When Not To Give TPA Steve Phillips Division of Neurology
|
|
|
- Maude Mosley
- 5 years ago
- Views:
Transcription



1 When Not To Give TPA Steve Phillips Division of Neurology
2 AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers Squibb Hoffmann-LaRoche Merck Frosst Pfizer sanofi-aventis Servier The QEII Acute Stroke Program has received support from GlaxoWellcome, Hoffmann-La Roche, Merck Frosst, sanofi-aventis, Servier, Bayer
3 Disclosures - 2 I was Canadian coordinator for the third International Stroke Trial of t-pa (IST-3) I am a Clinical Advisor for Cardiovascular Health Nova Scotia (CVHNS) I was inaugural co-chair of the Best Practices & Standards Advisory Committee of the Canadian Stroke Strategy


4 Give em the juice! Michael Hill, MD
5 IV t-pa works for A broad spectrum treatment mild, moderate, and severe strokes men and women Stroke Thrombolysis Trialists Collaborative Group, 2014 & 2018
6 Treatment and outcome IV thrombolysis within 6 h of AMI* - alive 35 days later Benefit N / 1000 treated 30 *Fibrinolytic Therapy Trialists' Collaborative Group. Lancet. 1994; 343:
7 Treatment and outcome IV thrombolysis within 6 h of AMI* - alive 35 days later IV tpa within 6 h of stroke^ - alive & independent months later Benefit N / 1000 treated *Fibrinolytic Therapy Trialists' Collaborative Group. Lancet. 1994; 343: ^Emberson J, et al. Lancet. 2014; 384:
8 Treatment and outcome IV thrombolysis within 6 h of AMI* - alive 35 days later IV tpa within 6 h of stroke^ - alive & independent months later IV tpa within 3 h of stroke^ - alive & independent months later Benefit N / 1000 treated *Fibrinolytic Therapy Trialists' Collaborative Group. Lancet. 1994; 343: ^Emberson J, et al. Lancet. 2014; 384:
9 Odds Ratio (95% CI) Effect of timing of IV t-pa on good outcome (mrs 0-1) Treatment delay (h) Emberson, et al. Lancet 2014; 384:

10

11 Life is short; and the art long; and the right time an instant; and treatment precarious; and the crisis grievous. Hippocrates (translator Dickinson Richards)

12 TPA is chemical neurosurgery

13 A case from the Annals of the QEII Emergency Department
14 74 year-old woman 10:00 h sudden left arm weakness & slurred speech One month earlier had transient left leg weakness & found to be in AF. Declined anticoagulant therapy Cognitively intact & functionally independent (CIFI) T+33 mins 911 Pre-hospital Acute Stroke Protocol activation T+46 mins triaged into ED
15 74 year-old woman BP 190/100; AF on ECG Alert Dysarthric Visual fields full Left facial droop, arm paralyzed, leg drift No sensory loss or neglect
16 Diagnosis Probable ischemic stroke Localization: Syndrome: Severity: Mechanism: Prognosis: Anterior right hemisphere Partial MCA Moderate (NIHSS=8) Probable cardiogenic embolism 45% probability of death or dependency at 1 year
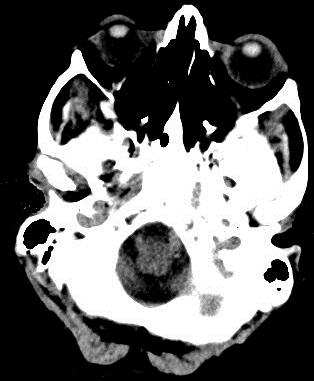


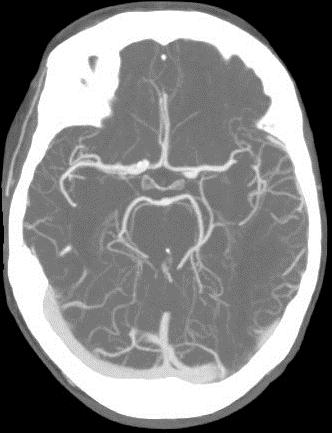
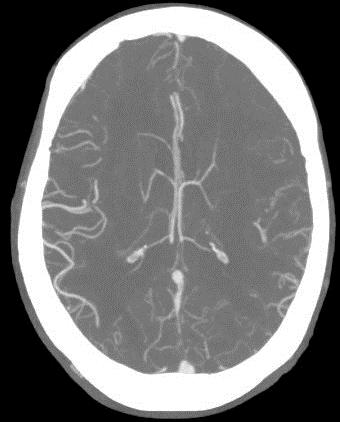
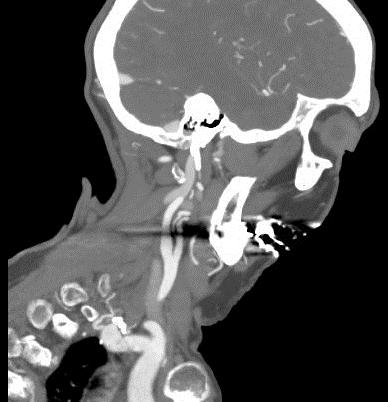
17 Multimodal CT imaging at T+90 mins Non-contrast CT head
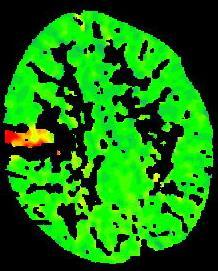
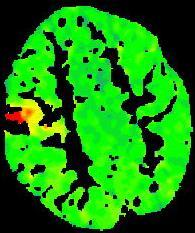
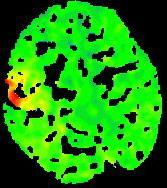
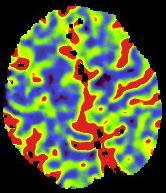
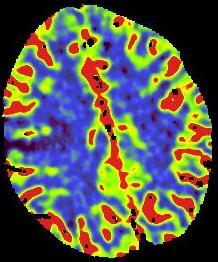

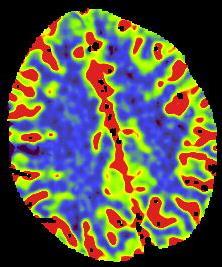
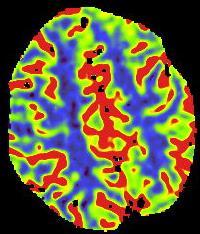
18 Time-to-Peak Cerebral Blood Flow Cerebral Blood Volume
19
20 Labetalol 10 mg IV x2 BP 170/90 PLT 250, INR 1.0 Consent discussion; 7-10% bleeding risk
21 Consent issues US guidelines recommend obtaining informed consent when feasible Canadian Best Practice Recommendations 2018: TPA is considered standard of care. Routine procedures for emergency consent apply. Obtaining consent delays treatment
22 In cases of medical emergency when the patient (or substitute decision maker) is unable to consent, a physician has the duty to do what is immediately necessary without consent.

23 a contemporaneous record (at the time) should be made explaining the circumstances which forced the physician's hand.
24 And If you don t treat, document why and explain to the patient s family


25 ED physicians more often sued for not giving tpa for stroke Liang BA, Zivin JA. Empirical characteristics of litigation involving tissue plasminogen activator and ischemic stroke. Ann Emerg Med. 2008; 52:

26 This is not America
27 or
28 Labetalol 10 mg IV x2 BP 170/90 PLT 250, INR 1.0 Consent discussion; 7-10% bleeding risk TPA started 2 h 20 m after stroke onset
29 Labetalol 10 mg IV x2 BP 170/90 PLT 250, INR 1.0 Consent discussion; 7-10% bleeding risk TPA started 2 h 20 m after stroke onset ~1 hour later: BP 180/100, mute, right gaze preference



30 NCCT 80 mins after start of t-pa Patient deceased 7 hours after stroke onset

31 Predicting brain hemorrhage after t-pa
32 age BP blood glucose creatinine prior antiplatelets stroke severity visible infarct on CT cerebral microbleeds very low cerebral blood volume Karaszewski B, et al. J Neurol Neurosurg Psychiatry 2015; 86:

33 first released December 2006 continuously updated since
34 Acute Ischemic Stroke Treatment Update 5.3.i All eligible patients with disabling ischemic stroke should be offered IV t-pa. Eligible patients are those who can receive treatment within 4.5 hours of stroke onset. [Evidence Level A]
35 Acute Ischemic Stroke Treatment Update 5.3.ii All eligible patients should receive IV t-pa as soon as possible after hospital arrival. [Evidence Level A] Target door-to-needle time <60 min in 90% of treated patients & median 30 min. [Evidence Level B]
36 Update 2018 Thrombolytic Therapy Inclusion Criteria Age >18 <4.5 h since onset (or LSN) Absolute Exclusion Criteria Intracranial hemorrhage (ICH) At risk of major extracranial hemorrhage
37 Update 2018 Thrombolytic Therapy Patients on a Direct Oral Anticoagulant IV t-pa should not be routinely administered In centers with access to specialized tests of DOAC levels and reversal agents, IV t-pa could be considered
38 Update 2018 Thrombolytic Therapy Relative Exclusion Criteria History of ICH Stroke or head trauma in prior 3 months Major surgery in prior 14 days Arterial puncture in prior 7 days Refractory hypertension >180/105

 2. tpa normal dose O: mrs N: Target 4,800 www.")
39 Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED) PI: Craig Anderson, The George Institute for Global Health, Australia P: Ischemic stroke, <4.5 hours, SBP>140 I: 1. Intensive BP lowering (SBP ) 2. tpa low dose (0.6 mg/kg) C:1. Guideline BP lowering (SBP <180) 2. tpa normal dose O: mrs N: Target 4,800
40 Update 2018 Thrombolytic Therapy Relative Exclusion Criteria Blood glucose <2.7 or >22.2 INR >1.7 PTT PLT <100 ASPECTS <6



41 Alberta Stroke Program Early CT Score Examine all the images at the ganglionic and supra-ganglionic levels Take off 1 pt from 10 for every region affected 8-10 Small core 6-7 Moderate core 0-5 Large core aspectsinstroke.com
42 Stroke Thrombolysis in Nova Scotia
43 Stroke Thrombolysis in Nova Scotia 2004/05* 2015^ Ischemic stroke patients Treated with t-pa 3% 13% Arrived in time & treated 11% 40% Median door-to-needle 93 min 68 min *Provincial Stroke Audit ^CVHNS Provincial Stroke Registry
44 Bleeding Complications sich Nova Scotia 2015 (n=183) 8%* sich=symptomatic intracranial hemorrhage *CT confirmed or death within 48 h post-tpa
45 Bleeding Complications sich mech Nova Scotia 2015 (n=183) 8% Systematic Review 2012 (n=3548) 8% IST-3 (n=1515) 7% 1% SITS Registry (n=6483) 7% sich=symptomatic intracranial hemorrhage; mech=major extracranial hemorrhage
46 Update 2018 Thrombolytic Therapy Treatment of Bleeding Complications Insufficient evidence to support use of: cryoprecipitate or fresh-frozen plasma prothrombin complex concentrate platelet transfusion tranexamic acid

47 When Would I Not Treat? Very mild stroke causing non-impairing deficit Very severe stroke in the frail elderly or terminally ill

48 What Do We Do?

49 Insights from 1. Patients who arrive in time but are not thrombolysed 2. Patients whose treatment is complicated by brain hemorrhage Data from QEII Acute Stroke Registry
50 Acute Ischemic Strokes Admitted Through QEII Emergency Department Total N TPA 73 (28%) 66 (25%) 52 (23%) 191 (26%)
51 Acute Ischemic Strokes Admitted Through QEII Emergency Department Arrived <3.5 h but no TPA Total N TPA 73 (28%) 66 (25%) 52 (23%) 191 (26%) 57 (22%) 51 (19%) 50 (22%) 158 (21%)
52 Lysed cf Not- lysed (1/3) TPA No TPA TPA No TPA TPA No TPA Age % men % living at home % living alone
53 Lysed cf Not- lysed (1/3) TPA No TPA TPA No TPA TPA No TPA Age % men % living at home % living alone Untreated patients older
54 Lysed cf Not- lysed (2/3) % Prior: TPA No TPA TPA No TPA TPA No TPA stroke cognition dependency
55 Lysed cf Not- lysed (2/3) % Prior: TPA No TPA TPA No TPA TPA No TPA stroke cognition dependency Untreated patients older; and more likely to have prior stroke, cognitive and functional impairment
56 Lysed cf Not- lysed (3/3) TPA No TPA TPA No TPA TPA No TPA % ASP activated % Mild stroke % Moderate stroke % Severe stroke
57 Lysed cf Not- lysed (3/3) TPA No TPA TPA No TPA TPA No TPA % ASP activated % Mild stroke % Moderate stroke % Severe stroke Untreated patients older; more likely to have prior stroke, cognitive and functional impairment, and mild stroke; and less likely to be code strokes
58 Intracerebral hemorrhage after TPA at the HI
59 Intracerebral hemorrhage after TPA at the HI Total TPA [no EVT] ICH, n (%) 3 (4.8) 1 (1.9) 4 (10) 8 (5.2)
60 TPA [No EVT] ICH No ICH n=8 n=148 Age (median) % men % prior stroke % prior cognition % prior dependency Bleeders more likely to cognitively impaired, dependent
61 TPA [No EVT] ICH No ICH n=8 n=148 LSN to TPA (median mins) % AF % mild stroke 0 5 % moderate stroke % severe stroke Bleeders more likely to cognitively impaired, dependent, in AF
62 TPA [No EVT] ICH No ICH Stroke syndrome n=8 n=148 % MCA % Lacunar Bleeders more likely to cognitively impaired, dependent, in AF, with a lacunar stroke
63 TPA [No EVT] ICH No ICH n=8 n=148 % death in hospital % survivors dependent at discharge 80 51
64 Last slide No useful clinical tool to predict who will bleed after t-pa Guidelines are helpful! Mild strokes are difficult! Frailty, comorbidity, impaired cognition, and functional dependency may be reasons not to treat There are worse things than dying from a severe stroke

65 Thanks!
66 Symptomatic intracranial hemorrhage in systematic review of stroke t-pa trials Treated within 3 h All 5 trials before IST-3 IST-3 All 6 trials (n=1779) Treated between 3 to 6 h OR 4.6 ( ) All 6 trials before IST-3 IST-3 All 7 trials (n=4965) OR 3.7 ( ) Lancet 2012; 379:
67 Update 2018 Thrombolytic Therapy Treatment of tpa-induced Angioedema Stop t-pa Airway management Hydrocortisone 100 mg IV Diphenhydramine 50 mg IV Ranitidine 50 mg IV [risk of BP and ICH with nebulized epinephrine]
68 Door to Image/Needle (minutes) Number of patients Stroke Thrombolysis in Nova Scotia N, Door-to-CT & Door-to-Needle Times (median, IQR) Calendar Year 0 Number treated 0-3hrs from symptom onset Median door to image Number treated >3hrs from symptom onset Median door to needle

69 Stroke Thrombolysis in Helsinki Meretoja A, et al. Neurology. 2012; 79:
70 Content Give em the juice Summary of trial data (Emberson paper; Lees ESOC presentation) mild, moderate and severe strokes benefit timing difficulty predicting ICH (Will Whiteley) Canadian Stroke Best Practice Recommendations Local data ischemic stroke patients who arrive in time but are not treated treated patients who bled CVHNS data on bleeding Thrombolysis in the EVT era (TNK_mdhEditorial2018)
Acute Stroke Care. Steve Phillips Division of Neurology Dalhousie CPD Aberdeen Hospital, New Glasgow 11 th April 2018
 Acute Stroke Care DALHOUSIE UNIVERSITY Department of Medicine Steve Phillips Division of Neurology Stephen.Phillips@nshealth.ca Dalhousie CPD Aberdeen Hospital, New Glasgow 11 th April 2018 HEALTH For
Acute Stroke Care DALHOUSIE UNIVERSITY Department of Medicine Steve Phillips Division of Neurology Stephen.Phillips@nshealth.ca Dalhousie CPD Aberdeen Hospital, New Glasgow 11 th April 2018 HEALTH For
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Acute Stroke Management 2009
 Acute Stroke Management 2009 Saving the Brain Conference Royal York Hotel January 24, 2009 Frank L. Silver, MD, FRCPC Director, Toronto West Stroke Program Professor of Medicine (Neurology) University
Acute Stroke Management 2009 Saving the Brain Conference Royal York Hotel January 24, 2009 Frank L. Silver, MD, FRCPC Director, Toronto West Stroke Program Professor of Medicine (Neurology) University
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience
 Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Role of recombinant tissue plasminogen activator in the updated stroke approach
 Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Acute ischemic stroke is a major cause of morbidity
 Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017
 Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017 Dr André Peeters Service de Neurologie Cliniques Universitaires Saint-Luc / U.C.L. 1200 BRUXELLES Introduction 1. Aim NOACS
Boehringer-Ingelheim satellite symposium Ligue cardiologique belge 13/05/2017 Dr André Peeters Service de Neurologie Cliniques Universitaires Saint-Luc / U.C.L. 1200 BRUXELLES Introduction 1. Aim NOACS
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University
 Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University Disclosures Research Grants and speaking fees St. Jude
Stroke Prevention in AF: How will it change in the next 5 years? Jeff Healey MD, MSc, FHRS Population Health Research Institute McMaster University Disclosures Research Grants and speaking fees St. Jude
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II
 Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Inclusion criteria Cautionary inclusion Exclusion criteria 1. Diagnosis of ischemic stroke causing measurable neurological deficit.
 Guidelines for the use of IV recombinant tissue plasminogen activator (rt-pa), Endovascular Thrombectomy (EVT), or rt-pa+evt in the treatment of acute ischemic stroke at Kingston General Hospital Rationale
Guidelines for the use of IV recombinant tissue plasminogen activator (rt-pa), Endovascular Thrombectomy (EVT), or rt-pa+evt in the treatment of acute ischemic stroke at Kingston General Hospital Rationale
The tpa Cage Match. Disclosures. Cage Match. Cage Match 1/27/2014. January 8, Advisory Boards
 The tpa Cage Match January 8, 2014 Andy Jagoda, MD, FACEP Professor and Chair of Emergency Medicine Mount Sinai School of Medicine New York, New York Advisory Boards Disclosures Astra Zeneca, Pfizer, CSL
The tpa Cage Match January 8, 2014 Andy Jagoda, MD, FACEP Professor and Chair of Emergency Medicine Mount Sinai School of Medicine New York, New York Advisory Boards Disclosures Astra Zeneca, Pfizer, CSL
NOAC trials for AF: A review
 NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
First Year of 24/7 ASU and Stroke Thrombolytic Service
 First Year of 24/7 ASU and Stroke Thrombolytic Service Kwan M, Chang C, Mak W, Ip F, Chang R, Pang S, Hon S, Ho SL, Cheung RTF Division of Neurology, Department of Medicine, Queen Mary Hospital. IV Thrombolysis
First Year of 24/7 ASU and Stroke Thrombolytic Service Kwan M, Chang C, Mak W, Ip F, Chang R, Pang S, Hon S, Ho SL, Cheung RTF Division of Neurology, Department of Medicine, Queen Mary Hospital. IV Thrombolysis
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The HEMORR 2 HAGES, ATRIA and the HAS-BLED bleeding risk prediction scores in anticoagulated atrial fibrillation patients : The AMADEUS study
 The HEMORR 2 HAGES, ATRIA and the HAS-BLED bleeding risk prediction scores in anticoagulated atrial fibrillation patients : The AMADEUS study Apostolakis S 1, Lane DA 1, Buller H 2, Lip GY 1 1 University
The HEMORR 2 HAGES, ATRIA and the HAS-BLED bleeding risk prediction scores in anticoagulated atrial fibrillation patients : The AMADEUS study Apostolakis S 1, Lane DA 1, Buller H 2, Lip GY 1 1 University
Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial
 Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial Christopher Granger, John Alexander, Michael Hanna, Jerry Wang, Puneet Mohan, Jack Lawrence, Elaine Hylek, Jack Ansell,
Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial Christopher Granger, John Alexander, Michael Hanna, Jerry Wang, Puneet Mohan, Jack Lawrence, Elaine Hylek, Jack Ansell,
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia