Management in Cirrhosis
|
|
|
- Reynold Townsend
- 5 years ago
- Views:
Transcription
1 Management in Cirrhosis
2 Outline Introduction Cause of cirrhosis and management General management in cirrhosis Management complication and surveillance
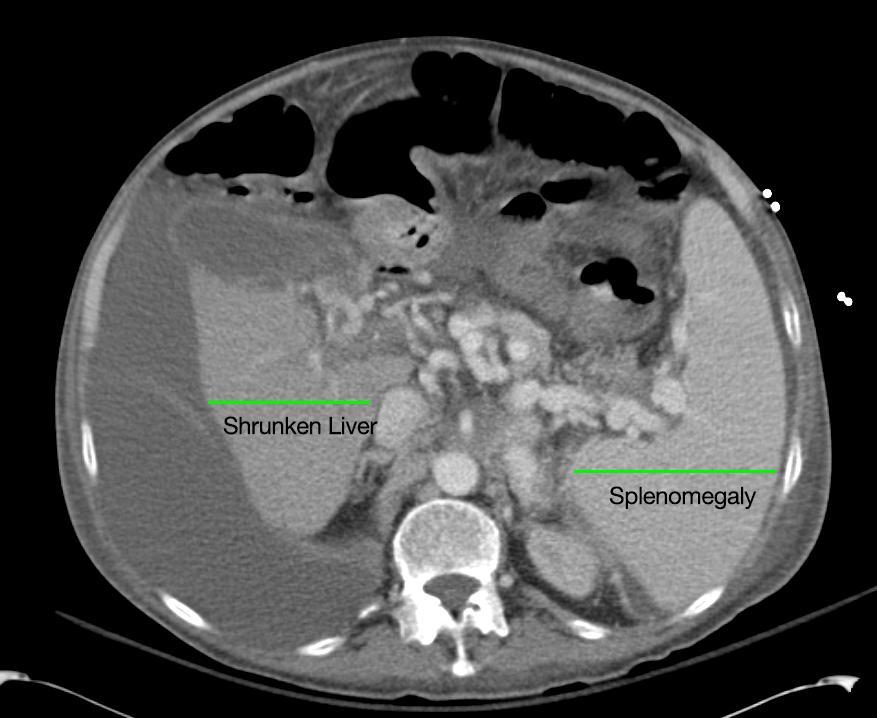
3 Clue of Chronic Liver Disease and Cirrhosis Risk factor Evidence of chronic liver disease Physical examination Sign CLD < 50% Sign portal Hypertension Laboratory AST/ALT > 1 Reverse AG ratio PT prolong Low platelet (<160000) Definite diagnosis : Liver biopsy Noninvasive test Biological Physiological






4
5 Serum Biomarker Advantages Transient elastography ARFI (pswe) 2D-SWE MR elastography Good reproducibility High applicability (95%) No cost and wide availability (non-patented) Well validated Can be performed in the outpatient clinic Most widely used and validated technique: standard to be beaten User-friendly (performed at bedside; rapid, easy to learn) High range of values (2-75 kpa) Quality criteria well defined Good reproducibility High performance for cirrhosis (AUROC >0.9) Prognostic value in cirrhosis Can be implemented on a regular US machine ROI smaller than TE but location chosen by the operator Higher applicability than TE (ascites and obesity) Performance equivalent to that of TE for significant fibrosis and cirrhosis Can be implemented on a regular US machine ROI can be adjusted in size and location and chosen by the operator Measures liver stiffness in real-time High range of values (2-150 kpa) Good applicability High performance for cirrhosis Can be implemented on a regular MRI machine Examination of the whole liver Higher applicability than TE (ascites and obesity) High performance for cirrhosis Disadvantages Non-specific of the liver Unable to discriminate between intermediate stages of fibrosis Performance not as good as TE for cirrhosis Cost and limited availability (proprietary) Limitations (hemolysis, Gilbert syndrome, inflammation...) Requires a dedicated device ROI cannot be chosen Unable to discriminate between intermediate stages of fibrosis Applicability (80%) lower than serum biomarker: (obesity, ascites, operator experience) False positive in case of acute hepatitis, extrahepatic cholestasis, liver congestion, food intake and excessive alcohol Unable to discriminate between intermediate stages of fibrosis Units (m/sec) different from that of TE (kpa) Narrow range of values ( m/sec) Quality criteria not well defined Prognostic value in cirrhosis? Further validation warranted Unable to discriminate between intermediate stages of fibrosis Quality criteria not well defined Learning curve? Influence of inflammation? Further validation warranted especially in comparison with TE Not applicable in case of iron overload Requires a MRI facility Time-consuming Costly
6 Complication Ascites SBP Varices(Esophageal, Gastric, Ectopic) Hepatorenal syndrome Hepatopulmonary syndrome Portopulmonary Hypertension Hepatic hydrothorax SBE Hepatic encephalopathy Hepatocellular carcinoma


7 Cirrhosis is a series of continuous and progressive stages, not a single stage Friedman S. Gastroenterology 2008
 D")

8 Clinical Course of Cirrhosis (Baveno IV) D Amico G., Garcia-Tsao G., Pagliaro L.J of Hepatol 2006;44:
9 Cause of cirrhosis Acute Chronic Viral A-E,CMV, EBV, Herpes Viral hepatits B and C Toxic Acetaminophen, Amanta, Alc, Drug Toxic Alcohol, MTX Ischemic Vascular BCS, SOS Metabolic Wilson Fatty liver Reye syndrome Autoimmune Liver disease Metabolic Wilson,Hemochromatosis alpha1 antitrypsin deficiency Fatty liver NASH Autoimmune Liver disease

10 Disorder Treatment Alcohol Viral hepatits B Viral hepatits C Wilson Hemochromatosis Autoimmune hepatitis Primary biliary cirrhosis NASH Quit alcohol, Nutritional support, Baclofen Peg-IFN NUC Peg-IFN with ribavirin DAA D penicillamine Zinc Phlebotomy Iron chelate for 2 nd hemochromatosis Prednisolone and Azathioprine UDCA Liver Transplantation MELD > 17 Weight reduction, Bariatric sx TZD Vitamin E
11 General management Correct cause : AIH, HBV, HCV, Alcohol Immunization : Hepatitis A, Hepatitis B Exercise Compensated without EV : ok EV : avoid isometric and weight training Surveillance Varices and HCC
12 General nutrition guidelines for cirrhosis kcal/kg dry body weight 50% - 60% of calories as carbohydrate 20% - 30% of calories as protein ( g/kg body weight) In hepatic encephalopathy : if patients is protein intolerant, consider increasing vegetable protein, dairy protein, and branched chain amino acids. 10% - 20% of calories as fat 4 7 small meals, late evening carbohydrate rich snack Low sodium diet (<2000 mg/d) only if ascites or edema Screen for deficiencies of serum zinc, calcium and vitamins A, D, E and K deficiency and supplement as needed
13 Management complication and surveillance Ascities Antibiotic prophylaxis in cirrhosis patient Esophageal varices Hepatorenal syndrome Hepatic encephalopathy Surveillance Varices and HCC

14 NO
15 Ascites Sodium restriction 2000 mg per day (88 mmol per day) Fluid restriction is not necessary Na < restrict lit or less than urine output Diuretic Single dose morning Spinololactone alone when minimal fluid overload Spinololactone furosemide 40 combination Shorten time to remove ascites and normokalemia Increase dose q 3-5 day No Edema : maximum 0.5 kg/day Edema : maximum 1 kg/day
16 Drug in cirrhosis patient Drugs To Be Avoided or Used With Caution NSAID Aminoglycoside ACEI and ARB PPI : increase risk of infection Propranolol in some condition?? Pain control in cirrhosis Avoid NSAID and Opioid Tramadol and Acetaminophen < 2-4 gm/day recommended Insomnia : Trazodone, Hydroxyzine Statin : Safely and maybe benefit
17
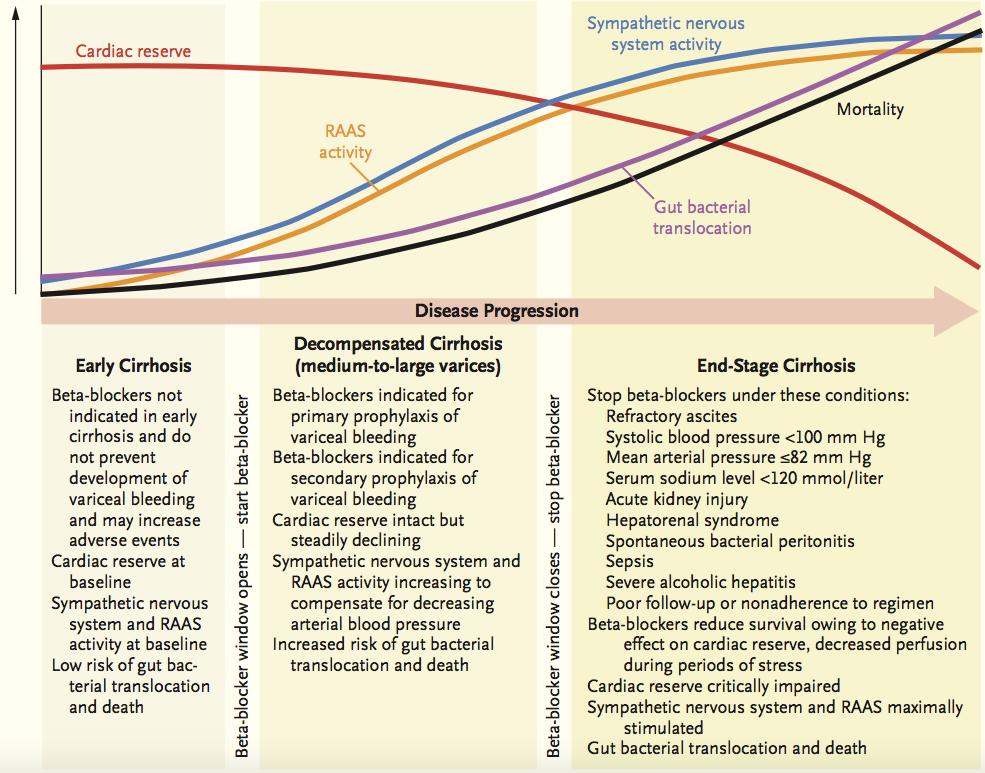
18 Beta blocker in Refractory ascites Close monitoring of BP, Cr, Na Reduce dose when Systolic blood pressure <90 mmhg Hyponatremia (<130 meq/l) Acute kidney injury
19 Refractory Ascites About 10 % Refractory ascites (Resistance) Unresponsive to sodium-restricted diet and high dose diuretic Recurs rapidly after therapeutic paracentesis Failure of diuretic therapy (Intractible) Minimal to no weight loss together with inadequate (<78 mmol per day) urinary sodium excretion despite diuretics Development of clinically significant complications of diuretics Encephalopathy Cr > 2.0 mg/dl Na <120 mmol/l K > 6.0 mmol/l
20 Treatment of refractory ascites Serial therapeutic paracenteses Liver transplantation Transjugular intrahepatic portasystemic stent-shunt (TIPS) Peritoneovenous shunt
21 Diagnosis of SBP Ascitic culture ANC (cell/mm 3 ) Negative < 250 Normal > 250 Culture-negative neutrocytic ascites Positive Monomicrobial nonneutrocytic bacterascites SBP CNNA -> 1/3 become culture positive MNBA -> 2/3 spontaneously resolved Culture no growth : 6 hrs ATB 86% Treatment Cefotaxime 2gm IV q 8 hr 5 days Ofloxacin 400 bid 8 days Without prior exposure to quinolones, vomiting, shock, HE grade II (or higher), Cr > 3 mg/ dl
22 Secondary peritonitis WBC many thousand Multiple organism 48 hr after treatment rising pretreatment 2/3 of Sugar < 50 TP > 1 LDH more than UNL Free perforate Sens 100, Spec 45% Non perforate sens 50% CEA > 5 or ALP > 240 Sens 92% Spec 88%
23 Antibiotic prophylaxis in cirrhosis 1 prophylaxis : prevent SBP and decrease mortality TP < 1.5 in ascites with Renal impair (Cr>1 or BUN > 25 or Na < 130) Liver impair (CPS 9 and TB 3) Norfloxacin 400mg OD 2 prophylaxis (Norfloxacin 400 od) : decrease SBP Recurrent SBP about 69% Everybody until no ascites or LT More drug resistance GI bleeding Ceftriaxone 1 gm V OD or Norfloxacin 400mg bid 7 days Decrease Rebleeding Infection and Short term Mortality
24 Variceal bleeding Acute Variceal bleeding Keep Hb 7-8 Vasoactive drugs (terlipressin(hypo Na), somatostatin, octreotide) should be used in combination with endoscopic therapy (In 12 hr) Early TIPS within 72 h Considered EV and GOV at high risk of treatment failure (CPG B to C (<14 points) with active bleeding) after fail treatment Primary prophylaxis (Propranolol, Nadolol, Carvedilol in primary) Medium to large varice (EVL or Beta blocker) Small with red wale mark sign or child C (Beta blocker) Secondary prophylaxis EVL + Betablocker Baveno VI. Journal of Hepatology 2015
25 Hepatorenal Syndrome Bleeding, paracentesis without plasma expansion, alcoholic hepatitis Bacterial infection, SBP Wong F et al. Gut 2011

26 Creatinine in cirrhosis effect by Muscle wasting Increase tubular secretion of creatinine Increase volume distributuin dilute createnine Interfere assay Cr by elevate bilirubin AKI as diagnosed with AKIN criteria associated with increased mortality in patients with cirrhosis in an AKIN stage-dependent fashion Urine NGAL suspected HRS Journal of Hepatology 2015 vol. 62 j


27 ICA-AKI criteria Journal of Hepatology 2015 vol. 62 j

28 2-4 day in hospital 2-4 wk outpatient
29 Prevention Albumin infusion in the setting of spontaneous bacterial peritonitis LVP Pentoxifylline Severe alcoholic hepatitis Cirrhosis, ascites, and creatinine clearances between 41 and 80 ml/min
30 Therapy for HRS Liver transplantation for both type TIP for bridging?? Vasoconstrictors and albumin reduce mortality on type 1 not type 2 (Terlipressin, norepinephrine, midodrine+ octreotide)
31
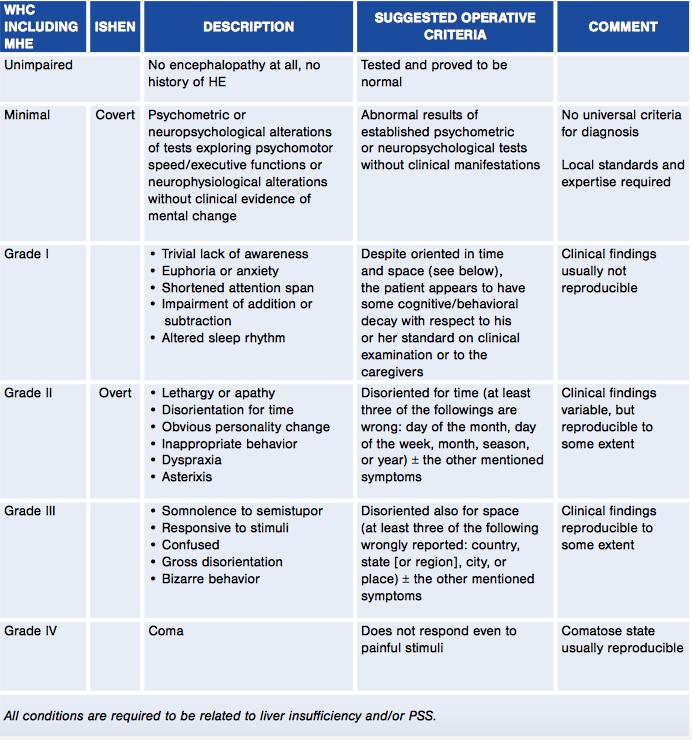
32 Hepatic encephalopathy Treatment convert hepatic encephalopathy in some condition (e.g., impairment in driving skills, work performance, quality of life, or cognitive complaints) Treatment in Overt hepatic encephalopathy Lactulose (2-3 bowel movement per day) is first line Oral BCAA,IV LOLA Neomycin, Metonidazole LT No primary prophylaxis Secondary prophylaxis for overt hepatic encephalopathy Lactulose Lactulose + Rifaximin Total calories : kcal/kg Ideal BW Total protein gm/kg/day (Restrict only first few day in overt HE)
33 Surveillance Surveillance Esophageal Varices (Liver stiffness < 20 and Plt > low risk) EGD q 2-3 yrs if no EV EGD q 1-2 yr if small EV Surveillance HCC U/S q 6-12 mth ± AFP
34 Surveillance HCC Cirrhosis Child A-B Child C with transplantation list CH-B Male > 40 years Female > 50 years HCC in first degree relative CH-C with fibrosis 3 U/S q 6-12 month +/- AFP
35
36 High AFP > 20 ng/ml 2 with normal U/S W/U other cause and F/U AFP 3-4 month Decrease AFP : Surveillance regular No decrease AFP : Dynamic imaging

37 Decrease readmisson, Mortality and Expenditure
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Care of the Patient With Cirrhosis
 REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
REVIEW Care of the Patient With Cirrhosis Anitha Yadav, M.D., and Hugo E. Vargas, M.D. Caring for patients with cirrhosis involves multidisciplinary and timely management of several complications while
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Optimal management of ascites
 Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Optimal management of ascites P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology Conference National Conference
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation
 Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
Primary Prophylaxis against Variceal Hemorrhage Pharmacotherapy vs Endoscopic Band Ligation Siwaporn Chainuvati, MD Faculty of Medicine Siriraj Hospital Outline Natural history of esophageal varices Which
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY
 COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
COMPLICATIONS OF CIRRHOSIS: ASCITES & HEPATIC ENCEPHALOPATHY DR. ESTER YAGUDAYEVA CLINICAL PHARMACIST HOSPICE PHARMACY SOLUTIONS OBJECTIVES Understand the prognosis of End Stage Liver Disease (ESLD) Identify
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Non-Invasive Testing for Liver Fibrosis
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Non-Invasive Testing for Liver Fibrosis John Scott, MD, MSc Associate Professor, University of Washington Associate Clinic Director, Hep/Liver Clinic, Harborview
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Non-Invasive Testing for Liver Fibrosis John Scott, MD, MSc Associate Professor, University of Washington Associate Clinic Director, Hep/Liver Clinic, Harborview
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France
 Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS
 NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Managing Cirrhosis. Cirrhosis of the liver is a progressive, fibrosing. Ascites. By Cameron Ghent, MD, FRCPC. Complications of Cirrhosis
 Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
Focus on CME at the University of Western Ontario Managing Cirrhosis By Cameron Ghent, MD, FRCPC Cirrhosis of the liver is a progressive, fibrosing process resulting in nodule formation and microvascular
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS
 MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
MANAGING END STAGE LIVER DISEASE IN RESOURCE LIMITED SETTINGS Mark W. Sonderup Division of Hepatology and Liver Laboratory Department of Medicine University of Cape Town & Groote Schuur Hospital Cirrhosis..
Management of Alcoholic Liver Disease. Hafez Fakheri Professor of medicine, Sari, Iran
 Management of Alcoholic Liver Disease Hafez Fakheri Professor of medicine, Sari, Iran Alcoholic Hepatitis Scores DF = (4.6 x [ PT- control PT]) + (bili ) MELD = 10 * ((0.957 * ln(cr)) + (0.378 * ln(bil))
Management of Alcoholic Liver Disease Hafez Fakheri Professor of medicine, Sari, Iran Alcoholic Hepatitis Scores DF = (4.6 x [ PT- control PT]) + (bili ) MELD = 10 * ((0.957 * ln(cr)) + (0.378 * ln(bil))
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
ASCITES. Dr KS Cheung Queen Mary Hospital
 ASCITES Dr KS Cheung Queen Mary Hospital Outline Pathophysiology Differential diagnosis of ascites Diagnostic paracentesis Ascitic fluid analysis Management of Ascites Management of spontaneous bacterial
ASCITES Dr KS Cheung Queen Mary Hospital Outline Pathophysiology Differential diagnosis of ascites Diagnostic paracentesis Ascitic fluid analysis Management of Ascites Management of spontaneous bacterial
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Pretreatment Evaluation
 Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Minimizing Complications in Cirrhosis
 Minimizing Complications in Cirrhosis Luis S. Marsano, MD, FACG, FAASLD Professor of Medicine Director of Clinical Hepatology University of Louisville & Louisville VAMC 2016 Nutrition in Cirrhosis What
Minimizing Complications in Cirrhosis Luis S. Marsano, MD, FACG, FAASLD Professor of Medicine Director of Clinical Hepatology University of Louisville & Louisville VAMC 2016 Nutrition in Cirrhosis What
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Transient elastography the state of the art
 Transient elastography the state of the art Laurent CASTERA, MD PhD Department of Hepatology, Hôpital Beaujon, Clichy Université Paris-7, France White Nights of Hepatology, St Petersburg, Russia, june
Transient elastography the state of the art Laurent CASTERA, MD PhD Department of Hepatology, Hôpital Beaujon, Clichy Université Paris-7, France White Nights of Hepatology, St Petersburg, Russia, june
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Topics to be covered
 Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Caring for the patient with cirrhosis Role of the hospitalist Danielle Brandman, MD, MAS Associate Professor of Clinical Medicine Associate Program Director, Transplant Hepatology Fellowship October 18,
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Initial Evaluation for HCV Therapy. Hope McGratty PA-C, MPH
 Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed?
 CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
CLINICAL How Should a Hospitalized Patient with Newly Diagnosed Cirrhosis Be Evaluated and Managed? The Hospitalist. 2016 August;2016(8) Author(s): Raj Sehgal, MD; Joshua Hanson, MD, MPH; Division OF The
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Program Disclosure. This program is supported by an educational grant from Salix Pharmaceuticals.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship
Transient elastography in chronic viral liver diseases
 4 th AISF POST-MEETING COURSE Roma, 26 Febbraio 2011 Transient elastography in chronic viral liver diseases CRISTINA RIGAMONTI, M.D., Ph.D. Transient elastography (TE): a rapid, non-invasive technique
4 th AISF POST-MEETING COURSE Roma, 26 Febbraio 2011 Transient elastography in chronic viral liver diseases CRISTINA RIGAMONTI, M.D., Ph.D. Transient elastography (TE): a rapid, non-invasive technique
RENAL DISEASE IN END STAGE LIVER DISEASE
 RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Hepatology For The Nonhepatologist
 Hepatology For The Nonhepatologist Andrew Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois Learning Objectives After attending this presentation, learners will be able
Hepatology For The Nonhepatologist Andrew Aronsohn, MD Associate Professor of Medicine University of Chicago Chicago, Illinois Learning Objectives After attending this presentation, learners will be able
Hepatorenal Syndrome and AKI in Cirrhosis
 Hepatorenal Syndrome and AKI in Cirrhosis Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 HRS Hepatorenal
Hepatorenal Syndrome and AKI in Cirrhosis Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 HRS Hepatorenal
Clinical Practice Guidelines for the Cirrhosis of Liver 2017 Development Committee
 1 P a g e C l i n i c a l P r a c t i c e G u i d e l i n e s f o r t h e c i r r h o s i s o f l i v e r 2 0 1 7 FOREWORD Cirrhosis of the liver is very common in Myanmar as the consequence to chronic
1 P a g e C l i n i c a l P r a c t i c e G u i d e l i n e s f o r t h e c i r r h o s i s o f l i v e r 2 0 1 7 FOREWORD Cirrhosis of the liver is very common in Myanmar as the consequence to chronic
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Nutritional Issues In Advanced Liver Disease. Corrie Clark, RDN, LD
 Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Variceal bleeding. Mainz,
 Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Variceal bleeding Mainz, 21.09.2008 Risk of complications 5 years 10 years Ascites 10 % 25 % HCC 10 % 25 % Bleeding < 5 % 5-10 % Enceph. < 5 % < 5 % Typical situation : Mortality 10 % to 40 % Sequence
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
Screening for Portal Hypertension in Cirrhosis
 Screening for Portal Hypertension in Cirrhosis MASSIMO PINZANI, MD, PhD, FRCP Sheila Sherlock Chair of Hepatology UCL Institute for Liver and Digestive Health Royal Free Hospital, London, UK m.pinzani@ucl.ac.uk
Screening for Portal Hypertension in Cirrhosis MASSIMO PINZANI, MD, PhD, FRCP Sheila Sherlock Chair of Hepatology UCL Institute for Liver and Digestive Health Royal Free Hospital, London, UK m.pinzani@ucl.ac.uk
EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis
 EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis European Association for the Study of the Liver 1 Ascites is the
EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis European Association for the Study of the Liver 1 Ascites is the
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT.
 Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Pretreatment Evaluation
 Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Pretreatment Evaluation Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study Key personnel for FOCUS HCV Screening Program through Vanderbilt University
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified