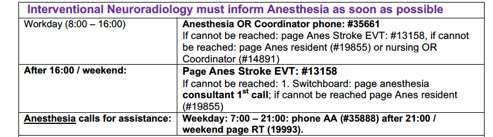
Acute Stroke Treatment: Mechanical Thrombectomy
|
|
|
- Ariel Ryan
- 5 years ago
- Views:
Transcription
1

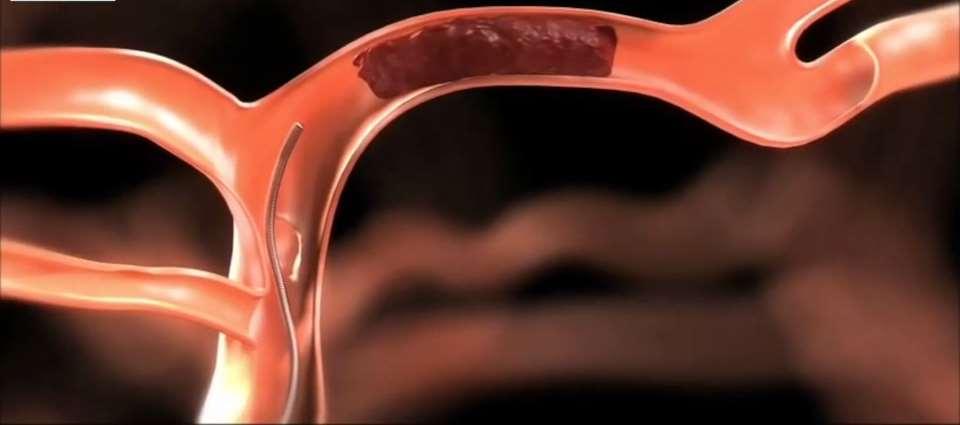
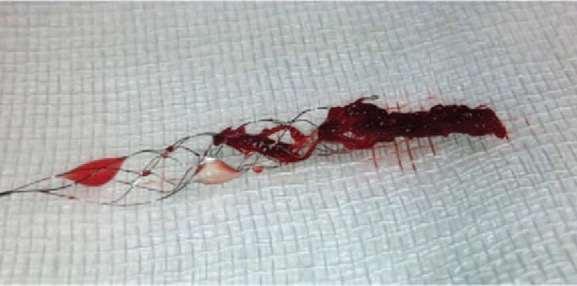
2 Acute Stroke Treatment: Mechanical Thrombectomy Rudy Noppens Department of Anesthesiology & Perioperative Medicine
3 CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Faculty: Dr. Ruediger Noppens, MD, PhD, FRCPC Relationships with financial sponsors: Grants/Research Support: none. Speakers Bureau/Honoraria: none. Consulting Fees: none. Patents: none. Other: Employee of London Health Sciences Center, Western University
4 CFPC CoI Templates: Slide 2 Disclosure of Financial Support This program has received financial support from CAS in the form of research grants. Potential for conflict(s) of interest: Dr. Ruediger Noppens has not received any payment/funding, etc. No organization developed/licenses/distributes/benefits from the sale of, etc. a product that will be discussed in this program
5 Code Stroke

6 Case: 68-year-old woman awoke from nap, difficulty getting up, kept falling back onto her left side. Weakness of her left arm, hand, and foot. Husband also noticed a left-sided facial droop and slurred speech. Rushed to hospital: CT / CT angio
7 Acute Stroke Cases for EVT at LHSC, London, ON 150 Stroke EVT cases Year

8
9

10 Time Window for EVT
11 What is the current time limit for interventional therapy? A.) 4 hrs B.) 6 hrs C.) 8 hrs D.) > 12 hrs

12 Time-window for endovascular treatment Meta-analysis of pooled individual patient data 1287 adults in 5 randomized trials Thrombectomy up to 7.3 hours after symptom onset: improved outcome functional improvement: 64% (3 hrs) vs 46% (8 hours)


13 Time-window for endovascular treatment RCT: 206 patients - clinical deficit disproportionately severe to CT scan thrombectomy + standard medical care vs standard medical care alone
![Time-window for endovascular treatment 0 [death] to 10 [no symptoms or disability]) Time window for EVT](/docs-images/88/115720612/images/14-1.jpg "and standard medical treatment: up to 24 hours in patients with mismatch clinical presentation / CT")
14 Time-window for endovascular treatment 0 [death] to 10 [no symptoms or disability]) Time window for EVT and standard medical treatment: up to 24 hours in patients with mismatch clinical presentation / CT scan


15 Presence of Anaesthesiologist
16 QI project: Anaesthesia - EVT Stroke 150 EVT Stroke Anaesthesia present Total Number %

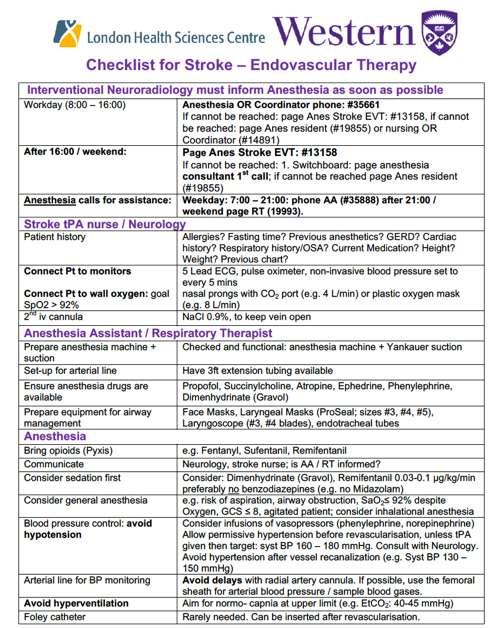
17 Code Stroke Checklist Call RT / AA
18 QI project: Anaesthesia for EVT Stroke 50 EVT Stroke Anaesthesia present Total Number

19 rtpa (Alteplase)
20 What is not a common complications after IV rtpa administration? A.) Intracerebral hemorrhage B.) Bleeding - small lesions C.) Hypotension D.) Angioedema



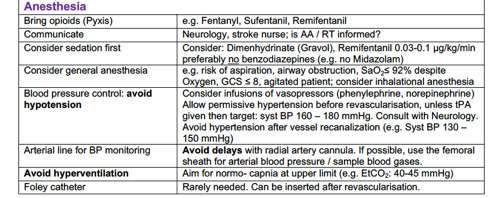
21 rtpa: side effects Intracranial hemorrhage: 5.8 % Orolingual angioedema: % Risk factors: ACE inhibitor Ischemia: insula / anterior frontal cortex Anaphylactoid-like response No nasal airway! No naso-gastric tube! Foster-Goldman A, McCarthy D. Am J Ther. 2013; 20:691-3


22 General Anaesthesia vs Sedation
23 When would you prefer general anesthesia over sedation? A.) Agitated patient B.) Stroke: anterior circulation C.) Stroke: posterior circulation D.) Always sedation (associated with better outcome)
24 GA vs. Sedation General Anesthesia PRO Immobilization Improved quality of imaging Fewer complications? Airway secured Reduced risk of aspiration Lower exposure to X-ray? CON Hemodynamics: risk of hypotension Ventilation: risk of hyperventilation Time to EVT: risk of delay More resources / expertise Conscious Sedation PRO Hemodynamics: more robust Neurological monitoring Time to EVT: shorter CON Uncontrolled airway Patient movements (risk of EVT complications) EVT procedure time prolonged Higher exposure to X-ray?
25 General Anesthesia / Sedation GA (23 %) CS (77 %)




26 Patient access is limited Conversion CS to GA can be challenging!

 infarct growth: MRI scans")
27 GA vs. Sedation randomly assigned: general anesthesia (n = 65) vs. sedation (n = 63) infarct growth: MRI scans before EVT and hours after EVT JAMA Neurol. 2018: 75:

28 GA vs. Sedation GA did not result in worse tissue outcomes compared with CS better clinical outcomes in the GA group JAMA Neurol. 2018: 75:
29 Anesthesia technique Individualized based on clinical characteristics of each patient GA : airway protection, stroke posterior circulation, depressed level of consciousness, respiratory compromise Sedation: stroke anterior circulation, sufficient gas exchange, cooperation Anesthesia-related procedures: as quickly as possible - avoid delays Talke PO et al. J Neurosurg Anesthesiol 2014;26:95 108

30 Blood pressure control
31 Patient just arrived from Emerg, rtpa is running. What syst BP do you aim for? A.) mmhg B.) mmhg C.) mmhg D.) mmhg

32 BP: impact on neurology and stroke volume Stroke. 2004;35:
33 Blood pressure control Before revascularization: Systolic blood pressure should be maintained >140mm Hg and <180mm Hg Vasopressor choice should be based on individual patient characteristics Talke PO et al. J Neurosurg Anesthesiol 2014;26:95 108

34 Oxygen

35 Oxygen: friend or foe? Vincent JL, Taccone FS, He X: Can Respir J. 2017;2017:
 Talke PO et al.")
36 Oxygenation / Ventilation Oxygen administration during moderate and deep sedation FiO 2 to maintain SpO 2 > 92% and PaO 2 > 60 mm Hg Ventilation: Normocapnia (PaCO 2, 35 to 45 mmhg) Talke PO et al. J Neurosurg Anesthesiol 2014;26:95 108
37 Checklist Code Stroke
38


39 Suggested literature
40
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Chapter 18. Objectives. Objectives 01/09/2013. Altered Mental Status, Stroke, and Headache
 Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Faculty/Presenter Disclosure. Intracranial EEG Recording. Objectives. General Themes. Why invasive recordings? 6/27/2018
 CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Acute Stroke Management What is State of the Art?
 Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Thrombolysis Delivery, Care, and Monitoring. 5 Acute Trusts - 6 Primary Care Trusts Ambulance Trust 4 Local Authorities
 Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA?
 INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
When Not To Give TPA Steve Phillips Division of Neurology
 When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE
 MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE KRISTA L. LANCTÔT, PHD PROFESSOR OF PSYCHIATRY AND PHARMACOLOGY, UNIVERSITY OF TORONTO; SENIOR SCIENTIST, HURVITZ BRAIN
MORTALITY ASSOCIATED WITH USE OF ANTIPSYCHOTICS IN DEMENTIA: REVIEWING THE EVIDENCE KRISTA L. LANCTÔT, PHD PROFESSOR OF PSYCHIATRY AND PHARMACOLOGY, UNIVERSITY OF TORONTO; SENIOR SCIENTIST, HURVITZ BRAIN
Endovascular treatment for pseudoocclusion of the internal carotid artery
 Endovascular treatment for pseudoocclusion of the internal carotid artery Daqiao Guo, Xiao Tang, Weiguo Fu Institute of Vascular Surgery, Fudan University, Department of Vascular Surgery, Zhongshan Hospital
Endovascular treatment for pseudoocclusion of the internal carotid artery Daqiao Guo, Xiao Tang, Weiguo Fu Institute of Vascular Surgery, Fudan University, Department of Vascular Surgery, Zhongshan Hospital
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery
 Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
NEURORADIOLOGY DIL part 4
 NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 4 Strokes and infarcts K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Resuscitation Patient Management Tool May 2015 MET Event
 OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
OPTIONAL: Local Event ID: Date/Time MET was activated: Time Not Documented MET 2.1 Pre-Event Pre-Event Tab Was patient discharged from an Intensive Care Unit (ICU) at any point during this admission and
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Nursing Management Pre /Post Thrombolysis in Stroke
 Craigavon Area Hospital Guidelines for Nursing Management Pre /Post Thrombolysis in Stroke 1. A senior nurse in the stroke unit will be required to monitor the patients condition post Thrombolysis on a
Craigavon Area Hospital Guidelines for Nursing Management Pre /Post Thrombolysis in Stroke 1. A senior nurse in the stroke unit will be required to monitor the patients condition post Thrombolysis on a
Anesthetic Considerations for Cerebrovascular Neurosurgery
 Anesthetic Considerations for Cerebrovascular Neurosurgery Ajith J. Thomas, MD Associate Professor of Neurosurgery BIDMC Brain Aneurysm Institute Mohamed M. Salem, MD Krishnan Ravindran MD Neurovascular
Anesthetic Considerations for Cerebrovascular Neurosurgery Ajith J. Thomas, MD Associate Professor of Neurosurgery BIDMC Brain Aneurysm Institute Mohamed M. Salem, MD Krishnan Ravindran MD Neurovascular
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Addendum/database Part 1 demographics
 Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Memorandum. Peoria Area EMS System Agencies & Providers. From: Peoria Area EMS System Office. Date: February 24, 2016
 Memorandum To: Peoria Area EMS System Agencies & Providers From: Peoria Area EMS System Office Date: February 24, 2016 Re: Glucagon Administration for BLS Agencies As discussed at the EMS Quarterly Update,
Memorandum To: Peoria Area EMS System Agencies & Providers From: Peoria Area EMS System Office Date: February 24, 2016 Re: Glucagon Administration for BLS Agencies As discussed at the EMS Quarterly Update,
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Cardiac Stress Testing What Stress is Best?
 Cardiac Stress Testing What Stress is Best? Jennifer Gerryts, Registered Respiratory Therapist Kati Tuomi, Medical Radiation Technologist, Nuclear Medicine Thunder Bay Regional Health Sciences Centre 1
Cardiac Stress Testing What Stress is Best? Jennifer Gerryts, Registered Respiratory Therapist Kati Tuomi, Medical Radiation Technologist, Nuclear Medicine Thunder Bay Regional Health Sciences Centre 1
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace