Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
|
|
|
- Sara Stewart
- 5 years ago
- Views:
Transcription



1 Treatment of Acute Hemorrhagic Stroke 5th QSVS Neurovascular Conference Dar Dowlatshahi MD PhD FRCPC Sept 14, 2012
2 Disclosure of potential conflicts of interest Quebec Society of Vascular Sciences presents : The 5th QSVS Neurovascular Conference Hemorrhagic Stroke September 14, 2012 Dr. Dar Dowlatshahi, Guest speaker Guest speaker (2011), Travel support (2012): Boehringer Ingelheim Moderating speaker (2012): Octapharma Advisory board (2010): Bayer Canada
3 All copyrighted material have been removed from the notes, and will only be shown during the presentation
4 Outline 1. Hematoma expansion & hemostasis 2. Indications for ICH surgery 3. Preventing complications of ICH
5 Levels of evidence Class I: benefit > risk Class II: benefit may > risk Class III: risk > benefit


6 Part 1: ICH Expansion 3 h 6 h 0% mortality 70% independence 30% mortality 35% independence
7 Hemostasis 1. rfviia 2. Reversal of antiplatelet activity platelets ddavp TXA 3. Coagulopathy correction/anticoagulant associated ICH PCC/Vit K FFP
8 Biological effect of rfviia
9

10 72 hr ICH growth Mean = 4.3 ml Median = 0.91 ml SD = ml Dowlatshahi D, Demchuk AM, Smith EE et al (in preparation)

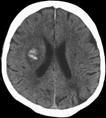
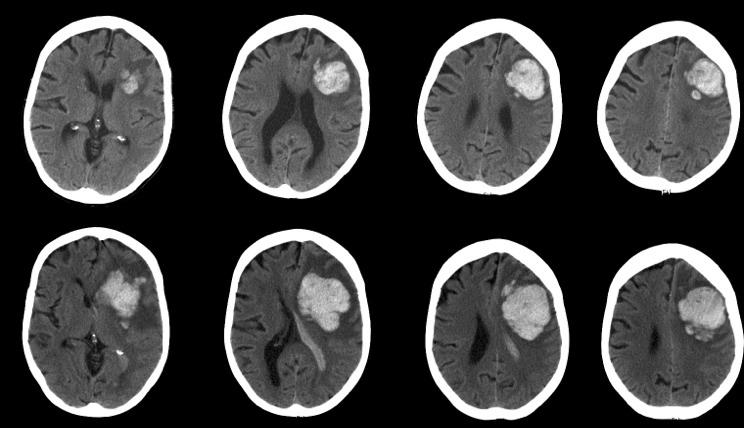
11 Imaging Marker of ICH Growth Identified Garcia Bermejo P et al. Neurology 2010;75;834
12


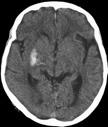
13 Spot Sign Demchuk, Dowlatshahi et al. Lancet Neurology 2012

14 Lancet Neurology 2012
15 Spot Sign hemostatic trials STOP- AUST
16 Factor VII: Bottom Line rfviia in unselected patients: Class III, Level A (Harm) If you have CTA for acute ICH: Spotlight Trial



17 Antiplatelets and hematoma expansion Neurology 2009 Neurology 2011 Increased mortality
18 Option 1: Platelet infusion Thrombocytopenia: platelet replacement (Class I, Level C) On antiplatelet agent: platelet infusion (Class II, Level B)
19 Option 2: ddavp / desmopressin releases endothelial vwf: platelet activator 0.3 mcg/kg over 30 minutes Currently no evidence or guidelines; consider for Plavix, uremia IMPACT study, phase 2 safety ddavp for acute ICH, results due Dec 2012.
20 Option 3: Tranexamic acid anti-fibrinolytic: clot-stabilization No evidence Consider: intra-operative, tpa bleeds

21 INR correction in anticoagulant associated hemorrhage
22 11h 24h
23 Fresh Frozen Plasma Time: Blood typing & thaw 15 ml/kg: >1L on average in patients with pre-existing cardiac disease Inconsistent Factor concentrations
24 Prothrombin Complex Concentrate
25 PCC small volumes (40-80 ml) reversal within minutes requires Vit-K 10mg IV co-administration
26 Adverse events
27 Clinical Outcomes INR reversal may be necessary but not sufficient to alter the natural history of warfarin-associated ICH. Dowlatshahi, Butcher at al, Stroke 2012
28 1. INR correction for patients with oral-anticoagulant associated ICH: Class I, Level C 2. PCC may have fewer complications to FFP and is a reasonable alternative: Class II, Level B
29 Part 2: Indications for Surgery 1. Cerebellar 2. IVH 3. Hemispheric
30 cerebellar Evacuation for clinical deterioration or brainstem compression or hydrocephalus: Class I, Level B Ventricular drainage alone not recommended: Class III, Level C
31 IVH Drainage for hydrocephalus with decreased LOC: Class II, Level B

32 Median 30 hours to surgery > 25% cross-over rate to surgery in medical arm Mendelow et al, Lancet 2005
33 Surface bleeds STICH sub-group analysis
34
35 Guidelines for supratentoral ICH Surgery 1. Usefulness uncertain: Grade II, Level C 2. Large lobar ICH <1cm from surface: Grade II, Level B 3. Minimally invasive evacuation investigational: Grade II, Level B

36 Eloquent cortex? Global Aphasia NIHSS 10 Post-op NIHSS 3 F/U NIHSS 0

37 MR-DTI guided MIS
38 PArt 3: Preventing complications Hematoma Expansion IVH/hydrocephalus Hypertension Seizures Infection DVT/PE Fever/Hyperglycemia
39 Seizure 8% (2-20%) 30-day risk (subclinical ceeg approx 30%). Associated with worse outcomes, but not clearly causative. Prophylactic treatment associated with worse outcomes in two recent studies. New Guidelines: Treat clinical seizures (Class I, level A) Treat electrographic seizures with altered LOC (Class I, Level C) No prophylactic therapy (Class III, Level B)
40 comment Study 1: covariate analysis for factors associated with poor outcome But only 23 patients treated with PHT Study 2: only 28 patients treated with PHT 12 treated with LEV with no adverse outcome
41 Infection Aspiration / swallowing assessments Foley catheters, IV lines
42 DVT/PE prophylaxis Intermittent pneumatic compression boots (Class I, Level B) After repeat imaging showing cessation of bleeding, SC Heparin/LMWH starting day 1-4 (Class IIb, Level B).
43 Metabolic Fever Hyperglycemia (normoglycemica Class I, Level C)
44 Summary 1. Hemostasis PCC for warfarin-associated ICH consider platelets if low consider ddavp if on antiplatelets No rfviia 2. Surgery cerebellar IVH with symptomatic hydrocephalus consider surgery for large superficial lobar bleeds 3. Complications prevent infections: aspiration, instrumentation normoglycemia, normothermia treat seizures, altered LOC with electrographic evidence start compression boots day 0, prophylactic anticoagulation between day 1-4 (after scan)
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Intracerebral Hemorrhage
 Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Review of Primary Intracerebral Hemorrhage Réza Behrouz, DO Assistant Professor of Neurology University of South Florida College of Medicine STROKE 85% ISCHEMIC 15% HEMORRHAGIC HEMORRHAGIC STROKE 1/3 Subarachnoid
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC
 Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Benjamin Anyanwu,MD Medical Director In-patient Neurology and Neuroscience ICU Novant Health Forsyth Medical Center, Winston-Salem NC Emergency Treatment of Hemorrhagic Stroke Objectives Discuss the etiology
Outlook for intracerebral haemorrhage after a MISTIE spell
 Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Outlook for intracerebral haemorrhage after a MISTIE spell David J Werring PhD FRCP Stroke Research Centre, Department of Brain Repair and Rehabilitation, UCL Institute of Neurology, National Hospital
Intracerebral Hemorrhage
 Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Intracerebral Hemorrhage J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director,
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Use of Anticoagulant Reversal Agents
 Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
Use of Anticoagulant Reversal Agents Lori Shutter, MD shutterla@upmc.edu Vice Chair of Education Director, Neurocritical Care Program Professor, Critical Care Medicine, Neurology & Neurosurgery University
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
AHA/ASA Guideline. Downloaded from by on September 4, 2018
 AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT. Neeraj Naval, MD Baptist Neurological Institute
 SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT Neeraj Naval, MD Baptist Neurological Institute Disclosures/ COI Nothing to disclose (what happens in Vegas stays in Vegas) No Conflict of interest
SPONTANEOUS INTRACEREBRAL HEMORRHAGE: MEDICAL MANAGEMENT Neeraj Naval, MD Baptist Neurological Institute Disclosures/ COI Nothing to disclose (what happens in Vegas stays in Vegas) No Conflict of interest
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke ESO.org. Csiba László.
 Stroke ESO.org Csiba László csiba@dote.hu Global mortality Cause of death Dept. of Neurology? 1938-1950 1990-2002 Tumor Stroke Tumor Infect. Stroke Normal lifestyle After MI 70-80% After stroke 10% Differential
Stroke ESO.org Csiba László csiba@dote.hu Global mortality Cause of death Dept. of Neurology? 1938-1950 1990-2002 Tumor Stroke Tumor Infect. Stroke Normal lifestyle After MI 70-80% After stroke 10% Differential
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Reversal of Anticoagulants at UCDMC
 Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant
Reversal of Anticoagulants at UCDMC Introduction: Bleeding complications are a common concern with the use of anticoagulant agents. In selected situations, reversing or neutralizing the effects of an anticoagulant
ADVOCATE HEALTHCARE GUIDELINE FOR ANTITHROMBOTIC REVERSAL
 Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Objectives. Definition 3/21/2017. Spontaneous, Nontraumatic Intracerebral Hemorrhage
 Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP-BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM Objectives
AHA/ASA Guideline. by guest on September 29, 2016
 AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
AHA/ASA Guideline Guidelines for the Management of Spontaneous Intracerebral Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
Reversal of direct oral anticoagulants in the patient with GI bleeding. Marc Carrier
 Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Reversal of direct oral anticoagulants in the patient with GI bleeding Marc Carrier Disclosure Faculty: Dr. Marc Carrier Relationships with commercial interests: Grants/Research Support: Leo Pharma, Bristol
Hemostasis and thrombosis in patients with liver disease. Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands
 Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Use of Prothrombin Complex Concentrates (PCC) CONTENTS
 CONTENTS") CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
5/15/2018. Reduced Platelet Activity
 ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
SPONTANEOUS INTRACEREBRAL HEMORRHAGE
 SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
SPONTANEOUS INTRACEREBRAL HEMORRHAGE Intracerebral hemorrhageis an acute and spontaneous extravasationof blood into the brain parenchyma that may extend into the ventricles and subarachnoid space. It is
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
When Not To Give TPA Steve Phillips Division of Neurology
 When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
When Not To Give TPA Steve Phillips Division of Neurology stephen.phillips@nshealth.ca AstraZeneca Disclosures - 1 I have given CME lectures and served on advisory boards for Boehringer Ingelheim Bristol-Myers
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
8/16/2016. Disclosures. Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco. Risk of Stroke Peri-Ablation
 Disclosures Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco Atul Verma, MD FRCPC FHRS Director, Heart Rhythm Program Southlake Regional Health Centre Newmarket, Ontario,
Disclosures Is Uninterrupted OAC Standard of Care for AF Ablation? CHRS 2016, San Francisco Atul Verma, MD FRCPC FHRS Director, Heart Rhythm Program Southlake Regional Health Centre Newmarket, Ontario,
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Hemorrhage. Dr. Al Jin Nov. 17, 2015
 Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Hemorrhage Dr. Al Jin Nov. 17, 2015 None Disclosures ICH Management in ER ABCs Treat hypertension What BP target? Reverse warfarin Hemorrhage vs Ischemic Stroke Lowering BP may be harmful in ischemic stroke
Case Report Minimally Invasive Subcortical Parafascicular Transsulcal Access for Clot Evacuation (Mi SPACE) for Intracerebral Hemorrhage
 for Intracerebral Hemorrhage") Case Reports in Neurological Medicine, Article ID 102307, 4 pages http://dx.doi.org/10.1155/2014/102307 Case Report Minimally Invasive Subcortical Parafascicular Transsulcal Access for Clot Evacuation
Case Reports in Neurological Medicine, Article ID 102307, 4 pages http://dx.doi.org/10.1155/2014/102307 Case Report Minimally Invasive Subcortical Parafascicular Transsulcal Access for Clot Evacuation
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia
 Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
Giuseppe Micieli Dipartimento di Neurologia d Urgenza IRCCS Fondazione Istituto Neurologico Nazionale C Mondino, Pavia Charidimou et al, 2012 Pathogenesis of spontaneous and anticoagulationassociated
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Perioperative risk reduction and B-blockers. Topics. Introduction 3/26/2012
 Perioperative risk reduction and B-blockers UCSF Department of Surgery Postgraduate Course John Maa MD, FACS March 25, 2012 Topics 1) The controversy over beta blockers and POISE --- is Clonidine the answer?
Perioperative risk reduction and B-blockers UCSF Department of Surgery Postgraduate Course John Maa MD, FACS March 25, 2012 Topics 1) The controversy over beta blockers and POISE --- is Clonidine the answer?
MANAGEMENT OF OVER-ANTICOAGULATION. Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas
 MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
MANAGEMENT OF OVER-ANTICOAGULATION Tammy K. Chung, Pharm.D. Critical Care & Cardiology Specialist Presbyterian Hospital Dallas Risk of Intracranial Hemorrhage in Outpatients (From Management of Oral Anticoagulant
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Tyler Carson D.O., Vladamir Cortez D.O., Dan E. Miulli D.O.
 Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Bedside Intracranial Hematoma Evacuation and Intraparenchymal Drain Placement for Spontaneous Intracranial Hematoma Larger than 30 cc in Volume: Institutional Experience and Patient Outcomes Tyler Carson
Management of Intracerebral Haemorrhage
 Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
Management of Intracerebral Haemorrhage It s the worst type of stroke. Least treatable form of stroke Evidence-base limited most Overall mortality 35-50% Half of these would die within first 24 hours
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Management of Spontaneous Intracerebral Hemorrhage (ICH)
") Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM 1 Objectives
Management of Spontaneous Intracerebral Hemorrhage (ICH) Mindy Mason, MSN, RN, ACNP BC University of New Mexico Academic Medical Center Level I Trauma Center 24 bed Neuroscience ICU Albuquerque, NM 1 Objectives
Content 1. Relevance 2. Principles 3. Manangement
 Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Intracranial haemorrhage and anticoagulation Department of Neurology,, Germany Department of Neurology, Heidelberg University Hospital, Germany Department of Clinical Medicine Copenhagen University, Denmark
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage
 Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
Incidence and Impact of Antithrombotic-related Intracerebral Hemorrhage John J. Lewin III, PharmD, MBA, BCCCP, FASHP, FCCM, FNCS Division Director, Critical Care & Surgery Pharmacy Services, The Johns
Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke
 Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke A Scientific Statement for Healthcare Professionals from the American Heart Association/American
Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke A Scientific Statement for Healthcare Professionals from the American Heart Association/American
Treatment of anticoagulant-associated intracerebral haemorrhage
 Treatment of anticoagulant-associated intracerebral haemorrhage Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester Academic Health Science Centre, Salford Royal NHS
Treatment of anticoagulant-associated intracerebral haemorrhage Adrian Parry-Jones NIHR Clinician Scientist & Honorary Consultant Neurologist Manchester Academic Health Science Centre, Salford Royal NHS
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke
 New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke 1 Wendy Ziai, MD, MPH Daniel F. Hanley, MD Johns Hopkins Medical Institutions Dept. of Neurology Division of
New Clinical Trials For ICH: MISTIE III Minimally invasive techniques for hemorrhagic stroke 1 Wendy Ziai, MD, MPH Daniel F. Hanley, MD Johns Hopkins Medical Institutions Dept. of Neurology Division of
Intracerebral Hemorrhage
 Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
Update on Intracerebral Hemorrhage November 8, 2013 Anne E. O Duffy, MD Assistant Professor of Neurology Stroke Division Intracerebral Hemorrhage Traumatic Spontaneous Primary (80-88%): due to spontaneous
>>FAST TRACK<< Hemostasis has three key components: platelets, the plasma coagulation. cascade, and the blood vessel wall (endothelium).
.") How to Reverse an Antithrombotic Agent The authors review options and precautions to consider when you need to restore hemostasis in a patient receiving an anticoagulant, antiplatelet, or fibrinolytic
How to Reverse an Antithrombotic Agent The authors review options and precautions to consider when you need to restore hemostasis in a patient receiving an anticoagulant, antiplatelet, or fibrinolytic
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage
 Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
Acute Management of Anticoagulation-Associated Intracerebral Hemorrhage Authors Joji B. Kuramatsu, Stefan T. Gerner, Hagen B. Huttner, Stefan Schwab Affiliation University Hospital Erlangen Department
New Oral Anticoagulants
 New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
New Oral Anticoagulants Tracy Minichiello, MD Associate Professor of Medicine Chief, San FranciscoVA Anticoagulation and Thrombosis Services What percentage of time do patients on warfarin spend in therapeutic
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Update in Management of Acute Spontaneous Intracerebral Haemorrhage
 Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Update in Management of Acute Spontaneous Intracerebral Haemorrhage Aldy S. Rambe Neurology Department, School of Medicine EPIDEMIOLOGY Although ICH represents only about 9% of all stroke, it accounts
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out?
 and Tranexamic acid (TXA): Is the Jury Still Out?") Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Pre-hospital Administration of Blood Products (PHBP) and Tranexamic acid (TXA): Is the Jury Still Out? Jessica K. Reynolds, MD Assistant Professor of Surgery University of Kentucky, Department of Trauma
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Managing Bleeding on NOACs
 Managing Bleeding on NOACs and Other Evolving ED Protocols Objectives Understand that NOACs are widely used in clinical practice Discuss the new and evolving protocols for managing bleeding in patients
Managing Bleeding on NOACs and Other Evolving ED Protocols Objectives Understand that NOACs are widely used in clinical practice Discuss the new and evolving protocols for managing bleeding in patients
Managing Bleeding in the Patient on DOACs
 Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Managing Bleeding in the Patient on DOACs Spring 2016 Jean M. Connors, MD Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine, HMS Conflicts
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Guidelines and Beyond: Traumatic Brain Injury
 Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
Guidelines and Beyond: Traumatic Brain Injury Aimee Gowler, PharmD, BCCCP, BCPS Neuromedicine Critical Care Clinical Pharmacy Specialist UF Health Shands Disclosures I have no financial interests to disclose.
CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin
 CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin DISCLOSURES None Objective(s): Our department routinely used
CABG in the Post-Aprotinin Era: Are We Doing Better? Ziv Beckerman, David Kadosh, Zvi Peled, Keren Bitton-Worms, Oved Cohen and Gil Bolotin DISCLOSURES None Objective(s): Our department routinely used
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
Jan 5, Coma 8 years. Jan 11, 2014
 Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Jan 5, 2006 Coma 8 years Jan 11, 2014 CT Scan of Head showing large right frontal ICH The Intracerebral Hemorrhage: Team Approach Rodney Leacock MD Introduction Intracerebral hemorrhage (ICH) is a very
Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage
 Last Updated: May 21st, 2013 Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage Canadian Best Practice Recommendations for Stroke Care 2012-2013 Update Contents Search
Last Updated: May 21st, 2013 Canadian Best Practice Recommendations for Stroke Care 3.7 Acute Intracerebral Hemorrhage Canadian Best Practice Recommendations for Stroke Care 2012-2013 Update Contents Search
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults
 Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Pelvic Inflammatory Disease
 The Articles Pelvic Inflammatory Disease Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med 2015 May;372(21):2039-48. 2018 LLSA Article Review Shared Decision-making Hess EP,
The Articles Pelvic Inflammatory Disease Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med 2015 May;372(21):2039-48. 2018 LLSA Article Review Shared Decision-making Hess EP,
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials
 New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials James Douketis, MD, FRCPC Specialty: Internal Medicine Professor, Department
New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials James Douketis, MD, FRCPC Specialty: Internal Medicine Professor, Department
Everything Your Pharmacist Wished You Knew About Anticoagulant Reversal Darrel W. Hughes, Pharm.D., BCPS University Health System & UT Health Science
 Everything Your Pharmacist Wished You Knew About Anticoagulant Reversal Darrel W. Hughes, Pharm.D., BCPS University Health System & UT Health Science Center at San Antonio Department of Pharmacotherapy
Everything Your Pharmacist Wished You Knew About Anticoagulant Reversal Darrel W. Hughes, Pharm.D., BCPS University Health System & UT Health Science Center at San Antonio Department of Pharmacotherapy
Anticoagulants: New and Old. Dr. David Carr February 23 rd 2014
 Anticoagulants: New and Old Dr. David Carr February 23 rd 2014 Objectives: Anticoagulants Nailing down the challenges docs face in dealing with patients on warfarin Introducing the newish agents Reversing
Anticoagulants: New and Old Dr. David Carr February 23 rd 2014 Objectives: Anticoagulants Nailing down the challenges docs face in dealing with patients on warfarin Introducing the newish agents Reversing
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Reversal Agents for Anticoagulants Understanding the Options. Katisha Vance, MD, FACP Alabama Oncology January 28, 2017
 Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately
Reversal Agents for Anticoagulants Understanding the Options Katisha Vance, MD, FACP Alabama Oncology January 28, 2017 Objectives Appropriately recommend reversal agents for Vitamin K antagonists Appropriately