Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
|
|
|
- Jessie McKinney
- 5 years ago
- Views:
Transcription
1 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE III Subjects Issam Awad, MD, University of Chicago Dialysis in the Setting of ICH Wendy Ziai, MD, MPH, Johns Hopkins University
2 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE III Subjects Issam Awad, MD, University of Chicago Dialysis in the Setting of ICH Wendy Ziai, MD, MPH, Johns Hopkins University


3 Surgical Center Report: Safety Forum April 6, 2016
4 Surgical Summary to Date (as of March 10, 2016) Patients Total 294 Surgical 144 (141 underwent surgery) Surgeon Status at time of surgery Pre-qualified 74 Qualified with probation 33 Fully qualified 34 Catheter Tract/ ICH/IVH Bleeds Symptomatic 4 * Asymptomatic 24 * * bleeds in surgical cases, only ICH/IVH expansion or CTH during active phase
5 Surgical Summary to Date Cont d Catheter Category Trajectory A Trajectory B Trajectory C Surgical cases that didn t go to surgery 144 SURGICAL CASES (141 underwent surgery) GOOD INITIAL 43 (66.2% of 65) 11 (35.5% of 31) 32 (71.1% of 45) *One case, the site exhausted their resources and did not attempt to retarget the clot. One case, site did not obtain permission from family for second procedure to retarget clot. 42 SUBOPTIMAL INITIAL 13 POOR INITIAL 32 CATHETERS REPOSITIONED AFTER DOSING OR REPLACED % Evacuated Absolute reduction (ml) % subjects reaching <15ml 19 (29.2% of 65) (16 dosed; 1 replaced and dosed; 1 replaced & reached endpoint) 3 (4.6% of 65) (2 replaced and dosed, 1 replaced and removed) 8 (1 replaced d/t dislodging by pt) 13 (41.9% of 31) (5 dosed; 4 replaced & dosed; 1 replaced & reached endpoint) 7 (22.6% of 31)* (6 replaced & dosed) 18 (includes 6 repositioned after dosing, 1 inadvertent pullback, and 1 replaced after dosing d/t dislodging) 10 (22.2% of 45) (10 dosed) 3 (6.7% of 45) (1 replaced & dosed, 1 replaced and removed) 6 (includes 1 new catheter placed during dosing to better target remaining clot) (1 pt herniated overnight before surgery, taken for crani; 1 pt improved overnight so surgeon didn t take to surgery, 1 prematurely randomized, ICH <30)
6 Surgical Summary to Date- Cont d Good Suboptimal Poor % Evacuated Absolute reduction (ml) % subjects reaching <15ml Prequalified (n=74) 44 (59.5% of 74) 20 (27.0% of 74) 10 (13.5% of 74) Qualified w/ probation (n=33) 18 (54.5% of 33) 14 (42.4% of 33) 1(3.0% of 33) Fully qualified (n=33) 23 (69.7% of 33) 9 (27.3% of 33) 1 (3.0% of 33) Note: 3 cases did not go to surgery so not counted here

 69")


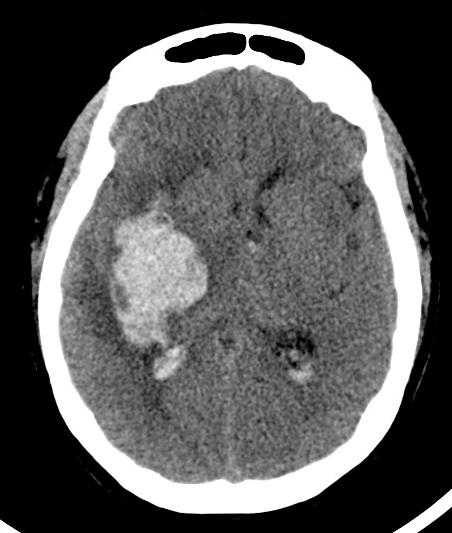
7 6275 Command performance 1 st case at site (German site) 69 y/o female with HTN; site gave 3 doses Volume on stability CT 24.36ml Final volume 0.76ml

8 Lessons learned When asked for the secret to their success, site mentioned several things: Refresher meeting organized by BIOS Online training modules Multiple staff meetings with local MISTIE and hospital staff to present and explain the study PI additionally mentioned: Having the coordinator and surgeon be the same person makes it easier as there is less to coordinate during surgical enrollments Doing a demo case in the EDC to train herself on entering data and randomizing a patient helped make the process smoother

9 6277 Post randomization diagnosis of Moyamoya 56 y/o M with hx of noncompliant HTN Platelets 208, INR 1.1 at baseline CTA reported negative Patient randomized to medical arm
10 CTA report excerpt There is occlusion at M1 segment of right MCA with reconstitution of flow just distal to the occlusion, this may represent chronic occlusion versus less likely vasospasm. Overall the caliber of the distal anterior cerebral and middle cerebral arteries is small and irregular. It is not clear whether this is secondary to vasospasm and edema, or if it is related to contrast bolus timing.



11


12 2 weeks later, site did IR angiogram, definitively diagnosing the patient with Moyamoya
13 Lessons learned Site should consider possible etiology factors even when not spelled out by CTA. Basal occlusive disease should have suggested Moyamoya. SC and study leadership cannot weigh in if a study is uploaded as negative. We cannot divine that there was basal occlusive disease, nor independently read negative scans It is imperative that site PI views and clears all etiology scans
14 6265 asymptomatic (but significant) bleed post catheter removal 69 y/o male; hx of : CAD s/p CABG, MI, hyperlipidemia and A-Fib On Coumadin and ASA upon arrival INR 4.3 initially, pt received Vit K, FFP, PCC, corrected to 1.2 CTA and MRI negative Platelets dropped to 93 and developed chest pain, determined to be A-fib acting up, resolved with resumption of home med Isosorbide Bleed expanded during screening from 13.43ml on Dx CT to 73.48ml on final stability CT Patient randomized to surgery and received 8 total doses Patient not on any anticoags; Lovenox 30mg twice/day for DVT prophylaxis Day 3 through discharge




15 Stability CT Post initial placement Asymptomatic new bleed Post treatment during dosing, post 5 doses - Catheter pulled back after 3 doses; stabilized and continued dosing - After 5 doses, site wanted to pullback again; new bleeding noted on scan; appropriately stabilized before catheter was pulled back. Suggested further 1cm pullback, site agreed. Pulled back, appropriately stabilized, continued dosing
16 Asymptomatic new bleed 24 hours post catheter removal - INR stable at 1.2 throughout - GCS never below 12 (which was immediately post op). Throughout hospitalization, GCS Patient did have 4 hour episode of increased intensity of headache after dose 5
17 Site Evaluation of Hemorrhages Per site PI, the primary ICH expansion as well as the 2 remote small bleeds first noted on D5 appear to be hemorrhagic conversion of ischemic strokes. This is not surprising given the patient s extensive cardiac history. As noted in the EDC, pt has CAD s/p CABG, A-fib, cardiomyopathy, pulmonary HTN, hx cardiac arrest, hypertriglyceridemia, and HTN.





18 Initial MRI (Day 1) GRE: no hemorrhagic microangiopathy ADC: possible ischemic stroke
")




19 Final MRI (Day 11) GRE: hemorrhage in ischemic stroke ADC: expanded ischemic stroke with hemorrhagic conversion
20 Lessons Learned With initial bleeding expansion and subsequent bleeding during dosing, should we have resumed dosing? (protocol allowed but was this patient a bleeder?) Should the patient have been excluded because of ischemic stroke on initial MRI? Is this another example of a tendency of DVT prophylaxis to increase asymptomatic bleeding during treatment? Aspirin effect in a demonstrated bleeder?
21 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE III Subjects Issam Awad, MD, University of Chicago Dialysis in the Setting of ICH Wendy Ziai, MD, MPH, Johns Hopkins University
22 DIALYSIS IN THE SETTING OF ICH CIII and MIII
23 AKI FOLLOWING ICH Four studies, which included 615,623 subjects, examined the prevalence of AKI after ICH. Pooled prevalence rate of AKI after ICH was 19.0% (95% CI = 8.3% %). ICH patients are at risk for acute kidney injury (AKI) due to sepsis, liver failure and other infections and vasculitides
24 RRT IN ICH PATIENTS Specific parameters to guide renal replacement therapy (RRT) mode and timing in neurocritical care patients including ICH are lacking Indications for RRT that may be seen in acute ICH patients other than pre-existing need for dialysis include: severe metabolic acidosis volume overload uremia with end-organ damage refractory hyperkalemia overdose maintenance therapy for patients undergoing outpatient RRT
25 NEUROLOGIC COMPLICATIONS OF RRT RRT especially intermittent RRT (IRRT) has been reported to cause several severe neurologic complications: increased cerebral edema increased intracranial pressure new or worsening intracerebral or subdural hemorrhages new ischemic stroke mental status decline seizures Dialysis disequilibrium syndrome = well-known entity that encompass several symptoms such as headache, lethargy, confusion, seizures or brain herniation events related to increased cerebral edema with or without a known intracranial pathology
26 COHORT CIII (n=500) and MIII (n=300) subjects were reviewed for need for RRT 19 subjects underwent dialysis during the acute hospitalization CIII n=14 (3%) MIII n=5 (2%) Dialysis methods (per review of available source documentation) IHD (intermittent hemodialysis): 8 CRRT (continuous renal replacement therapy) encompasses: CVVHD: continuous veno-veno hemodialysis: 8 CAVHD: continuous arterio-venous hemodialysis: 0 SLED: sustained low-efficiency dialysis: 0 PD: peritoneal dialysis: 0 UTD (unable to determine): 3
27 TIMELINE Dialysis therapy was initiated a mean of 10.9 days post symptom onset for 17 subjects (range: 1-26 days) 2 subjects continued pre-randomization dialysis For those subjects (n=11) who died, mean time to death after start of dialysis was 62.4 days (range: days)
28 DIALYSIS AND DEATH CIII Dead Yes Dead No Total p Dialysis Yes Dialysis No Total MIII Dead Yes Dead No Total p Dialysis Yes Dialysis No Total Three subjects died within 48 hours of dialysis start One received CVVHD (CIII) Two received HD (MIII) CIII & MIII Dead Yes Dead No Total p Dialysis Yes Dialysis No Total









29 Stability: Prior to randomization Day 2: Hours post dialysis Day 3: Day of death
30 CIII Dead Yes Dead No Total p Renal insufficiency prior to rnd Yes Renal insufficiency prior to rnd No Total RENAL INSUFFICIENCY ONSET PRIOR TO RANDOMIZATION AND DEATH MIII Dead Yes Dead No Total p Renal insufficiency prior to rnd Yes Renal insufficiency prior to rnd No Total CIII & MIII Dead Yes Dead No Total p Renal insufficiency prior to rnd Yes Renal insufficiency prior to rnd No Total
31 CIII Dead Yes Dead No Total p Renal insufficiency post rnd Yes Renal insufficiency post rnd No Total MIII Dead Yes Dead No Total p Renal insufficiency post rnd Yes Renal insufficiency post rnd No Total CIII & MIII Dead Yes Dead No Total p Renal insufficiency post rnd Yes Renal insufficiency post rnd No Total RENAL INSUFFICIENCY ONSET POST RANDOMIZATION AND DEATH
32 HYPOTENSION ONSET POST RANDOMIZATION AND DEATH CIII Dead Yes Dead No Total p Hypotension post rnd Yes Hypotension post rnd No Total MIII Dead Yes Dead No Total p Hypotension post rnd Yes Hypotension post rnd No Total Two subjects on dialysis experienced hypotension: one during dialysis one 8 days prior to dialysis CIII & MIII Dead Yes Dead No Total p Hypotension post rnd Yes Hypotension post rnd No Total
33 CHOICE OF TYPE OF RRT IN ACUTE ICH CRRT is chosen for following indications: hemodynamically unstable a higher mean arterial blood pressure is required to enhance cerebral perfusion severe cerebral edema poor intracranial compliance and high intracranial pressure rapid fluid and solute concentration shifts may not be tolerable Therefore, in the acute phase of a neurologic injury such as ICH where maintaining CPP is important, IHD should not usually be the first modality chosen Recommendation: communicate with your renal consultants and if RRT is necessary during acute phase of ICH, 1 st choice is CVVHD until cerebral edema has started to resolve and risk of herniation is low
34 CONSIDERATIONS DURING THE SCREENING ASSESSMENT Does the patient have acute or chronic renal failure? What is the severity of the patient s chronic renal failure and what are the requirements (or not) for dialysis? What is the likelihood of 1 year survival (exclusion factor: Not expected to survive to the day 365 visit due to comorbidities ), in evaluating the patient's candidacy for MISTIE III?
Welcome to our MISTIE III Safety Forum September 12, 2016
 Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Renal Replacement Therapy in Acute Renal Failure
 CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke
 New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke 1 Wendy Ziai, MD, MPH Daniel F. Hanley, MD Johns Hopkins Medical Institutions Dept. of Neurology Division of
New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke 1 Wendy Ziai, MD, MPH Daniel F. Hanley, MD Johns Hopkins Medical Institutions Dept. of Neurology Division of
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
STORMY DENGUE with bloody problems. Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai
 STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)).
).") 12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
12.0 Outcomes 12.1 Definitions 12.1.1 Neurologic Outcome Events a. Ischemic stroke An acute focal infarction of the brain or retina (and does not include anterior ischemic optic neuropathy (AION)). Criteria:
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
 Demographic Data Group Study Cohort Control p N 60 20 Age, Mean (years) 36.3 64.4 < 0.001 Age, Median (years) 33.2 64 < 0.001 Male 41 (68.4%) 4 (20%) 0.001 Female 19 (31.6%) 16 (80%) 0.001 Mechanism of
Demographic Data Group Study Cohort Control p N 60 20 Age, Mean (years) 36.3 64.4 < 0.001 Age, Median (years) 33.2 64 < 0.001 Male 41 (68.4%) 4 (20%) 0.001 Female 19 (31.6%) 16 (80%) 0.001 Mechanism of
Decision making in acute dialysis
 Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Nuts for Neuro and why I hate EMR
 Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
CLEAR III Monthly Webinar. November 2012
 CLEAR III Monthly Webinar November 2012 Agenda 1. Review of Recent Enrollments- Amanda Bistran-Hall 2. October 2012 World Cup Statistics Update- Andrew Mould 3. Safety Profiles & 9 Surgically Significant
CLEAR III Monthly Webinar November 2012 Agenda 1. Review of Recent Enrollments- Amanda Bistran-Hall 2. October 2012 World Cup Statistics Update- Andrew Mould 3. Safety Profiles & 9 Surgically Significant
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION
 PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION HAI NGUYEN, DO, MPH Anesthesiology Resident (University of Kansas Wichita) JOEL CAVAZOS, MD Pain
PSEUDO-SUBARACHNOID HEMORRHAGE AFTER INADVERTENT DURAL PUNCTURE DURING CERVICAL EPIDURAL STEROID INJECTION HAI NGUYEN, DO, MPH Anesthesiology Resident (University of Kansas Wichita) JOEL CAVAZOS, MD Pain
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD
 HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
HIP ATTACK Trial: Can we improve outcomes after a hip fracture with accelerated surgery? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting honorariums or other payments
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
Sid Bhende MD Sentara Vascular Specialists April 28 th Dialysis Access Review: Understanding the Access Options our Patients Face
 Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
Sid Bhende MD Sentara Vascular Specialists April 28 th 2018 Dialysis Access Review: Understanding the Access Options our Patients Face Disclosures Dialysis Background Why is it important? Outline National
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
- SLED Sustained Low-Efficiency Dialysis
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
VTE in Children: Practical Issues
 VTE in Children: Practical Issues Wasil Jastaniah MBBS,FAAP,FRCPC Consultant Pediatric Hem/Onc/BMT May 2012 Top 10 Reasons Why Pediatric VTE is Different 1. Social, ethical, and legal implications. 2.
VTE in Children: Practical Issues Wasil Jastaniah MBBS,FAAP,FRCPC Consultant Pediatric Hem/Onc/BMT May 2012 Top 10 Reasons Why Pediatric VTE is Different 1. Social, ethical, and legal implications. 2.
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Extracranial Carotid Artery Stenting With or Without Distal Protection Device
 Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
Place for Interventional Radiology in Acute Stroke
 Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
Place for Interventional Radiology in Acute Stroke Dr Lakmalie Paranahewa MBBS, MD(Radiology), FRCR Consultant Interventional Radiologist Asiri Group of Hospitals Objectives Imaging in Stroke Neurovascular
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic