MAKING RSI SAFER. Nick Taylor ETU THK 2015
|
|
|
- Nancy Gaines
- 5 years ago
- Views:
Transcription
1 MAKING RSI SAFER Nick Taylor ETU THK 2015
2 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY
3 PART 1 : AIRWAY ASSESSMENT AND PLAN
4
5 LEMON: AIRWAY ASSESS AND PLAN Look Evaluate Mallampatti Obstructions Neck Validated assessment technique to help predict poor laryngoscopy view. Emerg Med J 2005;22:99 102
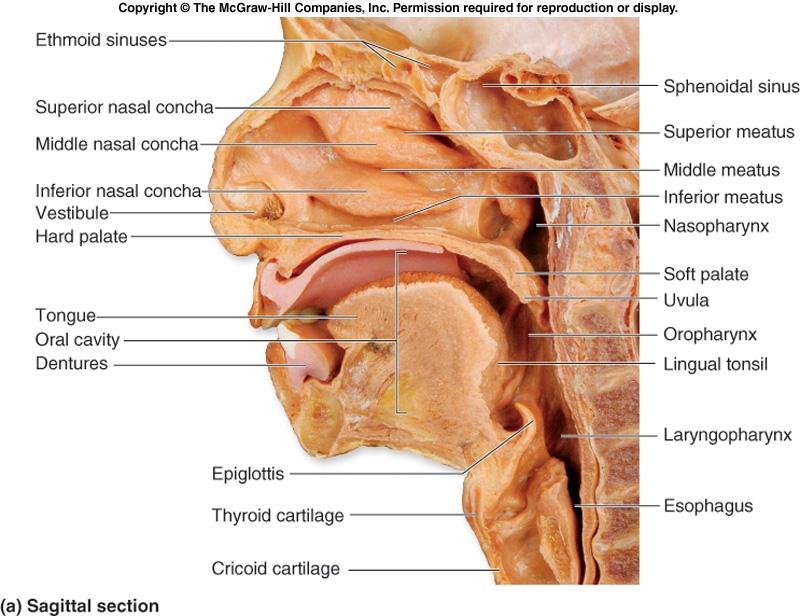
6 LOOK externally: Large incisors, facial hair, facial trauma, large tongue EVALUATE Interincisor distance (3 fingers) Hyomental distance (3 fingers) Floor of mouth to thyroid notch (2 patients own fingers)
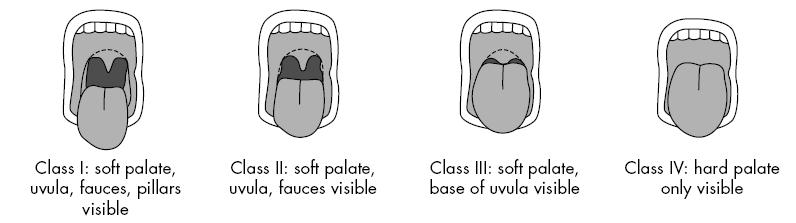
7 MALLAMPATTI
8 Obstructions: Masses, blood, teeth Stridor Swallowing difficulty OBSTRUCTIONS AND NECK Neck mobility Especially Hard collar, Ank spond, RA etc
9 OPTIMISE POSITIONING EARLOBE AT LEVEL STERNUM THIS MAY REQUIRE PILLOWS, TOWELS, RAMPING
10 OPEN AIRWAY Naso pharygeal airways Oro pharyngeal airways Occasionally x 3
11 VERBALLY EXPRESS YOUR PLAN BASED ON ASSESSMENT Should include primary and back up plan Pre allocate roles for back up if expected difficult
12
13 SUMMARY OF AIRWAY Formally assess each time Optimise position and adjuncts Verbally express primary and backup plan Use a checklist
14 PART 2 PREOXYGENATION
15
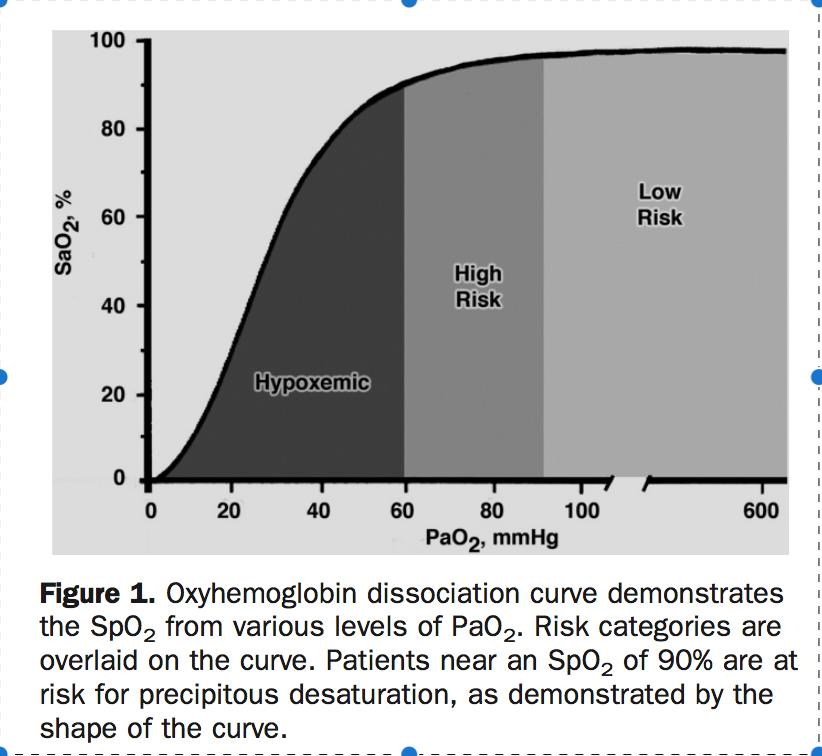
16 WHY PREOXYGENATE Extends safe apnoea time by 1. Get sats as high as possible 2. Denitrogenate lungs 3. Denitrogenate and oxygenate blood

17 STEP 1: DELIVER HIGH FI02 Self inflating bag and mask has a one way valve
18 RESERVOIR FACE MASK NRB only gives 60-70% FiO2 Turn up flow rate to beyond 15L/min Sit up 30 deg or incline bed 3-5 minutes or 8 VC breaths
19 STEP 2: ADDING PEEP Multiple studies show apnoea time extended and haemodynamics not affected Use NIV (CPAP) or PEEP valve Should consider if sats <95 after Pre 02 Leave on until laryngoscope
20 STEP 3: APNOEIC OXYGENATION Standard nasal prongs or high flow Use standard prongs at 15L/min Leave on during whole process High flow can extend out apnoea time to up to 20min
21 STEP4: CONSIDER BAGGING When Pre 02 has not achieved >95% When hypercarbia is dangerous Raised ICP Sodium Channel blocker overdose
22 STEP 5: CONSIDER DSI Ketamine 0.5mg/kg to facilitate NIV Especially in agitated patients We have done >10 minutes in severely ill patients with very good effect
23 SUMMARY OF PRE 02 Goal should be sats>95% Use: High flow mask 02 and nasal cannula in all Consider: Add PEEP or NIV Add bagging Add DSI
24 PART 3: HAEMODYNAMIC OPTIMIZATION
25 IDENTIFY THE AT RISK PATIENT Most/All Induction drugs are vasodilators and/or negative inotropes Hypotension during RSI can be catastrophic
26 HAEMODYNAMIC PREPARATION 2 Working large Cannulae All patients should be fluid loaded unless truly contraindicated (0.5-1L NS) Consider bolus vasoconstrictor or infusion if at risk (especially distributive shock, raised ICP)
27 DRUG CHOICE Propofol: Vasodilator, negative inotrope Hypotension in almost every patient Excellent drug for sedation Not used as much for induction
28 DRUG CHOICE Thiopentone: Vasodilator, negative inotrope Less hypotension than propofol Judicious dose important neuroprotective effect less important than BP maintenance
29 DRUG CHOICE Ketamine: Sympathomimetic Will still be a negative inotrope in at risk patient Excellent drug for sedation Raised ICP effect not as important as prevention of hypotension
30 DRUG CHOICE Fentanyl: In isolation, provides sympathetic ablation in high dose Additive effects when combined Need 5-10mcg/kg Chest wall rigidity not an issue when using MR
31 DRUG CHOICE Midazolam: Mild Vasodilator, negative inotrope esp when combined Slow onset and offset leads to non optimal timing when used as part of RSI Not used for induction in Oz
32 PART 4: PUTTING IT ALL TOGETHER CASES
33 CASE 1 24 yo male with head injury from MBA GCS 7 BP 100/45 P100 Sats 98% RA DOES HE NEED A TUBE?
34 Inline immobilisation required Unable to adequately position May have other injuries STEP 1: ASSESS AIRWAY AND PLAN May not be able to use NPA if BOS # May have facial injuries Desat associated with adverse neuro outcome
35 AIRWAY Collar off, inline needed Tilt bed to 15-30deg Have OPA/NPA ready Primary plan: RSI with laryngoscope backup is LMA
36 STEP 2: PRE02 Main issues are positioning and prevention desat High flow mask 02 and NP 02 Probably wont need PEEP/NIV/DSI given starting sats
37 STEP 3: HD PREP BP is borderline already BP <90 = bad outcome in head injury Needs IVF load 1L NS at least If BP not improved, consider using pressor cover for induction Choice of agent: Fentanyl mcg Ketamine 1-2mg/kg Thiopentone 2-3mg/kg
38
39 CASE 2 74 yo lady APO Sats 80% on 10L 02 BP 150/100 DOES SHE NEED A TUBE?
40 ASSESS AND PLAN LEMON Position: will need to stay sitting up as long as possible
41 PRE 02 Immediate need for PEEP: Start CPAP 10-20cm/H20 Consider DSI approach if not tolerating Remember to treat APO as well (GTN, diuretic if needed) Do not rush in to ETT
42 PEEP here is extremely important Leave on CPAP until laryngoscope in PEEP valve on BVM Pre setup oxylog
43 HD PREP Although BP OK now she has LVF Will be much more sensitive to effects of induction drug Drug Choice Fentanyl Ketamine Thio
44
45 CASE 3 35 yo man with T 39, BP 85/50, P 130, Sats 85% 15L NRB; GCS 14 Clinical pneumonia DOES HE NEED A TUBE?
46 AIRWAY AND PLAN LEMON ADJUNCTS POSITION: will need sitting up
47 PRE02 Needs NIV: PEEP very important DSI strategy if not tolerating
48 HD PREP Distributive shock Needs substantial filing (3L NS) If BP <120 by induction add norad first Ketamine ideal drug here
49
50 CASE 4 19F with large OD of tricyclic BP 85/50 Sats 98 RA P120 GCS 10 Does she need a tube?
51 AIRWAY AND PLAN LEMON POSITION TCA specific issues
52 PRE O2 No anticipated problems Needs HF 02 and NP BUT: Acidosis a big issue here, need to minimise apnoea time Use bagging during RSI
53 HD PREP Issue here is dilated and and risk arrhythmia Aggressive fluid load Bicarbonate pre induction Consider pressor cover Induction drug: rapid onset/offset; careful dosing
54
Kelowna June 2011 Airway Assessment and Management. Golden, BC
 Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
Kelowna June 2011 Airway Assessment and Management Dr. Bruce Starke Golden, BC Not really... I am unable to identify any potential conflict of interest and I am unable to identify any potential conflict
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
by Weingart S, Nickson C, Rabinovich J, Strayer R. version
 EMCrit Call/Response Intubation Ch Plan HOp Killers-Hemodynamics, Ox, ph RSI Awake DSI RSA ICP/Vascular Induction Agent/Muscle Relaxant Push-Dose Presss Failed Airway Plan Verbalized Cric-Con Evaluation
EMCrit Call/Response Intubation Ch Plan HOp Killers-Hemodynamics, Ox, ph RSI Awake DSI RSA ICP/Vascular Induction Agent/Muscle Relaxant Push-Dose Presss Failed Airway Plan Verbalized Cric-Con Evaluation
Airway Management in the Multiply Traumatized Patient
 Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
It costs you nothing, but gains everything for your patient!
 It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will
It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will
Acute Respiratory Failure
 Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
Acute Respiratory Failure Family Medicine Update Big Sky, Montana January, 2014 Mark Tieszen, MD, FCCM, FCCP Sanford Medical Center Fargo Critical Care Medicine mark.tieszen@sanfordhealth.org Acute Respiratory
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Airway 2015 Updates in Emergency Airway Management
 Airway 2015 Updates in Emergency Airway Management Gerry Maloney, DO, FACOEP Associate Medical Director, Metro Life Flight Attending Physician, Emergency Medicine, CWRU/MetroHealth Medical Center None
Airway 2015 Updates in Emergency Airway Management Gerry Maloney, DO, FACOEP Associate Medical Director, Metro Life Flight Attending Physician, Emergency Medicine, CWRU/MetroHealth Medical Center None
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
GENERAL ANAESTHESIA AND FAILED INTUBATION
 GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
GENERAL ANAESTHESIA AND FAILED INTUBATION INTRODUCTION The majority of caesarean sections in the UK are performed under regional anaesthesia. However, there are situations where general anaesthesia (GA)
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Scenario title. We re Coming Down Intrahospital Transfer post MET. Designed for (specific group) ICU MET team. Scenario Design team.
 ICU MET team. Scenario Design team.") Scenario title We re Coming Down Intrahospital Transfer post MET Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of
Scenario title We re Coming Down Intrahospital Transfer post MET Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked DRUG AND TREATMENT ORDERS
 are unchecked DRUG AND TREATMENT ORDERS") DRUG AND TREATMENT Intubation Phase Notify Therapy for STAT intubation Medications SUB Rapid Sequence Induction (SUB)* ***Reminder: Order SUB Rapid Sequence Induction (SUB) on a separate form*** lidocaine
DRUG AND TREATMENT Intubation Phase Notify Therapy for STAT intubation Medications SUB Rapid Sequence Induction (SUB)* ***Reminder: Order SUB Rapid Sequence Induction (SUB) on a separate form*** lidocaine
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
A Successful RSI Program
 RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
RSI A Successful RSI Program Requires understanding of: Indications Contraindications Limitations Requires knowledge of: Physiology Pharmacology Airway techniques Goals of RSI Success rates comparable
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Bringing It All Into View
 Bringing It All Into View Airway Management Strategies For the Rest of Us Bill Landon, FP-C, CCP October 25, 2018 S Introductory Disclaimer What this presentation is: A brief review of the pathophys and
Bringing It All Into View Airway Management Strategies For the Rest of Us Bill Landon, FP-C, CCP October 25, 2018 S Introductory Disclaimer What this presentation is: A brief review of the pathophys and
Financial Disclosures. Goal. Overview. Pre-Oxygenation N 2 O 2. Pre-Oxygenation 3/20/2017. Optimizing Intubation. None
 Financial Disclosures None Optimizing Intubation Rahul Bhat, M.D. FACEP Associate Program Director Associate Professor of Emergency Medicine MedStar Georgetown University Hospital MedStar Washington Hospital
Financial Disclosures None Optimizing Intubation Rahul Bhat, M.D. FACEP Associate Program Director Associate Professor of Emergency Medicine MedStar Georgetown University Hospital MedStar Washington Hospital
VANDERBILT UNIVERSITY MEDICAL CENTER DIVISION OF ANESTHESIOLOGY CRITICAL CARE MEDICINE AIRWAY MANAGEMENT
 These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
Tracheal Intubation in ICU: Life saving or life threatening?
 Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill
 Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid, assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Episode 110 Airway Pitfalls Live from EMU 2018
 Episode 110 Airway Pitfalls Live from EMU 2018 With Dr. Scott Weingart Prepared by Anton Helman, May 2018 The last decade has seen a torrent of literature and expert opinion on emergency airway management.
Episode 110 Airway Pitfalls Live from EMU 2018 With Dr. Scott Weingart Prepared by Anton Helman, May 2018 The last decade has seen a torrent of literature and expert opinion on emergency airway management.
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Anaphylaxis/Latex Allergy
 Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
Children s Acute Transport Service CATS Clinical Guideline Anaphylaxis/Latex Allergy Document Control Information Author D Lutman Author Position Consultant Document Owner E Polke Document Owner Position
@airwaycam airwaycam.com
 It s not just about the tube, its the VAPORS & Resuscitation Sequence Intubation What are our lives except a vapor that appears for a little while and vanishes and passes away? James 4:14 Ventilation Acidosis
It s not just about the tube, its the VAPORS & Resuscitation Sequence Intubation What are our lives except a vapor that appears for a little while and vanishes and passes away? James 4:14 Ventilation Acidosis
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Airway management. Gabriel Blecher
 Airway management Gabriel Blecher Richard Levitan 1: Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.e1.
Airway management Gabriel Blecher Richard Levitan 1: Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.e1.
Scenario title. Pear Shaped- prepare for intubation on the ward. Designed for (specific group) ICU MET team. Scenario Design team.
 ICU MET team. Scenario Design team.") Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
RAPID SEQUENCE INTUBATION FOR THE RURAL DOC
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 240 RAPID SEQUENCE INTUBATION FOR
General Medical Procedure. Emergency Airway Techniques (General Airway Protocol)
") General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
General Medical Procedure Appropriate airway management is often the most important intervention a prehospital care provider makes, as ensuring adequate oxygenation and ventilation is crucial to the survival
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
SESSION 3 OXYGEN THERAPY
 SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Airway and Breathing
 Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
Airway and Breathing ETAT Module 2 Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005 Learning Objectives Accurately determine whether
VUMC Multidisciplinary Surgical Critical Care Service
 VUMC Multidisciplinary Surgical Critical Care Service SICU Standard Operating Procedure: Guidelines for Intubation I. Definition Intubation is required for SICU patients who cannot maintain a patent airway,
VUMC Multidisciplinary Surgical Critical Care Service SICU Standard Operating Procedure: Guidelines for Intubation I. Definition Intubation is required for SICU patients who cannot maintain a patent airway,
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Surgical Care at the District Hospital 1 14 Practical Anesthesia Key Points 2 14.1 General Anesthesia Have a clear plan before starting anesthesia Never use an unfamiliar anesthetic technique in an emergency
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation Analgesia and Sedation for Major Trauma Patients.
 Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation and Sedation for Major Trauma Patients Participants: Dr. James French, SJRH EM and NBTP Sue Benjamin RN, NBTP Julie Ringuette RN,
Consensus Statement: ADULT Rapid Sequence Intubation and Post-Intubation and Sedation for Major Trauma Patients Participants: Dr. James French, SJRH EM and NBTP Sue Benjamin RN, NBTP Julie Ringuette RN,
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Prehospital Medication Assisted Intubation
 Prehospital Medication Assisted Intubation Supersedes: 09-11-06 Effective: 01-29-10 This document includes the protocol for prehospital medication assisted intubation (MAI). Also included are clinical
Prehospital Medication Assisted Intubation Supersedes: 09-11-06 Effective: 01-29-10 This document includes the protocol for prehospital medication assisted intubation (MAI). Also included are clinical
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
The Pediatric Airway. Andrew Wackett, MD
 The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
The Pediatric Airway Andrew Wackett, MD Objectives 1) Demonstrate understanding of the indications for intubation 2) Perform rapid sequence intubation 3) Learn the pharmacology behind emergency airway
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
PROCEDURAL SEDATION AND ANALGESIA
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 260 PROCEDURAL SEDATION AND ANALGESIA
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 260 PROCEDURAL SEDATION AND ANALGESIA
Redundancy of safety (primary and backup chute) Planned stepwise approach to deploy 1 ary chute Simple, fast, easy backup chute deployment Attention
 Planned stepwise approach to deploy 1 ary chute Simple, fast, easy backup chute deployment Attention") Rapid Sequence Intubation John Bradley, MD Metropolitan Hospital May 30, 2012 1 Lessons from Skydiving Levitan RM. Patient safety in emergency airway management and rapid sequence intubation: metaphorical
Rapid Sequence Intubation John Bradley, MD Metropolitan Hospital May 30, 2012 1 Lessons from Skydiving Levitan RM. Patient safety in emergency airway management and rapid sequence intubation: metaphorical
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
Jason Zurba BSc RRT Supervisor Royal Columbian Hospital
 Jason Zurba BSc RRT Supervisor Royal Columbian Hospital Outline Why we started looking at this What our own data has shown us What the literature tells us about intubation What we have changed How this
Jason Zurba BSc RRT Supervisor Royal Columbian Hospital Outline Why we started looking at this What our own data has shown us What the literature tells us about intubation What we have changed How this
Introducing the Fastrach-LMA. Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council
 Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Introducing the Fastrach-LMA Prepared by Jim Medeiros, NREMT-P Regional Field Coordinator Lord Fairfax EMS Council Objectives Review Anatomy of the Upper Airway Review LFEMSC LMA Protocol Discuss Indications
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
EMS Subspecialty Certification Review Course. Learning Objectives
 EMS Subspecialty Certification Review Course 1.1.2 Airway Compromise / Respiratory Failure 1.1.2.1 Devices for securing airway 1.1.2.2 Portable ventilator management 1.1.2.3 Pros and cons of drug assisted
EMS Subspecialty Certification Review Course 1.1.2 Airway Compromise / Respiratory Failure 1.1.2.1 Devices for securing airway 1.1.2.2 Portable ventilator management 1.1.2.3 Pros and cons of drug assisted
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM
 student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
student handbook BARS handbook September 2012.indd Front Cover 27/11/12 12:08 PM All materials regarding the Basic Airway Resuscitation Strategy Course were written and developed by Dr. Richard Morris
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
It s as easy as ABC. Dr Andrew Smith
 It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
EMERGENCY AIRWAY MANAGEMENT HANDBOOK
 St Vincent s & Mater Health Campus EMERGENCY AIRWAY MANAGEMENT HANDBOOK Don Harrison Patient Safety Simulation Centre EMERGENCY AIRWAY MANAGEMENT HANDBOOK 6 th Ed. 2015 Compiled by the staff of the Don
St Vincent s & Mater Health Campus EMERGENCY AIRWAY MANAGEMENT HANDBOOK Don Harrison Patient Safety Simulation Centre EMERGENCY AIRWAY MANAGEMENT HANDBOOK 6 th Ed. 2015 Compiled by the staff of the Don
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT AVOIDING THE CRASH 1: DON T INTUBATE, OPTIMIZE PRE-AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
CASE REPORT FORM (v )
") INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM (v 1.2 30.09.18) SITE INFORMATION
2007 Recertification Session. Airway review
 2007 Recertification Session Airway review Level of awareness: This is similar to the AVPU, the GCS is performed later Verbal, loud verbal, or pain stimulus. If pain stimulus, consider a trapezeus squeeze
2007 Recertification Session Airway review Level of awareness: This is similar to the AVPU, the GCS is performed later Verbal, loud verbal, or pain stimulus. If pain stimulus, consider a trapezeus squeeze
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ
 PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
Risky Extubation. Andy Higgs. Warrington Hospitals Cheshire UK
 Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
Andy Higgs Warrington Hospitals Cheshire UK Declaration COOKMEDICAL Extubation plan DAS guideline Airway Exchange Catheters # 11 CAEC post maxillo-facial surgery Used as intubation stylets Airway Exchange
PRACCTICE GUIDELINE EM015 RAPID SEQUENCE INTUBATION
 PRACTICE GUIDELINE EM015 RAPID SEQUENCE INTUBATION This Practice Guideline sets out algorithms for Intubation in the emergency environment. The evidence review supporting this Practice Guideline is presented
PRACTICE GUIDELINE EM015 RAPID SEQUENCE INTUBATION This Practice Guideline sets out algorithms for Intubation in the emergency environment. The evidence review supporting this Practice Guideline is presented
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients