Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
|
|
|
- Eugene Ramsey
- 6 years ago
- Views:
Transcription

1 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR

2 Outline State Statistics The Oregon Problem Time & Treatments Steps to Making a Difference The Future Resources
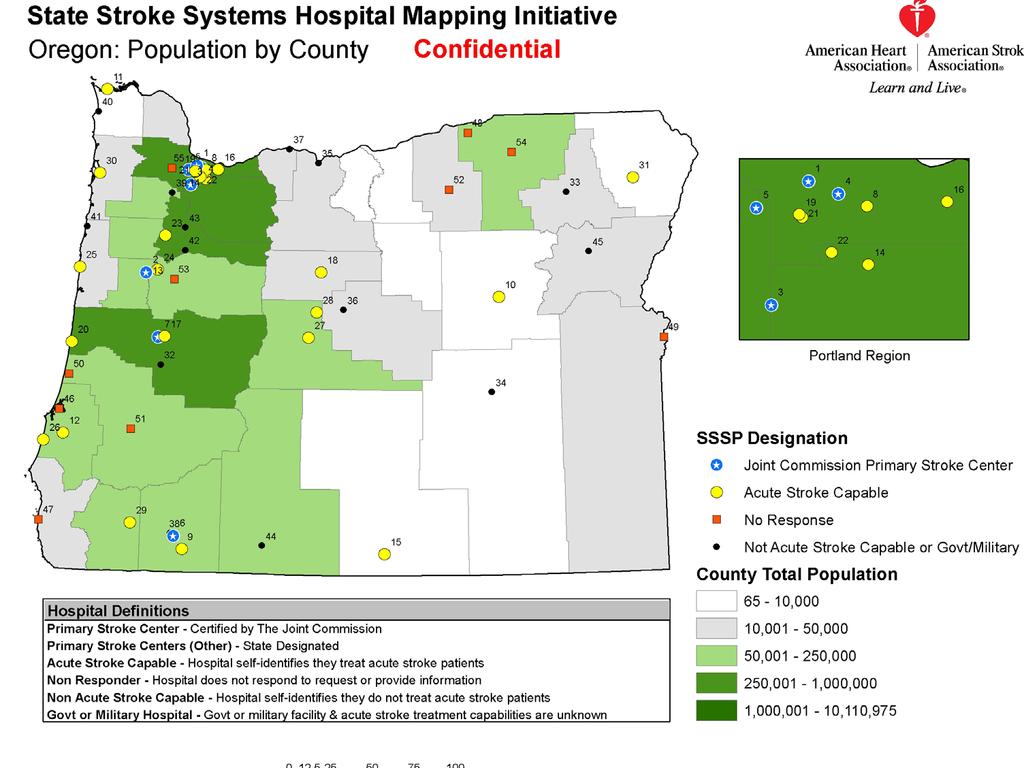
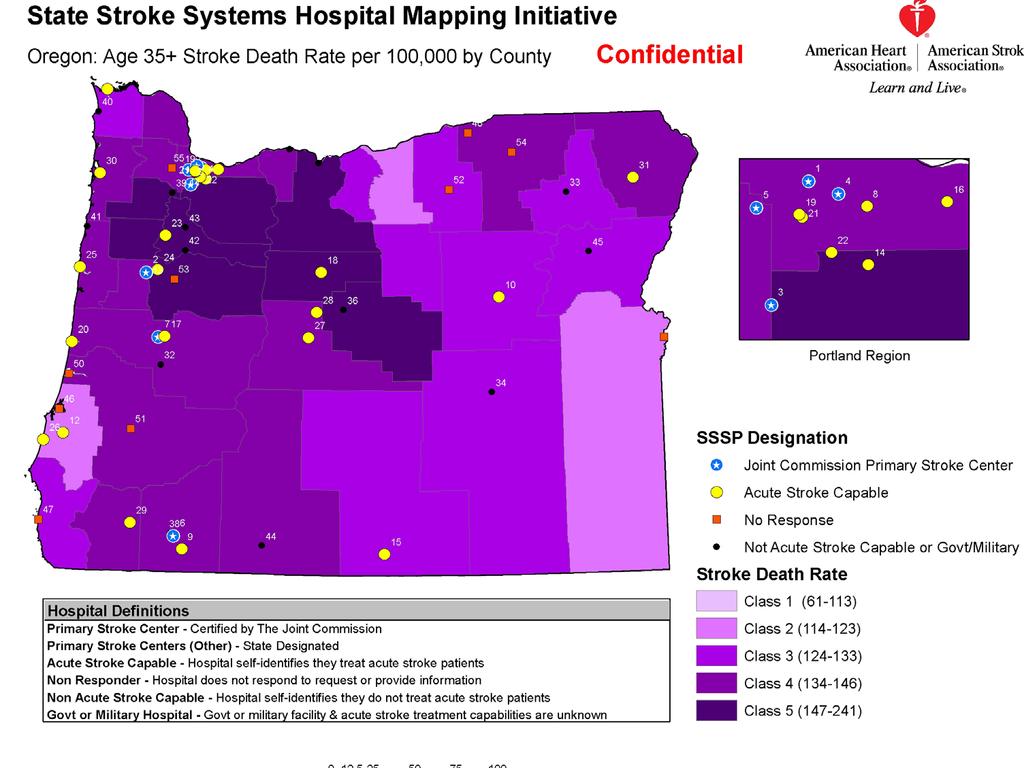
3 Third leading cause of death Leading cause of adult disability Leading diagnosis from hospital to LTC $181 million total cost of stroke hospitalizations in 2006 (OR) OR 5 th highest stroke death rate
4
5
6

7
8 Problem Small rural hospital Oregon (Oct. 2008) : Want to give most up to date stroke care Limited resources: Not a Primary Stroke Center No Neurology coverage Limited N. Surgery, pharmacy, radiology, Hospitalist coverage Limited knowledge of tpa / specialty care How can we better serve our patients?
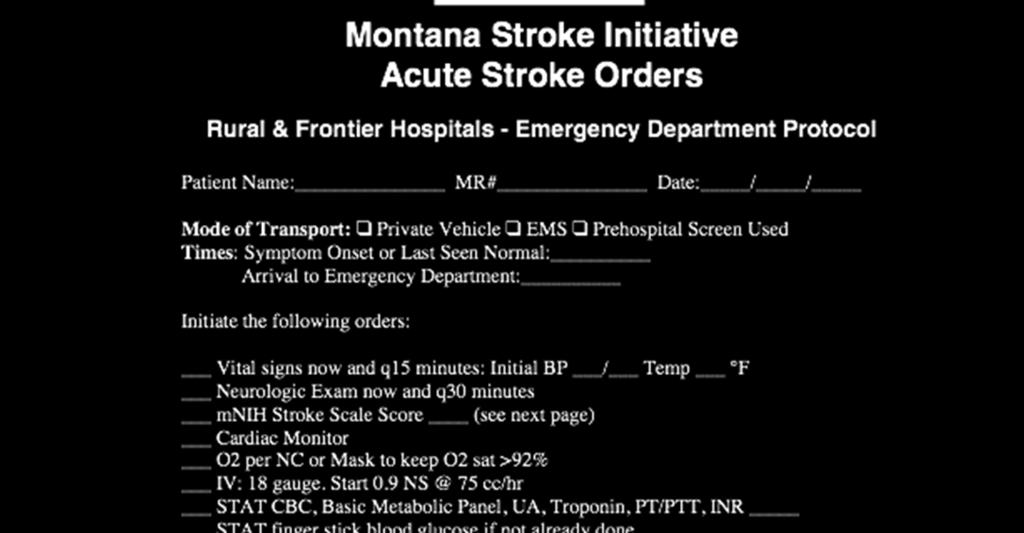
9 Stroke Treatment in Rural Oregon Local treatment is necessary due to Time dependent therapy and long distances between people and tertiary facilities capable and experienced with treatment Minimum requirements for administering thrombolytic therapy are: CT scanner 24/7 EMS Protocol for expediting transport & pre-notification Acute care/t-pa protocol
10 In the US only 4% stroke patients receive the only FDA approved treatment for acute stroke Patients don t often recognize their symptoms as stroke and don t understand the need to seek emergent care via 911 Primary providers have very little training or experience in treating stroke patients let alone use of t-pa Neurologists are in short supply and clustered in urban areas Until recently there was no economic incentive to treat acute stroke
 t-pa approved in 1996 ONLY APPROVED MEDICATION Must be given w/in 3 hrs of onset (last normal) Requires neurological expertise, urgent")
11 Stroke Treatment.. (Ischemic) t-pa approved in 1996 ONLY APPROVED MEDICATION Must be given w/in 3 hrs of onset (last normal) Requires neurological expertise, urgent CT scanning PROTOCOL necessary Primary Stroke Centers Protocols, experts, guidelines, registries, data, quality improvement, outcomes
12 Oregon, 2009 TJC certified Primary Stroke Centers Providence St. Vincent s, 2004 Legacy Good Samaritan, 2004 Legacy Meridian Park, 2004 Providence Portland, 2005 Rogue Valley (Medford), 2006 OHSU, 2007 Sacred Heart (Eugene), 2008 *24/7 Comprehensive Capability

 Clinical Trials Drugs and devices")
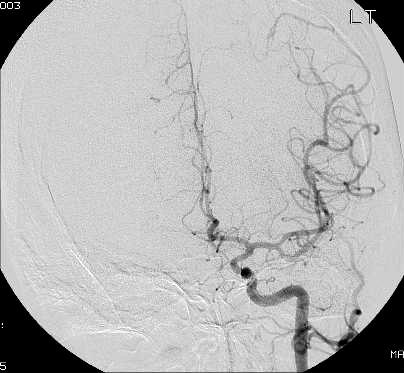
13 Treatment Options / Comprehensive Stroke Centers IV t-pa Intra-arterial t-pa Intra-arterial devices (up to 8 hr window) Clinical Trials Drugs and devices Hypothermia

14

15 Rural Oregon the beauty and the challenge.
16 Making a difference in your hospital & community YOU CAN: Find a clinical champion Recruit administrative support Assess resources (Pharmacy, Radiology, Lab, etc) Develop protocols (ED & in-patient) Work closely with first responders Relationship with experts for advice / transfer EDUCATE staff Educate community Quality review processes

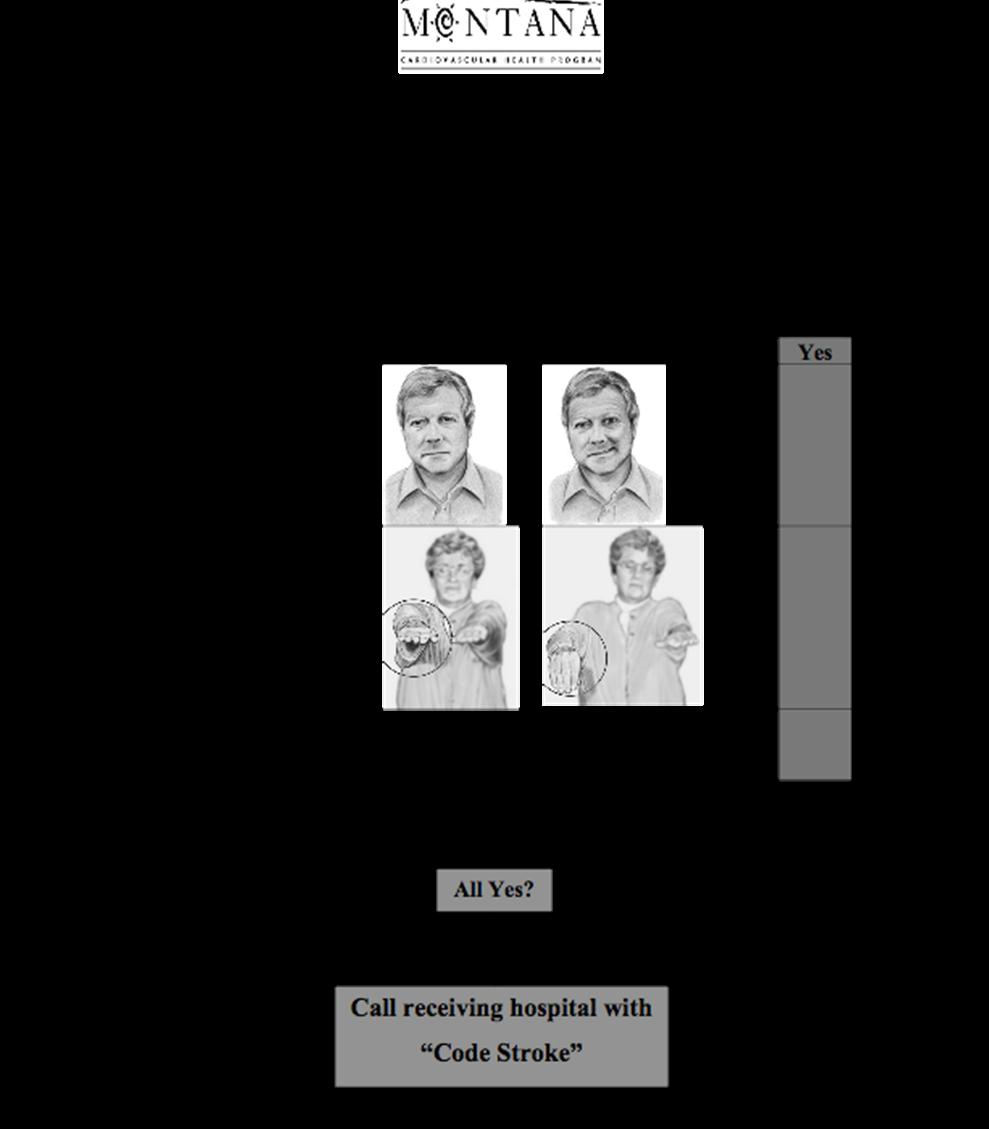
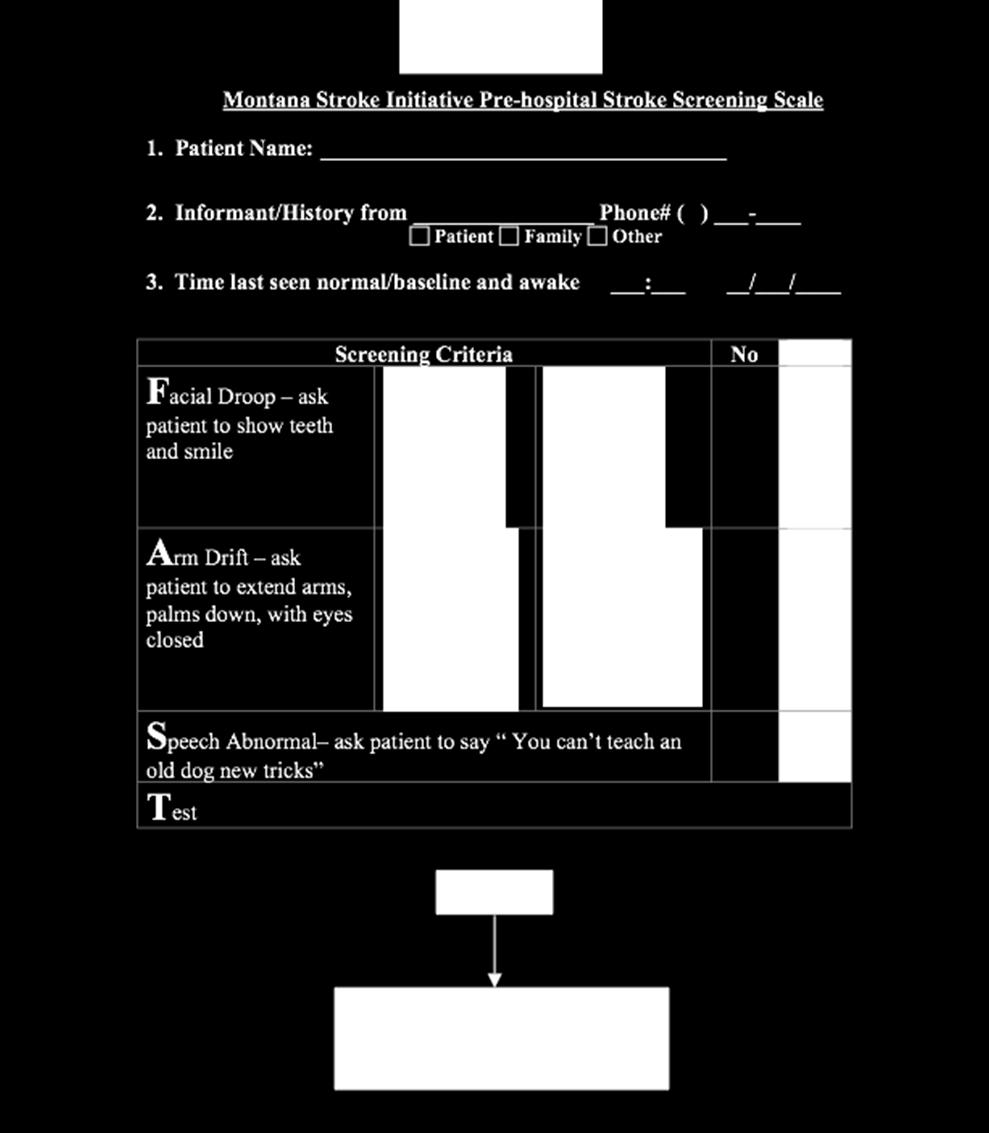
17 Pre-Hospital Stroke Care Scoop and go! Pre-notify Hospital
18
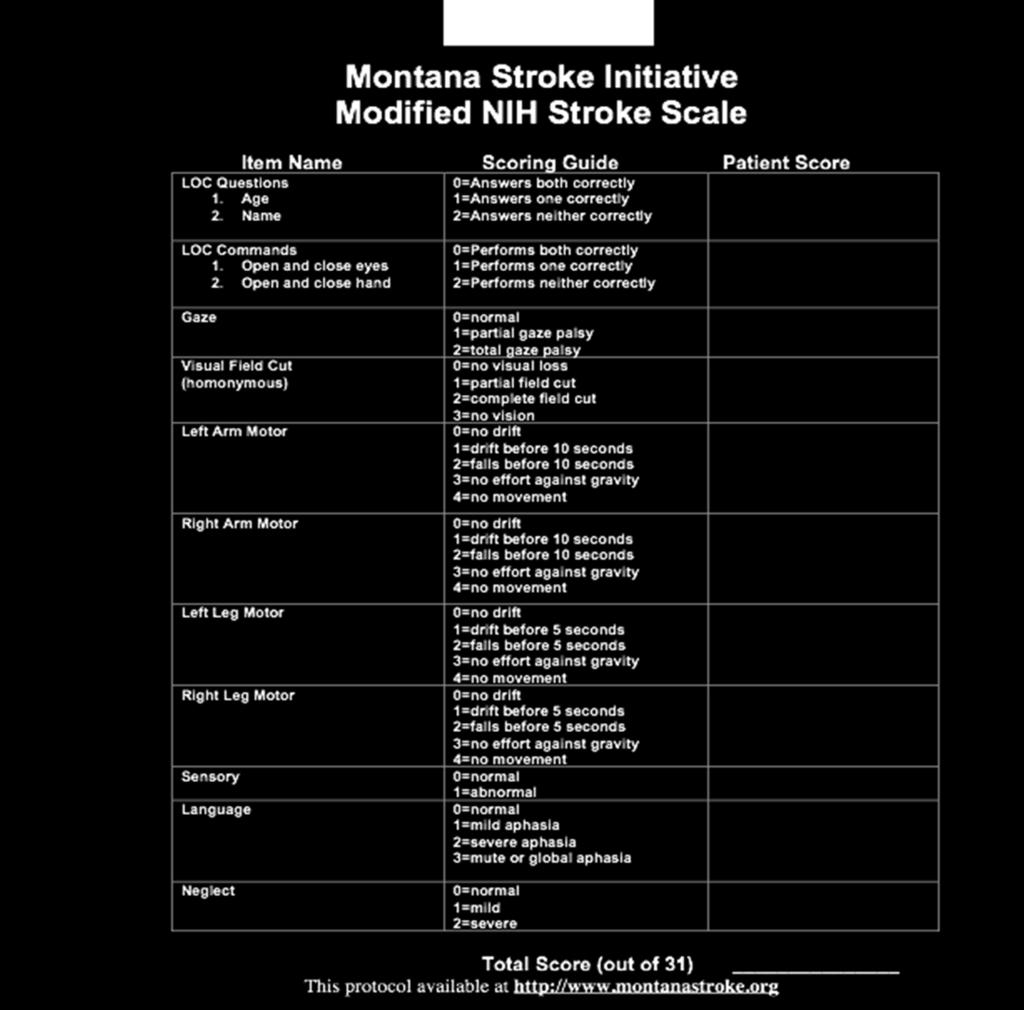
19 Neurological Assessment Patient With Stroke-Like Symptoms Exam elements: Level of consciousness Pupils and gaze Arm and leg motor exam strength and overall coordination Facial symmetry and smile effort Speech and understanding Slurred speech Clear but nonsensical speech Must be quick and simple Problems understanding simple commands

20 The Emergency Room
21
22
23
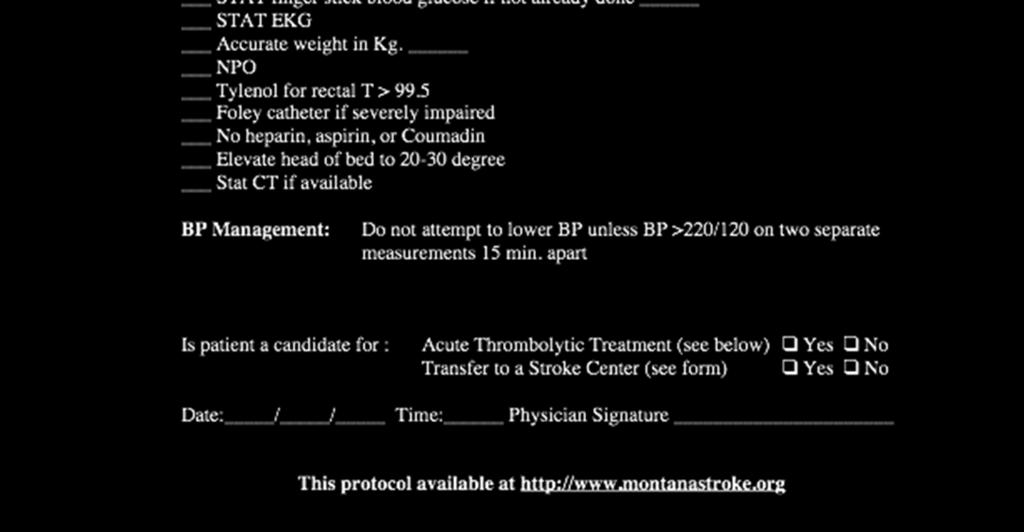
24 Beware! Common errors to avoid. Blood Pressure Do not treat elevated blood pressure unless > 220 systolic or, diastolic > 115 Treating with t-pa must be below 185/110 The brain needs the perfusion, can worsen stroke if lower blood pressure too low IV Fluids Avoid glucose containing solutions Correct hypotension and volume deficits from dehydration otherwise run fluids TKO

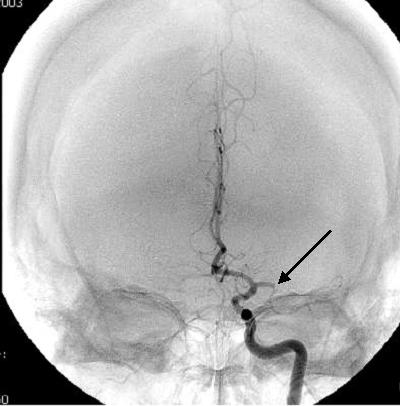
25 STAT Non-Contrast Head CT Two pts both present w/ L sided weakness: A. Ischemic stroke R. hemisphere not yet visible B. R. hemispheric intracerebral hemorrrhage

26 tpa Administration Considerations Must be started before 3 hours from onset (last normal) No blood on head CT Review patient s history for other risk factors Accurate inclusion / exclusion Record weight BP less than 185/110 to treat
27 Hemorrhage Suspected STOP TPA INFUSION, call MD immediately Stat head CT without contrast Draw blood for PT, PTT, plt ct, fibrinogen, and type and hold Prepare for administration of cryo and or platelets

28 Drip and Ship?


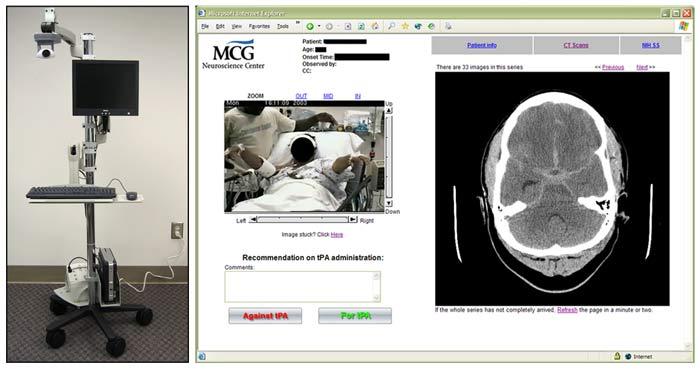
29 Remote Expert Options: Phone Consultation < OR > Bring the expert to you via Telestroke Future?
30
 Clinical Trials")
31 Other Treatment Options for Ischemic Strokes If symptom onset is greater than 3 hrs ~ consider up to 8 hrs: Interventions (IA, Merci, stenting) Clinical Trials
32 Treatment Cont If not a tpa candidate, ASA in ED. Rectal ASA if fails swallow eval. or if swallow eval. not complete. Keep NPO, until a formal swallow eval. is done. Admit as Inpatient and perform diagnostic testing: Carotid US, Echo, TEE, ECG monitoring for a-fib, MRI, fasting Lipid, Clotting disorder blood work (Antiphospholipid, Factor V, Antithrombin III) Rehabilitation
33
34 In-patient Considerations Nursing Issues Started on stroke prevention medications (antithrombotic within 48 hr)? Clinical pathway followed? Blood pressure within appropriate parameters (Mean 100) Know signs of suspected Intracranial Hemorrhage and actions to take (change in LOC?) DVT prophylaxis addressed by day 2? Compression Devices/Lovenox/heparin SQ per orders Therapies seeing patient? Review PT/OT/ST recommendations
35 Inpatient Cont IV fluids (Normal Saline or LR)? Nutrition? Dietary evaluation. Assistive devices for feeding. SWALLOW SCREEN DONE? Fever? Treat if greater than 99 F with Tylenol Blood glucose within appropriate parameters? Obtain sliding scale if necessary. Positioning? Pillows under affected limbs. Turn Q2hours. Accommodate limitations Rehab consults as soon as possible, if needed
 NPO, until swallow eval is completed Anticipate Neurosurgical consult Possible administration of blood")
36 Hemorrhagic Stroke Treatment Do not give antithrombotics or anticoagulants Monitor and treat blood pressure greater than 150/105 (Table 6, 2005 Guidelines update) NPO, until swallow eval is completed Anticipate Neurosurgical consult Possible administration of blood products
37 The ideal stroke system interface Stroke ready Dispatch and EMS personnel Clear routing to stroke ready hospitals Stroke ready ED s/hospitals/transfer systems Responsive ED/stroke care team Interdisciplinary, regional or state wide team to develop all of the above
38 Small rural hospital SE Oregon.. Scenario #2 future Providers will be educated on diagnosis and stroke options Will call experts for advise ASAP May treat with tpa at rural hospital Patient will be rapidly transferred to appropriate Primary / Comprehensive Stroke Center for treatment and/or further care. Inpatient protocols to guide best care

39 Building the Oregon Stroke System of Care: Connecting Rural and Urban Populations to Improve Outcomes Third Annual Meeting of the Oregon Stroke Network In Collaboration with Oregon EMS & Trauma Systems Program October 23, 2009 Riverhouse Resort, Bend, OR Information will be posted on the Office of Rural Health website
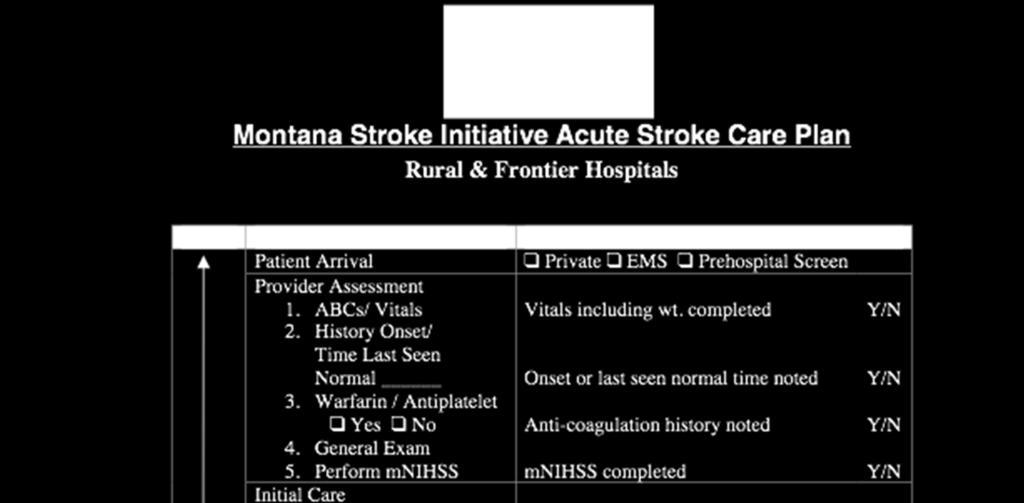
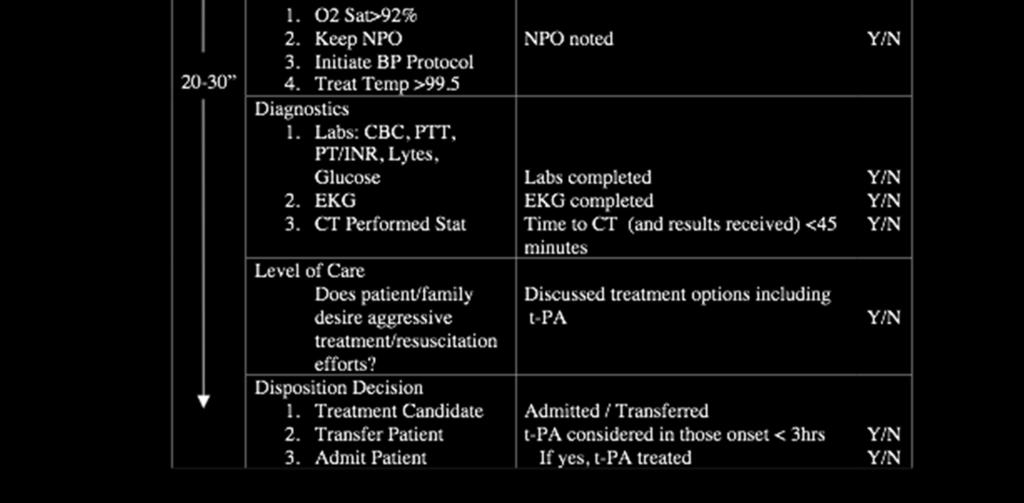
40 Resources Providence Stroke Center, Montana Stroke Network, (rural protocols/templates) 2008 Hospital Survey conducted by Heart Disease and Stroke Prevention Program with the Hospital association: Northwest Regional Stroke Network Burden Report Stroke-Network/publications/NWRSN-Burden-Doc.pdf 2007 EMS survey conducted by the Heart Disease and Stroke Prevention Program and the AHA/ASA Heart Disease and Stroke Prevention Program data and data related reports are at:
 opportunities for your hospitals to get involved with 1.")
41 Oregon State Stroke System of Care (Recommendations for the American Stroke Association s Establishment of Stroke Systems of Care can be found at opportunities for your hospitals to get involved with 1. Oregon Stroke Network: Steering Committee, Symposium Planning Committee Delivery of Care- EMS Subcommittee Data/Quality Improvement/ Surveillance Subcommittee: TBD 2. NWRSN: 3. Annual OR Stroke Symposium in October, Bend Get With The Guidelines: Stroke 5. Stroke Camp for Families living with Aphasia 6. Telemedicine/ Telehealth: Oregon Health Network (in development)
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Stroke Systems of Care. Sharon Webb, MD, FAANS, FACS, FAHA
 Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
UF HEALTH SHANDS CORE POLICY AND PROCEDURE. Stroke Alert Process
 UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
The Mercy Telehealth Network: Your direct connection to specialized care
 The Mercy Telehealth Network: Your direct connection to specialized care Mercy Telehealth Network Presentation Goal To provide an overview of the Mercy Telehealth Network To suggest that Telehealth is
The Mercy Telehealth Network: Your direct connection to specialized care Mercy Telehealth Network Presentation Goal To provide an overview of the Mercy Telehealth Network To suggest that Telehealth is
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
2017 Stroke Statistics
 2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
2017 Stroke Statistics 2017 LUMC Stroke Volumes by Type of Stroke Ischemic Stroke Treatment by Type 2017 17% 8% 75% Ischemic Intracerebral Hemorrhage Aneurysmal Subarachnoid Hemorrhage 31 42 25 r-tpa Administered
EMS Stroke Care in the Fox Valley
 EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
3. Screening Subject Identification Screening Overview
 3. Screening 3.1 Subject Identification Each site will be responsible for identifying and recruiting participants into the study. It is known that screening methods vary across sites. It is, however, important
3. Screening 3.1 Subject Identification Each site will be responsible for identifying and recruiting participants into the study. It is known that screening methods vary across sites. It is, however, important
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
Mission: Lifeline Stroke Nebraska
 Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Mission: Lifeline Stroke Nebraska What is Mission: Lifeline Stroke? Mission: Lifeline Stroke is the American Heart Association s national initiative to transform stroke care by focusing efforts on connecting
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field. Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke
 Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Mark J. Alberts, MD. Turning the Wheels of Stroke Care
 Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Impact of a Statewide Telestroke. IHI Triple Aim
 Impact of a Statewide Telestroke Network in Oregon: Meeting The IHI Triple Aim Nicholas J. Okon, DO Stroke Neurologist Medical Director Providence Telestroke Network CEO and Founder Northwest Stroke Solutions,
Impact of a Statewide Telestroke Network in Oregon: Meeting The IHI Triple Aim Nicholas J. Okon, DO Stroke Neurologist Medical Director Providence Telestroke Network CEO and Founder Northwest Stroke Solutions,
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
PATIENT S NOTES History and Physical Brain Attack Stroke
 UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Stroke Awareness. Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director
 Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Stroke Awareness Presented by: Duane Anderson, MD Snoqualmie Valley Hospital Emergency Department Medical Director What is a stroke? Stroke can happen to anyone. Stroke is the fourth leading cause of death
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Identifying Key Players for Early Stroke Management
 Identifying Key Players for Early Stroke Management Cabinet Peaks Medical Center Libby, Montana Presented by: Kimberlee Rebo and John Thornton OBJECTIVES Identify key players in early stroke care & management
Identifying Key Players for Early Stroke Management Cabinet Peaks Medical Center Libby, Montana Presented by: Kimberlee Rebo and John Thornton OBJECTIVES Identify key players in early stroke care & management
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Acute Ischaemic Stroke Pathways Drip and Ship
 Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Acute Ischaemic Stroke Pathways Drip and Ship Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
ED Stroke Panel Page 1 of 2
 ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
Overview. International Stroke Conference Update Clot buster use rises most among 80 and older stroke patients ACUTE STROKE 2/13/2015
 Overview International Stroke Conference Update 2015 Nerissa U. Ko, MD, MAS University of California, San Francisco Recent Advances in Neurology February 13, 2015 Nothing to disclose Non-endovascular treatment
Overview International Stroke Conference Update 2015 Nerissa U. Ko, MD, MAS University of California, San Francisco Recent Advances in Neurology February 13, 2015 Nothing to disclose Non-endovascular treatment
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Hospitals Capacity to Provide Acute Care for Heart Attack and Stroke, Oregon, 2008
 Hospitals Capacity to Provide Acute Care for Heart Attack and Stroke, Oregon, 2008 Background: In 2008, Oregon Heart Disease and Stroke Prevention Program (HDSP) at Oregon Department of Human Services
Hospitals Capacity to Provide Acute Care for Heart Attack and Stroke, Oregon, 2008 Background: In 2008, Oregon Heart Disease and Stroke Prevention Program (HDSP) at Oregon Department of Human Services
01: EMS Pre-Notification Door-To-Needle Processes for Success:
 01: EMS Pre-Notification Door-To-Needle Processes for Success: Greenville Memorial Hospital Shannon Sternberg, RN, MSN, CNRN Stroke Program Coordinator Greenville Hospital System 500 400 300 200 100 0
01: EMS Pre-Notification Door-To-Needle Processes for Success: Greenville Memorial Hospital Shannon Sternberg, RN, MSN, CNRN Stroke Program Coordinator Greenville Hospital System 500 400 300 200 100 0
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals
 Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Stroke Special Project 640 and 740 Resource For Health Information Management Professionals Linda Gould RPN Erin Kelleher, BA, CHIM Stefan Pagliuso PT, B.A. Kin(Hon.) Overview of this Resource Overview
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked DRUG AND TREATMENT ORDERS
 are unchecked DRUG AND TREATMENT ORDERS") DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
Coordination and Regionalization of Acute Care: What about stroke?
 Coordination and Regionalization of Acute Care: What about stroke? Tim Lukovits, M.D. Medical Director Cerebrovascular Disease and Stroke Program at DHMC Barriers to more organized acute care unique to
Coordination and Regionalization of Acute Care: What about stroke? Tim Lukovits, M.D. Medical Director Cerebrovascular Disease and Stroke Program at DHMC Barriers to more organized acute care unique to
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs
 The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
An Assessment of Acute Stroke Treatment in Nebraska Hospitals. September 2006
 An Assessment of Acute Stroke Treatment in Nebraska Hospitals September 2006 An Assessment of Acute Stroke Treatment in Nebraska Hospitals Project Report 06-06 July 2006 Katherine Jones, PhD, PT Michelle
An Assessment of Acute Stroke Treatment in Nebraska Hospitals September 2006 An Assessment of Acute Stroke Treatment in Nebraska Hospitals Project Report 06-06 July 2006 Katherine Jones, PhD, PT Michelle
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
2016 Stroke Statistics
 2016 Stroke Statistics Carotid Artery Procedure Mortality Rate *The Joint Commission Requirement < 6 % LUMC 3.0% *The Joint Commission Requirement < 3 % LUMC 0.0% Rate of stroke or death within 30 days
2016 Stroke Statistics Carotid Artery Procedure Mortality Rate *The Joint Commission Requirement < 6 % LUMC 3.0% *The Joint Commission Requirement < 3 % LUMC 0.0% Rate of stroke or death within 30 days
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL. StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian
 PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Thrombolysis Delivery, Care, and Monitoring. 5 Acute Trusts - 6 Primary Care Trusts Ambulance Trust 4 Local Authorities
 Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
Thrombolysis Delivery, Care, and Monitoring Documentation & Pathways Need to follow locally agreed policies and procedures Follow thrombolysis pathway? Need to complete Sits database Weight Dose matters!
STAND AND DELIVER: STANDARDIZATION OF TELEMEDICINE TRAINING FOR ACUTE STROKE CARE
 STAND AND DELIVER: STANDARDIZATION OF TELEMEDICINE TRAINING FOR ACUTE STROKE CARE LEE S CHUNG, MD PETER M HANNON, MD JALEEN SMITH, BS JENNIFER J MAJERSIK, MD, MS DEPT OF NEUROLOGY, UNIVERSITY OF UTAH VA
STAND AND DELIVER: STANDARDIZATION OF TELEMEDICINE TRAINING FOR ACUTE STROKE CARE LEE S CHUNG, MD PETER M HANNON, MD JALEEN SMITH, BS JENNIFER J MAJERSIK, MD, MS DEPT OF NEUROLOGY, UNIVERSITY OF UTAH VA
DISCLOSURES. Learning Objectives. David Lee Gordon, MD, FAHA Update in Stroke 2007 FINANCIAL DISCLOSURE UNLABELED/UNAPPROVED USES DISCLOSURE
 Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
Acute Stroke Care and the Role of EMS Ryan Hakimi, DO, MS April 30, 2015 Assistant Professor Director, Critical Care Neurology Department of Neurology University of Oklahoma Health Sciences Center DISCLOSURES
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Vote Using Your Phone!
 Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Update on Stroke Certification Jean Range, MS, RN The Joint Commission February 28, 2014 Vote Using Your Phone! Answer multiple choice questions by texting a code to 22333. Your phone carrier s texting
Update on Stroke in South Carolina: REACHing to Treat More Patients using Telestroke
 Update on Stroke in South Carolina: REACHing to Treat More Patients using Telestroke 1 Robert J Adams MS MD Professor of Neuroscience University Eminent Scholar Director South Carolina Center of Economic
Update on Stroke in South Carolina: REACHing to Treat More Patients using Telestroke 1 Robert J Adams MS MD Professor of Neuroscience University Eminent Scholar Director South Carolina Center of Economic
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)