Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM. Disclosures
|
|
|
- Matthew May
- 5 years ago
- Views:
Transcription
1 Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1
2 Our history with OUD Harm reduction, in brief: HONESTY, NOT PERFECTION 2
3 Patient selection: most responsive to OBOT: People in 20s or older Have an addiction to prescription opioids, but people with heroin use are treatable also Want to stop Stable support system at home Employed Stable on buprenorphine, transferred from more intensive addiction treatment program, with coordination from that program Case: Bob 30 y.o. single man with chronic back pain, lives with his parents. Was already on prescription oxycodone for a few years before transferring to your practice. Increasing pattern of running out early in the past 3 months, and unexpected opioids in his drug screen. You diagnose OUD, discuss starting buprenorphine/naloxone Bob agrees, shows up in withdrawal, does induction and stabilizes on 12 mg of buprenorphine/naloxone. You plan to see him back in 1 week. 3
4 A call from Bob He calls Thursday afternoon says: I ran out early, I m still in pain, and I am not sleeping well! What do you do? Bob s story Was taking 4 mg film three times a day With breakfast, lunch and dinner 4
5 Absorption technique: buccal vs. sublingual Pharmacokinetics: Circadian rhythm considerations Delay between starting buprenorphine and noticing pain relief Can expect to see gradual improvement in pain relief over the next 2 months Can use adjunctive modalities and reassurance during this time Divide total dose and take 3 4 times per day for chronic pain Case 2: Cindy 39 y.o. woman, living at home with significant other who doesn t use any illicit substances, is supportive. Medical history significant for type I DM, on insulin, stable. Has been maintained on buprenorphine/naloxone for 1 year on 8 mg sublingual dose per day, had prior Rx opioid misuse with subsequent heroin use. Is currently stable, employed, and has Medicaid insurance. You ve been seeing her monthly, at last visit found out she got a job promotion. 5
6 Cindy s woes Calls on Wednesday afternoon that she has run out early by 3 days. What do you do? Recall HONESTY, NOT PERFECTION 6
7 Cindy s response Has diabetic neuropathy. With new job promotion, had increased stress and physical demands. Neuropathy became severely painful, she was not sure what else to do. Had taken a few half strips extra over the past week. Please help me out, I don t want to lose my job! What do you do? OBOT guidelines: Follow up Assess stability: Ongoing use of illicit substances Taking medications as prescribed, side effects Changes in social function work, relationships Changes in medical health/ consequences of use Counseling/ community support group participation If stable, use positive reinforcement: Allow more time between visits every 2 weeks, then monthly. Prescribe larger quantities of medication as people demonstrate stability policy on data 2000 and treatment of opioidaddiction in the medical office.pdf 7
8 Cindy in 2 months Has stabilized, taking divided doses as you suggested. Is grateful to have been understood and not cut off, agreed that coming in more often and having fewer strips available at a time was helpful for staying on track with counts. Started and found good relief of neuropathy from duloxetine. Is still stressed about new job. Can I get a dose increase of my Suboxone? I notice it s not lasting as long as it used to. What do you do? Role of therapy Counseling is a good adjunct, and often helpful Not necessary, and if person refuses, medication should not be withheld. However, medication can be used to leverage participation in counseling if there is need Counseling can help modulate stress response 8
9 Cindy Cindy tries counseling, learns some stress management techniques. After a few weeks, she is still noticing withdrawal symptoms later in the day. Now, what can you do? Tom: wants to start on MAT 35 y.o. Man, generally healthy, with daily heroin use, seeks your care. Is already taking lorazepam, 1 mg bid, for anxiety, prescribed by his PCP. He feels it is working well, has been on it for years. Hasn t tried much else for treatment. How do you proceed? 9
10 Common concerns: benzodiazepines Avoid concomitant prescriptions of opioids and benzodiazepines for risk of respiratory suppression. FDA in 9/2017: DON T withhold MAT from people taking benzodiazepines, but DO try other strategies for managing anxiety What is more deadly: heroin and benzodiazepines or buprenorphine and benzodiazepines? Enlist help of family member or use shorter prescriptions to avoid misuse. For Tom, suggest taper of lorazepam and try other anxiety medications as/ or before starting buprenorphine. Tom Tom, 35 y.o. man, now stable on 12 mg of buprenorphine/naloxone. Has been tapered off lorazepam successfully, and is doing well with sertraline and tizanidine as needed. He has done well with recovery, now stable for 1 year. Has dental procedure upcoming, horrible fear of dentist. Asks for something to help with anxiety. What do you do? 10
11 Mindy Mindy is a 48 y.o. Woman stable on 16 mg of buprenorphine/ naloxone for 1.5 years. Has done well with treatment, and has chronic arthritis. Her knee pain becomes worse in the winter, she slips and falls. Goes to the ER, tells them she is on buprenorphine. They call for assistance with pain management. What do you tell them? Common concerns: Acute Pain Management Usually continue buprenorphine through procedure Divide into more frequent doses (3 4 times per day vs. daily) Remember adjunctive pain measures: muscle relaxer, NSAID, ice, etc. If not sufficient, can use full agonist opioids plus buprenorphine but will often need % usual doses If hospitalized, or severe pain, can use fentanyl in monitored setting Ensure anxiety and depression, if present, are adequately treated Signals can often get confused 11

12 Mindy s surgery It is determined that she needs surgery to repair her broken leg. Surgeon and anesthesiologist call for direction about the buprenorphine/naloxone for the procedure. How do you advise Mindy and them? Anderson T et al. To Stop or Not, That is the Question. Anesthesiology 2017; 126:

13 Anderson T et al. To Stop or Not, That is the Question. Anesthesiology 2017; 126: Common concerns: Peri operative care Elective surgery: if anesthesia and major surgery, can stop buprenorphine before the procedure. If mild to moderate pain procedure, continue right through procedure (including delivery). Typical opioid doses for post operative pain will need to be % higher to account for tolerance. Prescribe these for as long as you would for someone who wasn t opioid dependent. Enlist help of family member or use shorter prescriptions to avoid misuse. 13
14 Peri operative management of buprenorphine patients Buprenorphine maintenance and muopioid receptor availability in the treatment of opioid use disorder: implications for clinical use and policy Mark K. Greenwalda,*, Sandra D. Comerb, and David A. Fiellin Drug Alcohol Depend November 1; 0: Case: Jack Jack is a 35 y.o. man who lives alone. Was using heroin, up to 1 g per day up to 3 months ago, when he started buprenorphine/naloxone with you. Otherwise healthy, no co morbidities Has been coming in every 2 weeks for buprenorphine/naloxone medication management, has stabilized on 16 mg sublingual dose per day. Last urine drug screen was positive for buprenorphine, on confirmation showed levels of 230 ng/ml, norbuprenorphine of 2000 ng/ml. 14
15 Urine Drug Screens: the basics.. And beyond Point of care is a SCREENING tool Adulterants as monitor for honesty Low temperature (falsified urine) Low creatinine (dilution) Abnormal ph Many false positives Can request buprenorphine metabolite levels once at a stable dose Opioid and benzodiazepine metabolism 15
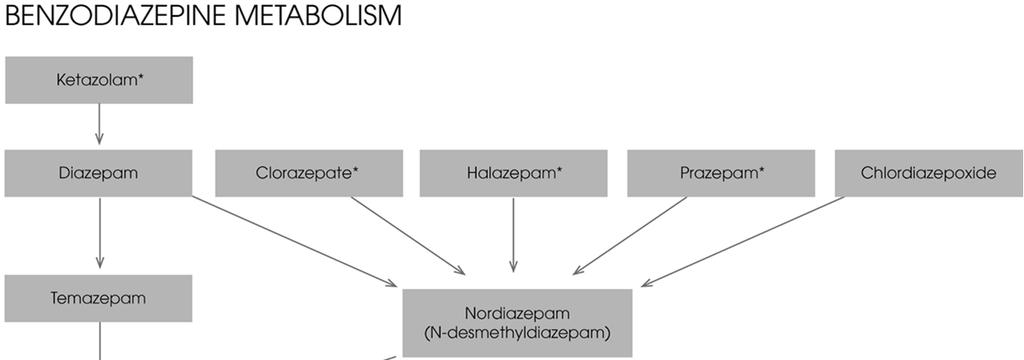
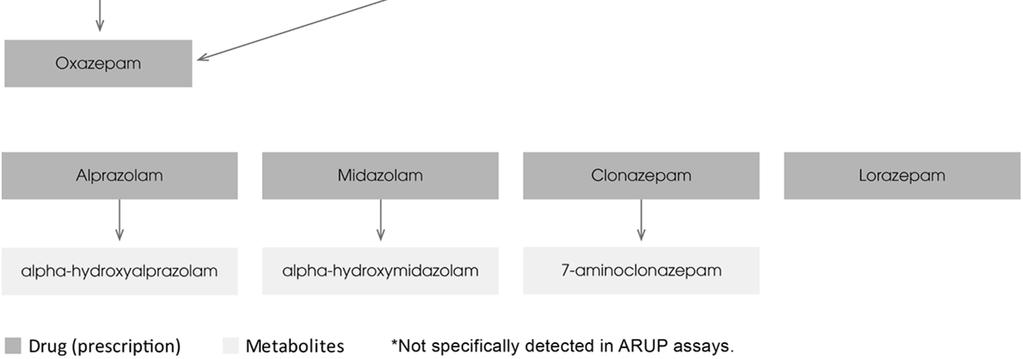
16 16
17 Helen 35 y.o. Woman, married, with 3 young children, h/o prescription opioid dependence for really bad migraine headaches. Now stable on 4 mg Suboxone daily for 6 months. On asking, you discover she has been drinking quite regularly with her husband to unwind, celebrate, and perhaps more often... What do you do? Alcohol biomarkers Help quantify the amounts over the last hours NOT a CLIA waived dipstick test, so can t always use this. These helped Helen be honest about the extent of her use. Counselor then discussed ways to cut down/ stop entirely. 17
18 Helen s challenge Harder to stop drinking alcohol than she realized Eventually realized anxiety was driving some of her drinking. Accepted sertraline for anxiety treatment. Also did well with topiramate to help reduce her cravings for alcohol, and helped her headaches, without weight gain. Are things going ok? Pattern of early refills Stolen/ lost medications Presence of other substances in urine drug screen Adulterated urine Drug screen confirmation: High buprenorphine, low (or absent) norbuprenorphine Diversion risk 18

19 What to do when Illicit substance use continues? Contingency Management processes for minor problems Invite person in for more frequent visits to discuss barriers to recovery Institute random pill/ film counts Random urine drug screens Reduced frequency of refills Can reduce dose Provide comfort medications Pt to file police report for stolen meds 19


20 Recognizing signs of IV drug use Track marks Hand, foot, leg, neck Long sleeves on hot days Do good physical exam Look for soft tissue/ skin infections When to refer Person is continuing to use other illicit substances Psychiatric co morbidity is interfering with treatment manage or refer to psychiatrist/ counselor Good to decide internal clinic rules for variability in progress: if presented early in treatment agreement, then not a surprise to person Consider harm reduction as part of the road to full recovery 20

21 21
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
2/7/2017. Avoid compassion traps. Avoid All or Nothing Traps. Some Explanatory Models of Addiction
 Avoid compassion traps Do you want me to lose my job, do you want me to be on the street? I want you to have safe and effective pain control and it is my medical opinion that your current medicine won
Avoid compassion traps Do you want me to lose my job, do you want me to be on the street? I want you to have safe and effective pain control and it is my medical opinion that your current medicine won
Principles and language suggestions for talking with patients
 SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers
 Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
AN INTRODUCTION TO THE TREATMENT OF OPIOID USE DISORDERS IN PRIMARY CARE
 AN INTRODUCTION TO THE TREATMENT OF OPIOID USE DISORDERS IN PRIMARY CARE Valerie Carrejo, MD Assistant Professor UNM Family Medicine Advances in Primary Care April 14, 2017 Objectives Review the basic
AN INTRODUCTION TO THE TREATMENT OF OPIOID USE DISORDERS IN PRIMARY CARE Valerie Carrejo, MD Assistant Professor UNM Family Medicine Advances in Primary Care April 14, 2017 Objectives Review the basic
John Murphy DO, MS Lynx Healthcare
 Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St.
 MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners, Albany, NY Assistant Professor of Medicine,
Agenda. Case Discussions. Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT. Daniel Alford, MD Disclosures
 in Patients on MAT. Daniel Alford, MD Disclosures") Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
OPIOIDS. Questions about opioids, and the Answers that may SURPRISE YOU. A booklet for people who may benefit from reducing or stopping their opioid
 OPIOIDS Questions about opioids, and the Answers that may SURPRISE YOU A booklet for people who may benefit from reducing or stopping their opioid Generic Name morphine hydromorphone oxycodone tramadol
OPIOIDS Questions about opioids, and the Answers that may SURPRISE YOU A booklet for people who may benefit from reducing or stopping their opioid Generic Name morphine hydromorphone oxycodone tramadol
OPIOIDS. Questions about opioids, and the Answers that may SURPRISE YOU. A booklet for people who may benefit from reducing or stopping their opioid
 OPIOIDS Questions about opioids, and the Answers that may SURPRISE YOU A booklet for people who may benefit from reducing or stopping their opioid Generic Name morphine hydromorphone oxycodone tramadol
OPIOIDS Questions about opioids, and the Answers that may SURPRISE YOU A booklet for people who may benefit from reducing or stopping their opioid Generic Name morphine hydromorphone oxycodone tramadol
The Social Worker s Role in Medication Assisted Treatment
 The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Recognizing Narcotic Abuse and Addiction and Helping Those With It
 Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment
 some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
Medication-Assisted Treatment (MAT) for Opioid Use Disorders
 for Opioid Use Disorders") Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Striking a Balance: a provider perspective.
 Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Screening, Identification, Counseling, and Treatment of Opioid Use Disorder
 Screening, Identification, Counseling, and Treatment of Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry, Harvard Medical School Director, Division of Addiction Psychiatry, Brigham
Screening, Identification, Counseling, and Treatment of Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry, Harvard Medical School Director, Division of Addiction Psychiatry, Brigham
About Your Pain Management
 UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions This handout outlines the goals of pain management treatment. It also reviews the guidelines that you are expected to
UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions This handout outlines the goals of pain management treatment. It also reviews the guidelines that you are expected to
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE BUPRENORPHINE/NALOXONE CLINIC VISITS
 Provider Name: NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE Provider Signature: Date: BUPRENORPHINE/NALOXONE CLINIC VISITS Once stable, schedule clinic visits every 2 to 4 weeks, with refills that coincide
Provider Name: NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE Provider Signature: Date: BUPRENORPHINE/NALOXONE CLINIC VISITS Once stable, schedule clinic visits every 2 to 4 weeks, with refills that coincide
About Your Pain Management
 UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions about opioids This handout explains the goals of managing pain with opioids, which are a type of prescription pain medicine.
UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions about opioids This handout explains the goals of managing pain with opioids, which are a type of prescription pain medicine.
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
OBSERVATION SHEET TOPIC CLINICAL SCENARIO. OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation)
") OBSERVATION SHEET TOPIC CLINICAL SCENARIO OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation) FEEDBACK: WHAT WENT WELL FEEDBACK: THINGS TO CONSIDER DEBRIEF: Observer
OBSERVATION SHEET TOPIC CLINICAL SCENARIO OBSERVATIONS MADE (Use the skills objectives/ provider tasks to evaluate the conversation) FEEDBACK: WHAT WENT WELL FEEDBACK: THINGS TO CONSIDER DEBRIEF: Observer
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics
 Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Patient and Family Agreement on Opioids
 Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
Today the overuse of opioids is a problem. Many of
 A PPENDIX B A Word About Opioid Use Today the overuse of opioids is a problem. Many of these opioids are prescribed and thus are legal. Other people steal or buy opioids on the streets. These are illegal.
A PPENDIX B A Word About Opioid Use Today the overuse of opioids is a problem. Many of these opioids are prescribed and thus are legal. Other people steal or buy opioids on the streets. These are illegal.
The science of the mind: investigating mental health Treating addiction
 The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
OPIOID PRESCRIBING RULES. May 17, 2017 Webinar
 OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
OUD & MAR: Caring for Our Communities
 OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION
 sublingual film (CIII) IMPORTANT SAFETY INFORMATION") SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
Treatment of Substance Use Disorders in the Real World. Jessica M. Peirce, Ph.D. Johns Hopkins University School of Medicine
 Treatment of Substance Use Disorders in the Real World Jessica M. Peirce, Ph.D. Johns Hopkins University School of Medicine Objectives identify the core components of the most common substance use disorder
Treatment of Substance Use Disorders in the Real World Jessica M. Peirce, Ph.D. Johns Hopkins University School of Medicine Objectives identify the core components of the most common substance use disorder
WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
The Challenging Patient with Chronic Opioid Usage MD ACP Meeting
 The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Steven Prakken MD Director Medical Pain Service Duke Pain Medicine
 Steven Prakken MD Director Medical Pain Service Duke Pain Medicine Misuse Abuse Addiction Total Pain Population Webster LR, Webster RM. Pain Med. 2005;6(6):432-442. DSM IV Abuse defined as 2 elements
Steven Prakken MD Director Medical Pain Service Duke Pain Medicine Misuse Abuse Addiction Total Pain Population Webster LR, Webster RM. Pain Med. 2005;6(6):432-442. DSM IV Abuse defined as 2 elements
History of Present Illness (HPI) Assessment and Plan Template
 Assessment and Plan Template") History of Present Illness (HPI) Assessment and Plan Template Templates for induction and follow-up appointments for medication assisted treatment (MAT) in opioid use disorder (OUD). Consider saving this
History of Present Illness (HPI) Assessment and Plan Template Templates for induction and follow-up appointments for medication assisted treatment (MAT) in opioid use disorder (OUD). Consider saving this
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain
 Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Latest Press Release. How much for 30 mg adderall
 corp@stantec.com Latest Press Release How much for 30 mg adderall S 14-2-2008 Hi my name is Rachel i have been on suboxone for almost a year as of OCT 1st, and I have become the person I guess I am to
corp@stantec.com Latest Press Release How much for 30 mg adderall S 14-2-2008 Hi my name is Rachel i have been on suboxone for almost a year as of OCT 1st, and I have become the person I guess I am to
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Treating Opioid Addiction
 Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Pain CONCERN. Medicines for long-term pain. Opioids
 Pain CONCERN Medicines for long-term pain Opioids Opioids are a group of medicines that come from the extract of poppy seeds or other medicines that work in the same way. Types of opioid The first opioids
Pain CONCERN Medicines for long-term pain Opioids Opioids are a group of medicines that come from the extract of poppy seeds or other medicines that work in the same way. Types of opioid The first opioids
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Prescription Drug Safety for Teens
 Prescription Drug Safety for Teens Curriculum Guide Recommended Grade Level 9-12 Total Time 30-45 minutes Subject Fit Health Standards Alignment National Health Education Standards (NHES) With prescription
Prescription Drug Safety for Teens Curriculum Guide Recommended Grade Level 9-12 Total Time 30-45 minutes Subject Fit Health Standards Alignment National Health Education Standards (NHES) With prescription
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
FACING ADDICTION OVER DINNER
 FACING ADDICTION OVER DINNER The NATIONAL NIGHT of CONVERSATION November 17, 2016 The dinner table is one of the most important places in the house for improving the health of your family, but not only
FACING ADDICTION OVER DINNER The NATIONAL NIGHT of CONVERSATION November 17, 2016 The dinner table is one of the most important places in the house for improving the health of your family, but not only
Traumatic Brain Injury and Sleep
 Traumatic Brain Injury and Sleep Javier has a hard time falling asleep and his lack of sleep made his anxiety worse. He Also became fatigued and irritable easily, It really made our lives harder. Sleep
Traumatic Brain Injury and Sleep Javier has a hard time falling asleep and his lack of sleep made his anxiety worse. He Also became fatigued and irritable easily, It really made our lives harder. Sleep
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER
 MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners Grand Rounds October 11, 2017 Disclosures One
MANAGING PAIN IN PATIENTS WITH SUBSTANCE USE DISORDER Melissa B. Weimer, DO, MCR Chief of Behavioral Health & Addiction Medicine St. Peter s Health Partners Grand Rounds October 11, 2017 Disclosures One
Medication Agreements Promoting awareness, dialogue and level-set expectations
 Medication Agreements Promoting awareness, dialogue and level-set expectations A young man had his leg amputated following a work-related injury. His pain doctor, by all accounts, was trying to responsibly
Medication Agreements Promoting awareness, dialogue and level-set expectations A young man had his leg amputated following a work-related injury. His pain doctor, by all accounts, was trying to responsibly
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
IntNSA Webinar Series
 BUPRENORPHINE CLINIC: A MULTIDISCIPLINARY MODEL FOR OPIOID MAINTENANCE THERAPY Stephen Strobbe, PhD, RN, NP, PMHCNS-BC, CARN-AP Monday, June 4, 2012 IntNSA Webinar Series Funding for this webinar was made
BUPRENORPHINE CLINIC: A MULTIDISCIPLINARY MODEL FOR OPIOID MAINTENANCE THERAPY Stephen Strobbe, PhD, RN, NP, PMHCNS-BC, CARN-AP Monday, June 4, 2012 IntNSA Webinar Series Funding for this webinar was made
PATIENT INTAKE: MEDICAL HISTORY. Name. Address. Phone (W) (H) (C) DOB Age SS# Emergency Contact. Relationship to patient Phone
 (H) (C) DOB Age SS# Emergency Contact. Relationship to patient Phone") PATIENT INTAKE: MEDICAL HISTORY Name Address Phone (W) (H) (C) DOB Age SS# Emergency Contact Relationship to patient Phone Primary care physician Phone Have you ever had an EKG? Y N Date Current or past
PATIENT INTAKE: MEDICAL HISTORY Name Address Phone (W) (H) (C) DOB Age SS# Emergency Contact Relationship to patient Phone Primary care physician Phone Have you ever had an EKG? Y N Date Current or past
STARTING SUBOXONE IN PRIMARY CARE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences STARTING SUBOXONE IN PRIMARY CARE MARK DUNCAN MD UNIVERSITY OF WASHINGTON OBJECTIVES 1. Review evidence of how to
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences STARTING SUBOXONE IN PRIMARY CARE MARK DUNCAN MD UNIVERSITY OF WASHINGTON OBJECTIVES 1. Review evidence of how to
Patient Information Form
 Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Basics of Benzodiazepine Use Disorder. DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction
 Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL
 OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Trends and Challenges: The Kentucky Opioid Crisis. Jason Smith, MD PhD University of Louisville
 Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
OPIOID PAIN MEDICATION Agreement and Informed Consent
 OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
MAT for Opioid Dependence. MAT and Pain Management. Epidemiology. Epidemiology. Factors Impacting Pain Perception 9/23/2014
 MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
MAT for Opioid Dependence Methadone maintenance treatment (MMT) Buprenorphine/naloxone (suboxone) Buprenorhine/naloxone (BupNX) Buprenorphine SL Parenteral naltrexone (P-ntx) Oral naltrexone (ntx) MAT
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT MARK DUNCAN MD UNIVERSITY OF WASHINGTON SPEAKER DISCLOSURES Any conflicts
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT MARK DUNCAN MD UNIVERSITY OF WASHINGTON SPEAKER DISCLOSURES Any conflicts
Acupuncture. Opioid Prescribing: Pitfalls for Occupational Medicine Physicians
 Opioid Prescribing: Pitfalls for Occupational Medicine Physicians Presented by Scott Levy M.D. M.P.H. FACOEM Assistant Regional Medical Director, Occupational Health Services The Permanente Medical Group
Opioid Prescribing: Pitfalls for Occupational Medicine Physicians Presented by Scott Levy M.D. M.P.H. FACOEM Assistant Regional Medical Director, Occupational Health Services The Permanente Medical Group
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Treatment of Pain in an Emergent Setting
 Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of Toronto
 Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Resist the Opioid Pendulum: Understanding Opioids and Pain, and how they relate to Addiction
 Resist the Opioid Pendulum: Understanding Opioids and Pain, and how they relate to Addiction Stefan G. Kertesz, MD, MSc Diplomate, American Board of Addiction Medicine Associate Professor, University of
Resist the Opioid Pendulum: Understanding Opioids and Pain, and how they relate to Addiction Stefan G. Kertesz, MD, MSc Diplomate, American Board of Addiction Medicine Associate Professor, University of
Patient information sheet: BuTrans Patch This information should be read in conjunction with the Taking Opioids for pain information leaflet
 Page 1 of 6 Patient information sheet: BuTrans Patch This information should be read in conjunction with the Taking Opioids for pain information leaflet What type of drug is it? BuTrans transdermal patches
Page 1 of 6 Patient information sheet: BuTrans Patch This information should be read in conjunction with the Taking Opioids for pain information leaflet What type of drug is it? BuTrans transdermal patches
What happens if you stop taking klonopin cold turkey
 Home Search What happens if you stop taking klonopin cold turkey Quitting oxycodone cold turkey. How long does it take withdrawals from stopping oxycodone to go away when you quit cold. What if you stop
Home Search What happens if you stop taking klonopin cold turkey Quitting oxycodone cold turkey. How long does it take withdrawals from stopping oxycodone to go away when you quit cold. What if you stop
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
The Chronic Disease of Addiction Evidence and Lessons from Practice
 The Chronic Disease of Addiction Evidence and Lessons from Practice Laura G. Kehoe, MD, MPH Medical Director, MGH Substance Use Disorders Unit Bridge Clinic Massachusetts General Hospital Assistant Professor
The Chronic Disease of Addiction Evidence and Lessons from Practice Laura G. Kehoe, MD, MPH Medical Director, MGH Substance Use Disorders Unit Bridge Clinic Massachusetts General Hospital Assistant Professor
National Council on Patient Information and Education
 National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
The Difficult Patient: Risk Mitigation Strategies
 The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
Opioids: Safe Use and Side Effects
 Opioids: Safe Use and Side Effects Your doctor has prescribed an opioid (OHpee-oyd). This drug can control moderate to severe pain without increased risk of bleeding and kidney problems. Always take the
Opioids: Safe Use and Side Effects Your doctor has prescribed an opioid (OHpee-oyd). This drug can control moderate to severe pain without increased risk of bleeding and kidney problems. Always take the
Opioid Prescribing for Acute Pain
 Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Medication Assisted Treatment in an Ideal Micro-Practice. Case: Typical Opioid Dependent Patient. John Machata, MD Wickford Family Medicine
 Medication Assisted Treatment in an Ideal Micro-Practice Case: Typical Opioid Dependent Patient John Machata, MD Wickford Family Medicine Micro Practice No Secretary No Nurse(¼ FTE NCM mandated by RI-CTC)
Medication Assisted Treatment in an Ideal Micro-Practice Case: Typical Opioid Dependent Patient John Machata, MD Wickford Family Medicine Micro Practice No Secretary No Nurse(¼ FTE NCM mandated by RI-CTC)