Acute Respiratory Failure
|
|
|
- Suzan Jenkins
- 5 years ago
- Views:
Transcription
1 Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine
2 Acute Respiratory Failure Recognition Etiology Airway assessment and management RSI/induction agents Alternate devices
3 Dx Acute Resp Failure Difficult to define but I know it when I see it Very subjective diagnosis
4 Signs and Symptoms subjective feeling of shortness of breath tachypnea using accessory muscles of respiration paradoxical abdominal movements with breathing inability to talk w/o gasping for air cyanosis (mucus membranes, nail beds) skin mottling decreased mental status unstable vital signs abnormal lung sounds cough and purulent sputum
5 Important Signs and Symptoms tachypnea using accessory muscles of respiration paradoxical abdominal movements with breathing inability to talk w/o gasping for air
6 Stages of ABG s ph pco 2 po 2 Stage normal Stage Stage Stage Stage
7 Stages of ABG s ph pco 2 po 2 RR Stage Stage Stage Stage Stage
8 ABG Stages in COPD ph pco 2 po 2 Stage baseline Stage Stage Stage Stage
9 Etiology Resp Failure Lung Parenchymal Disease COPD Pneumonia CHF Sepsis Hypoventilation Drug overdose Head injury Neuromuscular disease Pulmonary Embolism
10 Pulmonary Pathophysiology CO 2 diffuses across the alveolar membrane 200 x better than O 2 Hypoxia with normal po 2 is always lung parenchymal disease Hypoxia with an elevated pco 2 could be primary hypoventilation or could be severe lung parenchymal disease Hypoxic resp failure vs Hypercapnic resp failure
11 A-a gradient Alveolar to arterial oxygen gradient A is estimated from a formula a is from the ABG
12 A is estimated from the following formula: A = FiO 2 (Pb - PH 2 O) - pco 2 /RQ A = FiO 2 (760-47) - pco 2 /RQ A = FiO 2 (713) - pco 2 /RQ A = FiO 2 (700) - pco 2 A-a gradient = FiO 2 (700) - pco 2 po 2
13 In the normal individual breathing room air with a normal po 2 of 100 and a pco 2 of 40 A = 0.21(700) - 40 A = (147) - 40 A = 107 A-a gradient = = 7 The normal A-a gradient is < 10
14 FORMULAS TO REMEMBER A-a on room air = pco 2 - po 2 A-a on oxygen = (FiO 2 x 700) - pco 2 - po 2
15 Resp Failure Differential Diagnosis A-a inc FiO 2 Etiology hypoventilation nl PaO 2 inc Drugs, head injury dead space inc PaO 2 inc COPD shunt fraction inc PaO 2 not inc pneumonia, CHF, PE
16 Resp Failure Differential Diagnosis A-a inc FiO 2 Etiology hypoventilation nl PaO 2 inc Drugs, head injury dead space inc PaO 2 inc COPD shunt fraction inc PaO 2 not inc pneumonia, CHF, PE Really only applies at high FiO2 levels > 60 % 100 % oxygenation FiO2 challenge and calculate the change in the pf ratio (po2/fio2)
17 Pulmonary Embolism Yes, in autopsy series there are some missed PEs In the real world, common things happen commonly If your patients presents with a good explanation for their resp failure there is no reason to add PE to the list
18 Pulmonary Embolism D-dimer only helpful when negative negative means no PE positive means nothing a very high D-dimer still means nothing Not all D-dimers are created equal know which one your hospital uses Use a prediction score Wells score
19 Wells Criteria Clinical symptoms of DVT (leg swelling, pain with palpation) 3.0 Other diagnosis less likely than pulmonary embolism 3.0 Heart rate > Immobilization ( 3 days) or surgery in the previous four weeks 1.5 Previous DVT/PE 1.5 Hemoptysis 1.0 Malignancy 1.0 Probability Score High >6.0 Moderate 2.0 to 6.0 Low <2.0
20 Data needed to make decisions History Acute HPI Chronic Past Med Hx Exam Vital signs General assessment How do they look Lung sounds ABG CXR
21 In shock? Do they need mechanical support Hypercapnic with complications? Hypotension,hypoxia, widened QRS complex, etc. Hypoxia not resolved with O2? Look Bad? Increased work of breathing Decreased level of consciousness
22 What kind of mechanical support? Non-Invasive Ventilation (NIV) BiPap or CPAP Endotracheal intubation
23 Indications for NIV Acute Respiratory Failure intact mental status airway protected absence facial trauma patient will tolerate success rate 25 %
24 Non-Invasive Ventilation Takes patience to initiate Try several different masks to find right fit Start with low settings and work up to full settings and mask fitting May need some sedation versed
25 How long to try After get patient settled on NIV minutes Should look better in one hour If not better consider intubation
26 Indications for intubation Acute Respiratory Failure failure of NIV decreased mental status unprotected airway shock emergencies need high pressures
27 Transport Decisions Complex question Equipment and personnel available Distance of transport
28 Intubation and Sedation Please keep your patient comfortable post intubation Sedation and analgesia If hypotension develops then More fluid Early pressors Avoid repeat doses of neuromuscular blockers for transport
29 Medications for Transport Sedation Analgesia Isotonic fluids Vasopressor Paralytics rarely needed for transport
30 Airway Management Endotracheal Intubation is by far and away the best, safest and preferred technique to management the acute respiratory failure patients airway
31 Novice Intubation is perceived as scary Reality is that is not that hard a skill to master Frist resource for training should be on a dummy one hour once in a lifetime sufficient In OR do some elective intubations repeat that every 1-2 years
32 RAPID SEQUENCE INTUBATION RSI is the standard of care in emergency airway management for intubations not anticipated to be difficult simultaneous administration of a sedative and a neuromuscular blocking agent to render a patient rapidly unconscious and flaccid in order to facilitate emergent endotracheal intubation and to minimize the risk of aspiration. Multiple studies confirm the high-success rate of RSI using the combination of a sedative and a paralytic drug
33 Induction Agents midazolam (Versed) Propofol Fentanyl Ketamine Etomidate Neosphyenine Fluids
34 midazolam (Versed) Dose 2-4 mg (induction dose is listed as mg/kg) Onset 1-5 minutes Duration 5-30 minutes Amnesic effect
35 Propofol 60 kg 100 kg Dose (1.5-3 mg/kg) 50 mg 100 mg Onset seconds Duration minutes 5-10 minutes Reduces airway resistance, decreases ICP, good antiepileptic Does vasodilate cause hypotension
36 Fentanyl Personal experience more than guidelines 60 kg 100 kg Dose 0.5 mcg/kg 60 mcg 100 mcg Onset minutes 1 Duration minutes 5-15
37 Rocuronium 60 kg 100 kg Dose 0.6 mg/kg 35 mg 60 mg Onset 1-2 minutes (typically faster) Duration 5-15 minutes (typically quicker) Nondepolarizing agent
38 Succinylcholine 60 kg 100 kg Dose 1.5 mg/kg 90 mg 150 mg Onset seconds Duration minutes 6-10 Depolarizing agent Hyperkalemic cardiac arrest (Are defined risks groups but can occur in anyone) No longer recommended in any patients
39 Etomidate 60 kg 100 kg Dose 0.3 mg/kg 20 mg 30 mg Onset minute Duration 3-5 minutes Causes less hypotension Adrenal insufficiency, inc mortality in septic patients, no longer used in the ICU
40 Ketamine 60 kg 100 kg Dose 1-2 mg/kg mg mg Onset 1 minutes Duration 5-15 minutes Less hypotension May increase ICP (evidence weak) Can be used for awake intubations (preserves resp drive) Reemergence phenomenon concerning
41 Phenylephrine Neosynephrine IV bolus dosing 100 mcg q 5 minutes IV infusion dose 0-4 mcg/kg/min mcg/minute Hypotension is so common Neo should be part of your induction agent medical list
42 Most Patients are Dry Have NS hanging and do not hesitate to give 1-3 liters Have not been eating well Induction agents will vasodilate Even the CHF patient may be intravascular dry and need some fluid
43 What do I do Versed 4 mg IV given while I set up to intubate mcg fentanyl and mg of propofol Start to bag mask ventilate as they fall asleep (eyelash test) Look, if fail then more sedation +/- rocuronium
44 What do I do (2) 3 attempts with laryngoscope Watch sat s and heart rate abort attempt and bag when pulse starts to fall Glidescope Consider a intubating stylet Cricothyroidotomy (kit)
45 To RSI or Not to RSI Most fellowship trained ED MDs always RSI I will usually try once without paralytic and use it if I think I will get a better view on the second attempt More likely to use RSI if no concerns after an LEMON airway assessment, TBI, overdose patient, full stomach
46 Intubation Failure Rates Difficult intubation rate quoted as 30 % more than one attempt Unsuccessful intubation rate 10 %
47 Prediction of the Difficult Airway LEMON approach Look externally Evaluate rule Mallampati score Obstruction/Obesity Neck mobility
48 Look externally Clinician s general impression abnormal facies or body habitus unusual anatomy facial trauma Specific but not sensitive If it looks like a difficult airway then it most likely will be Absence of external signs of a difficult airway does not predict success
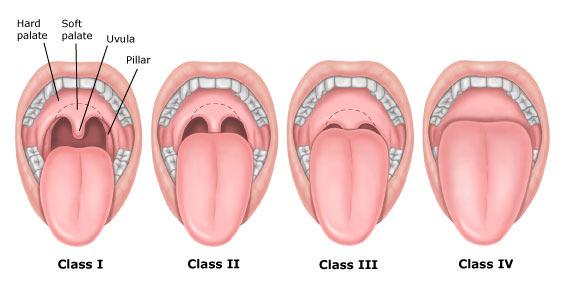
49 3-3-2 Rule A. Extent of mouth opening B. Size of the mandible C. Distance between mentum and hyoid bone
50 A. Extent of mouth opening Patient should be able to fit three of their own fingers between the incisors
51
52 B. Size of the mandible Patient should be able to place three of their own fingers along the floor of the mandible between the mentum and the neck/mandible junction
53
54 C. Distance between mentum and hyoid bone Patient should be able to place 2 of their own fingers in the superior laryngeal notch If larynx is too high (anterior) hard to see

55
56 Mallampati Predicts the view during laryngoscopy based on the view looking into the patients open mouth Class I or II easy laryngoscopy Class III difficult Class IV extreme difficultly
57
58 M score in the ED Often patients unable to cooperate Open the mouth with tongue blade of laryngoscope blade and try to get the best view possible
59 O: Obstruction/Obesity Upper airway obstruction (rare) mass, foreign body, infection Redundant tissues obese patient can make views difficult, may want a bigger laryngoscope blade
60 N: Neck Mobility Ideal position for intubation sniffing position Flexing neck forward and elevating the head Trauma patients with concern neck injury require in-line stabilization which can limit views Medical conditions like RA, ankylosing spondylitis, DJD in the elderly
61 How to use LEMON Do as much assessment of the airway as possible prior to intubation If factors present that predict difficult intubation then plan ahead gather special supplies alert personnel Proceed with intubation +/- paralysis
62 Alternative devices Glidescope Awake intubation/nasal intubation Extraglottic airway devices LMA/Intubating LMA Combitube, Kingair, others Intubation over a bronchoscope Surgical airway (cric/trach)
63 Glidescope Plastic lighted laryngoscope with a camera

64


65

66
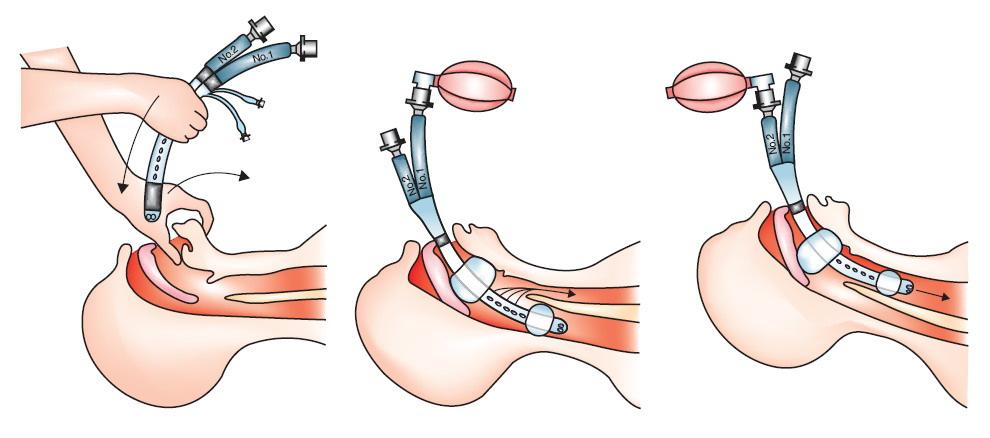
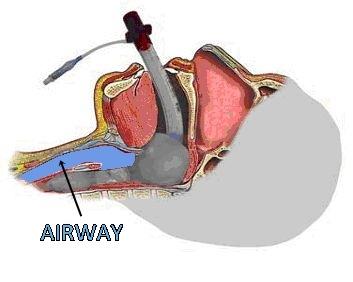
67 Extraglottic Airway Devices LMA Combitube Kingair
68 LMA Laryngeal Mask Airway Video regarding use and placement NEJM Nov 4, 2013 e26 Not as easy to place as pictures and videos imply Should practice on dummy or in OR

69
70

71
72

73
74
75
76 Questions
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Kelowna June 2011 Airway Assessment and Management. Golden, BC
 Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
MAKING RSI SAFER. Nick Taylor ETU THK 2015
 MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
A Successful RSI Program
 RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Pearls and Pitfalls of Rapid Sequence Intubation
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Airway 2015 Updates in Emergency Airway Management
 Airway 2015 Updates in Emergency Airway Management Gerry Maloney, DO, FACOEP Associate Medical Director, Metro Life Flight Attending Physician, Emergency Medicine, CWRU/MetroHealth Medical Center None
Airway 2015 Updates in Emergency Airway Management Gerry Maloney, DO, FACOEP Associate Medical Director, Metro Life Flight Attending Physician, Emergency Medicine, CWRU/MetroHealth Medical Center None
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
When I started. 10/27/2009. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine
 When I started. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine When I started. When I started. When I started. When I started. How To Make A Fertile
When I started. Gerald Wydro, MD Clinical Associate Professor Emergency Medicine Temple University School of Medicine When I started. When I started. When I started. When I started. How To Make A Fertile
Procedural Sedation in the Rural ER
 Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill
 Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
EMS Subspecialty Certification Review Course. Learning Objectives
 EMS Subspecialty Certification Review Course 1.1.2 Airway Compromise / Respiratory Failure 1.1.2.1 Devices for securing airway 1.1.2.2 Portable ventilator management 1.1.2.3 Pros and cons of drug assisted
EMS Subspecialty Certification Review Course 1.1.2 Airway Compromise / Respiratory Failure 1.1.2.1 Devices for securing airway 1.1.2.2 Portable ventilator management 1.1.2.3 Pros and cons of drug assisted
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
POST TEST: PROCEDURAL SEDATION
 POST TEST: PROCEDURAL SEDATION Name: Date: Instructions: Complete the Post-Test (an 85% is required to pass). If there are areas that you are unsure of, please review the relevant portions of the learning
POST TEST: PROCEDURAL SEDATION Name: Date: Instructions: Complete the Post-Test (an 85% is required to pass). If there are areas that you are unsure of, please review the relevant portions of the learning
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
PAEDIATRIC ANAESTHETIC EMERGENCIES PART I. Dr James Cockcroft, South West School of Anaesthesia. Dr Sarah Rawlinson, Derriford Hospital, Plymouth, UK
 PAEDIATRIC ANAESTHETIC EMERGENCIES PART I Original Article by: Dr Claire Todd, South West School of Anaesthesia Dr James Cockcroft, South West School of Anaesthesia Dr Sarah Rawlinson, Derriford Hospital,
PAEDIATRIC ANAESTHETIC EMERGENCIES PART I Original Article by: Dr Claire Todd, South West School of Anaesthesia Dr James Cockcroft, South West School of Anaesthesia Dr Sarah Rawlinson, Derriford Hospital,
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Indications for Respiratory Assistance. Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer
 Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT AVOIDING THE CRASH 1: DON T INTUBATE, OPTIMIZE PRE-AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Intubation sedation intubation
 Intubation sedation Mar 29, 2017. When a paralytic agent is used for intubation without sedation, the patient may be fully aware of his or. Oct 11, 2016. This post will review sedation and analgesia regimens
Intubation sedation Mar 29, 2017. When a paralytic agent is used for intubation without sedation, the patient may be fully aware of his or. Oct 11, 2016. This post will review sedation and analgesia regimens
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Tracheal Intubation in ICU: Life saving or life threatening?
 Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
DON T PRACTICE UNTIL YOU GET IT RIGHT. PRACTICE UNTIL YOU CAN T GET IT WRONG.
 ADVANCED AIRWAY MANAGEMENT AND THE DIFFICULT AIRWAY DON T PRACTICE UNTIL YOU GET IT RIGHT. PRACTICE UNTIL YOU CAN T GET IT WRONG. The Decision to Intubate n Can the patient protect their airway? n Can
ADVANCED AIRWAY MANAGEMENT AND THE DIFFICULT AIRWAY DON T PRACTICE UNTIL YOU GET IT RIGHT. PRACTICE UNTIL YOU CAN T GET IT WRONG. The Decision to Intubate n Can the patient protect their airway? n Can
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
VANDERBILT UNIVERSITY MEDICAL CENTER DIVISION OF ANESTHESIOLOGY CRITICAL CARE MEDICINE AIRWAY MANAGEMENT
 These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
Polytrauma. Same stuff-different day! 9/14/2012. Managing the difficult airway in Multi-Systems Trauma. Jerry J Ryman CRT
 Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
The Pediatric Airway. Andrew Wackett, MD
 The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital
 Difficult & Failed Intubation Queen Charlotte s Hospital") (ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
(ix) Difficult & Failed Intubation Queen Charlotte s Hospital Pre-operative Assessment Clinical assessment of airway and risk of difficult intubation: (can be performed in a matter of seconds): 1. Mouth
DESCRIPTIONS FOR MED 3 ROTATIONS Critical Care A2 ICU
 Critical Care A2 ICU A. Neurological 1. Delirium Discuss the differential diagnosis and appropriate investigation for delirium. Provide non-pharmological and pharmological treatment options for delirium.
Critical Care A2 ICU A. Neurological 1. Delirium Discuss the differential diagnosis and appropriate investigation for delirium. Provide non-pharmological and pharmological treatment options for delirium.
CASE REPORT FORM (v )
") INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Redundancy of safety (primary and backup chute) Planned stepwise approach to deploy 1 ary chute Simple, fast, easy backup chute deployment Attention
 Planned stepwise approach to deploy 1 ary chute Simple, fast, easy backup chute deployment Attention") Rapid Sequence Intubation John Bradley, MD Metropolitan Hospital May 30, 2012 1 Lessons from Skydiving Levitan RM. Patient safety in emergency airway management and rapid sequence intubation: metaphorical
Rapid Sequence Intubation John Bradley, MD Metropolitan Hospital May 30, 2012 1 Lessons from Skydiving Levitan RM. Patient safety in emergency airway management and rapid sequence intubation: metaphorical
Problem Based Learning. Problem. Based Learning
 Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Management of the Airway
 Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Management of the Airway Kristen Bridges, M.D. Kings County Hospital Center November 12 th 2015 Case Presentation 64F PMHx CHF EF 5-10%, NYHF III-IV, atrial fibrillation/la thrombus, CVA x2, DM, HTN Home
Jason Zurba BSc RRT Supervisor Royal Columbian Hospital
 Jason Zurba BSc RRT Supervisor Royal Columbian Hospital Outline Why we started looking at this What our own data has shown us What the literature tells us about intubation What we have changed How this
Jason Zurba BSc RRT Supervisor Royal Columbian Hospital Outline Why we started looking at this What our own data has shown us What the literature tells us about intubation What we have changed How this
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur