Delirium and Dementia in Acute Care. Megan Walsh, CRNP, PMHNP-BC Bloomsburg University Geisinger Health System Villanova University
|
|
|
- Clare Preston
- 6 years ago
- Views:
Transcription



1 Delirium and Dementia in Acute Care Megan Walsh, CRNP, PMHNP-BC Bloomsburg University Geisinger Health System Villanova University
2 Disclosures O Nothing to disclose
3 Objectives O Understand the differences between dementia and delirium O Discuss non-pharmacologic management strategies for dementia and delirium O Understand the risks and benefits associated with using psychotropic medications to treat dementia and delirium
4 Delirium O A confused mental state that causes changes in awareness and behavior and may come and go during the day. A person with delirium may also have problems with attention, thinking and memory, hallucinations, emotion, judgement, muscle control, sleep and waking (NIH, n.d.)
5 Delirium O Represents a stark change from baseline O Related to a physiologic disturbance O Infection O Trauma O Hypoxia O Stressors on body O Time and course are unpredictable
6 Two Types of Delirium O Hypoactive O Clinicians tend to miss this sub-type of delirium as patient is usually quiet and intermittently sleeping throughout the day O Hyperactive O More classic picture of delirium O Often some behavioral disturbances present

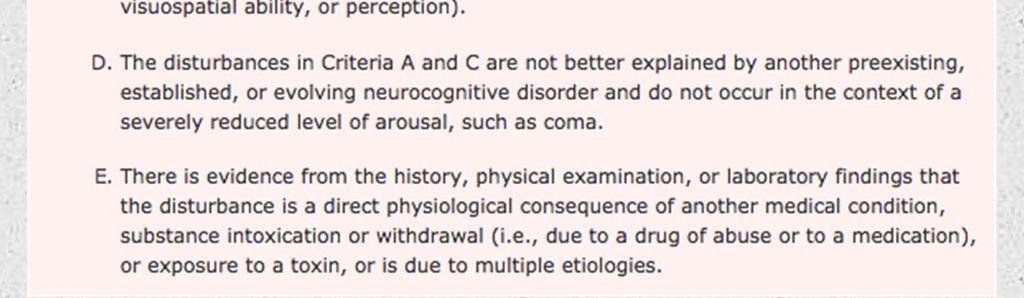
7 Delirium (APA, 2013)
8 Delirium O Characteristics: O Abrupt or sudden onset O Disturbance in orientation/awareness O Disturbance in attention O Sleep-wake disturbance O Disturbance in cognition (memory, language, visuospatial perception) O Behavioral Disturbances O Hallucinations (APA, 2013)
9 Delirium O Acute brain failure ( O Less cognitive reserve increases likelihood of its occurrence O Experiencing delirium linked with: O Fatalities O Irreversible cognitive impairment O Contributing to development of dementia O (Inouye et al., 2014)
10 Delirium O Most serious and frequent complication in hospitalized older adults O Delirium is present in O 29-64% of patients older than 65 in general (non- ICU) hospitalized units O 19-82% of older adults in ICU O 8-17% of community dwelling seniors present to the ED with delirium O 40% of nursing home residents present to the ED with delirium (Saczynski & Inouye, 2015)
11 Delirium and Outcomes O 2014 Literature Review by Inouye and colleagues identified the following common outcomes: O Functional decline O Longer LOS O Falls O Nursing Home/Institutional Placement O Death
12 Diagnosing Delirium O Clinical diagnosis O Often missed by providers (Inouye et al., 2014) O Study by Han et al., (2009) found that 76% of delirium cases were missed by ER physicians and that increased the likelihood that this would also be missed by hospitalists on admission
13 Diagnosing Delirium O EEG O Can show diffuse slowing in delirium O Other laboratory studies are of little clinical benefit in confirming delirium O Although, they may assist clinicians in identifying the causative agent of delirium (Saczynski & Inouye, 2015)
14 Diagnosing Delirium O Can use screening instruments O Adamis et al (2010) identified and reviewed 24 scales that were in existence to identify delirium O Found that CAM, DRS, MDAS, and NEECHAM were the most robust in terms of undergoing rigorous psychometric testing
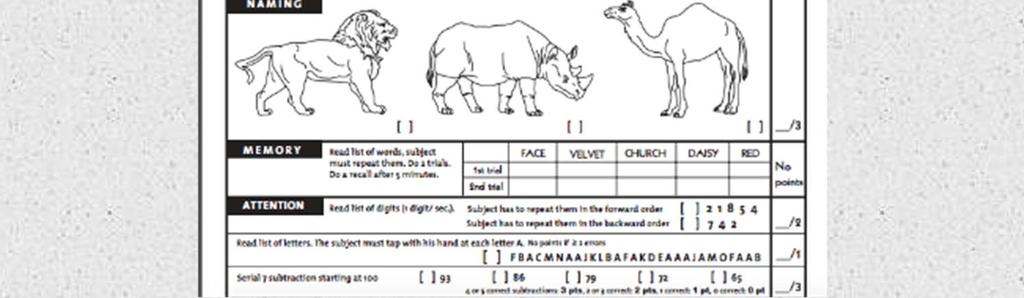
15 Confusion Assessment Method (CAM) O Developed in 1990 by Inouye and colleagues O Based on DSM-III criteria for delirium O Designed to be completed in less than 5 minutes O Has progressed to have a specialized version specific to the ICU (CAM-ICU)
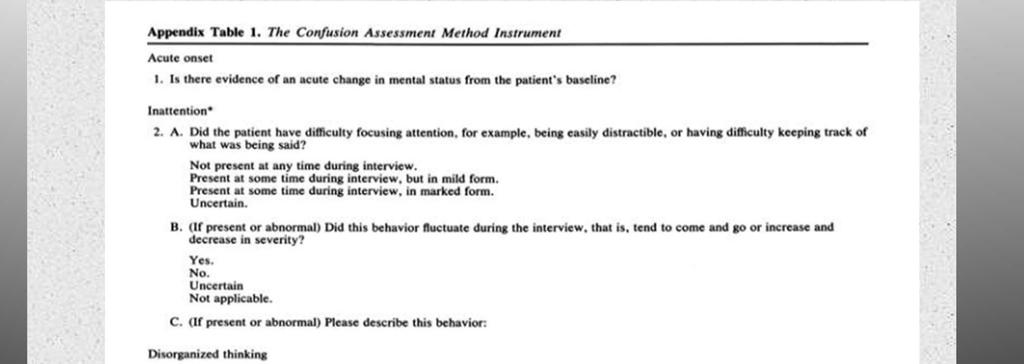

16 CAM
17 CAM
18 CAM O Has been used in about 227 studies as of 2010 O Requires some basic training in order to successfully use the scale O Has been validated for use with strong specificity and sensitivity (89% and 94% respectively) and high interrater reliability O (Han et al., 2010; Saczynski & Inouye, 2015)
19 CAM O Addresses the 4 main domains of delirium O Acute Onset/Fluctuating Course O Inattention O Disorganization O Altered level of consciousness O (Inouye et al., 1990)
20 Why Not Just Use MMSE? O MMSE or Mini-Mental Status Exam test cognitive function O This is not specific to delirium O Scores on MMSE can be low in delirium but may also be low in dementia O MMSE does not help differentiate delirium from other cognitive impairment O (Han et al., 2010)
21 Dementia O Umbrella term to describe a cluster of symptoms with a number of etiological causes O Many subtypes O Interferes with independent functioning O Prevalence increases with age (Kimchi & Lyketsos, 2015)
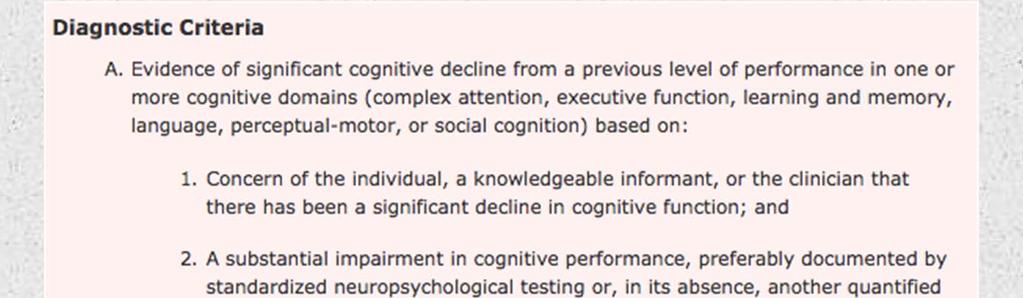
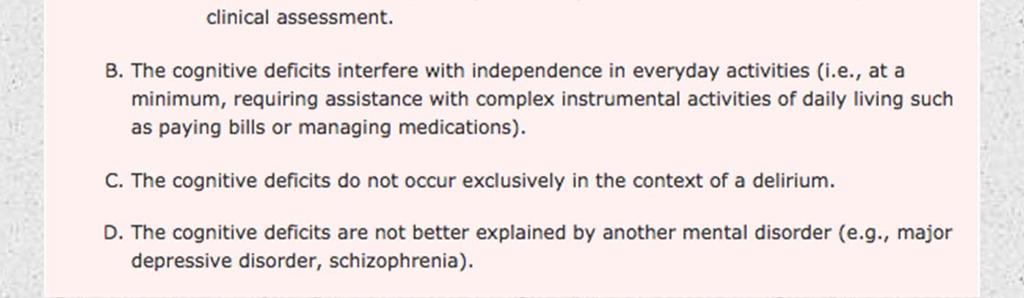
22 Major Neurocognitive Disorder
23 Dementia O 2010 estimates listed 35.6 million individuals with dementia O By 2050 it is predicted that million people worldwide will have dementia O Estimated $203 billion dollars spent on caring for individuals with dementia in 2013 (Kimchi & Lyketsos, 2015)
24 Features of Dementia O Global cognitive impairment O Attention O Executive function O Learning/memory O Language O Motor O Social O Results in impaired functioning that is a deterioration from baseline O Evident in ADLs Lyketsos, 2015) (Kimchi &
25 Psychiatry and Dementia O Often psychiatry is involved due to presence of neuropsychiatric symptoms O Affective O Motivational O Psychosis O Disturbances in basic drives (sleep, sex, eating) O Disinhibited or socially inappropriate behaviors O (Kimchi & Lyketsos, 2015)
26 Diagnosing Dementia O Thorough History O Likely need to involve family/loved ones for collateral O Looking for progressive as opposed to abrupt cognitive decline O Cognitive Assessment O Combined thorough assessment and cognitive assessment can prevent unnecessary referrals to neuropsychologists O Reserve specialists for specific questions or difficult cases


27 MMSE (Folstein, Folstein, & McHugh, 1975)
28 Issues with MMSE O Does not identify mild cognitive impairment O Biases toward well educated O Relies heavily on orientation questions `` (Kimchi & Lysetkos, 2015)

29 MoCA

30 MoCA
31 MoCA O Incorporates clock drawing which tests executive functioning O Tests a larger number of the components of cognition as compared to the MMSE
32 Delirium and Dementia O Having dementia is a risk factor for developing delirium O Having delirium is a risk factor for developing dementia or worsening dementia progression O They can overlap (delirium superimposed on dementia) O (Fong et al., 2015)
33 Differentiating Delirium and Dementia O Often will need collateral information O Look at any previous diagnoses of dementia or a progressive decline O Look at nature of confusion abrupt vs progressive O Waxing and waning pattern O Inattention
34 Treating Delirium O Most important: O TREAT WHATEVER IS CAUSING THE DELIRIUM O Provide supportive care during medical treatment
35 Treating Delirium O Address areas where disturbance could precipitate or exacerbate delirium: O Sleep O Sensory perception O Pain O Medications O Look carefully at medication regimen and try to trim this down and/or use medications that are not going to exacerbate delirium (Kimchi & Lysetkos, 2015)
36 Non Pharmacologic Approaches to Delirium O All members of the health care team need to be actively involved in using nonpharmacologic approaches as these are often continuous O Need to allow for tincture of time O Course of delirium and time it takes until delirium clears despite correction of underlying medical condition is variable
37 Non Pharmacologic Approaches to Delirium O Address sensory impairment O Make sure client has accessory devices to help with sight/hearing O Use translators if needed O Promote use of adequate light (during daytime hours) (Kimchi & Lysetkos, 2015)
38 Non Pharmacologic Approaches to Delirium O Reorientation/redirection O Try to engage family or loved ones of the patient in this process as much as possible O Frequent if not constant supervision for safety and reorientation O Regularly communicate with the client O Even if confused, you can still communicate regularly O This can help to foster ability to redirect (Kimchi & Lysetkos, 2015)
39 Non Pharmacologic Approaches to Delirium O Sleep is essential O Promote sleep O Sleep schedule O Relaxation O Incorporate music/massage O Bright lights during day/low light at night O Engage in activities during day as able to discourage napping O Quiet room at night O Try to avoid waking patient in middle of the night (Kimchi & Lysetkos, 2015)
40 Non Pharmacologic Approaches to Delirium O Keep the patient mobile O Ambulate during the day O Avoid use of loud equipment when patient moves in bed (like bed alarms) as these can further disorient and agitate the patient O Focus on self-care and include the patient in the provision of self care when possible (Kimchi & Lysetkos, 2015)
41 Non Pharmacologic Approaches to Delirium O Be vigilant for any physiological change that could exacerbate delirium and work to correct this through nursing care O Discomfort/pain O Hypoxia O Both of these may be corrected with repositioning for example
42 Delirium and Medications O Must take a careful and critical look at medications O Can use the Beers Criteria as a guide (American Geriatrics Society 2015 Beers Criteria Update Expert Panel, 2015) O Less is more in delirium O Use lowest doses of medications possible O Avoid medications that have action on CNS O Benzodiazpines*--with one exception O Opioids O Anticholinergic medications (Kukreja et al., 2015)
43 Pharmacologic Treatment for Delirium O The actual treatment is to use appropriate pharmacology to address the underlying cause O For example, appropriate antibiotics to treat UTI O Otherwise, pharmacologic agents are employed to manage behavioral disturbances of delirium
44 Pharmacologic Strategies for Delirium O In managing the symptoms of delirium, pharmacology should only be used when the client is demonstrating risk of harm to self or others OR will prevent the client from receiving appropriate medical care O There are no FDA medications available to address delirium O These options should never be used for convenience al., 2015) (Kukreja et
45 Pharmacologic Strategies for Delirium O Antipsychotics are primary intervention as benzodiazepines have been demonstrated to worsen delirium O These should be used for the shortest amount of time O Can be administered IM or PO
46 Pharmacologic Strategies for Delirium O Low dose haloperidol has largest amount of evidence to suggest its efficacy O Second generation antipsychotics have also been used O quetiapine (Seroquel) O risperidone (Risperdal) O olanzapine (Zyprexa) (Kukreja et al., 2015)
47 Antipsychotics and Elderly O Linked to sudden cardiac death O Particularly when they are used in clients with dementia O Use of antipsychotics has been demonstrated to be associated with a 4.5 % death rate in this population O Increased rates of death are linked with first and second generation antipsychotics al., 2010) (Narang et
48 Additional Risks of Antipsychotics O Extrapyramidal Symptoms O Side effects of al antipsychotic agents O Has been linked with causing aspiration O Neurological Concerns O Antipsychotics have been linked with increased risk for stroke (Narang et al., 2010)
49 Addressing Risk of Antipsychotics O Employ non-pharmacologic methods first to try O O O O to avoid use in delirium and dementia Use only when necessary Monitor for EPS Monitor neurological functioning Careful monitoring of cardiac status O Including fluid and electrolyte balance O Monitoring of QTc O EKG monitoring (Narang et al., 2010)
50 Non Pharmacologic Management of Dementia in Acute Care O First need to have an understanding of the level of cognitive impairment (can use one of the brief screening tools discussed earlier) O Provide redirection and orientation O Avoid changing locations frequently O Keep familiar environment as much as possible O Close supervision for safety
51 Non Pharmacologic Strategies for Dementia in Acute Care O Training for nursing staff O Understanding that disruptive behaviors usually are brought about by a stimulus that the individual cannot express O Assess for unmet needs and attempt to meet them (Moyle et al., 2008)
52 Non Pharmacologic Management of Dementia in Acute Care O Sensitivity to communication O Clear and direct O Soft tone O Remain calm O Keep environment quiet when attempting to communicate O Stand still/sit still when communicating O Use preferred name to address the patient O (Moyle et al., 2008)
53 Non Pharmacologic Management of Dementia in Acute Care O Pay attention to the environment O Modify the environment to be calm O Eliminate excess stimulation O Decrease stressors in the environment O Account for any sensory deficits (Moyle et al., 2008)
54 Non Pharmacologic Management of Dementia in Acute Care O Reminiscence therapy principles O Discuss past events with clients O Can use prompts O Can help you to redirect the client O (Woods et al., 2009)
55 Pharmacologic Strategies for Dementia in Acute Care O In an acute care setting, pharmacology would only be employed to manage any behavioral or psychiatric disturbances of dementia O Would manage these primarily with antipsychotics O The same risks and administration concerns exist as when these medications are used in delirium
56 Questions
57 References O O O O O O O O O O O O O O O Adamis, D., Sharma, N., Whelan, P.J.P., & Macdonald, A.J.D. (2009). Delirium scales: a review of current evidence. Aging & Mental Health, 14(5), American Geriatrics Society 2015 Beers Criteria Update Expert Panel. (2015). American Geriatrics Society Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. Journal of the American Geriatrics Society, 63(11), American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. (5th ed.). Arlington, VA: American Psychiatric Publishing. Folstein, M.F., Folstein, S.E., & McHugh, P.R. (1975). Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, Fong, T.G., Davis, D., Growdon, M., Albuquerque, A., & Inouye, S.K. (2015). The interface of dementia and delirium in older persons. Lancet Neurology, 14(8), Han, J.H., Zimmerman, E.E., Cutler, N., Schnelle, J., Morandi, A., Dittus, R.S., Storrow, A.B., & Ely, E.W. (2009). Delirium in older emergency department patients: recognition, risk factors, and psychomotor subtypes. Academy of Emergency Medicine, 16(3), Inouye, S.K., van Dyck, C.H., Alessia, C.A., Balkin, S., Siegal, A.P., & Horowitz, R.I. (1990). Clarifying confusion: the confusion assessment method: a new method for the detection of delirium. Annals of Internal Medicine, 113(12), Inouye, S.K., Westendorp, R., & Saczynski, J.S. (2014). Delirium in elderly people. Lancet, 383(9920), Kimchi, E.Z. & Lyketsos, C.G. (2015). Dementia and mild neurocognitive disorders. In Steffens, C., Blazer, D.G., Thakur, M.E. (Eds.). The American Psychiatric Publishing Textbook of Geriatric Psychiatry, (5th ed). Arlington, VA: American Psychiatric Publishing. Kukreja, D., Gunther, U., & Popp, J. (2015). Delirium in the elderly: current problems with increasing geriatric age. Indian Journal of Medical Research, 142, Moyle, W., Olorenshaw, R., Wallis, M., & Borbasi, S. (2008). Best practice for the management of older people with dementia in the acute care setting: a review of the literature. International Journal of Older People Nursing, 3(2), Narang, P., El-Refai, M., Parlapalli, R., Danilov, L., Manda, S., Kaur, G., & Lippman, S. (2010). Antipsychotic drugs; sudden cardiac death among elderly patients. Psychiatry, 7(10), Nasreddine, Z. (2017). The Montreal Cognitive Assessment. Retrieved from Saczynski, J.S. & Inouye, S.K. (2015). Delirium In Steffens, C., Blazer, D.G., Thakur, M.E. (Eds.). The American Psychiatric Publishing Textbook of Geriatric Psychiatry, (5th ed). Arlington, VA: American Psychiatric Publishing. Woods, B., Specter, A.E., Jones, C.A., Orrell, M.,& Davies, S.P. (2009). Reminiscence therapy for dementia. Cochrane Database of Systematic Reviews, 2, 1-34.
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
nicheprogram.org 16th Annual NICHE Conference Forging New Paths and Partnerships 1
 Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
Improving Patient Outcomes in Geriatric Post-Operative Orthopedic Patients: Translating Research into Practice Tripping into The CAM Presented by: Diana LaBumbard, RN, MSN, ACNP/GNP-BC, CWOCN Denise Williams,
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Delirium Pilot Project
 CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
CCU Nurses: Delirium Pilot Project Our unit has been selected to develop and implement a delirium assessment and intervention program. We are beginning Phase 1 with education and assessing for our baseline
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
Psychotropic Medication. Including Role of Gradual Dose Reductions
 Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Psychotropic Medication Including Role of Gradual Dose Reductions What are they? The phrase psychotropic drugs is a technical term for psychiatric medicines that alter chemical levels in the brain which
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Cognitive Status. Read each question below to the patient. Score one point for each correct response.
 Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
Diagnosis of dementia or delirium Cognitive Status Six Item Screener Read to the patient: I have a few questions I would like to ask you. First, I am going to name three objects. After I have said all
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Care of Patient with Delirium
 Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Care of Patient with Delirium Introduction Delirium is an alteration in consciousness involving confusion and other changes in cognitive ability that has a brief duration. 1 Patients specifically at risk
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium assessment and management. Dr Kim Jeffs Northern Health
 Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
Delirium assessment and management Dr Kim Jeffs Northern Health What do you need to know? Epidemiology How big is the problem? Who is at risk? Assessment Tools for diagnosis Prevention Evidence base Management
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Case Presentation. Cognition: changes with Normal Aging? Synonyms
 Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Case Presentation 78 yr old new patient presenting for new PCP after discharge from hospital stay Discharged 3 days ago Summary : admitted with new atrial fibrillation, with history of DM, CHF. In hospital,
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias. Aaron H. Kaufman, MD
 Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, MD Psychiatric and Behavioral Symptoms in Alzheimer s and Other Dementias Aaron H. Kaufman, M.D. Health Sciences
Delirium in Older Persons: An Investigative Journey
 Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
Delirium in Older Persons: An Investigative Journey Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Disentangling Delirium and Dementia
 Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Disentangling Delirium and Dementia Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy Family Chair Director, Aging
Interprofessional Webinar Series
 Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Management of the Acutely Agitated Long Term Care Patient
 Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
Management of the Acutely Agitated Long Term Care Patient 80 60 Graying of the Population US Population Over Age 65 Millions of Persons 40 20 0 1900 1920 1940 1960 1980 1990 2010 2030 Year Defining Dementia
DELIRIUM. Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine
 DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
DELIRIUM Sabitha Rajan, MD, MSc, FHM Scott &White Healthcare Texas A&M Health Science Center School of Medicine Disclosure Milliman Care Guidelines - Editor Objectives Define delirium Epidemiology Diagnose
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
MN/OH Delirium Collaborative. Place picture here
 MN/OH Delirium Collaborative Place picture here November 16, 2017 Housekeeping Introductions: MHA- Naira Polonsky OHA- Rosalie Weakland OHA- Jim Guliano In December 2015, the Minnesota and Ohio HENS began
MN/OH Delirium Collaborative Place picture here November 16, 2017 Housekeeping Introductions: MHA- Naira Polonsky OHA- Rosalie Weakland OHA- Jim Guliano In December 2015, the Minnesota and Ohio HENS began
Recognition and Management of Behavioral Disturbances in Dementia
 Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Recognition and Management of Behavioral Disturbances in Dementia Danielle Hansen, DO, MS (Med Ed), MHSA INTRODUCTION 80% 90% of patients with dementia develop at least one behavioral disturbances or psychotic
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
David A Scott Lis Evered. Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne
 David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
David A Scott Lis Evered Department of Anaesthesia and Acute Pain Medicine St Vincent s Hospital, Melbourne University of Melbourne This talk will include live polling so please be sure to have the meeting
Delirium in Cancer: Psychopharmacologic Management
 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York Delirium in Patients with Cancer
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Behavioral Interventions
 Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
Behavioral Interventions Linda K. Shumaker, R.N.-BC, MA Pennsylvania Behavioral Health and Aging Coalition Behavioral Management is the key in taking care of anyone with a Dementia! Mental Health Issues
NEUROPSYCHOMETRIC TESTS
 NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
NEUROPSYCHOMETRIC TESTS CAMCOG It is the Cognitive section of Cambridge Examination for Mental Disorders of the Elderly (CAMDEX) The measure assesses orientation, language, memory, praxis, attention, abstract
Delirium Screening: The next nurse sensitive indicator?
 Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium Screening: The next nurse sensitive indicator? Sharon Gunn, MSN, MA, RN, ACNS-BC, CCRN Clinical Nurse Specialist Critical Care Baylor University Medical Center Dallas, TX Objectives Recognize
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
5 older patients become. What is delirium? (Acute confusional state) Where We ve Been and
 Where We ve Been and") Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Update on Delirium: Where We ve Been and Where We re Going Sharon K. Inouye, M.D., M.P.H. M PH Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley F. Levy
Recognizing Dementia can be Tricky
 Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Dementia Abstract Recognizing Dementia can be Tricky Dementia is characterized by multiple cognitive impairments that cause significant functional decline. Based on this brief definition, the initial expectation
Objectives. Antipsychotics 7/25/2016. LeadingAge Florida 53rd Annual Convention & Exposition
 Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Reducing the Use of Antipsychotics in Long Term Care Communities Alan W. Obringer RPh, CPh, CGP Executive Director Senior Care Pharmacy Objectives Recognize the clinical evidence for the need to change
Delirium and Care Giving
 Delirium and Care Giving Marianne McCarthy, PhD, RN Advanced Practice Nurse Sun Health Geriatric Fellowship Program Associate Professor Arizona State University Presentation Questions What happens when
Delirium and Care Giving Marianne McCarthy, PhD, RN Advanced Practice Nurse Sun Health Geriatric Fellowship Program Associate Professor Arizona State University Presentation Questions What happens when
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Strategies to Recognize & B.E.A.T. Delirium. Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student
 Strategies to Recognize & B.E.A.T. Delirium Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student The very first requirement in a hospital is that it should
Strategies to Recognize & B.E.A.T. Delirium Amy E. Seitz Cooley, MS, RN, ACNS-BC Clinical Nurse Specialist York College of Pennsylvania DNP Student The very first requirement in a hospital is that it should
Management of Agitation in Dementia. Kimberly Triplett Ferguson, MS4
 Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
Management of Agitation in Dementia Kimberly Triplett Ferguson, MS4 Objectives 1. Review recommended evaluation of agitated patients with dementia. 2. Discuss evidence concerning nonpharmacologic management.
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
How to prevent delirium in nursing home. Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium
 How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
How to prevent delirium in nursing home Dr. Sophie ALLEPAERTS Geriatric department CHU-Liège Belgium 1 CONFLICT OF INTEREST DISCLOSURE I have no potential conflict of interest to report 2 Outline 1. Introduction
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Cognitive Assessment 4/29/2015. Learning Objectives To be able to:
 Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Supporting the Desire to Age in Place: Important Considerations for the Aging Population AGENDA 8:45 9:00 AM Geriatric Principles Robert L. Kane, MD *9:00 9:55 AM Cognitive Assessments Ed Ratner, MD 10:00
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Transitioning to Adult-Gerontology APRN Education: Slide Library
 Transitioning to Adult-Gerontology APRN Education: Slide Library APRN Assessment and Management of Older Adults with Delirium Authors: Lois Evans, PhD, RN, FAAN Pamela Z. Cacchione, PhD, APRN, GNP, BC
Transitioning to Adult-Gerontology APRN Education: Slide Library APRN Assessment and Management of Older Adults with Delirium Authors: Lois Evans, PhD, RN, FAAN Pamela Z. Cacchione, PhD, APRN, GNP, BC
Delirium, Depression and Dementia
 Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
Delirium, Depression and Dementia Martha Watson, MS, APRN, GCNS Some material included in this presentation is adapted from: NICHE (2009). Geriatric Resource Nurse Core Curriculum [Power Point presentation].
How to prevent delirium in the Emergency Room. Nice September 21, 2017 Steffen Schlee/ Katrin Singer
 How to prevent delirium in the Emergency Room Nice September 21, 2017 Steffen Schlee/ Katrin Singer CONFLICT OF INTEREST DISCLOSURE K. Singler and St. Schlee have no potential conflict of interest to report.
How to prevent delirium in the Emergency Room Nice September 21, 2017 Steffen Schlee/ Katrin Singer CONFLICT OF INTEREST DISCLOSURE K. Singler and St. Schlee have no potential conflict of interest to report.
Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
 Shu-Ming Chen RN, PhD, Assistant Professor, College of Nursing, Fooyin University, Kaohsiung, Taiwan, R. O.C. 29th International Nursing Research Congress Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
Shu-Ming Chen RN, PhD, Assistant Professor, College of Nursing, Fooyin University, Kaohsiung, Taiwan, R. O.C. 29th International Nursing Research Congress Monday, 23 July 2018: 8:30 AM-9:45 AM STTI Australia
Delirium, The Geriatrics Ward Challenge
 American Journal of Pharmacology and Pharmacotherapeutics Research Article Delirium, The Geriatrics Ward Challenge Pardo Pastor Ricardo Fernandes 1, Rafaela Veríssimo 2 and António Agripino Oliveira 3*
American Journal of Pharmacology and Pharmacotherapeutics Research Article Delirium, The Geriatrics Ward Challenge Pardo Pastor Ricardo Fernandes 1, Rafaela Veríssimo 2 and António Agripino Oliveira 3*
Geriatric Screening in Five Minutes or Less: Skills Stations
 Geriatric Screening in Five Minutes or Less: Skills Stations Charlotte A. Paolini, D. O., CMD June 14, 2014 (Special thanks to Sarah Hallen, M.D., for allowing the use of her materials for this presentation.)
Geriatric Screening in Five Minutes or Less: Skills Stations Charlotte A. Paolini, D. O., CMD June 14, 2014 (Special thanks to Sarah Hallen, M.D., for allowing the use of her materials for this presentation.)
Geriatric Grand Rounds
 Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Geriatric Grand Rounds Prevalence and Risk Factors of Delirium in Older Patients Admitted to a Community Based Acute Care Hospital Tuesday, October 27, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose
Dementia and Fall Geriatric Interprofessional Training. Wael Hamade, MD, FAAFP
 Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
Dementia and Fall Geriatric Interprofessional Training Wael Hamade, MD, FAAFP Prevalence of Dementia Age range 65-74 5% % affected 75-84 15-25% 85 and older 36-50% 5.4 Million American have AD Dementia
J Donna Sullivan, LCSW, C-ASWCM. AgeWiseConnections
 J Donna Sullivan, LCSW, C-ASWCM AgeWiseConnections Medical terminology Assessment procedures Medication & Medication Mismanagement Caregiver Stress Family Health Care Decision Act Resources Dementia vs.
J Donna Sullivan, LCSW, C-ASWCM AgeWiseConnections Medical terminology Assessment procedures Medication & Medication Mismanagement Caregiver Stress Family Health Care Decision Act Resources Dementia vs.