The AHEAD Study: Managing anticoagulatedpatients who suffer head injury
|
|
|
- Maximillian Pierce
- 5 years ago
- Views:
Transcription

1 AHEAD Study The AHEAD Study: Managing anticoagulatedpatients who suffer head injury Suzanne Mason 1,2, Maxine Kuczawski 1, Matthew Stevenson 1, Dawn Teare 1, Michael Holmes 1, ShammiRamlakhan 1, Steve Goodacre 1,2, Rosemary Harper, Francis Morris 2 1. School of Health and Related Research, University of Sheffield 2. Sheffield Teaching Hospitals NHS Foundation Trust
2 The problem Head injury is a common problem in emergency departments, worldwide ~1% UK population receives anticoagulation therapy Most commonly prescribed oral anticoagulant, Warfarin Anticoagulated patients who suffer head injury:- Increased risk of suffering serious complications. But how big? Lack of evidence on how patients should be managed Prospective research needed to gain understanding of complications and develop management strategies 2
3 NICE Guidance: old & new NICE Guidance CG56, 2007 CT head scan patients with any of the following risk factors within 1 hour: GCS<13 GCS<15 at 2 hours Open or depressed skull fracture Sign of fracture at base of skull Post-traumatic seizure Focal neurological deficit >1 episode of vomiting Amnesia >30minutes before impact CT head scan patients that have experienced LOCor amnesiaandany of the following risk factors: LoC Within 8 hours Aged 65 years or over Dangerous mechanism of injury Within 1 hour Coagulopathy NICE Guidance CG176, 2014 CT head scan with any of the following risk factors within 1 hour: GCS<13 GCS<15 at 2 hours Open or depressed skull fracture Any sign of basal skull fracture Post-traumatic seizure Focal neurological deficit >1 episode of vomiting CT head scan patients that have experienced LoCor amnesia AND any of the following risk factors: Within 8 hours Aged 65 years or over History of bleeding or clotting disorders Dangerous mechanism of injury >30 minutes retrograde amnesia of events CT head scan patients with no other indications for CT head scan ANDhaving warfarin treatment, within 8 hours
4 Current Evidence Study No. of patients in study % of patients anticoagulated Incidence of ICH in anticoagulated patients Li, % (144) 6.2% Lavoie, % (35) incidence of ICH not measured -mortality only Fabbri, % (66) 24% Reynolds, % (32) 25% Gittleman, % (89) 30.4% if GCS 14, 0% if GCS =15 Menditto, % (97) 27.6% Nishiijima, % (768) 5.1%
5 Study aims Identify and determine incidence of clinically significant outcomes Identify predictors of adverse outcomes Identify cost-effectiveness of different models of care Develop robust clinical guidance to reduce risk of complication and death 5
6 Setting & participants 33 acute hospital trusts with Type 1 Emergency Departments (EDs) throughout the UK Patient inclusion criteria:- Aged 16 years and older Anticoagulated, prescribed Warfarin only Presenting with a head injury (defined as a clinically apparent injury to the head including facial trauma) within the preceding 48 hours of ED attendance. Study sample size 3,000 patients based on 5% estimated complication rate 6
7 Study process Patient attendance at the Emergency Department ELIGIBLE STUDY DATABASES On identification Create record and submit basic demographic and ED attendance data FOLLOW-UP (FUP) QUESTIONNAIRE Approx. 6 WEEKS (42 days) after ED attendance Sent to patient s home address Excluded due to not meeting inclusion criteria NON-RESPONSE REMINDER Approx. 4 WEEKS (28 days) after FUP Sent to patient s home address ON-LINE AHEAD DATABASE Approx. 5 WEEKS (35 days) after FUP Submit anonymised clinical data ScHARR University of Sheffield 7
8 Outcomes Primary outcome Incidence of clinically significant brain injury defined by:- Head injury-related death Neurosurgery resulting from the initial injury Clinically-significant CT head scan Re-attendance to the ED with related significant complication (up to 10 weeks after the original attendance) Secondary outcomes :- Identification of predictors of adverse clinical outcome Costs per patient of the head injury as managed in the participating centres and when applied to a derived ideal model 8
9 Recruitment Total sites (England& Scotland)= 33 Total number of patients = 3,566 Figure excludes withdrawals (154) Clinical records (anonymised) = 3,534 (99%) 9
10 Patients N (3534) % Male Age (Mean(SD)) 78.5 (11.6) INR (mean(sd)) 2.67 (1.34) INR < INR INR> GCS GCS GCS < Cause of injury: Fall
11 Outcomes n (3534) % Admission CT grading (n=2114) Significant intracranial abnormality likely to be due to injury Other abnormality likely to be due to injury (e.g. scalp haematoma, uncomplicated fracture) Other abnormality unlikely to be due to injury Normal CT head scan Reversal therapy Prothrombin complex concentrate Intravenous Vitamin K Oral Vitamin K Other Neurosurgical procedures Further hospital attendances Head-injury related to original attendance Other Died Head-injury related Other OVERALL COMPLICATION RATE
12 Basic data Adverse outcomes = 208 (5.9%) 41 (1.1%) deaths, 16 (0.5%) neurosurgery, 145 (4.1%) CT scans grade 1 Further Hospital Attendances (n=37, HI-related): 4 CT scans grade 1, 0 deaths, 2 neurosurgery (overall 0.16% delayed complication) Aim to identify variables (measured at presentation) which may predict the adverse outcome. Variables considered: age, gender, INR, GCS, symptoms: vomiting, amnesia, headache, loss of consciousness 12
13 Univariateanalyses Univariate analysis OR Lower limit 95% CI Upper limit 95%CI No. of records Age(70-79) Age(80+) Age (70+) Gender (female) GCS(3-12) INR (2-3.9) INR(4+) INR(4+) Vomiting Loss of consciousness Headache Amnesia Logistic regression with adverse outcome as outcome and hospital site treated as a random effect

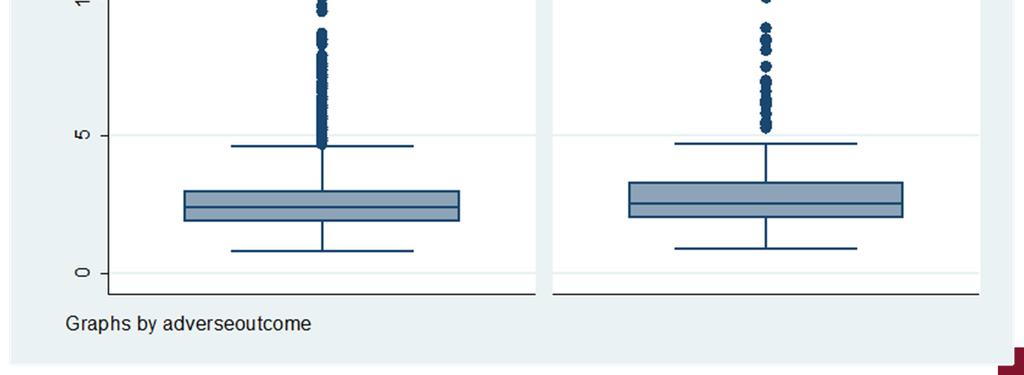
14 Distribution of INR by adverse outcome
15 GCS below patients have a GCS below 13 and 29 of these have an adverse outcome. The absolute risk for this group is 48% (95% CI35.69% to60.97%). Compared to those with GCS 13 and above, the relative risk is 8.7 (95%CI ). As the risk in this small group is very high we removed these from the analysis to try to predict risk for those with GCS of 13 and above.
16 Univariateanalysis (GCS 13) Univariate analysis OR Lower limit 95% CI Upper limit 95%CI No. of records Age(70-79) Age(80+) Age (70 plus) Gender (female) INR (2-4) INR(>4) INR(>4) Vomiting Loss of consciousness Headache Amnesia So when limiting the analysis to those with GCS 13 only the four symptoms above are significant.
17 Risk level GCS=15 and no neurological symptoms GCS=15 and at least one neurological symptom Patients, n Relative Risk of Adverse Adverse events, n (%) Outcome 1838 (52.0%) 52 (2.8%) -- RR 95%CI p-value 828 (23.4%) 70 (8.5%) <0.001 GCS below (10.1%) 75(20.9%) <0.001 Excludes records with missing data 17
18 NICE patients eligible for a CT scan, 70% identified due to risk factors other than warfarin In real practice, of these 756 patients: 82.4% [623] patients had a CT scan performed 14.2 % [107] significant intracranial abnormality identified Average time to scan 4 hrs 42 mins, 75%scanned within 4hrs 133 patients eligible for a CT scan (according to NICE) but no CT scan performed 18
19 NICE 2007: eligible patients Patient outcomes CT scan (n=623) n % Admitted Length of stay, mean 9.2 days Reversal therapy Neurosurgery HI-related deaths Re-attended ED due to HI No CT scan (n=133) n % days * * RTA, patient died in ED before CT could be done 19
20 NICE 2007: site variability CT Eligible CT Performed 50 Patients, n Hospital site
21 CT scanning Real World According to NICE 2007 criteria, 20.4%[756] AHEAD patients should have had a CT scan In practice, 60%[2,114] patients actually had a CT scan Significant intracranial abnormality identified in 9.2%[195] Average time to scan 6.3 hours Outcomes for all anticoagulated patient cohort HI-related deaths 1.2%[42], no CT scan for 4 patients Re-attended ED due to HI 1.0%[37], no CT scan for 20 patients initially. 4 CT scans grade 1, 0 deaths, 2 neurosurgery (overall 0.16% delayed complication) Lots of variability across sites in use of CT scans 21
22 CT scanning: site variability % CT scan No CT scan % 23% 200 Patients, n Hospital site
23 NICE 2014 All patients taking warfarin that experience a head injury should receive a CT scan Based on this cohort, additional 40%[1,420] patients Additional costs, time, resources Burden may not be felt the same across all hospital sites, impact some sites significantly more than others 23
24 Various scenarios modelled to explore costeffectiveness including:- CT scan no patients CT scan patients with significant risk factors (vomiting; LoC) CT scan all patients (NICE 14) CT scan Real World Cost-effectiveness Impact/ yearly costs and utility costs assigned to GOS level Considerable uncertainty i.e. observed data only, estimation of GOS score, assessment of the counterfactual 24
25 Take Home message Largest cohort of anticoagulated head injury patients reported Complication rate in all, 4.3% in GCS=15 Delayed bleeds very Risk of complication significantly increased in alert patients who present with amnesia, vomiting, loss of consciousness, headache 25
26 Majority of patients that fulfilled the NICE 2007 criteria did have a CT scan (82%), but significant inter-site variation A significant number of patients that did not fulfill the NICE 2007 criteria also had a CT scan Require a significant increase in CT scans performed to adhere to NICE 2014 Modelling suggests Real World CT scanning practice most cost-effective strategy go with your gut!! Further studies include validation of these findings
27 Barts Health NHS Trust With thanks to all our study sites for their participation Blackpool Teaching Hospitals NHS Foundation Trust Cambridge University Hospitals NHS Foundation Trust County Durham and Darlington NHS Foundation Trust Gateshead Health NHS Trust Heatherwood and Wexham Park Hospitals NHS Foundation Trust Hull and East Yorkshire Hospitals NHS Trust King's College Hospital NHS Foundation Trust Mid Essex Health Services NHS Trust Milton Keynes Hospital NHS Foundation Trust Newcastle Upon Tyne Hospitals NHS Foundation Trust NHS Lothian North Bristol NHS Trust North Tees And Hartlepool NHS Foundation Trust Northampton General Hospital NHS Trust Nottingham University Hospitals NHS Trust Plymouth Hospitals NHS Trust Poole Hospital NHS Foundation Trust Portsmouth Hospitals NHS Trust Royal Berkshire NHS Foundation Trust Royal United Hospital Bath NHS Trust Sheffield Teaching Hospitals NHS Foundation Trust South Tees Hospitals NHS Foundation Trust The Queen Elizabeth Hospital King's Lynn NHS Foundation Trust University Hospitals Bristol NHS Foundation Trust University Hospitals of Leicester NHS Trust University Hospitals Of Morecambe Bay NHS Foundation Trust Western Sussex Hospitals NHS Trust York Teaching Hospital NHS Foundation Trust This presentation presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme(Grant Reference Number PB-PG ). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
BMJ Open. The AHEAD Study: An evaluation of the management of anticoagulated patients who suffer head injury
 The AHEAD Study: An evaluation of the management of anticoagulated patients who suffer head injury Journal: BMJ Open Manuscript ID bmjopen-0-0 Article Type: Research Date Submitted by the Author: -Sep-0
The AHEAD Study: An evaluation of the management of anticoagulated patients who suffer head injury Journal: BMJ Open Manuscript ID bmjopen-0-0 Article Type: Research Date Submitted by the Author: -Sep-0
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
A bout million patients present to UK hospitals
 420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
420 ORIGINAL ARTICLE Application of the Canadian CT head rules in managing minor head injuries in a UK emergency department: implications for the implementation of the NICE guidelines H Y Sultan, A Boyle,
National Haemoglobinopathy Registry. Annual Report 2017/18
 National Haemoglobinopathy Registry Annual Report 2017/18 National Haemoglobinopathy Registry Annual Report (2017/18) Compiled by Mark Foster MDSAS 3 1 Introduction CHAPTER 1 The 2017/18 Annual Report
National Haemoglobinopathy Registry Annual Report 2017/18 National Haemoglobinopathy Registry Annual Report (2017/18) Compiled by Mark Foster MDSAS 3 1 Introduction CHAPTER 1 The 2017/18 Annual Report
Imaging Biomarkers Significance S100B NSE. Admitted within 6 hours of injury and CT scan occurred after initial examination. N = 1,064 CT+ N = 50 4.
 Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Concussion Guidelines Step 1: Systematic Review of Prevalent Indicators Supplemental Content 7 Evidence Table. Included Studies For Key Question 4 Imaging and Biomarker Publications Medium Potential for
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision
 Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Avoidable Imaging Learning Collaborative: 2008 Mild Traumatic Brain Injury Clinical Policy Success Story BWH Head and PE CTs with Clinical Decision Support Using the Canadian CT Head Rule to Reduce Unnecessary
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
GRASP-AF- The National Picture. Dr Richard Healicon National Improvement Lead Ian Robson Senior Analyst NHS Improvement February 2012
 GRASP-AF- The National Picture Dr Richard Healicon National Improvement Lead Ian Robson Senior Analyst NHS Improvement February 2012 Outline AF and stroke Objective Management of stroke risk Stroke risk
GRASP-AF- The National Picture Dr Richard Healicon National Improvement Lead Ian Robson Senior Analyst NHS Improvement February 2012 Outline AF and stroke Objective Management of stroke risk Stroke risk
National Haemoglobinopathy Registry. Annual Report 2015/16. mdsas
 National Haemoglobinopathy Registry Annual Report 2015/16 mdsas National Haemoglobinopathy Registry Annual Report (2015/16) 3 1 Introduction CHAPTER 1 This 2015/16 data update follows the same format as
National Haemoglobinopathy Registry Annual Report 2015/16 mdsas National Haemoglobinopathy Registry Annual Report (2015/16) 3 1 Introduction CHAPTER 1 This 2015/16 data update follows the same format as
Can we abolish skull x-rays for head injury?
 ADC Online First, published on April 25, 2005 as 10.1136/adc.2004.053603 Can we abolish skull x-rays for head injury? Matthew J Reed, Jen G Browning, A. Graham Wilkinson & Tom Beattie Corresponding author:
ADC Online First, published on April 25, 2005 as 10.1136/adc.2004.053603 Can we abolish skull x-rays for head injury? Matthew J Reed, Jen G Browning, A. Graham Wilkinson & Tom Beattie Corresponding author:
Referral Criteria for Medical CT Radiation Exposures. Neuro Referrals
 Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Referral Criteria for Medical CT Radiation Exposures Neuro Referrals CHH & HRI The Ionising Radiation (Medical Exposure) Regulations 2017 Document Control Reference No: 3.2 First published: 2016 Version:
Use of CT in minor traumatic brain injury. Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD
 Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
Use of CT in minor traumatic brain injury Lisa Ayoub-Rodriguez, MD Bert Johansson, MD Michael Lee, MD No financial or other conflicts of interest Epidemiology of traumatic brain injury (TBI) Risks associated
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Efficiency
 Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
Measure #416: Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 2 Through 17 Years - National Quality Strategy Domain: Efficiency and Cost Reduction
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Correspondence to:
 The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
The risk of a bleed after delayed head injury presentation to the ED: systematic review protocol. Carl Marincowitz, Christopher M. Smith, William Townend Emergency Department, Hull Royal, Hull, UK Correspondence
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
recommendations of the Royal College of
 Archives of Emergency Medicine, 1993, 10, 138-144 Skull X-ray after head injury: the recommendations of the Royal College of Surgeons Working Party Report in practice R. E. MACLAREN, H. I. GHOORAHOO &
Archives of Emergency Medicine, 1993, 10, 138-144 Skull X-ray after head injury: the recommendations of the Royal College of Surgeons Working Party Report in practice R. E. MACLAREN, H. I. GHOORAHOO &
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Fracture Liaison Service database-first review of patient data
 Fracture Liaison Service database-first review of patient data Professor Finbarr C Martin Clinical lead for the National Falls and Fragility Fracture Audit Programme (emeritus consultant geriatrician,
Fracture Liaison Service database-first review of patient data Professor Finbarr C Martin Clinical lead for the National Falls and Fragility Fracture Audit Programme (emeritus consultant geriatrician,
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
O ne million patients are treated annually in United
 859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
859 ORIGIAL ARTICLE Can we abolish skull x rays for head injury? M J Reed, J G Browning, A G Wilkinson, T Beattie... See end of article for authors affiliations... Correspondence to: Matthew J Reed, Accident
DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY
 J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
J Rehabil Med 2004; Suppl. 43: 61 75 DIAGNOSTIC PROCEDURES IN MILD TRAUMATIC BRAIN INJURY: RESULTS OF THE WHO COLLABORATING CENTRE TASK FORCE ON MILD TRAUMATIC BRAIN INJURY Jörgen Borg, 1 Lena Holm, 2
:: Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of :: Closed Head Injury in Adults Suggested citation: Dr Duncan Reed 2007, Adult Trauma Clinical Practice Guidelines, Initial Management of
EVIDENCE ON MINOR HEAD INJURY IN GERIATRICS. Janet Talbot-Stern, FACEM, FRCEM, FACEP
 EVIDENCE ON MINOR HEAD INJURY IN GERIATRICS Janet Talbot-Stern, FACEM, FRCEM, FACEP Definition: Minor head injury 1 Minor HI GCS 15, LOC, amnesia or confusion Minimal HI GCS 15, no LOC, amnesia or confusion
EVIDENCE ON MINOR HEAD INJURY IN GERIATRICS Janet Talbot-Stern, FACEM, FRCEM, FACEP Definition: Minor head injury 1 Minor HI GCS 15, LOC, amnesia or confusion Minimal HI GCS 15, no LOC, amnesia or confusion
The research questions are presented in priority order, and are further elaborated with lay summaries and three-part questions where applicable.
 Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
Top 30 Emergency Medicine Research Priorities 23 January 2017 The rankings were established by consensus at the final prioritisation workshop run by the James Lind Alliance Emergency Medicine Priority
The New England Journal of Medicine A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES
 A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
A POPULATION-BASED STUDY OF SEIZURES AFTER TRAUMATIC BRAIN INJURIES JOHN F. ANNEGERS, PH.D., W. ALLEN HAUSER, M.D., SHARON P. COAN, M.S., AND WALTER A. ROCCA, M.D., M.P.H. ABSTRACT Background The risk
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
London School of Hygiene and Tropical Medicine, Keppel Street, London, UK 2
 CRASH-2 (Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage) intracranial bleeding study: the effect of tranexamic acid in traumatic brain injury a nested, randomised, placebo-controlled
CRASH-2 (Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage) intracranial bleeding study: the effect of tranexamic acid in traumatic brain injury a nested, randomised, placebo-controlled
Preventing the uptake of smoking by children
 Action on Smoking and Health (ASH) ASLEF Association of Directors of Adult Social Services Association of Pschoanalytic Psychotherapy in the NHS Association of Public Health Observatories Asthma UK Bedfordshire
Action on Smoking and Health (ASH) ASLEF Association of Directors of Adult Social Services Association of Pschoanalytic Psychotherapy in the NHS Association of Public Health Observatories Asthma UK Bedfordshire
Funding research for the future
 Funding research for the future Dr Helen Compton (helen.compton@nihr.ac.uk) Stakeholder Engagement Manager NIHR, Central Commissioning Facility The future of health and social care depends on today's research
Funding research for the future Dr Helen Compton (helen.compton@nihr.ac.uk) Stakeholder Engagement Manager NIHR, Central Commissioning Facility The future of health and social care depends on today's research
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Registered childcare providers and places in England, 30 September October 2004
 Registered childcare providers and places in England, 30 September 2004. 21 October 2004 Contents: Childcare statistics About this publication Registered childcare providers and places in England, by Ofsted
Registered childcare providers and places in England, 30 September 2004. 21 October 2004 Contents: Childcare statistics About this publication Registered childcare providers and places in England, by Ofsted
Acute Frailty Network.
 Acute Frailty Network The Acute Frailty Network brings together an effective blend of practical expertise and experience to support organisations to successfully implement and improve Acute Frailty Services
Acute Frailty Network The Acute Frailty Network brings together an effective blend of practical expertise and experience to support organisations to successfully implement and improve Acute Frailty Services
Outcomes after Elective Repair of Infra-renal Abdominal Aortic Aneurysm. A report from The Vascular Society
 Outcomes after Elective Repair of Infra-renal Abdominal Aortic Aneurysm A report from The Vascular Society March 2012 Contents Contents 1 Foreword 3 Preface 4 Authors 6 Glossary 7 About this report 8 Executive
Outcomes after Elective Repair of Infra-renal Abdominal Aortic Aneurysm A report from The Vascular Society March 2012 Contents Contents 1 Foreword 3 Preface 4 Authors 6 Glossary 7 About this report 8 Executive
Initial Management of Closed Head Injury in Adults
 ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of Closed Head Injury in Adults Summary Document 2nd Edition NSW Ministry of Health 73 Miller St NORTH SYDNEY NSW 2060 Tel (02) 9391 9000 Fax
ADULT TRAUMA CLINICAL PRACTICE GUIDELINES Initial Management of Closed Head Injury in Adults Summary Document 2nd Edition NSW Ministry of Health 73 Miller St NORTH SYDNEY NSW 2060 Tel (02) 9391 9000 Fax
CCLG National Febrile Neutropenia Audit Report 2015
 CCLG National Febrile Neutropenia Audit Report 2015 Audit co-ordinators: Emma Johnson (Associate Specialist in Paediatric Oncology, Edinburgh), Bob Phillips (Hon. Consultant in Paediatric and Adolescent
CCLG National Febrile Neutropenia Audit Report 2015 Audit co-ordinators: Emma Johnson (Associate Specialist in Paediatric Oncology, Edinburgh), Bob Phillips (Hon. Consultant in Paediatric and Adolescent
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG)
") USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
USASOC Neurocognitive Testing and Post Injury Evaluation and Treatment Clinical Practice Guideline (CPG) Note: The intent of this CPG is to serve as general guidance for medics and medical officers. It
Neurological examination of the neurosurgical patient. Dániel Bereczki SU Department of Neurology
 Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Neurological examination of the neurosurgical patient Dániel Bereczki SU Department of Neurology E-learning Indivudual study Interactive learning Self assessment at the end of chapters E-learning Indivudual
Severe Head Injury in an Army Pilot
 Severe Head Injury in an Army Pilot Royal Aeronautical Society Aerospace Medicine Symposium Lt Col C Goldie RAMC 12 Dec 17 Joint Helicopter Command Scope Case History Literature review Aeromedical policy
Severe Head Injury in an Army Pilot Royal Aeronautical Society Aerospace Medicine Symposium Lt Col C Goldie RAMC 12 Dec 17 Joint Helicopter Command Scope Case History Literature review Aeromedical policy
Transplant Activity in the UK
 Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study)
") Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study) Laura Green 1,2,3, Joan Morris 1, Raza Alikhan 4, Nicola Curry 5, Rhona Maclean 6, Khalid Saja 7, Simon Stanworth 3,5,
Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study) Laura Green 1,2,3, Joan Morris 1, Raza Alikhan 4, Nicola Curry 5, Rhona Maclean 6, Khalid Saja 7, Simon Stanworth 3,5,
spontaneous localises pain withdraws to pain abnormal flexion abnormal extension none > 5 years 2 5 years 0 2 years
 APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
APPENDIX. GLASGOW COMA SCALES (GCS) For Adults Alert patients have a total score of 5 Eye Opening: to voice to pain Verbal Score: 5 oriented confused but answers questions inappropriate words: recognises
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report.
 NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults
 Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
Research Brief Clinical Report: Recognizing Subdural Hemorrhage in Older Adults Mark T. Pfefer, RN, MS, DC *1 ; Richard Strunk MS, DC 2 Address: 1 Professor and Director of Research, Cleveland Chiropractic
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Root cause analysis of major lower limb amputations in diabetes 2013/14 at County Durham and Darlington Foundation Trust (CDDFT).
.") Root cause analysis of major lower limb amputations in diabetes 2013/14 at County Durham and Darlington Foundation Trust (CDDFT). By Dr Sara Haq GP Registrar, Durham and Tees Valley Deanery Diabetes Audit
Root cause analysis of major lower limb amputations in diabetes 2013/14 at County Durham and Darlington Foundation Trust (CDDFT). By Dr Sara Haq GP Registrar, Durham and Tees Valley Deanery Diabetes Audit
Andrzej Żyluk 1, Agnieszka Mazur 1, Bernard Piotuch 1, Krzysztof Safranow 2
 POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
POLSKI PRZEGLĄD CHIRURGICZNY 2013, 85, 12, 699 705 10.2478/pjs-2013-0107 Analysis of the reliability of clinical examination in predicting traumatic cerebral lesions and skull fractures in patients with
A primary care response to domestic abuse from research to mainstream: the IRIS story. Gene Feder. Domestic abuse summit 2018 London 4 th May 2018
 A primary care response to domestic abuse from research to mainstream: the IRIS story Gene Feder Domestic abuse summit 2018 London 4 th May 2018 Constance 43 year old care worker who had been my patient
A primary care response to domestic abuse from research to mainstream: the IRIS story Gene Feder Domestic abuse summit 2018 London 4 th May 2018 Constance 43 year old care worker who had been my patient
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 29th April 2014 Compliance
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Regional Trauma Network Trauma Centre Trauma Service RMTN Network Organisation Measures (T13-1C-1) - 2013/14 Peer Review Visit Date 29th April 2014 Compliance
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
The optimum time to assess complete clinical response (CR)
") The optimum time to assess complete clinical response (CR) following chemoradiation (CRT) using mitomycin C (MMC) or Cisplatin (CisP) with or without Maintenance CisP/5FU in squamous cell carcinoma of
The optimum time to assess complete clinical response (CR) following chemoradiation (CRT) using mitomycin C (MMC) or Cisplatin (CisP) with or without Maintenance CisP/5FU in squamous cell carcinoma of
National Peer Review Report: Brain and CNS Cancer Services Report 2012/2013
 National Peer Review Programme National Peer Review Report: Brain and CNS Cancer Services Report 2012/2013 www.nationalpeerreview.nhs.uk Brain and CNS Cancer Network (Non-Surgical) MDTs) Overall Performance
National Peer Review Programme National Peer Review Report: Brain and CNS Cancer Services Report 2012/2013 www.nationalpeerreview.nhs.uk Brain and CNS Cancer Network (Non-Surgical) MDTs) Overall Performance
Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan
 DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
DOI 10.1186/s40064-016-1781-9 RESEARCH Open Access Canadian CT head rule and New Orleans Criteria in mild traumatic brain injury: comparison at a tertiary referral hospital in Japan Daddy Mata Mbemba 1,2,
Nicotine Management and Smoke Free
 Nicotine Management and Smoke Free From 31 May 2016 Information for Service Users Why are we smoke free? l Tobacco smoking is the largest cause of early deaths and preventable illnesses in England. l One
Nicotine Management and Smoke Free From 31 May 2016 Information for Service Users Why are we smoke free? l Tobacco smoking is the largest cause of early deaths and preventable illnesses in England. l One
Other NCAS Providers. Locality Region Organisation responsible Helpline/Contact number. Barking and Dagenham London Pohwer ICAS
 Other NCAS Providers Locality Region Organisation responsible Helpline/Contact number Barking and Dagenham London Pohwer ICAS 0300 456 2370 Barnet London Pohwer ICAS 0300 456 2370 Barnsley Y&H Barnsley
Other NCAS Providers Locality Region Organisation responsible Helpline/Contact number Barking and Dagenham London Pohwer ICAS 0300 456 2370 Barnet London Pohwer ICAS 0300 456 2370 Barnsley Y&H Barnsley
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older
 emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older emeasure Identifier (Measure Authoring Tool) NQF Number Measurement
emeasure Title Emergency Medicine: Emergency Department Utilization of CT for Minor Blunt Head Trauma for Patients Aged 18 Years and Older emeasure Identifier (Measure Authoring Tool) NQF Number Measurement
Liver biopsy. Information for patients Hepatobiliary
 Liver biopsy Information for patients Hepatobiliary page 2 of 8 What is a liver biopsy? A liver biopsy is a procedure in which we remove a small sample of tissue from your liver and examine it under a
Liver biopsy Information for patients Hepatobiliary page 2 of 8 What is a liver biopsy? A liver biopsy is a procedure in which we remove a small sample of tissue from your liver and examine it under a
Outlook for intracerebral haemorrhage after a MISTIE spell
 Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Type of intervention Other: transplantation. Economic study type Cost-utility analysis.
 Midterm cost-effectiveness of the liver transplantation program of England and Wales for three disease groups Longworth L, Young T, Buxton M J, Ratcliffe J, Neuberger J, Burroughs A, Bryan S Record Status
Midterm cost-effectiveness of the liver transplantation program of England and Wales for three disease groups Longworth L, Young T, Buxton M J, Ratcliffe J, Neuberger J, Burroughs A, Bryan S Record Status
A protocol for the development of a prediction model in mild traumatic brain injury with CT scan abnormality: which patients are safe for discharge?
 Marincowitz et al. Diagnostic and Prognostic Research (2018) 2:6 https://doi.org/10.1186/s41512-018-0027-4 Diagnostic and Prognostic Research PROTOCOL A protocol for the development of a prediction model
Marincowitz et al. Diagnostic and Prognostic Research (2018) 2:6 https://doi.org/10.1186/s41512-018-0027-4 Diagnostic and Prognostic Research PROTOCOL A protocol for the development of a prediction model
Pediatric head trauma: the evidence regarding indications for emergent neuroimaging
 DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
DOI 10.1007/s00247-008-0996-5 ALARA: BUILDING BRIDGES BETWEEN RADIOLOGY AND EMERGENCY MEDICINE Pediatric head trauma: the evidence regarding indications for emergent neuroimaging Nathan Kuppermann Received:
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Major Trauma Service in England - TARN s supporting role
 The Trauma Audit & Research Network Major Trauma Service in England - TARN s supporting role Scottish Trauma Audit Group National Meeting 11 th November 2016 Major Trauma Services in England - TARN s supporting
The Trauma Audit & Research Network Major Trauma Service in England - TARN s supporting role Scottish Trauma Audit Group National Meeting 11 th November 2016 Major Trauma Services in England - TARN s supporting
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Correlation of Computed Tomography findings with Glassgow Coma Scale in patients with acute traumatic brain injury
 Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
Journal of College of Medical Sciences-Nepal, 2014, Vol-10, No-2 ABSTRACT OBJECTIVE To correlate Computed Tomography (CT) findings with Glasgow Coma Scale (GCS) in patients with acute traumatic brain injury
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma
 Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Just like Adults? Evaluating the Impact of Fluid Resuscitation in Pediatric Trauma Abbas PI 1,2, Carpenter K 2, Sheikh F 1,2, Peterson ML 1,2, Kljajic M 1, Naik-Mathuria B 1,2 1 Texas Children s Hospital
Hospital Norovirus Outbreak Reporting
 Second Report of the Health Protection Agency. Hospital Norovirus Outbreak Reporting Summary findings In January 2009 the HPA in conjunction with the Infection Prevention Society launched a voluntary National
Second Report of the Health Protection Agency. Hospital Norovirus Outbreak Reporting Summary findings In January 2009 the HPA in conjunction with the Infection Prevention Society launched a voluntary National
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Sentinel Stroke National Audit Programme (SSNAP) Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017
 Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017") Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Effect of antiplatelet/anticoagulant agents in elderly patients of chronic subdural hematoma: a case control study from a tertiary care centre
 International Journal of Research in Medical Sciences Potdar NV et al. Int J Res Med Sci. 2017 Jul;5(7):2947-2951 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172538
International Journal of Research in Medical Sciences Potdar NV et al. Int J Res Med Sci. 2017 Jul;5(7):2947-2951 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20172538
20s Plenty for Us Action on Smoking & Health Action on Smoking & Health (ASH) Action on Smoking & Health (ASH) Scotland Advertising Standards
 Action on Smoking & Health (ASH) Scotland Advertising Standards") 20s Plenty for Us Action on Smoking & Health Action on Smoking & Health (ASH) Action on Smoking & Health (ASH) Scotland Advertising Standards Authority Advertising Standards Authority (ASA) Age Concern
20s Plenty for Us Action on Smoking & Health Action on Smoking & Health (ASH) Action on Smoking & Health (ASH) Scotland Advertising Standards Authority Advertising Standards Authority (ASA) Age Concern
Guideline for Treatment of Head Injury in the Anticoagulated Patient
 Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
Concussion Update and Case Presentations
 Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
National Peer Review Report: Sarcoma Cancer Services Report 2012/2013
 National Peer Review Programme National Peer Review Report: Sarcoma Cancer Services Report 2012/2013 www.nationalpeerreview.nhs.uk Sarcoma MDT Overall Performance All 15 services reviewed against the 36
National Peer Review Programme National Peer Review Report: Sarcoma Cancer Services Report 2012/2013 www.nationalpeerreview.nhs.uk Sarcoma MDT Overall Performance All 15 services reviewed against the 36
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
Position statement: Anti-coagulants and Risk Assessment
 Position statement: Anti-coagulants and Risk Assessment Document information Protective marking: NOT PROTECTVELY MARKED Author: Matt Johnston Force/Organisation: College of Policing NPCC Coordination Committee
Position statement: Anti-coagulants and Risk Assessment Document information Protective marking: NOT PROTECTVELY MARKED Author: Matt Johnston Force/Organisation: College of Policing NPCC Coordination Committee
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.15.12.2016/04 Title: Taking the cancer strategy forward: programme update Lead Director: Professor Sir Bruce Keogh, National Medical Director Cally Palmer, National Cancer
NHS ENGLAND BOARD PAPER Paper: PB.15.12.2016/04 Title: Taking the cancer strategy forward: programme update Lead Director: Professor Sir Bruce Keogh, National Medical Director Cally Palmer, National Cancer
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Smoking Cessation in Secondary Care: list of registered stakeholders
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Smoking Cessation in Secondary Care: list of registered stakeholders List of Registered Stakeholders as of 4 th June 2013 20s Plenty for Us Abbey Community
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Smoking Cessation in Secondary Care: list of registered stakeholders List of Registered Stakeholders as of 4 th June 2013 20s Plenty for Us Abbey Community
Durham Research Online
 Durham Research Online Deposited in DRO: 4 June 29 Version of attached file: Published Version Peer-review status of attached file: Peer-reviewed Citation for published item: Macknight, N. and Bailey,
Durham Research Online Deposited in DRO: 4 June 29 Version of attached file: Published Version Peer-review status of attached file: Peer-reviewed Citation for published item: Macknight, N. and Bailey,
NICE Guidelines for C-Spine Imaging: Real Life Impact
 NICE Guidelines for C-Spine Imaging: Real Life Impact Poster No.: C-1367 Congress: ECR 2017 Type: Scientific Exhibit Authors: D. Weinberg, I. Djoukhadar, G. Potter; Salford/UK Keywords: Trauma, Audit and
NICE Guidelines for C-Spine Imaging: Real Life Impact Poster No.: C-1367 Congress: ECR 2017 Type: Scientific Exhibit Authors: D. Weinberg, I. Djoukhadar, G. Potter; Salford/UK Keywords: Trauma, Audit and
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
National audit of inpatient falls
 National audit of inpatient falls Commissioners report 2015 North West In association with: Commissioned by: Contents Key issue 4 Methodology 4 Organisational audit 4 Clinical audit 4 Key findings 5 Organisational
National audit of inpatient falls Commissioners report 2015 North West In association with: Commissioned by: Contents Key issue 4 Methodology 4 Organisational audit 4 Clinical audit 4 Key findings 5 Organisational
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
SCHEDULE 2 THE SERVICES. A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 04/MSKT/0013 Service PAN DORSET FRACTURE LIAISON SERVICE Commissioner Lead CCP for Musculoskeletal & Trauma Provider Lead Deputy
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 04/MSKT/0013 Service PAN DORSET FRACTURE LIAISON SERVICE Commissioner Lead CCP for Musculoskeletal & Trauma Provider Lead Deputy
Thrombosis and Anticoagulation Team. Warfarin. Information for patients, relatives and carers
 Thrombosis and Anticoagulation Team Warfarin Information for patients, relatives and carers What is warfarin? Warfarin is an anticoagulant. Anticoagulants are drugs which prevent harmful blood clots forming
Thrombosis and Anticoagulation Team Warfarin Information for patients, relatives and carers What is warfarin? Warfarin is an anticoagulant. Anticoagulants are drugs which prevent harmful blood clots forming
Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian. Barry McKenzie, MD St. Vincent Healthcare
 Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian Barry McKenzie, MD St. Vincent Healthcare Objectives Describe the increasing frequency of trauma patients being
Under Triage and Anticoagulants in the Geriatric Trauma Population Fragile Must be Italian Barry McKenzie, MD St. Vincent Healthcare Objectives Describe the increasing frequency of trauma patients being
Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study
 136 Original Article Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study Kairav S. Shah 1 Jayun Shah 1 Ponraj K. Sundaram 1 1 Department of Neurosurgery,
136 Original Article Phenytoin versus Levetiracetam for Prevention of Early Posttraumatic Seizures: A Prospective Comparative Study Kairav S. Shah 1 Jayun Shah 1 Ponraj K. Sundaram 1 1 Department of Neurosurgery,
The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
Clinical Oncology UK Workforce Report 2012 Faculty of Clinical Oncology
 www.rcr.ac.uk Clinical Oncology UK Workforce Report 2012 Faculty of Clinical Oncology www.rcr.ac.uk Contents Foreword 3 1. Introduction and objectives 4 2. Census methodology 5 3. UK clinical oncology
www.rcr.ac.uk Clinical Oncology UK Workforce Report 2012 Faculty of Clinical Oncology www.rcr.ac.uk Contents Foreword 3 1. Introduction and objectives 4 2. Census methodology 5 3. UK clinical oncology