DEMENTIA IN PARKINSON`S DISEASE. DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
|
|
|
- Alicia Barton
- 5 years ago
- Views:
Transcription
1 DEMENTIA IN PARKINSON`S DISEASE DR C PADMAKUMAR MD FRACP FRCP(Edin) Director-Parkinson`s Disease Service for the Older Person HNELHD
2 DEMENTIA IN PD The concept of Non Motor Symptoms in PD Dementia in Parkinson`s Disease ( PDD) How is PDD different from Alzheimer`s Dementia Management of Dementia in PD

3 DR JAMES PARKINSON 1817 Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with a propensity to bend the trunk forward, and to pass from a walking to a running pace: the senses and intellects being uninjured

4 Mov Disord Apr 30;23(6): doi: /mds The Sydney multi center study of Parkinson's disease; the inevitability of Dementia at 20 years Hely MA, Reid WG, Adena MA, Halliday GM, Morris JG. Source Department of Neurology, Westmead Hospital, Westmead, New South Wales, Australia.
5 BRAIN FAILURE The common denominator for disease burden in Elderly Stroke/ Dementia/Parkinson`s Disease

6 IDIOPATHIC PARKINSON`S DISEASE

7 IDIOPATHIC PARKINSONS DISEASE
8 PARKINSON`S DISEASE DIAGNOSIS The 4 S! SLOWNESS STIFFNESS SHAKES STUMBLES 2 out 4 diagnostic of Idiopathic PD Bradykinesia Must be present
9

10 BRAAK`S HYPOTHESIS Challenging the conventional wisdom. Staging of Brain Pathology related to Parkinson's Disease. Neurobiology of Aging 2003 : 24;
11 ALPHA SYNUCLEIN
12 EARLY NMS Loss of Smell Urinary Incontinence Sexual dysfunction Orthostatic & Post Prandial Hypotension Depression,Anxiety,Apathy Sleep : RBD, Increased day time sleep, Insomnia
13 LATE NMS DEMENTIA DEPRESSION POSTURAL HYPOTENSION URINARY INCONTINENCE PAIN FALLS NEUROPSYCHIATRIC SYMPTOMS
14 HOW TO DIAGNOSE NMS? PD NMS QUESTIONNAIRE

15 PD IS NOT JUST A MOVEMENT DISORDER IT`S A MOOD DISORDER The Tremulous Mind Anxiety, Apathy, Depression, Anhedonia. Dementia
16 DEMENTIA DSM 1V edition Multiple cognitive deficits that affect Memory Aphasia Apraxia Agnosia Executive dysfunction
17 WHERE IS THE PROBLEM? Degeneration of Limbic & Neo-cortex in addition to Corpus Striatum changes. Motor Putamen Cognition Caudate Nucleus & Cortico striate fibres.
18 COGNITION PROFILE IN PD Executive dysfunction : Dopaminergic fibres Attention deficits : Nor Adrenergic fibres Mnemonic deficits : Cholinergic fibres
19 DEMENTIA IN PD PD carries a 6 fold risk of getting Dementia Point prevalence of 30%-40% Increasing longevity may explain the increase incidence PDD represents 3-4% of Dementias Age, more than 70,increases Dementia risk Severe motor features,axial rgidity and postural instability gait disorder ( PGID) increases the risk
20 EXECUTIVE FUNCTION Ability to plan initiate complex, goal directed behaviour Difficulty processing information Shifting focus.difficult to concentrate Struggle to solve multiple step problems Difficulty in actively retrieving information Relies heavily on the integrity of Pre Frontal Cortex
21 PATIENT DESCRIPTION `I do well, if I`m doing things that are routine and if I do them slowly. I have always been a clear thinker,with good attention to detail. I can still do that, but not if I have to think of more than one thing at a time.
22 Today I have been helping my 2 grandchildren learn to play a board game. Just the teaching of things like this me makes me irritable and frustrated, The 7 year old can`t sit still and spills and knocks things onto the floor all the time ;while the 10 year old knows everything.i was also trying to put dirty dishes into my daughter`s dishwasher at the same time.
23 By the time the game was over I was at the end of my tether.i have now decided that I can play a game with the kids one at a time, even if I have to play twice in a row and then wash the dishes!`
24 KEY PROBLEM Difficulty in resisting cognitive interference Trivial tasks become important; difficulty ignoring them 2 or 3 things cannot happen at the same time together
25 DEMENTIA IN PD 1. Dopaminergic dysfunction Lack of dopamine Disruption of striatal-frontal connections Anatomical substrate : Frontal lobe Functional deficit : Executive impairment
26 DEMENTIA IN PD 2.Cortical Cholinergic deficit Nucleus Basalis of Meynert situated in the basal forebrain full of cholinergic neurons that project into the cortex Significant loss of basal forebrain in PDD Critical threshold of forebrain loss ( 60-80%)
27 CRITICAL ASSOCIATION 3. LEWY BODIES in Cortex and Limbic system LB in Cortex 91%sensitive and 90% specific for PDD Lewy Bodies : can be found in normal patients ; hence `where` it is found is more important than it`s actual presence
28 LEWY BODY
29 DEMENTIA IN PD APOE increases risk of AD MAPT gene increases risk of Dementia in PD H1/H1 genotype of MAPT gene is an independent predictor of Dementia in PD
30 DIFFERENCE BETWEEN AD & PDD Subcortical v Cortical dementia Slowing of the mind ( Bradyphrenia) Changes in personality & mood Inability to use acquired knowledge Diminished ability to retrieve learned information forgetfulness PDD
31 CORTICAL DEMENTIAS Frank amnesia Aphasia Apraxia Agnosia AD These are absent in PDD Also INSIGHT IS RELATIVELY INTACT in PDD.
32 DIAGNOSIS MMSE not suitable,since executive symptoms are affected. ACE-R Frontal Assessment Battery MOCA
33 DEMENTIA LEWY BODY DLB Second commonest type of Dementia 15% Extensive overlap between the pathological features of both AD & PD Dementia Fluctuations in attention and arousal Visual Hallucinations Parkinsonism 1-2 year rule in Diagnosis
34 DLB PDD and DLB not 2 separate entities but represent a spectrum of same pathological process ; difference because of parts of the brain affected No single pathological feature separating PD & DLB Early involvement of Amygdala cognitive changes and Temporal lobe - Hallucinations
35 PD MILD COGNITIVE IMPAIRMENT ( PD MCI) PD MCI now a well described clinical entity Compared to MCI in AD, Non amnestic type more common in PD PD MCI is a risk factor for getting PDD Memory loss or difficulty concentrating, but functioning well otherwise ; good scores on cognitive assessment
36 AD Gross pathology Brain atrophy Loss of neurons Gliosis Loss of Synapses
37 AD Abnormally phosphorylated TAU protein present in surviving neurons as paired helical filaments.nft NFT within the cell body Neuropil threads NT in the dendritic processes Specific to AD
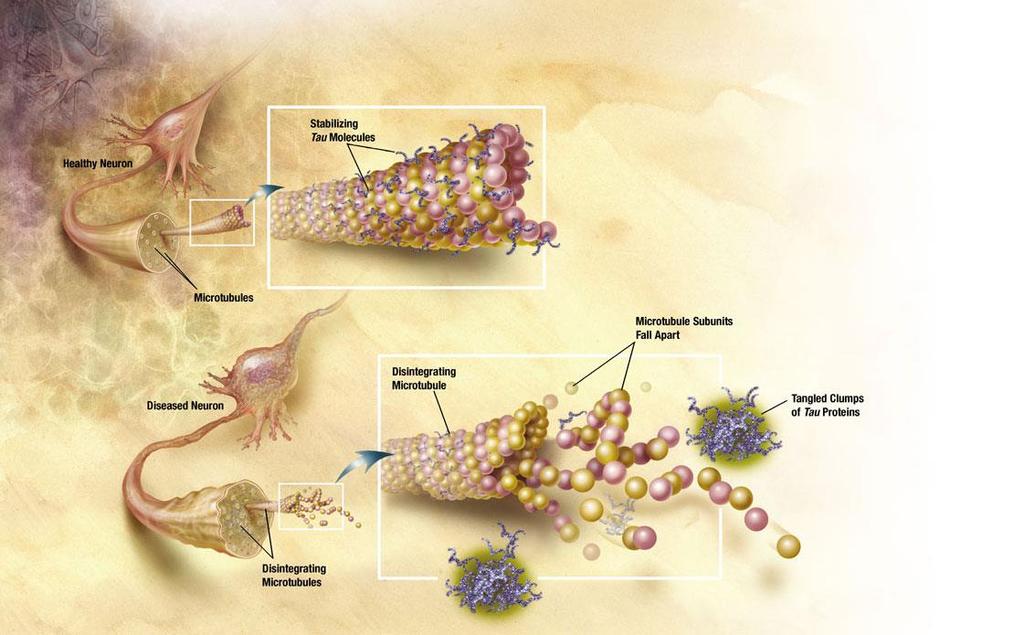
38 TAU & AD
39 ALPHA SYNUCLEIN
40 PD Gross Neuronal loss Gliosis Presence of Lewy Bodies LB : Eosinophilic inclusions found in the nerve cells made up of Ubiquitin and Aggregations of Alpha Synculein Lewy Neurites : Thread like inclusions within neurites
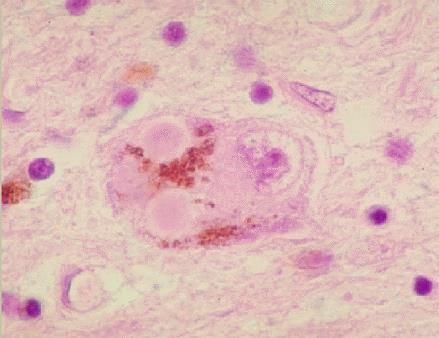
41 LEWY BODY
42 TREATMENT OF DEMENTIA IN PD Important for family members and carers to realise, acknowledge and adapt to patient`s limitations, which may not be just physical. Tremors of the Mind need looking after as well.
43 TREATMENT OF PDD Aerobic exercise evidence based WALKING..the best treatment for Dementia
44 TREATMENT OF DEMENTIA FOOD! REGULAR MEALS 1 HOT MEAL PER DAY, MINIMUM!! Attention to Nutrition reduces risk of infection and mortality Gil Gregolino P et al J Nutr Health Aging 2003: 7:304-8
45 TREATMENT Mind the Mind! Nintendo ( Mind-Gym) Avoid distractions.especially while driving Pro actively planning for the future POA& EG. Social support Improving interactions
46 MEDICAL TREATMENT OF PDD Not which tablet to start but.which tablet to stop! Reduce the dose / eliminate medications which will worsen cognition Dopa agonists MAO B inhibitors Anticholinergic drugs like trihexyphenidyl Amantadine Never Stop suddenly in PD!
47 MEDICAL TREATMENT OF PDD Maintaining the patient on lowest possible dose of monotherapy with L-Dopa, without leading to unacceptable immobility
48 CHOLINE ESTERASE INHIBITORS Used in AD Cholinergic transmission is reduced Cholinergic neurons depleted Similar pathology in PDD ; especially in DLB Hence should be useful
49 EXPRESS Rivastigmine 541 patients randomised to Placebo or Rivastigmine daily Followed for 26 weeks Modest but statistically significant improvement in ADAS-Cog scores
50 EDON Donepezil in PDD 549 patients studied 24 weeks Dose dependent benefit with Donepezil
51 TREATMENT PDD patients doesn`t tolerate Dopaminergic treatment as well those without Dementia Hence motor symptoms suffer because of restriction in the use of L-Dopa doses PDD is a contraindication for DBS
52 CHOLINE ESTERASE INHIBITOR IN PDD A trial with choline esterase inhibitor is reasonable and should be offered to any patient with cognitive dysfunction serious enough to impair QOL.
53 THE FUTURE Disease modifying agents for PD. Inhibition of Alpha Synuclein accumulation in susceptible brain cells. Drugs which stimulate cholinergic receptors rather than ChEIs needed.

54 GP,GERIATRICIAN,NEUROLOGIST NEUROPSYCHIATRIST & PD SPECIALIST NURSE

55

56 1 HOXTON SQUARE, SHOREDITCH 200 YEARS OF PARKINSON`S DISEASE 5/09/
57

58 THE ALE HOUSE SERMON

59 SHOREDITCH CHAPEL
60
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
The Spectrum of Lewy Body Disease: Dementia with Lewy Bodies and Parkinson's Disease Dementia
 Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Disclosures Research support, Parkinson Society Canada, Canadian Institutes of Health Research, Ministry of Economic Development and Innovation, Teva Novartis clinical trial, Principal Investigator CME
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Cheyenne 11/28 Neurological Disorders II. Transmissible Spongiform Encephalopathy
 Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Cheyenne 11/28 Neurological Disorders II Transmissible Spongiform Encephalopathy -E.g Bovine4 Spongiform Encephalopathy (BSE= mad cow disease), Creutzfeldt-Jakob disease, scrapie (animal only) -Sporadic:
Overview of neurological changes in Alzheimer s disease. Eric Karran
 Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Overview of neurological changes in Alzheimer s disease Eric Karran Alzheimer s disease Alois Alzheimer 1864-1915 Auguste D. 1850-1906 Case presented November 26 th 1906 Guildford Talk.ppt 20 th March,
Clinical Features and Treatment of Parkinson s Disease
 Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Clinical Features and Treatment of Parkinson s Disease Richard Camicioli, MD, FRCPC Cognitive and Movement Disorders Department of Medicine University of Alberta 1 Objectives To review the diagnosis and
Parkinson's Disease KP Update
 Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
Parkinson's Disease KP Update Andrew Imbus, PA-C Neurology, Movement Disorders Kaiser Permanente, Los Angeles Medical Center No disclosures "I often say now I don't have any choice whether or not I have
P20.2. Characteristics of different types of dementia and challenges for the clinician
 P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
P20.2. Characteristics of different types of dementia and challenges for the clinician, professor Danish Dementia Research Center Rigshospitalet, University of Copenhagen (Denmark) This project has received
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
SECTION 1: as each other, or as me. THE BRAIN AND DEMENTIA. C. Boden *
 I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
I read all the available books by other [people with] Alzheimer s disease but they never had quite the same problems as each other, or as me. I t s not like other diseases, where there is a standard set
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016
 Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016") Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
Let s Look at Parkinson s (PD) Sheena Morgan Parkinson s Disease Nurse Specialist Isle of Wight NHS Trust November 2016 What is Parkinson s? Parkinson's is a progressive neurological condition. People
CAREGIVER SUMMIT. The PD You Can't See: Dealing with Non-Motor Symptoms. Kaitlyn Roland, PhD. Sponsored by:
 CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
CAREGIVER SUMMIT The PD You Can't See: Dealing with Non-Motor Symptoms Kaitlyn Roland, PhD Sponsored by: Cognition VS Dementia Memory Executive Function Attention Bradyphrenia Visuospatial Language Hallucinations
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Dementia and Alzheimer s disease
 Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
Since 1960 Medicine Korat โรงพยาบาลมหาราชนครราชส มา Dementia and Alzheimer s disease Concise Reviews PAWUT MEKAWICHAI MD DEPARTMENT of MEDICINE MAHARAT NAKHON RATCHASIMA HOSPITAL 1 Prevalence Increase
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask. Presented By: Tuesday, March 22, 2011 at 1:00 PM ET
 PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
PD ExpertBriefing: Cognition and PD: What You ve Always Wanted to Know But Were Too Afraid to Ask Presented By: Alexander I. Tröster, PhD, ABPP University of North Carolina, Chapel Hill, NC Tuesday, March
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Neuropathology of Neurodegenerative Disorders Prof. Jillian Kril
 Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Neurodegenerative disorders to be discussed Alzheimer s disease Lewy body diseases Frontotemporal dementia and other tauopathies Huntington s disease Motor Neuron Disease 2 Neuropathology of neurodegeneration
Non Alzheimer Dementias
 Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
Non Alzheimer Dementias Randolph B Schiffer Department of Neuropsychiatry and Behavioral Science Texas Tech University Health Sciences Center 9/11/2007 Statement of Financial Disclosure Randolph B Schiffer,,
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Part I Parkinson Disease Diagnosis and Treatment
 Part I Parkinson Disease Diagnosis and Treatment Parkinson Disease A Health Policy Perspective. Edited by Wayne Martin, Oksana Suchowersky, Katharina Kovacs Burns, and Egon Jonsson Copyright 2010 WILEY-VCH
Part I Parkinson Disease Diagnosis and Treatment Parkinson Disease A Health Policy Perspective. Edited by Wayne Martin, Oksana Suchowersky, Katharina Kovacs Burns, and Egon Jonsson Copyright 2010 WILEY-VCH
How to Diagnose Early (Prodromal) Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.
 Lewy Body Dementia. Ian McKeith MD, FRCPsych, F Med Sci.") How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
How to Diagnose Early (Prodromal) Lewy Body Dementia Ian McKeith MD, FRCPsych, F Med Sci. Parkinson s Disease Lewy Body Disease Time PD Dementia Lewy Body Dementias Dementia with Lewy Bodies (DLB) Diagnostic
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER
 OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
OVERCOMING THE CHALLENGES OF MANAGING CHRONIC DISEASES IN PERSONS WITH DEMENTIA DEMENTIA, THE BRAIN AND HOW IT WORKS AND WHY YOU MATTER LEARNING OBJECTIVES Be familiar with the diagnostic criteria for
First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy"
 Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
Parkinson's Disease First described by James Parkinson in his classic 1817 monograph, "An Essay on the Shaking Palsy" Parkinson s disease (PD) is a neurological disorder characterized by a progressive
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
Understanding Dementia
 Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
Dementia Handbook for Carers Essex Understanding Dementia What is dementia? 1 Summary of dementia symptoms 4 Medication and treatment 5 1 Dementia is the name for several conditions that lead to the progressive
The PD You Don t See: Cognitive Symptoms. Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health
 The PD You Don t See: Cognitive Symptoms Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health OBJECTIVES To understand why cognitive changes occur in a motor disease
The PD You Don t See: Cognitive Symptoms Joanne M. Hamilton, PhD, ABPP Clinical Neuropsychologist Division of Neurology Scripps Health OBJECTIVES To understand why cognitive changes occur in a motor disease
Improving diagnosis of Alzheimer s disease and lewy body dementia. Brain TLC October 2018
 Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Improving diagnosis of Alzheimer s disease and lewy body dementia Brain TLC October 2018 Plan for this discussion: Introduction to AD and LBD Why do we need to improve diagnosis? What progress has been
Parkinsonian Disorders with Dementia
 Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Parkinsonian Disorders with Dementia George Tadros Consultant in Old Age Liaison Psychiatry, RAID, Heartlands Hospital Professor of Dementia and Liaison Psychiatry, Aston Medical School Aston University
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD
 DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
DEMENTIA 101: WHAT IS HAPPENING IN THE BRAIN? Philip L. Rambo, PhD OBJECTIVES Terminology/Dementia Basics Most Common Types Defining features Neuro-anatomical/pathological underpinnings Neuro-cognitive
Issues for Patient Discussion
 onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
onmotor complications radykinesia Screening Tools asked PD micrographia eurodegeneration Designed for Use by Family Practitioners remor on-off opamine agonists tiffness depression ostural instability wearing
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University
 Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Ian McKeith MD, F Med Sci, Professor of Old Age Psychiatry, Newcastle University Design of trials in DLB and PDD What has been learnt from previous trials in these indications and other dementias? Overview
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Parkinson e decadimento cognitivo. Stelvio Sestini
 Parkinson e decadimento cognitivo Stelvio Sestini Patients with PD can develop a spectrum of cognitive symptoms Heterogeneity of cognitive deficits The cognitive symptoms can evolve to dementia (Mov Disorder
Parkinson e decadimento cognitivo Stelvio Sestini Patients with PD can develop a spectrum of cognitive symptoms Heterogeneity of cognitive deficits The cognitive symptoms can evolve to dementia (Mov Disorder
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Clinical Differences Among Four Common Dementia Syndromes. a program of Morningside Ministries
 Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
Clinical Differences Among Four Common Dementia Syndromes a program of Morningside Ministries Introduction Four clinical dementia syndromes account for 90% of all cases after excluding reversible causes
If you have dementia, you may have some or all of the following symptoms.
 About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
About Dementia Dementia may be caused by a number of illnesses that affect the brain. Dementia typically leads to memory loss, inability to do everyday things, difficulty in communication, confusion, frustration,
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Making Things Happen 2: Motor Disorders
 Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Making Things Happen 2: Motor Disorders How Your Brain Works Prof. Jan Schnupp wschnupp@cityu.edu.hk HowYourBrainWorks.net On the Menu in This Lecture In the previous lecture we saw how motor cortex and
Dementia: It s Not Always Alzheimer s
 Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Dementia: It s Not Always Alzheimer s A Caregiver s Perspective Diane E. Vance, Ph.D. Mid-America Institute on Aging and Wellness 2017 My Background Caregiver for my husband who had Lewy Body Dementia
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Origins. Update on Parkinson s Disease
 Update on Parkinson s Disease Melinda Burnett, MD Origins First described in 1817 by James Parkinson: Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported;
Update on Parkinson s Disease Melinda Burnett, MD Origins First described in 1817 by James Parkinson: Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported;
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care.
 Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Dr Georgina Train Consultant Psychiatrist EMDASS service and Continuing Care. Consultant Psychiatrist of both General adult and Old Age Psychiatry. Work with Memory Service and a Continuing Care ward.
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Non-motor symptoms as a marker of. Michael Samuel
 Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Appendix N: Research recommendations
 Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Appendix N: recommendations N.1 First-line treatment of motor symptoms recommendation 1 Interventions What is the effectiveness of initial levodopa monotherapy versus initial levodopa-dopamine agonist
Behavioral Aspects of Parkinson s Disease
 Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Behavioral Aspects of Parkinson s Disease Joseph H. Friedman, MD Director, Movement Disorders Program Butler Hospital Dept of Neurology Alpert Medical School of Brown University 1 Disclosures Drugs will
Assessment Toolkits for Lewy Body Dementia
 Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
Study : Assessment Toolkits for Lewy Body Dementia There are two toolkits, depending on whether the patient is presenting with a primary cognitive problem or with cognitive decline in the context of established
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.
, also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia.") CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
CHAPTER 3 Alzheimer's disease (AD), also known as Senile Dementia of the Alzheimer Type (SDAT) or simply Alzheimer s is the most common form of dementia. This incurable, degenerative, terminal disease
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
Alzheimer s Disease. Pathophysiology: Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior,
 is a progressive dementia affecting cognition, behavior,") 2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
2 Alzheimer s Disease Alzheimer s disease (AD) is a progressive dementia affecting cognition, behavior, and functional status with no known cause or cure. Patients eventually lose cognitive, analytical,
Dementia. Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine
 Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Dementia Jeanette Norden, Ph.D. Professor Emerita Vanderbilt University School of Medicine What is Dementia? Dementia is a general term referring to a decline in cognitive/mental functioning; this decline
Nature, prevalence and clinical significance. Barcelona, Spain
 Nature, prevalence and clinical significance Jaime Kulisevsky Barcelona, Spain 1 Non motor (neuropsychiatric) symptoms are an integral part of Parkinson s s disease (PD) Affective disorders And are associated
Nature, prevalence and clinical significance Jaime Kulisevsky Barcelona, Spain 1 Non motor (neuropsychiatric) symptoms are an integral part of Parkinson s s disease (PD) Affective disorders And are associated
Assessing and Managing the Patient with Cognitive Decline
 Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Assessing and Managing the Patient with Cognitive Decline Center of Excellence For Alzheimer s Disease for State of NY Capital Region Alzheimer s Center of Albany Medical Center Earl A. Zimmerman, MD Professor
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Dementia. Dr Maria Foundas Consultant Physician. Training support Skills development Competency Assessment Scholarships Education
 Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
Dementia Dr Maria Foundas Consultant Physician Training support Skills development Competency Assessment Scholarships Education Preamble and disclaimer These slides are made available by the Western Australian
The human brain. of cognition need to make sense gives the structure of the brain (duh). ! What is the basic physiology of this organ?
. ! What is the basic physiology of this organ?") The human brain The human brain! What is the basic physiology of this organ?! Understanding the parts of this organ provides a hypothesis space for its function perhaps different parts perform different
The human brain The human brain! What is the basic physiology of this organ?! Understanding the parts of this organ provides a hypothesis space for its function perhaps different parts perform different
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
A BRIEF LOOK AT DEMENTIA
 Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia A BRIEF LOOK AT DEMENTIA David Kaufman, MD Neurology Consultants of Bellin Health November 2, 2017 Defined as a progressive decline in cognitive function that impairs daily activities. Always
Dementia. Amber Eker, MD. Assistant Professor Near East University Department of Neurology
 Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Dementia Amber Eker, MD Assistant Professor Near East University Department of Neurology Dementia An acquired syndrome consisting of a decline in memory and other cognitive functions Impairment in social
Depression and Anxiety in Parkinson s Disease. Bill Collins Symposium for Parkinson s Disease 2018 Robert Underwood, Ph.D. Licensed Psychologist
 Depression and Anxiety in Parkinson s Disease Bill Collins Symposium for Parkinson s Disease 2018 Robert Underwood, Ph.D. Licensed Psychologist Today s Discussion Review of Parkinson s Disease and Nonmotor
Depression and Anxiety in Parkinson s Disease Bill Collins Symposium for Parkinson s Disease 2018 Robert Underwood, Ph.D. Licensed Psychologist Today s Discussion Review of Parkinson s Disease and Nonmotor
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817.
 Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
Parkinsonism or Parkinson s Disease I. Symptoms: Main disorder of movement. Named after, an English physician who described the then known, in 1817. Four (4) hallmark clinical signs: 1) Tremor: (Note -
REDEFINING PARKINSON S DISEASE
 REDEFINING PARKINSON S DISEASE Did James Parkinson Get It Right? Matthew B. Stern, M.D. University of Pennsylvania USA 1 Hoxton Square W. Poewe, Austria J. Obeso, Spain E. Tolosa, Spain M. Stern, USA To
REDEFINING PARKINSON S DISEASE Did James Parkinson Get It Right? Matthew B. Stern, M.D. University of Pennsylvania USA 1 Hoxton Square W. Poewe, Austria J. Obeso, Spain E. Tolosa, Spain M. Stern, USA To
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
FDG-PET e parkinsonismi
 Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Parkinsonismi FDG-PET e parkinsonismi Valentina Berti Dipartimento di Scienze Biomediche, Sperimentali e Cliniche Sez. Medicina Nucleare Università degli Studi di Firenze History 140 PubMed: FDG AND parkinsonism
Dementia in Parkinson s disease:
 Dementia in Parkinson s disease: A 20 year Prospective Neuropsychological Study Sydney Multicentre Study Associate Professor Wayne GJ Reid PhD FAPS 149 newly diagnosed community living Parkinson s Disease
Dementia in Parkinson s disease: A 20 year Prospective Neuropsychological Study Sydney Multicentre Study Associate Professor Wayne GJ Reid PhD FAPS 149 newly diagnosed community living Parkinson s Disease
COGNITIVE IMPAIRMENT IN PARKINSON S DISEASE
 1 GENERAL INTRODUCTION GENERAL INTRODUCTION PARKINSON S DISEASE Parkinson s disease (PD) is a neurodegenerative movement disorder, named after James Parkinson who described some of its characteristic
1 GENERAL INTRODUCTION GENERAL INTRODUCTION PARKINSON S DISEASE Parkinson s disease (PD) is a neurodegenerative movement disorder, named after James Parkinson who described some of its characteristic
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
PD AND FALLS J U MALLYA FALLS AWARENESS MEETING
 PD AND FALLS J U MALLYA FALLS AWARENESS MEETING 23-09-2016 PD Chronic Progressive neurodegenerative disease Motor system disorder Degeneration of Dopaminergic neurons in Substantia nigra in the midbrain.
PD AND FALLS J U MALLYA FALLS AWARENESS MEETING 23-09-2016 PD Chronic Progressive neurodegenerative disease Motor system disorder Degeneration of Dopaminergic neurons in Substantia nigra in the midbrain.
The Parkinson s You Can t See
 The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
Parkinson s UK Brain Bank
 Parkinson s UK Brain Bank From Brain to Breakthrough Dr George Gveric Manager 19 October 2018 Coordinated approach Donors Relatives Information Reporting Researchers Tissue supply Quality assurance Expertise
Parkinson s UK Brain Bank From Brain to Breakthrough Dr George Gveric Manager 19 October 2018 Coordinated approach Donors Relatives Information Reporting Researchers Tissue supply Quality assurance Expertise
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,