Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
|
|
|
- Kelley Wood
- 5 years ago
- Views:
Transcription

1 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
2 Nothing to disclose

3 Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss recognition, evaluation and management strategies
4 Acute onset, focal neurologic symptoms attributed to vascular abnormality 4 th Leading cause of death Leading cause of disability Prevalence 6.6M $71 Billion/Yr


5 Hemorrhagic 12% Subarachnoid 3% Ischemic 85% Roger et al. Heart disease and Stroke Statistics. Circulation 2012; 126: e2-220






6 Risk Factors Diabetes CAD/PVD Hyperlipidemia Atrial Fibrillation Hypertension Stroke Smoking/Drugs Roger et al. Heart disease and Stroke Statistics. Circulation 2012; 126: e2-220
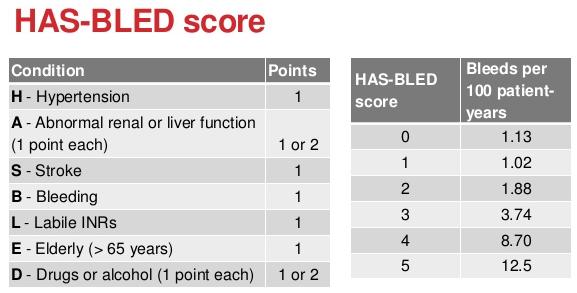
7 Primary Prevention includes management of Risks HTN, HPL, DM, CAD Smoking cessation counseling There is no role for aspirin Atrial fibrillation Meschia et al. Guidelines for primary prevention of stroke, Stroke 2014

8 CHADS2, CHA2DS2-VASc, and long-term stroke outcome in patients without atrial fibrillation. March 12, : ; published ahead of print February 13, 2013
9
10 47yo man with a history of smoking and no other known history who presents with R arm and leg weakness noted at 1230pm upon waking. His wife states she also noted a R facial droop R Hemiparesis

11 Early Recognition TIME BRAIN

:607-15. doi: 10.1093/qjmed/hct057.")
12 Middle Cerebral Artery Syndrome R MCA distribution L Face,arm weakness L Sensory loss L Neglect R Gaze preference L MCA distribution R Face,arm weakness R Sensory loss Aphasia R Gaze preference QJM Jul;106(7): doi: /qjmed/hct057. Epub 2013 Mar 1

:607-15. doi: 10.")
13 R ACA distribution L leg weakness Cognitive abnl R Gaze preference Anterior Cerebral Artery Syndrome QJM Jul;106(7): doi: /qjmed/hct057. Epub 2013 Mar 1


14 Posterior Cerebral Artery Syndrome R PCA distribution L Sensory loss L Hemianopia QJM Jul;106(7): doi: /qjmed/hct057. Epub 2013 Mar 1


15 QJM Jul;106(7): doi: /qjmed/hct057. Epub 2013 Mar 12. Vertebrobasilar Syndrome Vetebrobasilar distribution CN findings Ataxia Vertigo
16 Stroke Mimics Hypoglycemia Migraine Toxic/Metabolic Infection/Sepsis Mass lesion Seizure Conversion disorder Hand et al. Distinguishing between stroke and mimic at the bedside, Stroke 2006
17 Questions to ask to determine Mimic Are there vacular/stroke risks? Is the nature of the symptoms (+) or (-) (loss of function or gain of function) What is the onset and progression? What is the duration? Was there precipitating factor? What are other associated symptoms? Do the symptoms fit a stroke syndrome?

18 47yo man with a history of smoking and no other history who presents with R arm and leg weakness noted at 1230pm. Vitals: BP 184/97, HR 75, RR 16 99% RA, T 37 ED arrival 1:05pm Stroke Code 1:09pm NIHSS 1:11pm


19 Last known well Brief history NIHSS Labs
20 Last known well Brief history Previous day 930pm Smokes 2-3ppd, Doesn t see doctors, No medications Felt tired, went to bed, skipped work, woke 730am with R weakness back to bed and woke 1230pm worsened NIHSS Labs 6 (range 0-42) Glucose: 238 Creatinine 0.69 INR 1 Platelets 247 Level of consciousness: alertness, Orientation, follow commands Best Gaze Visual Fields Facial Palsy Limb strength x all 4 extremities Limb ataxia Sensation Language/aphasia Dysarthria Extinction/Inattention

21 ED arrival Stroke Code NIHSS CT/CTA 1:05pm 1:09pm 1:11pm 1:19, 1:27


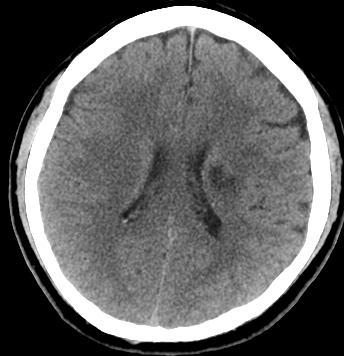
22 Examples of Stroke on CT

23 41yo man with acute onset R hemiparesis
24



25 ED arrival 1:05pm Stroke Code 1:09pm NIHSS 1:11pm CT/CTA 1:19, 1:27 tpa none
26 Eligibility Diagnosis of ischemic stroke causing measurable neurological deficit. The neurological signs should not be clearing spontaneously. The neurological signs should not be minor and isolated. Onset < 3 hours from initiating IV tpa Patient 18 years old Head CT no hemorrhage or large infarct Adams HP. et al AHA Guidelines Stroke 2007;38:
27 Absolute Contraindications Major head trauma or stroke in last 3 months Symptoms of stroke suggestive of SAH Blood pressure elevated, BP >185/110 (may treat) Prior history of ICH Prior history neoplasm, AVM, aneurysm Intracranial or spinal surgery last 3 months Arterial puncture at noncompressible site LP in last 7 days Evidence of active bleeding or trauma Platelet < 100,000 Received heparin in last 48 hrs AND abnormal PTT On coumadin AND INR >1.7, PT > 15 On dabigatran, rivaroxaban, or apixaban (NOACs) within 48 hours Blood glucose abnormal, <50 mg/dl (2.7 mmol/l) Head CT large hypodensity > 1/3 middle cerebral artery territory Relative Contraindications (Use caution 1 or more positive) Stroke symptoms are minor and improving rapidly Pregnancy Seizure and post-ictal residual Major surgery or trauma in the last 14 days GI or GU hemorrhage in the last 21 days Myocardial infarction last 3 months Additional considerations Patient and family understand risks Caution in treating patients with major deficits Caution using tpa if low molecular heparin used last 24 hours Adams HP. et al AHA Guidelines Stroke 2007;38:
28 NIHSS Risk of Intracerebral Hemorrhage % % >20 17% Additional inclusion between hrs Meet all criteria of < 3 hour since onset of stroke Age 80 years of age No anticoagulant use, regardless of INR NIHSS 25 No combined history of prior stroke and diabetes NINDS and Stroke TPA Study Group N Engl J Med 1995; 333: ECASS-3 trial. NEJM 2008;359:




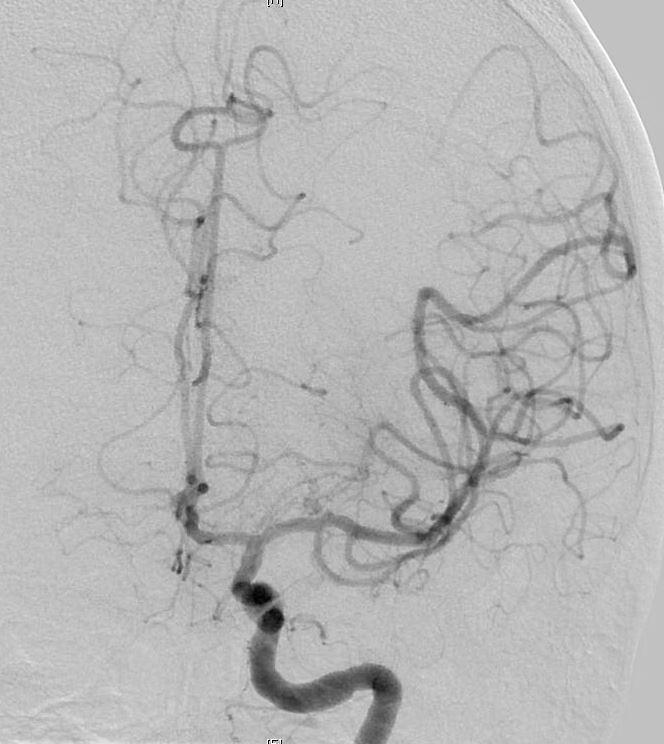
29 ED arrival 1:05pm Stroke Code 1:09pm NIHSS 1:11pm CT/CTA 1:19pm, 1:27pm tpa None IR 2:25pm

30


31 CT Perfusion Scan Cerebral Blood Flow Mean Transit Time Time to Peak


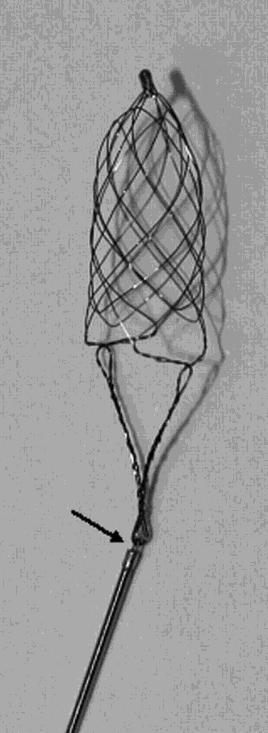
32 MR CLEAN Swift Prime Extend IA

33


34


35 MRI BRAIN DWI ADC FLAIR
36 LDL 116 (goal <70) Lipitor 80mg A1C: 10.1 Avoid hyperglycemia Endocrine CS Smoking cessation counseling Blood pressure control (SBP <140) Aspirin for secondary prevention 30d event monitor at discharge
37 Hemorrhagic 12% Subarachnoid 3% Ischemic 85%


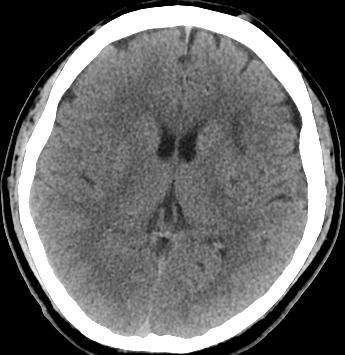
38 Most common cause of nontraumatic ICH is Hypertension Initial BP and CT findings help with determination of cause 220/ / /90
39 65yo woman with a history of hypertension, noncompliant with medications presents with R arm weakness and word finding difficulties BP on arrival 220/126, HR 100, RR 16 99% RA



40 ED arrival Stroke Code NIHSS CT/CTA
41

42 SPOT Sign Wada et al. CT angiography spot sign predicts hematoma expansion in acute cerebral hemorrhage. Stroke 2007, 38:4
43 Early and rapid blood pressure control is essential Goal SBP <140 Labetalol or Hydralazine 20mg IV Q15min Nicardipine infusion mg/hr Start oral medications as soon as possible Reverse coagulopathy Coumadin: PCC or FFP, Vit K 10mg IV Dabigatran/Pradaxa: Idarucizumab/Praxabind Xa inhibitors: PCC
44 What about role of surgery? No indication unless cerebellar origin Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, Shaw MD, Barer DH; STICH investigators. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005; 365 (9457):
45 This patient improved and was able to be discharged to rehab. Blood pressure control took multiple medications and she will need close followup HCTZ, Labetalol, Lisinopril, Amlodipine
46 Hemorrhagic 12% Subarachnoid 3% Ischemic 85%

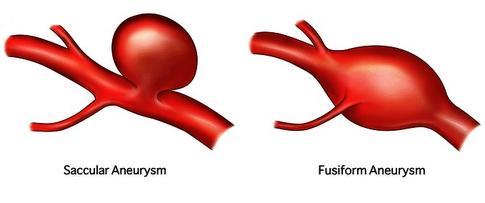
47
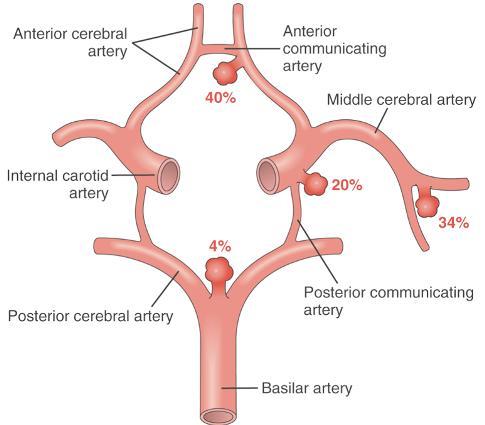
48 F>>M Smokers HTN Family history of aneurysms or SAH Cocaine use
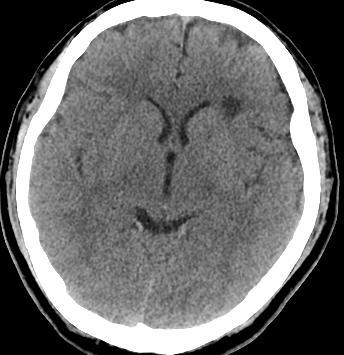
49 47yo woman with a history of migraine headaches, smoking and hypertension presents with severe headache that began 3h PTA.


50 History Exam CTh LP
51 History is key Describe headache Previous episode? Other associated features N/V, neck pain, loss of consciousness Neurologic symptoms Brief Neurologic examination Mental status, confusion, pupil changes, weakness
52 Who to Image? Severe worst headache of life Loss of consciousness at the onset Acute onset headache different from usual Not responding to typical treatment Othr accompanying symptoms Neurologic changes Meningismus

53 Sensitivity 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Sensitivity CT for SAH 3 days 1 week 2 weeks Time Since Headache Onset

54 Lumbar puncture if CTh (-) Must be >8h post hemorrhage Xanthochromia
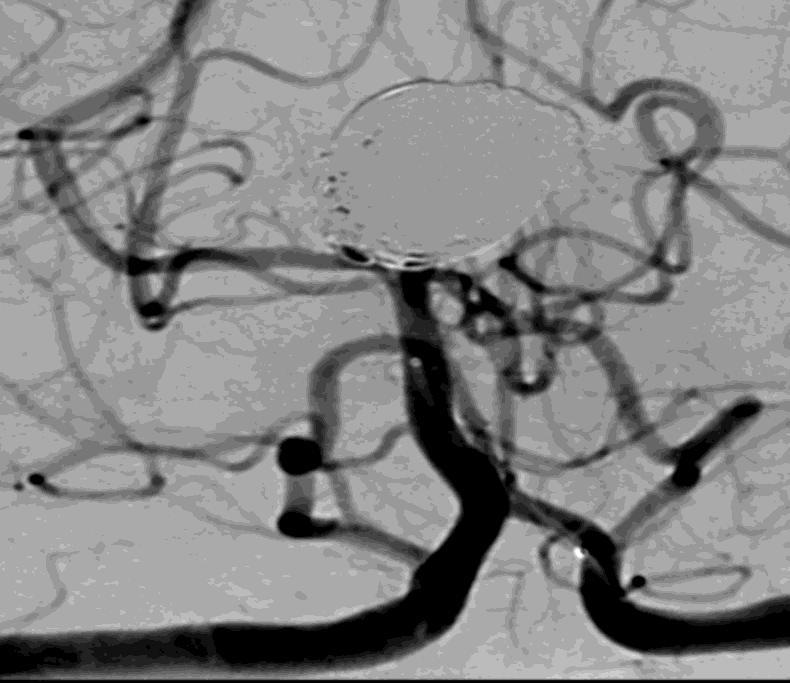
55 Presented to ED, Severe headache though no other symptoms, thought to be migraine Re-presented 3d later with AMS, Confusion and drowsiness
56

57

58



59 Early Complications Late Complications Initial Rupture Rebleed Hydrocephalus Brain edema Seizure Takotsubo Vasospasm DCI Modify Risk: Smoking, HTN Screening if family history Drainage of CSF Hypertonic saline/mannitol Seizure prophylaxis Early recognition ECG, Troponins, Echo Source control Blood pressure control (<140) Proper analgesia/sedation Euvolemia Hypertesion Normothermia Proper analgesia/sedation Screening

60 External Ventricular Drain (EVD)
61

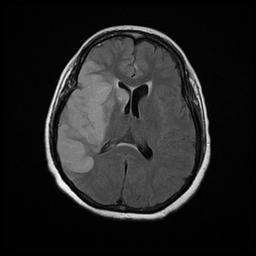
62 MRI BRAIN Flair sequence

63 Strokes are common neurologic emergencies Early recognition and treatment are paramount Management strategies continue to advance Those that survive are at high risk for further complications Risk factor modification before and after is essential
64
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
AGWS Stroke Thrombolysis Clinical Profoma
 AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
AGWS Stroke Thrombolysis Clinical Profoma Incorporating Salisbury NHS Foundation Trust guidance Date: On Arrival: Affix patient label here) GCS NIHSS Score: Pulse SaO on Air Give O only if < 95 % on Air
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
What Do You Think of My Posterior?
 What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
What Do You Think of My Posterior? Posterior Stroke and Stroke Mimics Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School of Medicine Disclosures
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Thrombolysis Assessment
 Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Thrombolysis Assessment Brief Clinical Summary of symptom onset of arrival of patient of assessment BP GCS BM If BM
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
PATIENT S NOTES History and Physical Brain Attack Stroke
 UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1,
 I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
I n t e r h o s p i t a l Tr a n s fe r s o f t h e A c u t e S t r o ke Pat i e n t E M S G r a n d Ro u n d s : Febr u a r y 2 1, 2 0 1 8 Elaine Skalabrin, MD S t r o k e M e d i c a l D i r e c t o
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
NIHSS. Category Scale Definition Date/Time Date/Time Date/Time. Score Initial. Drip & Ship Protocol. Initials: Signature: Initials: Signature:
 NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
NIHSS 1a. Level of Consciousness (Alert, drowsy, etc.) Category Scale Definition Date/Time Date/Time Date/Time 1b. LOC Question (Month, age) 1c. LOC Commands (Open, close eyes, make fist, let go) 2. Best
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
ED Stroke Panel Page 1 of 2
 ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
ED Stroke Panel Page 1 of 2 Reference EMMC *************************Usec: Call Operator to page a Stroke Alert ********************** Laboratory Bedside Glucose Monitoring ONCE Notify provider if glucose
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor
 Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor Lori Massaro, RN, MSN, CRNP Bethanne McCabe, RN, MSN, CNRN Sue Underwood, RN, MSN, CNRN Requirement RN s caring for
Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor Lori Massaro, RN, MSN, CRNP Bethanne McCabe, RN, MSN, CNRN Sue Underwood, RN, MSN, CNRN Requirement RN s caring for
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Ischemic Stroke: Treatment Update. American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD
 Ischemic Stroke: Treatment Update American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD Objectives Understand the treatment of acute stroke Thrombectomy
Ischemic Stroke: Treatment Update American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD Objectives Understand the treatment of acute stroke Thrombectomy
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Code Stroke in real life. Disclosures. Parkland Memorial Hospital. I have no disclosures. Has 1 million patient visits annually. Level 1 Trauma Center
 Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Code Stroke in real life Alejandro Magadán, M.D. University of Texas Southwestern Medical Center Medical Director for Stroke Parkland Memorial Hospital Disclosures I have no disclosures Parkland Memorial
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Lothian Audit of the Treatment of Cerebral Haemorrhage (LATCH)
") 1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
1. INTRODUCTION Stroke physicians, emergency department doctors, and neurologists are often unsure about which patients they should refer for neurosurgical intervention. Early neurosurgical evacuation
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
HPI Signs and Symptoms Considerations
 SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
SECTION: Adult General Medical Emergencies PROTOCOL TITLE: Medical Stroke/TIA REVISED: 07/2017 Protocol OVERVIEW: Stroke is a major cause of disability and a leading cause of death in the U.S. There are
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of