Management of Traumatic Brain Injury (and other neurosurgical emergencies)
|
|
|
- Britney Walton
- 5 years ago
- Views:
Transcription
1 Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019

2 Greetings from Michigan!
3 Objectives for Today s Discussion How to manage refractory intracranial hypertension in the OR Intraoperative aneurysm rupture Major hemorrhage in spine surgery Risks of new minimally invasive spine procedures I have no financial disclosures

4 This is what it s all about A Few Definitions: Intracranial pressure = ICP Mean arterial pressure = MAP Cerebral perfusion pressure = CPP = MAP-ICP TBI = traumatic brain injury


5 There are many reasons for intraoperative intracranial hypertension

6 Neurosurgery 2017; 80:6-15

7 Monro-Kellie Doctrine Intracranial Contents Brain CSF Blood

8 The Intracranial Pressure-Volume Curve Miller s Anesthesia 2015


9 Determinants of cerebral blood flow under normal conditions Miller s Anesthesia 2015 Cottrell and Young s Neuroanesthesia 2010
10 When should we treat intracranial hypertension? It is the burden of intracranial hypertension that affects outcome ICP should be monitored in unconscious (or sedated) patients with abnormal head CT BTF would suggest treat for ICP 22 mmhg ICP monitoring and CPP management have unclear effect on long-term outcomes This speaks to the need to individualize therapy


11 Stepwise approach to ICP management in the OR
12 OR checklist and first line therapies for intracranial hypertension Is cerebral venous drainage optimized? Are respiratory parameters okay? Normocapnia Normoxia Ventilatory pressures Adapted from Drummond, Patel & Lemkuil Miller s Anesthesia 2015

13 OR checklist and first line therapies for intracranial hypertension Is the patient s blood pressure adequate? Rhoney Crit Care Clinics 2006 Miller s Anesthesia 2015
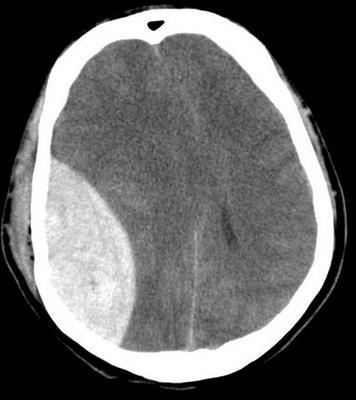
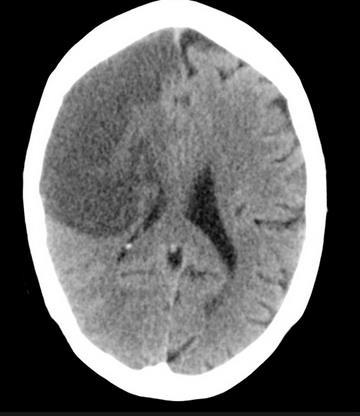
14 OR checklist and first line therapies for intracranial hypertension Are there cerebral vasodilators that can be eliminated? Are metabolic requirements increased for unrecognized reasons? Can anesthetic be altered to increase metabolic suppression? Is there intracranial pathology that is not visible? Hematoma CSF Venous obstruction or infarction
15 When first line measures fail to help Osmotic diuresis Mannitol (2ml/kg of 20% solution or gm/kg) Hypertonic saline (HTS 2ml/kg of 3% solution) Hyperventilation CSF drainage (AV Lele, J Neurosurg Anesthesiol 2017) Optimization of blood pressure
16 Hypertonic saline (HTS) and Mannitol: Establish osmotic gradient across intact blood brain barrier Both initially produce increase in cardiac output and improved laminar flow in microcirculation Both may have anti-inflammatory effects Very similar osmolarity (M = 1098, HTS = 1026 mosm/l)
17 Advantages of each osmotic agent: Mannitol Easily accessed Easily administered Rapid onset Familiarity Hypertonic saline Probably more effective than mannitol daily and cumulative ICP burden Supports intravascular volume Rapid onset and sustained effect May be effective when other rx have failed Possibly more effective at CPP and brain oxygenation

18 Disadvantages of each osmotic agent: Mannitol May crystallize Potential for rebound in ICP Intravascular volume depletion Hypertonic saline May require central access Less familiarity with drug Caution with abnormal Na values 3, 7.5, 23.4% available 1.8% for peripheral administration

19 HTS provides improved ICP control compared to mannitol A Ali, JNA ml/kg 20% mannitol vs. 3% HTS
20 Effects of 3 ml/kg 20% Mannitol and 3% HTS Hernandez-Pelazon Br J Neurosurgery 2016
21 Third line measures for refractory intracranial hypertension: Hypothermia Metabolic suppression Decompressive hemicraniectomy (DC)


22 Decompressive Hemicraniectomy (DC): Not currently recommended by Brain Trauma Foundation* Is effective at reducing ICP and time in ICU If DC planned flap 12 x 15 cm recommended Does improve survival and functional status for malignant stroke in patients 60 years Courtesy of Dr. Aditya Pandey University of Michigan Neurosurg Clin N Am 28 (2017)
23 Intraoperative aneurysm rupture

24 In advance of high risk aneurysm clipping consider: Type and cross 2 u PRBC Large bore IV access (in addition to arterial line) Pacing pads on chest and attached to defibrillator/pacer Adenosine mg/kg available in OR CMRO 2 depressant agents available (propofol) Pressors at hand Physiologic monitoring including EEG very helpful

25 In case of rupture: Call for help Discuss options with surgeons including adenosine or hypotension with CMRO 2 depressing agent until temporary clip placed Once clip placed consider volume replacement and/or induced hypertension Anesth Pain Med 2012; 7: 55-58

26 Major bleeding during spine surgery

27 PMTSS: The Prediction Model of Transfusion in Spine Surgery Anesthesiology 2009;110:
28 Strategies for major bleeding during spine surgery Adequate venous access Appropriate positioning on bolsters Role of colloid? Tranexamic acid (TXA) mg/kg bolus followed by 1-10 mg/kg/hr. Consider baseline thromboelastometry (TEG or ROTEM) PRBC:FFP = 1:1, follow platelets closely Transfusion trigger depends on rate of blood loss Goal hematocrit vs. transfusion trigger


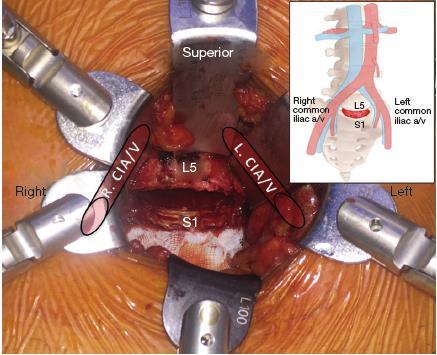
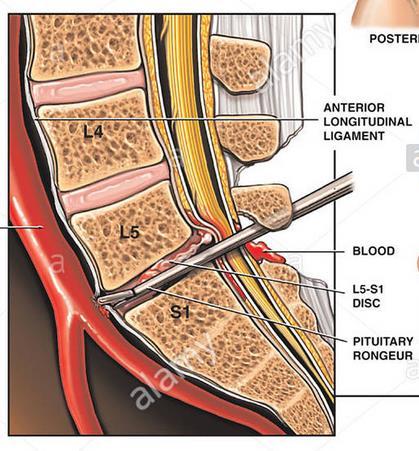
29 Iliac bifurcation at L3-4 (Images from Synthes Spine Technique Module)
, Transforaminal and Posterior Lumbar Interbody")
30 Interbody fusion approaches Journal of Spine Surgery 2015 Anterior, Lateral, Oblique (retroperitoneal, Anterior To Psoas), Transforaminal and Posterior Lumbar Interbody Fusion

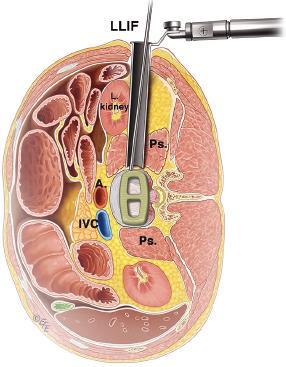
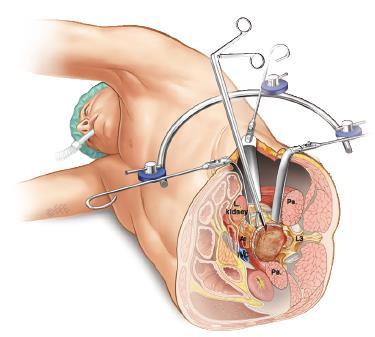
31 OLIF ALIF LLIF
32 In Conclusion: Management of ICP should follow logical physiologic principles in stepwise fashion Neurosurgical procedures are becoming increasingly complex on increasingly sick patients Some technical advances including endovascular and minimally invasive spine procedures are helpful given our aging patient population
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS
 Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED
 ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient
 Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient David J. Stone MD I. Introduction and General Issues The focal point in the care of neurosurgical patients is the control
Physiology and Monitoring of Intravascular Volume Status in the Neurosurgical Patient David J. Stone MD I. Introduction and General Issues The focal point in the care of neurosurgical patients is the control
ICP. A Stepwise Protocol
 ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along?
 Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Preoperative assessment of ureter using double-phase contrast enhanced CT. Shunsuke Fujibayashi
 EUROSPINE 2015 SEPT.2-4, COPENHAGEN, DENMARK Preoperative assessment of ureter using double-phase contrast enhanced CT Shunsuke Fujibayashi Bungo Otsuki, Hiroaki Kimura, Shuichi Matsuda Department of Orthopaedic
EUROSPINE 2015 SEPT.2-4, COPENHAGEN, DENMARK Preoperative assessment of ureter using double-phase contrast enhanced CT Shunsuke Fujibayashi Bungo Otsuki, Hiroaki Kimura, Shuichi Matsuda Department of Orthopaedic
Drug Choices and Outcomes in Neuroanesthesia
 Robert Breeze, MD Daniel Janik, MD Benjamin Scott, MD NEUROANESTHESIA PANEL CRASH 2015 Your Anesthetic? Balanced technique opiate/volatile? Nitrous/narcotic technique? TIVA propofol/opiate Does choice
Robert Breeze, MD Daniel Janik, MD Benjamin Scott, MD NEUROANESTHESIA PANEL CRASH 2015 Your Anesthetic? Balanced technique opiate/volatile? Nitrous/narcotic technique? TIVA propofol/opiate Does choice
Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester, MA.
 Shobana Rajan, M.D. Staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester, MA. This
Shobana Rajan, M.D. Staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester, MA. This
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading)
") 1 Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading) The least I should read Anesthetic agents Neuroprotection Carotids Aneurysms Avms TUMors Awake craniotomy Trauma/emergencies
1 Stanford Neuroanesthesia Syllabus: Journal Article Directory (click on section heading) The least I should read Anesthetic agents Neuroprotection Carotids Aneurysms Avms TUMors Awake craniotomy Trauma/emergencies
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery
 Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Index Note: Page numbers of article titles are in boldface type. A Ablation, radiofrequency, anesthetic considerations for, 479 489 Acute aortic syndrome, thoracic endovascular repair of, 457 462 aortic
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Is the use of hypertonic saline effective in reducing intracranial pressure after traumatic brain injury?
 Is the use of hypertonic saline effective in reducing intracranial pressure after traumatic brain injury? Clinical bottom line Hypertonic saline appears to be effective in reducing intracranial pressure
Is the use of hypertonic saline effective in reducing intracranial pressure after traumatic brain injury? Clinical bottom line Hypertonic saline appears to be effective in reducing intracranial pressure
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Emergency Management of the Head
 Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Emergency Management of the Head Trauma Patient Adam Schneider, DVM Neurology and Neurosurgery Blue Pearl 9500 Marketplace Rd Fort Myers Head trauma Common cause of morbidity and mortality 25% of blunt
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Anterior and Lateral Lumbar Minimally Invasive Approaches: How to Choose
 Anterior and Lateral Lumbar Minimally Invasive Approaches: How to Choose Lukas P. Zebala, MD Assistant Professor Washington University School of Medicine St. Louis, MO Disclosures Consultant: K2M, Inc.
Anterior and Lateral Lumbar Minimally Invasive Approaches: How to Choose Lukas P. Zebala, MD Assistant Professor Washington University School of Medicine St. Louis, MO Disclosures Consultant: K2M, Inc.
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
Acute Stroke Treatment: Mechanical Thrombectomy
 Acute Stroke Treatment: Mechanical Thrombectomy Rudy Noppens Department of Anesthesiology & Perioperative Medicine CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure
Acute Stroke Treatment: Mechanical Thrombectomy Rudy Noppens Department of Anesthesiology & Perioperative Medicine CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure
Cold Topic: Advanced Treatment Modalities in Acute Stroke
 Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
Cold Topic: Advanced Treatment Modalities in Acute Stroke William M. Coplin, MD, FCCM Associate Prof, Neurology & Neurosurgery Wayne State University Chief, Neurology Medical Director, Neurotrauma & Critical
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
ANESTHESIA FOR SUPRATENTORIAL TUMOR
 ANESTHESIA FOR SUPRATENTORIAL TUMOR Diana Christine Lalenoh, MD, PhD, Neuroanesthesiologist consultant, Obstetric Anesthesia consultant Department of Anesthesiology & Intensive Care, Medical Faculty of
ANESTHESIA FOR SUPRATENTORIAL TUMOR Diana Christine Lalenoh, MD, PhD, Neuroanesthesiologist consultant, Obstetric Anesthesia consultant Department of Anesthesiology & Intensive Care, Medical Faculty of
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Quality Metrics. Stroke Related Procedure Outcomes
 Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Quality Metrics Stroke Related Procedure Outcomes Below is a description of some of the stroke-related procedures performed at St. Dominic Hospital in Jackson, with quality information on the complication
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Is Hypertonic Saline Superior to Mannitol in Reducing Cerebral Edema?
 Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 3-2012 Is Hypertonic Saline Superior to Mannitol in Reducing Cerebral Edema? Shana Hilson Follow this and additional
Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 3-2012 Is Hypertonic Saline Superior to Mannitol in Reducing Cerebral Edema? Shana Hilson Follow this and additional
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA?
 INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
INTRACEREBRAL HEMORRHAGE FOLLOWING ENUCLEATION: A RESULT OF SURGERY OR ANESTHESIA? - A Case Report - DIDEM DAL *, AYDIN ERDEN *, FATMA SARICAOĞLU * AND ULKU AYPAR * Summary Choroidal melanoma is the most
Raised Intracranial Pressure (ICP): Management in Emergency Department
: Management in Emergency Department") Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow