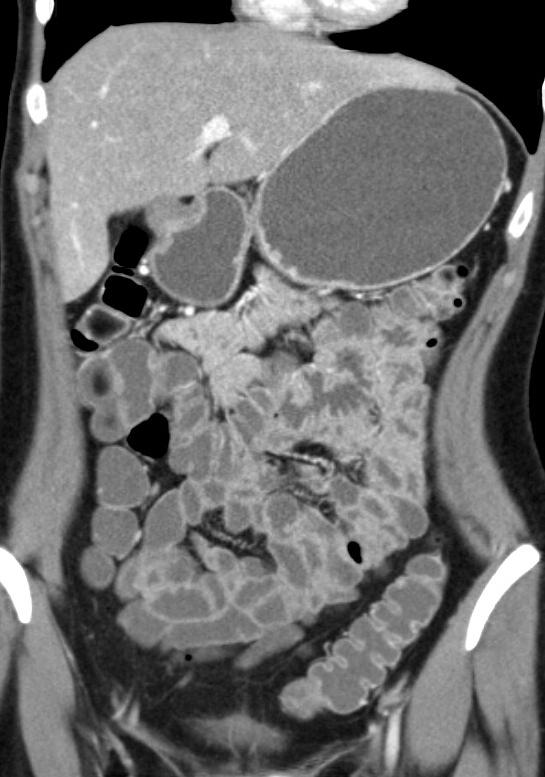
43 Case F with acute onset lower abdominal pain, N/V, no fever, normal WBC, no prior surgical history, you are worried about an acute small bowel obstruction Best study to do first: If the first study is normal, the next test:

44

45

46

47 CT
48 Abdomen utility of KUB Excellent for suspected perforation (supine abdomen, erect CXR), If suspected bowel obstruction with history of prior obstruction (supine and upright) In most other instances not very helpful as negative or positive result usually leads to another imaging test such as CT or US
49 Abdomen-Clinical Problem:? Small bowel obstruction KUB good first test if: prior surgery, obstruction; may be normal rarely in acute obstruction Acute SBO: if further imaging, CT far better than small bowel follow through (barium study) to diagnose obstruction and its etiology Unexplained chronic or recurrent SBO: CT/MRI enterography CT to look for other etiologies for pain

50




51 mucosal hyperenhancement: segmental attenuation greater than adjacent jejunum or ileum (+/- wall thickening [> 3mm])


52


53


54
55 Case F, with 2 day history of RLQ pain, anorexia, fever, no prior surgical history, peritoneal signs in the RLQ, WBC = 12k, negative BHCG Best study to do first If first study is normal, the next test:
56 Case M diabetic with 2 day history of RLQ pain, fever, WBC = 6k, elevated blood sugars, could be acute appendicitis Best study to do first: If first study is normal, the next test:

57

58
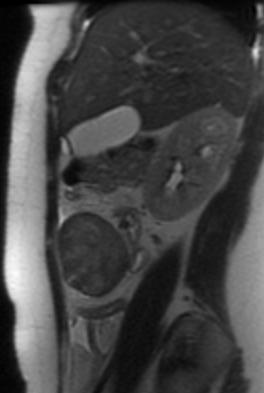
59 Case 12 variant RLQ pain x2days, 16 wks pregnant Best study to do first: If first study is normal, the next test:

60
61 Abdomen-Clinical Problem: appendicitis Clinical diagnosis, imaging not routinely indicated If equivocal clinical diagnosis: CT is test of choice in this scenario with sensitivity and specificity > 95% In pregnancy, ultrasound in expert hands, MRI best test NEJM 1/98: CT on all patients with RLQ pain-not standard of care CT decreased negative appendectomy rate to <2% BWH NAR 30% in females, 12% in males in 1990 NAR 1.5% females, 1.8% males in 2007 >95% of appendectomies had preoperative CT 14.6% of CT for appendicitis went to OR Estimate 20 CT per 1 less appendectomy-need further studies
62 How about harm from radiation exposure? Substantial concern for harm from radiation exposure from Medical Imaging, esp CT- Real but overblown in the media 1-2% potential (many assumptions) incrementally increased risk of malignancy over baseline of approximately 40% lifetime cancer risk in US
63 How about harm from CT radiation exposure? If CT is clinically appropriate and superior to other imaging modalities, its benefits substantially exceed the potential harm We do need better science to more accurately assess risk
64 Case F with an incidental 2.5 cm right adrenal mass found on CT, performed to elevate an incidental liver lesion on RUQ US looking for gallstones! Best study to do first: If the first study is normal, the next test:

65


66 In-Phase Out of Phase



67 Lipid-poor Delayed Washout A B C A: Unenhanced CT HU= 29 B: Enhanced HU= 73 C: 15 min. HU= 44 Absolute enhancement washout= (73-44/73-29)x100= 66%
68 Abdomen-Clinical Problem: adrenal lesion Adrenal imaging predominantly anatomic, diagnosis of functional adrenal tumors requires biochemistry In patients with an incidental adrenal lesion or those with a primary malignancy, a noncontrast CT, limited adrenal MR, washout CT, or occasionally PET CT may obviate the need for follow up or biopsy
69 Case M, medical malpractice lawyer, found to have an incidental 6 cm simple right renal cyst on abdominal ultrasound Best study to do first: If first study is normal, the next test:
70 Case F, who has a 2 cm echogenic mass in the liver found incidentally on ultrasound, no prior medical history Best study to do first: If first study is normal, the next test:


71 CT with Contrast T2 Weighted MRI




72 Dynamic MRI sequence with Gadolinium: FNH
73 Incidental Liver lesions Great majority are benign cysts, hemangiomas- diagnosis can be made on ultrasound, CT, MRI If no prior malignancy, indeterminate solitary <15 mm hepatic lesion is highly likely to be benign (>98%), options: Do nothing Re-image in 6-12 months-show stability-then stop Make benign diagnosis with MRI then stop
74 Incidental Liver lesions Modality of choice for characterization is MRI
75 Case M physician, s/p fall with right hip pain, unable to move right hip Best study to do first: If the first study is normal, the next test:

76 Best study to do first: Plain films

77 Next imaging study?: MRI

78
79 Musculoskeletal Clinical Problem:? Hip fracture Plain films are the first choice Normal plain films, high clinical suspicion: MRI is the study of choice to exclude occult fracture
80 Case y.o F with presentation suggestive of appendicitis. There is a 30% chance in your estimation that she has appendicitis. We have a test with 95% sensitivity, 95% specificity. The test is positive. What is the chance that she has appendicitis? <30% 30-75% 75-90% >90%
81 Case y.o F with presentation unlikely of appendicitis. There is a 2% chance in your estimation that she has appendicitis. We have a test with 95% sensitivity, 95% specificity. The test is positive. What is the chance that she has appendicitis? <30% 30-75% 75-90% >90%
82 Prevalence 30% Appy Normal P appendix Positive test Negative test Total
83 Prevalence 2% Appy Normal P appendix Positive test Negative test Total
84 III. Key Points & Next Best Steps Think of how the result of an imaging test may change the management of your patient BEFORE you request an examination best test applied to the wrong patient may provide misleading results Give as much clinical information as reasonable on the requisition history more helpful than rule out s!! blank requisition may result in a radiologist missing a subtle but important finding
85 III. Key Points & Next Best Steps Use your radiologist as a consultant, this is her/his Job!! Get familiar with the new Law pertaining to Imaging CDS-begins January 2020
Clinical Decision Support Technologies for Oncologic Imaging
 Clinical Decision Support Technologies for Oncologic Imaging Ramin Khorasani, MD, MPH Professor of Radiology Harvard Medical School Distinguished Chair, Medical Informatics Vice Chair, Department of Radiology
Clinical Decision Support Technologies for Oncologic Imaging Ramin Khorasani, MD, MPH Professor of Radiology Harvard Medical School Distinguished Chair, Medical Informatics Vice Chair, Department of Radiology
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS
 JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
11/1/2014. Radiologic incidentalomas Ordering pitfalls Newer technology and applications
 Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
n Make tremendous difference in patients lives: n Diagnosing or excluding disease and injury n Evaluating response to therapy
 Imaging: Choosing the Appropriate Exam Rob Milman, MD Austin Radiological Association What is a Radiologist? A physician who specializes in diagnosing and treating disease and injury by using medical imaging
Imaging: Choosing the Appropriate Exam Rob Milman, MD Austin Radiological Association What is a Radiologist? A physician who specializes in diagnosing and treating disease and injury by using medical imaging
Imaging Appropriateness: What s out there
 Imaging Appropriateness: What s out there Anish Kirpalani, MD FRCPC Staff Radiologist & Co-Director of MRI Department of Medical Imaging St. Michael's Hospital and University of Toronto Outline Why are
Imaging Appropriateness: What s out there Anish Kirpalani, MD FRCPC Staff Radiologist & Co-Director of MRI Department of Medical Imaging St. Michael's Hospital and University of Toronto Outline Why are
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
Implementing Clinical Decision Support. C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science
 Implementing Clinical Decision Support C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science Objectives What is imaging clinical decision support? Does it work? How should it be
Implementing Clinical Decision Support C Craig Blackmore, MD, MPH, FASER Center for Health Care Improvement Science Objectives What is imaging clinical decision support? Does it work? How should it be
Breast Cancer Screening
 Scan for mobile link. Breast Cancer Screening What is breast cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease
Scan for mobile link. Breast Cancer Screening What is breast cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease
PREAMBLE GENERAL DIAGNOSTIC RADIOLOGY
 PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
Appropriate Imaging Tests Lead to Meaningful Results. Dr. Richard Wasley May 2011
 Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
Appropriate Imaging Tests Lead to Meaningful Results Dr. Richard Wasley May 2011 Summarize the advantages and limitations of specific imaging tests and why clinical information is so important to radiologists
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Contributors. Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images:
 Contributors Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images: Peter Miller, MD, Indiana University School of Medicine Chapter 1: Figure
Contributors Thanks to Peter Miller, MD; LCDR Kevin Preston, MD; and Keith Newbrough, MD for their generous contribution of images: Peter Miller, MD, Indiana University School of Medicine Chapter 1: Figure
Effective Utilization of Imaging. John V. Roberts, M.D. Premier Radiology Abdominal Imaging
 Effective Utilization of Imaging John V. Roberts, M.D. Premier Radiology Abdominal Imaging Safety Contrast and Radiation What to order Abdomen/Pelvis Brain/Spine Chest Musculoskeletal Ob/Gyn Head and Neck
Effective Utilization of Imaging John V. Roberts, M.D. Premier Radiology Abdominal Imaging Safety Contrast and Radiation What to order Abdomen/Pelvis Brain/Spine Chest Musculoskeletal Ob/Gyn Head and Neck
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
FOR CMS (MEDICARE) MEMBERS ONLY NATIONAL COVERAGE DETERMINATION (NCD) FOR MAGNETIC RESONANCE IMAGING:
 MEMBERS ONLY NATIONAL COVERAGE DETERMINATION (NCD) FOR MAGNETIC RESONANCE IMAGING:") National Imaging Associates, Inc. Clinical guidelines BONE MARROW MRI Original Date: July 2008 Page 1 of 5 CPT Codes: 77084 Last Review Date: September 2014 NCD 220.2 MRI Last Effective Date: July 2011
National Imaging Associates, Inc. Clinical guidelines BONE MARROW MRI Original Date: July 2008 Page 1 of 5 CPT Codes: 77084 Last Review Date: September 2014 NCD 220.2 MRI Last Effective Date: July 2011
Basic Abdominal and Pelvic Imaging Concepts. David L. Smith, MD Assistant Professor of Radiology
 Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
Basic Abdominal and Pelvic Imaging Concepts David L. Smith, MD Assistant Professor of Radiology Basic Imaging Concepts Contrast Resolution vs Spacial Resolution Spacial Resolution......refers to the ability
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Radiological Tests: Which One is Most Appropriate for My Patient?
 Radiological Tests: Which One is Most Appropriate for My Patient? Robert Hartman, M.D. 2016 MFMER slide-1 Disclosures No Disclosures 2016 MFMER slide-2 Objectives Discuss tools to aid in the ordering of
Radiological Tests: Which One is Most Appropriate for My Patient? Robert Hartman, M.D. 2016 MFMER slide-1 Disclosures No Disclosures 2016 MFMER slide-2 Objectives Discuss tools to aid in the ordering of
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Radiology. Undergraduate Radiology Sample Questions
 Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Radiology Undergraduate Radiology Sample Questions April 2012 The following examples are offered of questions that might be used to assess undergraduate radiology. There are 3 different styles: An OSCE
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Radiology. Undergraduate Radiology Curriculum
 Radiology Undergraduate Radiology Curriculum April 2012 INTRODUCTION This curriculum is intended to form a framework for undergraduate learning and teaching in radiology. It refers to the relevant competencies
Radiology Undergraduate Radiology Curriculum April 2012 INTRODUCTION This curriculum is intended to form a framework for undergraduate learning and teaching in radiology. It refers to the relevant competencies
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
BREAST MRI. VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece
 BREAST MRI VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece Breast ΜR Imaging (MRM) Breast MR imaging is an extremely powerful diagnostic tool, that when used in
BREAST MRI VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece Breast ΜR Imaging (MRM) Breast MR imaging is an extremely powerful diagnostic tool, that when used in
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Breast Cancer Imaging
 Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Breast Cancer Imaging I. Policy University Health Alliance (UHA) will cover breast imaging when such services meet the medical criteria guidelines (subject to limitations and exclusions) indicated below.
Alice Fung, MD Oregon Health and Science University
 Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
Alice Fung, MD Oregon Health and Science University Disclosure Comments The speaker Alice Fung, MD Has relevant financial relationships to disclose. Received honorarium from (Guerbet). This individual
BI-RADS and Breast MRI. Kathy Borovicka, M.D. Thursday February 15, 2018
 BI-RADS and Breast MRI Kathy Borovicka, M.D. Thursday February 15, 2018 Learning Objectives Be familiar with the Breast Imaging Reporting and Data System (BI-RADS) Understand the components of a breast
BI-RADS and Breast MRI Kathy Borovicka, M.D. Thursday February 15, 2018 Learning Objectives Be familiar with the Breast Imaging Reporting and Data System (BI-RADS) Understand the components of a breast
Armed Forces Institute of Pathology.
 Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Armed Forces Institute of Pathology www.radpath.com Armed Forces Institute of Pathology Breast Disease www.radpath.org Armed Forces Institute of Pathology Interpretation of Breast MRI Leonard M. Glassman
Breast Imaging! Ravi Adhikary, MD!
 Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
Contrast-enhanced Breast MRI RSSA 2013
 Contrast-enhanced Breast MRI RSSA 2013 Prof. dr. Maurice van den Bosch University Medical Center Utrecht, the Netherlands Index 1) Breast cancer 2) Why MRI of the breast 3) Technique 4) Interpretation
Contrast-enhanced Breast MRI RSSA 2013 Prof. dr. Maurice van den Bosch University Medical Center Utrecht, the Netherlands Index 1) Breast cancer 2) Why MRI of the breast 3) Technique 4) Interpretation
Radiology. General radiology department. X-ray
 The radiology directorate provides a diagnostic, interventional and therapeutic service for its local population, and a tertiary service for the region. It also provides support to some national work such
The radiology directorate provides a diagnostic, interventional and therapeutic service for its local population, and a tertiary service for the region. It also provides support to some national work such
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Screening Mammograms: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
Appendicitis USG vs CT
 Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
September 6, Dear Centers for Medicare & Medicaid Services,
 September 6, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1631-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: Revisions
September 6, 2016 Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1631-P Mail Stop C4-26-05 7500 Security Boulevard Baltimore, MD 21244-1850 Re: Revisions
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008
 Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
ADI Procedure Codes. August 2016 Revised April 2017 Page 1 of 7 ADI Procedure Codes
 Code Description 70450 CT Head without contrast 70460 CT Head with contrast 70470 CT Head with & without contrast 70480 CT Orbit, et al without contrast 70481 CT Orbit, et al with contrast 70482 CT Orbit,
Code Description 70450 CT Head without contrast 70460 CT Head with contrast 70470 CT Head with & without contrast 70480 CT Orbit, et al without contrast 70481 CT Orbit, et al with contrast 70482 CT Orbit,
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
FOR CMS (MEDICARE) MEMBERS ONLY NATIONAL COVERAGE DETERMINATION (NCD) FOR MAGNETIC RESONANCE IMAGING:
 MEMBERS ONLY NATIONAL COVERAGE DETERMINATION (NCD) FOR MAGNETIC RESONANCE IMAGING:") National Imaging Associates, Inc. Clinical guidelines SINUS MRI Original Date: November 2007 Page 1 of 5 CPT Codes: 70540, 70542, 70543 Last Review Date: July 2014 NCD 220.2 MRI Last Effective Date: July
National Imaging Associates, Inc. Clinical guidelines SINUS MRI Original Date: November 2007 Page 1 of 5 CPT Codes: 70540, 70542, 70543 Last Review Date: July 2014 NCD 220.2 MRI Last Effective Date: July
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
X-ray (Radiography) - Bone
 - Bone") Scan for mobile link. X-ray (Radiography) - Bone Bone x-ray uses a very small dose of ionizing radiation to produce pictures of any bone in the body. It is commonly used to diagnose fractured bones or
Scan for mobile link. X-ray (Radiography) - Bone Bone x-ray uses a very small dose of ionizing radiation to produce pictures of any bone in the body. It is commonly used to diagnose fractured bones or
HEALTHCARE AI DEVELOPMENT CYCLE
 Dr. Keith Dreyer Chief Science Officer, ACR Data Science Institute ACR Board of Chancellors, Chairman Informatics Commission Chief Data Science Officer, MGH, BWH, Partners Healthcare Associate Professor
Dr. Keith Dreyer Chief Science Officer, ACR Data Science Institute ACR Board of Chancellors, Chairman Informatics Commission Chief Data Science Officer, MGH, BWH, Partners Healthcare Associate Professor
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
National Diagnostic Imaging Symposium 2013 SAM - Breast MRI 1
 National Diagnostic Imaging Symposium 2013 December 8-12, 2013 Disney s Yacht Club Resort Lake Buena Vista, Florida Self Assessment Module Questions, Answers and References Day SAM Title - Each SAM title
National Diagnostic Imaging Symposium 2013 December 8-12, 2013 Disney s Yacht Club Resort Lake Buena Vista, Florida Self Assessment Module Questions, Answers and References Day SAM Title - Each SAM title
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
R-SCAN: Engaging Clinicians in Value-based Care
 R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
R-SCAN: Engaging Clinicians in Value-based Care Nancy Fredericks, MBA R-SCAN Director rscan.org What is R-SCAN? A collaborative between referring clinicians and radiologists to improve patient care R-SCAN
Guideline Summary NGC-7922
 NGC banner Guideline Summary NGC-7922 Guideline Title ACR Appropriateness Criteria right lower quadrant pain suspected appendicitis. Bibliographic Source(s) Rosen MP, Ding A, Blake MA, Baker ME, Cash BD,
NGC banner Guideline Summary NGC-7922 Guideline Title ACR Appropriateness Criteria right lower quadrant pain suspected appendicitis. Bibliographic Source(s) Rosen MP, Ding A, Blake MA, Baker ME, Cash BD,
Advances in Emergency Imaging
 Hampton Symposium,, October 16 th, 2010 Advances in Emergency Imaging Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General Hospital
Hampton Symposium,, October 16 th, 2010 Advances in Emergency Imaging Robert A. Novelline, MD Professor of Radiology, Harvard Medical School Director of Emergency Radiology, Massachusetts General Hospital
Pitfalls and Limitations of Breast MRI. Susan Orel Roth, MD Professor of Radiology University of Pennsylvania
 Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Pediatric Imaging Spine MRI and Spine CT Test Request Tip Sheet
 Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
Imaging for Pediatric Trauma and the Acute Patient What to Order When
 Imaging for Pediatric Trauma and the Acute Patient What to Order When Paula Shultz, MD Pediatric Radiologist Central Oregon Radiology Associates November 8, 2013 5 yr old male involved in multicar accident,
Imaging for Pediatric Trauma and the Acute Patient What to Order When Paula Shultz, MD Pediatric Radiologist Central Oregon Radiology Associates November 8, 2013 5 yr old male involved in multicar accident,
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Tissue Breast Density
 Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Hepatic Imaging: What Every Practitioner Should Know
 Hepatic Imaging: What Every Practitioner Should Know Shuchi K. Rodgers, MD Section Chief, Abdominal Imaging Director of Ultrasound Department of Radiology Einstein Medical Center rodgerss@einstein.edu
Hepatic Imaging: What Every Practitioner Should Know Shuchi K. Rodgers, MD Section Chief, Abdominal Imaging Director of Ultrasound Department of Radiology Einstein Medical Center rodgerss@einstein.edu
Complete Summary GUIDELINE TITLE. Liver lesion characterization. BIBLIOGRAPHIC SOURCE(S)
") Complete Summary GUIDELINE TITLE Liver lesion characterization. BIBLIOGRAPHIC SOURCE(S) Foley WD, Bree RL, Gay SB, Glick SN, Heiken JP, Huprich JE, Levine MS, Ros PR, Rosen MP, Shuman WP, Greene FL, Rockey
Complete Summary GUIDELINE TITLE Liver lesion characterization. BIBLIOGRAPHIC SOURCE(S) Foley WD, Bree RL, Gay SB, Glick SN, Heiken JP, Huprich JE, Levine MS, Ros PR, Rosen MP, Shuman WP, Greene FL, Rockey
BENEFITS OF CT AND HOW LEADING ACADEMIC INSTITUTIONS ARE COMMUNICATING RISK TO PATIENTS. James A. Brink, MD Massachusetts General Hospital
 BENEFITS OF CT AND HOW LEADING ACADEMIC INSTITUTIONS ARE COMMUNICATING RISK TO PATIENTS James A. Brink, MD Massachusetts General Hospital BENEFITS OF CT Standard Axial Imaging Superb Anatomic Depiction
BENEFITS OF CT AND HOW LEADING ACADEMIC INSTITUTIONS ARE COMMUNICATING RISK TO PATIENTS James A. Brink, MD Massachusetts General Hospital BENEFITS OF CT Standard Axial Imaging Superb Anatomic Depiction
High Tech Imaging Quick Reference Guide
 High Tech Imaging Quick Reference Guide 1 High Tech Imaging Authorizations may now be requested through our secure provider portal, BlueAccess. Getting Started Step 1: Log into BlueAccess from www.bcbst.com
High Tech Imaging Quick Reference Guide 1 High Tech Imaging Authorizations may now be requested through our secure provider portal, BlueAccess. Getting Started Step 1: Log into BlueAccess from www.bcbst.com
RADIOLOGIC TECHNOLOGY (526)
") RADIOLOGIC TECHNOLOGY (526) 526-133 DMS General Procedures 2 Radiologic Technology (526) 1 526-130 Introduction to Diagnostic Medical Sonography This course introduces the student to the history of ultrasound
RADIOLOGIC TECHNOLOGY (526) 526-133 DMS General Procedures 2 Radiologic Technology (526) 1 526-130 Introduction to Diagnostic Medical Sonography This course introduces the student to the history of ultrasound
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/20/2011 Radiology Quiz of the Week # 34 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/20/2011 Radiology Quiz of the Week # 34 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION
 FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION CPT/HCPCS Codes 72192 Computed tomography, pelvis; without contrast material 72193 with contrast material(s) 72194 without
FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION CPT/HCPCS Codes 72192 Computed tomography, pelvis; without contrast material 72193 with contrast material(s) 72194 without
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
BREAST CANCER SCREENING IS A CHOICE
 BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
created by high-voltage devices Examples include medical and dental x-rays, light, microwaves and nuclear energy
 What is radiation? Radiation is energy emitted from a source, that travels through space and can penetrate matter. Listed below are two types that we are exposed to and contribute to our overall radiation
What is radiation? Radiation is energy emitted from a source, that travels through space and can penetrate matter. Listed below are two types that we are exposed to and contribute to our overall radiation
Breast Cancer Screening and Diagnosis
 Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
BI-RADS Update. Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital
 BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January
BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
Imaging Work-Up of a Neck Mass - Adults & Children
 Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
MAKING THE BEST USE OF CLINICAL RADIOLOGY SERVICES. Dr Martina Paetzel Consultant Radiologist
 MAKING THE BEST USE OF CLINICAL RADIOLOGY SERVICES Dr Martina Paetzel Consultant Radiologist LEARNING OBJECTIVES To be aware of guidelines regulating ionising radiation & radiation dose To introduce how
MAKING THE BEST USE OF CLINICAL RADIOLOGY SERVICES Dr Martina Paetzel Consultant Radiologist LEARNING OBJECTIVES To be aware of guidelines regulating ionising radiation & radiation dose To introduce how
BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers
 BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers Arnold Honick, MD Radiology Consultants of Iowa, PLC ahonick@rciowa.com BREAST DENSITY LEGISLATION Nancy
BREAST DENSITY WHAT IS IT? WHY IS IT IMPORTANT? & What IOWA SF250 Means to Patients and Providers Arnold Honick, MD Radiology Consultants of Iowa, PLC ahonick@rciowa.com BREAST DENSITY LEGISLATION Nancy
Here are examples of bilateral analog mammograms from the same patient including CC and MLO projections.
 Good afternoon. It s my pleasure to be discussing Diagnostic Breast Imaging over the next half hour. I m Wei Yang, Professor of Diagnostic Radiology and Chief, the Section of Breast Imaging as well as
Good afternoon. It s my pleasure to be discussing Diagnostic Breast Imaging over the next half hour. I m Wei Yang, Professor of Diagnostic Radiology and Chief, the Section of Breast Imaging as well as
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Introduction to WVU Radiology
 Introduction to WVU Radiology Lana Winkler, MD Assistant Professor Department of Radiology Section of Cardiothoracic Imaging Special thanks to Jeffery P. Hogg, MD Radiology Orientation Objectives Why is
Introduction to WVU Radiology Lana Winkler, MD Assistant Professor Department of Radiology Section of Cardiothoracic Imaging Special thanks to Jeffery P. Hogg, MD Radiology Orientation Objectives Why is
Abdomen Sonography Examination Content Outline
 Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Abdomen Sonography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 Anatomy, Perfusion, and Function Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy
Message of the Month for GPs June 2013
 Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Digital tomosynthesis (DT) has been well described as a
 has been well described as a") Case Report The Usefulness of Digital Tomosynthesis (DT) in Assisting in Cases of Doubtful Routine Radiography and/or Computed Tomography (CT) Image. Abstract Digital tomosynthesis is useful in assisting
Case Report The Usefulness of Digital Tomosynthesis (DT) in Assisting in Cases of Doubtful Routine Radiography and/or Computed Tomography (CT) Image. Abstract Digital tomosynthesis is useful in assisting
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O
 ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
ASSESSING THE PLAIN ABDOMINAL RADIOGRAPH M A A M E F O S U A A M P O F O Introduction The abdomen (less formally called the belly, stomach, is that part of the body between the thorax (chest) and pelvis,
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Coding Companion for Urology/Nephrology. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Urology/Nephrology A comprehensive illustrated guide to coding and reimbursement 2014 Contents Getting Started with Coding Companion...i Integumentary...1 Arteries and Veins...15 Lymph
Coding Companion for Urology/Nephrology A comprehensive illustrated guide to coding and reimbursement 2014 Contents Getting Started with Coding Companion...i Integumentary...1 Arteries and Veins...15 Lymph
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention