I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
|
|
|
- Augustus Gregory
- 5 years ago
- Views:
Transcription

1 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o r P e a c e H e a l t h S a c r e d H e a r t M e d i c a l C e n t e r R i v e r B e n d
2 Objectives Know the basic pathophysiology of acute stroke subtypes Understand the time sensitive nature of acute stroke Review inter-hospital transfer guidelines to mediate transport risks Explain the new ASA stroke guidelines Explore new proposals for triage and stroke systems of care
3 Stroke Definitions: Stroke = Acute disruption of blood flow to the brain leading to focal neurologic deficits TIA (transient ischemic attack) =acute disruption of blood flow of the brain leading to focal neurological symptoms last less than 24 hours ( MOST CONSIDER TIA when less than ONE HOUR duration)
4 Deficits: Acute Stroke (What do you see?) Unilateral (though not always) weakness Unilateral sensory deficit Visual deficits (blindness, gaze palsy, double) Speech (slurred a motor dysfunction) Language (aphasia damage to the brain s speech center) Ataxia (lack of coordinated movement) Cognitive impairment Like real estate Location, Location, Location
 Intracerebral Hemorrhage (59%)")


5 Cerebrovascular Disease: Pathogenesis Hemorrhagic Stroke (17%) Intracerebral Hemorrhage (59%) Subarachnoid Hemorrhage (41%) Clinical Presentation similar to ischemic stroke Clinical Presentation WORSE HEADACHE OF MY LIFE Albers GW, et al. Chest. 1998;114:683S-698S. Rosamond WD, et al. Stroke. 1999;30:

6 Cerebrovascular Disease: Pathogenesis Ischemic Stroke: 83%



7 Types of Strokes Large artery territory CT scan initially normal CT scan shows changes after 6 hours
 Language deficit if in dominant hemisphere Gaze palsy eyes directed towards side of AIS")
8 Types of Strokes (Middle Cerebral Artery MCA) The most common artery occluded in AIS can be proximal or from carotid circulation. Features: Motor/Sensory Deficit: face, arm, leg Speech deficit dysarthria (slurred speech) Language deficit if in dominant hemisphere Gaze palsy eyes directed towards side of AIS Blindness visual field cut (homonymous hemianopsia)

9 Lacunar Strokes These strokes are ischemic in nature. Occurs in the small penetrating arteries of the brain. Presentation affects the arm, leg, and face, equal to all areas.

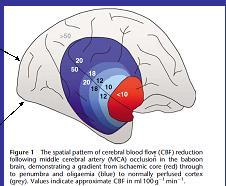


10 PENUMBRA (That tissue surrounding the infarct that is salvageable, but at risk.)

11 Early EMS Notification of Possible Stroke Patient FAST/Cincinnati Stroke Scale to assess a patient for stroke: Facial droop Arm drift Speech Time Sensitive

12 HOW ARE WE DOING?

13 OREGON Percentage of Ischemic Stroke Patients Receiving any Reperfusion Therapy

14 RAPID ADVANCEMENT IN STROKE CARE
15 INTERHOSPITAL TRANSFER- DRIP AND SHIP Rapid Initial Report and Assessment Age, name, DOB, pertinent past history Neurological deficits ( NIHSS if available) Last Seen Well (witnessed or non-witness onset) IV Access ( 20 gauge) at least one above the wrist VS Family contact cell number


16 ACTIVASE- tpa (1mg/ml) Ischemic stroke dose- 0.9mg/kg iv First 10% given as bolus over 1 minute, the remainder over 60 minutes ( maximum dose 90mg) TPA TOTAL DOSE: 72 mg BOLUS DOSE: 7.2 mg INFUSION DOSE: 64.8 mg AMOUNT DISGARDED: 28 mg


17 TPA infusions- Do and Don'ts Avoid transferring pumps but if necessary take care to minimize drug loss and minimize infusion interruptions When pump alarms to signify infusion complete WATCH for the drip chamber to empty, to confirm tpa bag is empty Remove tpa bag( or bottle) and hang 50mL normal saline at same rate as tpa. Note: There is still tpa in the tubing that needs to be infused. NS
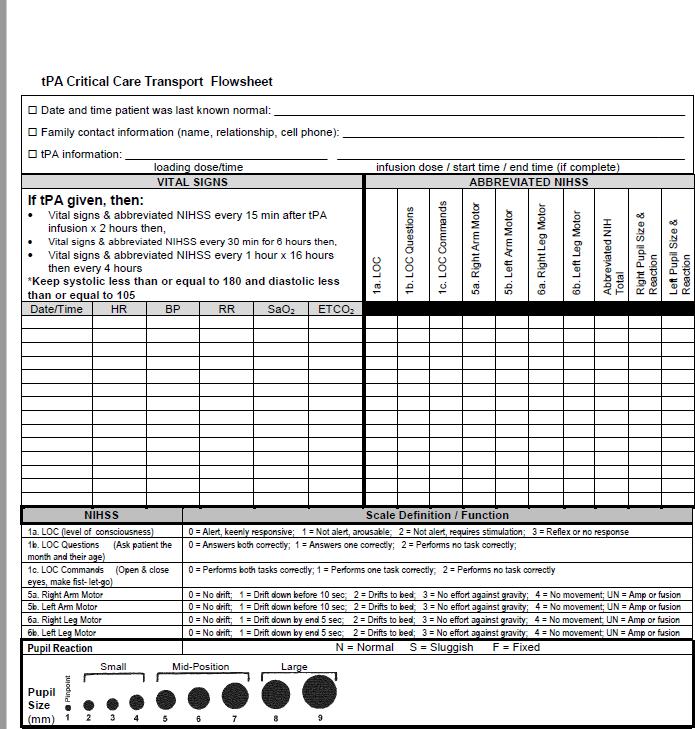
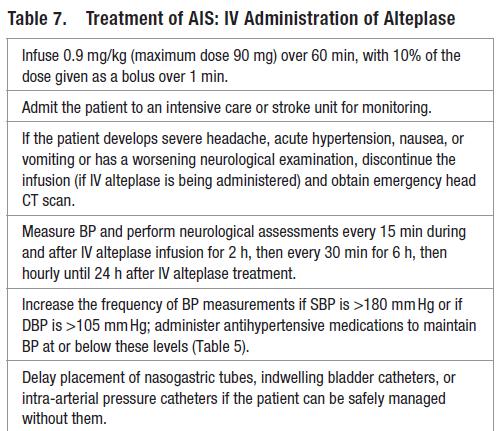

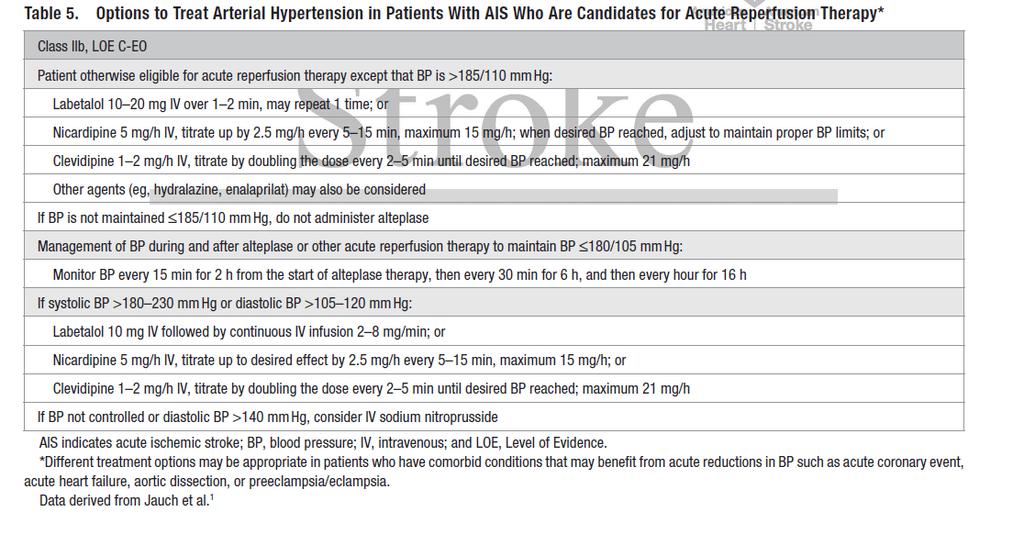
18 < 180/105
19
20 Case #1 72 year old woman present to her local hospital with aphasia and mild right sided weakness onset In ED, BP 220/110. Head CT was normal. CTA showed a left middle cerebral artery thrombus. She was started on a nicardipine drip to control her BP. IV tpa was started at Upon request, you arrive at 0930 to transfer the patient to the closest endovascular center.
21 En Route VS: BP 110/50 P 100, R 12, sat 100% Neuro exam: Awake, alert, calm but globally aphasic (can t speak or follow commands), but now the right arm is completely paralyzed Next Step? Stop Nicardipine- Allow BP to rise ( but not over 180/105) Call receiving hospital with changes and await additional instructions

22 INTERHOSPITAL TRANFER DRIP AND SHIP Complications En Route Secondary Hemorrhage Allergic reaction BP and/or exam fluctuations Aspiration


23 Signs of secondary intracranial hemorrhage 1. Sudden Severe headache 2. New onset vomiting 3. Sudden decline in neurological condition 4. Sudden spike in BP Secure Airway Stop vomiting Control BP Call Receiving facility


24

25 Prevent Aspiration
26 Most frequent errors NO family contact obtained Failure to verify total and remaining dose Lost tpa in tubing Long tpa interruptions Lack of BP checks Lack of Neuro checks Failure to maintain BP within parameters Failure to call ahead with status changes
27 Case # 2 32 year old previously healthy man presents to her local hospital with sudden severe headache without a history of trauma. Initially his BP is elevated 240/120. Head CT reveals a head bleed. He has severe headache but GCS is 14 and he is neurologically intact. He received one dose of Labetolol 20mg iv and his BP drops to 160/80. You are transferring a higher level of care to a hospital 2 hours away
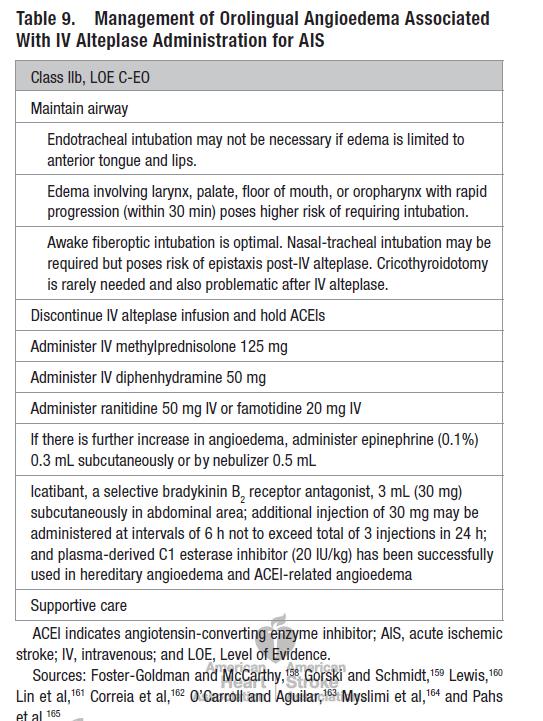
28 Covered under head trauma guidelines What kind of head bleed? Intracerebral hemorrhage (ICH) Focal symptoms, risk for seizure, hydrocephalus or worsening neurological symptoms Maintain BP < 150/ 90, q 5 BP until stable than 15 min Subarachnoid hemorrhage (SAH)- Usually non-focal, severe headache and meningismus Maintain BP < 160/90, q 5 BP until stable then 15 min Pain control, low stimulation, avoid Valsalva and vomiting Re- bleeding (aneurysm rupture) risk is high with poor outcomes Subdural Hematoma or Other traumatic hemorrhage

29
30 VS: BP 175/ 95 P100 En Route? BP Goal ( for SAH < 140/90) Neuro examination- Sleepy but arouses quickly, is oriented flows commands and moves all 4 extremities Then. Suddenly he begins vomiting profusely

31
32 Emergent stabilization ABCs Rapid Sequence intubation CALL receiving facility with change BP control Vomiting control Seizure Control Mannitol


33 ELVO STEMI

34 LAST SEEN WELL < 6 hours
35
36 b


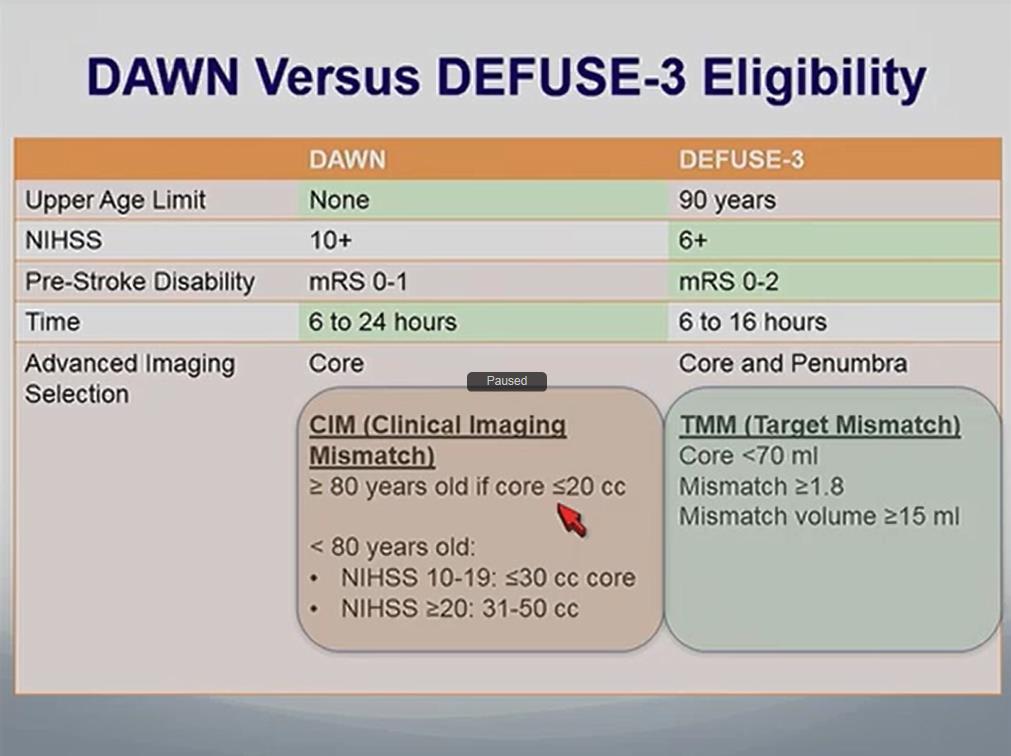
37 within 6-24
38

39 US Stroke Centers and Endovascular Treatment Centers

40 Oregon Hospitals Endovascular Treatment Centers Portland Metro Kaiser Sunnyside Legacy Emanuel Legacy Meridian Park OHSU PeaceHealth SW- Vancouver WA Providence Portland Providence St Vincent Central and Southern Oregon PeaceHealth Riverbend- Springfield Providence Medford St Charles- Bend


41 LKW to IA 349 min (5.8 hrs)
42


43 What is an ELVO? EMERGENT LARGE ARTERY OCCLUSION
44 Cortical Findings
45

46 WHY NOT JUST TRANSFER ALL STROKES TO ENDOVASCULAR TREATMENT CENTER? Iv tpa remains the mainstay for most ischemic strokes LVO make up 10 % of all acute stroke Many tertiary stroke center have capacity issues Our ability to predict LVO using in-the-field scales is limited Long transport times could exclude some patient from getting iv tpa ANSWER? DEVELOP LOCAL AND REGIONAL TRIAGE PROTOCOLS

47 PORTLAND METRO
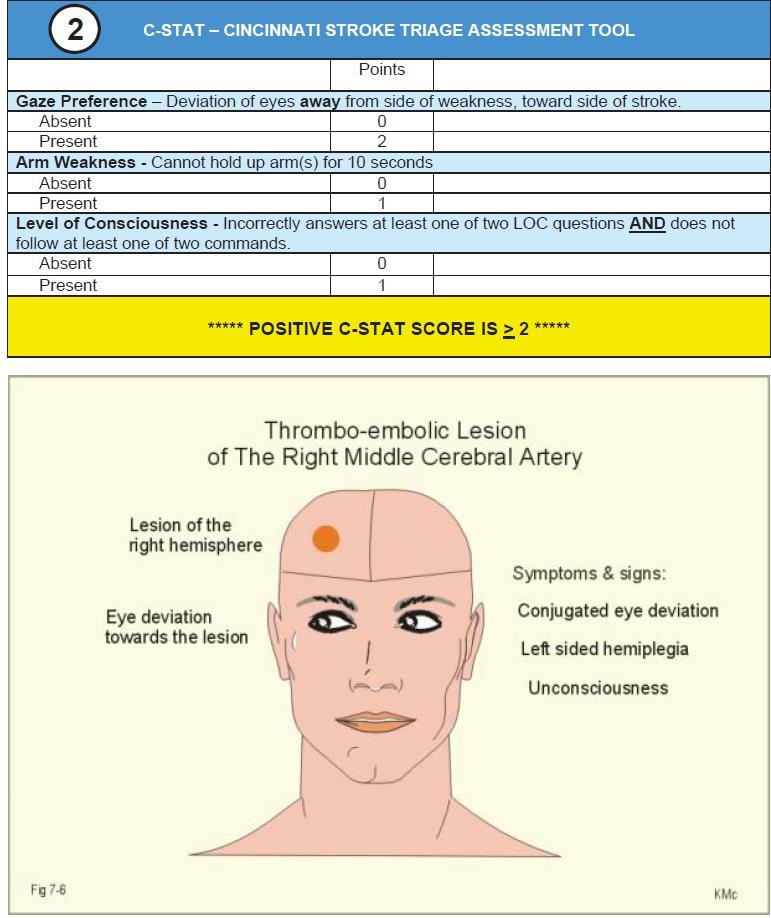
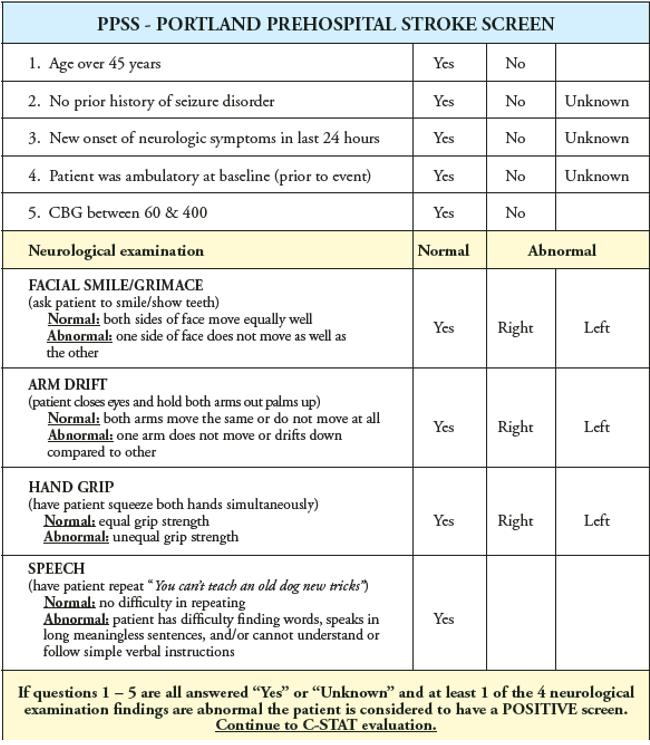
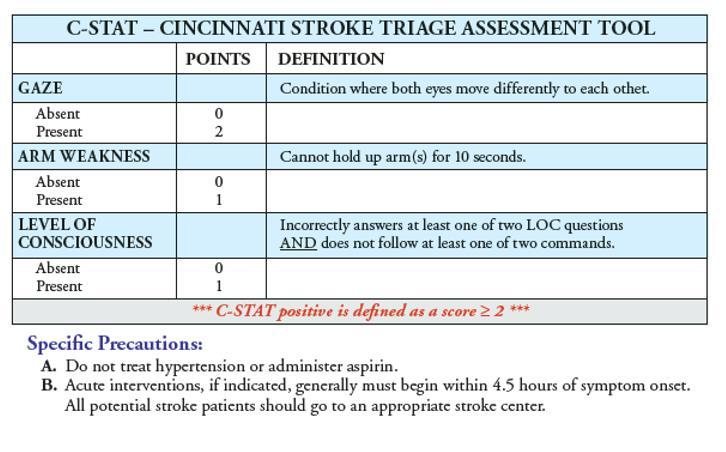
48 Case # 3 13:10 79 y/o healthy woman while walking with her husband had a witnessed collapsed with left hemiplegia and rightward gaze deviation activated 1318 EMS arrives Primary survey and VS ok Cincinnati stroke scale is positive? CSTAT? Where to transport
49 Case # 3 WILL PATIENT ARRIVE at EVT center within 2 hours from LSW? 13:24 Medical air transport contacted 13:25 Patient loaded in ambulance and began driving to rendezvous location (high school football field) 13:47 Rendezvoused with helicopter 1404 Lift-0ff 14:25 Helipad Arrival at EVT center ED 14:34 ED arrival NIHSS 19 Cortical signs: Right-sided eye deviation Left-sided hemiplegia Neglect Left-sided visual field cut 1442 CT: Hyperdense MCA 1443 CT Angiography: Right ICA/MCA occlusion 14:57 IV tpa (Door to Needle: 23 minutes; Onset to Needle Time 1 hour 47 minutes) 14:49 ELVO Alert initiated


50 15:08 Cath Lab arrival Case # 3 15:10 Groin puncture (door to groin: 36 minutes) Right ICA terminus occlusion Second pass revascularization 1536
 Discharged home day 3 with mild residual")
51 Case # 3 LSW to revascularization (2 hours and 26 minutes) Discharged home day 3 with mild residual neglect


52 Acute ischemic strokes patient who are C-STAT positive and up to 24 hours from LSW should be treated as a Code 3. All C-STAT positive patients should receive IV tpa if eligible.







53 ACUTE STROKE CHAIN OF SURVIVAL Patient has sudden stroke symptoms 911 dispatch EMS transport Stroke Ready Hospital ED assess Head CT Iv tpa initiated Transport to EVT Center CTA/CTP To Cath lab Mechanical thrombectomy Time 1 hr 2 hrs 3 hrs

54 TIME IS BRAIN

55 Elaine Skalabrin, MD-Stroke Program Medical Director Diane Soik, NP, MSN,ANP- Stroke Program Manager Questions RESOURCES ONLINE:

56 Wednesday, March 21, 2018 from Next EMS Grand Rounds Trauma Update-TXA, Whole blood in EMS, tourniquets, Stop-the-bleed Free sign up at

57 Thanks for Attending
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
ELVO update. Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon
 ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
ELVO update Michael Wilder, MD Director, Neurointerventional Program PeaceHealth Sacred Heart Springfield, Oregon Riverbend 24/7 thrombectomy ELVO alert Access PH PACU Anesthesia Goyal et al. Lancet. 2016
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Shands at the University of Florida Stroke Program
 Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Shands at the University of Florida Stroke Program The only Comprehensive Stroke Center in north central Florida as designated by the Florida Agency for Health Care Administration. To transfer a stroke
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
EMS Stroke Care in the Fox Valley
 EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
EMS Stroke Care in the Fox Valley MARK D. WESTFALL, D.O., FACEP, FACP MEDICAL DIRECTOR, GOLD CROSS AMBULANCE SERVICE EMERGENCY PHYSICIAN, THEDA CLARK MEDICAL CENTER Objectives Introduce / Review our Regional
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Slide 1. Slide 2. Slide 3 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER DISCLOSURES MY PATH TO EMS
 Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Slide 1 EMS STROKE CARE AND CSTAT OREGON STROKE NETWORK CONFERENCE 2018 SHAWN WOOD, CLINICAL MANAGER METRO WEST AMBULANCE Slide 2 DISCLOSURES No Financial Conflicts. I work as the Clinical Manager for
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare
 Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Top 5 Big Things in Acute Stroke Care! Raymond W. Grams II, DO Vascular Neurology Stroke Medical Director DRMC, Intermountain Healthcare Late Time Window Endovascular Trials 48.6% WITH intervention vs
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field. Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke
 Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Urgent Care/Triage & Transport of the Severe Stroke Patient in the Field Robert Knight, BSN, RN, CEN, NRP, CCEMT/P INTEGRIS TeleStroke Suggested Protocols Suggested protocols are just that. They are not
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Statewide Acute Stroke Triage The Washington Story
 Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
Statewide Acute Stroke Triage The Washington Story David Tirschwell, MD, MSc Medical Director of Comprehensive Stroke Care Professor, Department of Neurology UW Medicine Comprehensive Stroke Center at
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
ABNORMAL STROKE EXAM FINDINGS:
 Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Stroke Assessment Scenario Case Information PATIENT INFORMATION: 68-year-old male patient complaining of left sided weakness and an unsteady gait. Reported last normal time 3 minutes prior to EMS arrival
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools
 Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Getting the Right Stroke Patient to the Right Hospital: Pre-hospital Assessment Tools Francis X Guyette, MD, MPH Associate Professor of Emergency Medicine University of Pittsburgh School of Medicine Medical
Chapter 18. Objectives. Objectives 01/09/2013. Altered Mental Status, Stroke, and Headache
 Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
Chapter 18 Altered Mental Status, Stroke, and Headache Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
When Not To Give TPA Steve Phillips Division of Neurology
 When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL. StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian
 PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
PREHOSPITAL ACUTE STROKE TRIAGE TIME: A PRAGMATIC TRIAL StrokeNet SC Call November 8, 2017 Jason McMullan, Opeolu Adeoye, Nerses Sanossian STATUS UPDATE Original presentation to ASWG 6/2017 Reviewed at
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 3 September 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Overview. Introduction. New Interventions for Acute Stroke. New Approaches to hemorrhagic Strokes
 Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
Overview New Interventions for Acute Stroke Paula Eboli, MD Department of Neurosurgery Rockwood Clinic, Deaconess Hospital Introduction New Approaches to hemorrhagic Strokes New Approaches to Ischemic
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
The Language of Stroke
 The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
The Language of Stroke Examination / Imaging / Diagnosis / Treatment Dr Suzanne Busch A lot of letters! CBF CVA ICH CVD CBV DWI US MRI/MRA CAA CTA CTP ICA MCA SAH WMD TIA MCA Agnosia A lot of big words!
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience
 Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
Code Stroke Optimizing Stroke Care in the Field: The Alberta Experience June 1st, 2018 Thomas Jeerakathil BSc, MD, MSc, FRCP(C) Professor Division of Neurology University of Alberta Northern Stroke Lead
11/2/2016. The Acute Phase of Cerebrovascular Accident. L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV
 The Acute Phase of Cerebrovascular Accident L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV 1 Faculty Disclosure Information 1. SPEAKER: L. Michael Peterson, D.O.
The Acute Phase of Cerebrovascular Accident L. Michael Peterson, DO Medical Director HealthNet Aeromedical Services Charleston, WV 1 Faculty Disclosure Information 1. SPEAKER: L. Michael Peterson, D.O.
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University