Circulation T. Manchester July 5 th 2006
|
|
|
- Wesley Garrett
- 6 years ago
- Views:
Transcription
1 Circulation T Manchester July 5 th 2006
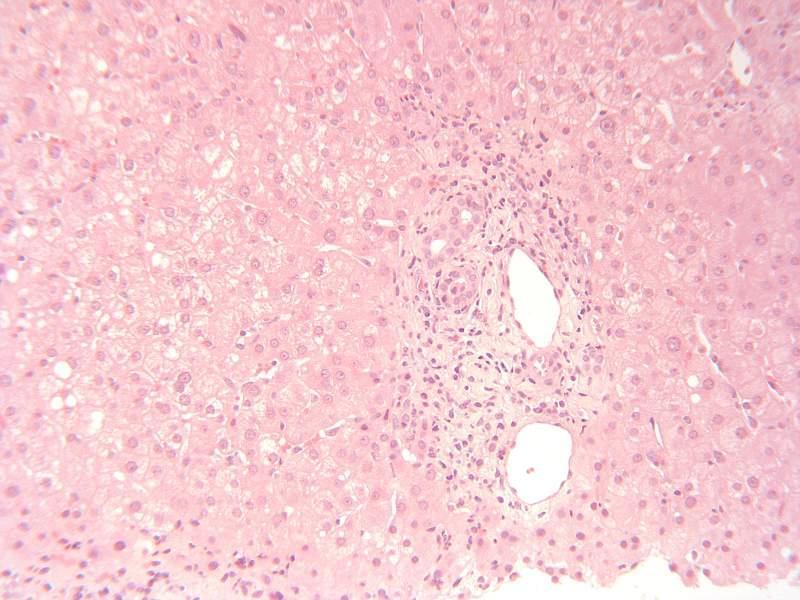
2 Case year old female with polycystic disease Section from explanted liver.

3 Case 242

4 Case 242

5 Case 242

6 Case 242

7 Case 242
8 Case Congenital hepatic fibrosis 13 Autosomal recessive polycystic kidney disease 11 in the spectrum of polycystic disease 3 ductal plate malformation 3?caroli s
9 Case 242 Scoring: Accept all diagnoses Discussion: The dilatation of large ducts against the background of congenital hepatic fibrosis indicates that this is an example of Caroli s syndrome (dilatation of intra-hepatic ducts + congenital hepatic fibrosis), rather then congenital hepatic fibrosis alone.
10 Case 242 Follow up: The clinical details received with this liver were ' polycystic disease'. The patient had one episode of early acute rejection at which time we were also told that there had been a combined liver and kidney transplant performed as there had been previous bilateral nephrectomy in another hospital for cystic kidneys. No further biopsies have been received and therefore the patient is presumed to be doing well.
11 Case female Liver nodule noted at time of organ transplantation Liver wedge biopsy 4mm pale tan nodule on wedge

12 Case 243

13 Case 243

14 Case 243


15 Case 243 nodule Background liver

16 Case 243 Background liver
17 Case adenoma 4 FNH or benign? FNH 3 benign?adenoma or FNH 3 regenerative or hyperplastic nodule 2 regenerative nodular hyperplasia 2 focal fatty change or adenoma 3 focal steatosis comments: steatosis in the adenoma 13 mild hepatitis in background liver 4
18 Case 243 Scoring: Accept responses that indicate this is a focal benign hepatocellular lesion (see comment) Discussion: perhaps best characterized as a focal benign hepatocyte lesion this lacks characteristics of adenoma (because it is encapsulated, with no unaccompanied arteries in the lesion) as well as lacking characteristics of focal nodular hyperplasia. Responses that did not indicate the focality of the lesion where rejected. Regenerative nodular hyperplasia is a diffuse change without fibrosis and focal steatosis is seen as a patch of fatty change within a group of liver cells with no architectural alteration.
19 Case female Alcoholic liver disease,? Cirrhosis 2 cores of tissue up to 10mm long (H&E and HVG slides)


20 Case 244

21 Case 244

22 Case 244

23 Case 244

24 Case 244

25 Case 244
26 Case Alcoholic steatohepatitis 6 alcoholic liver disease, not otherwise specified 1 no mention of alcohol 20 severe fibrosis 18 developing/incomplete cirrhosis 3 early cirrhosis 11 Cirrhosis 2 central sclerosing hyaline necrosis Comments:? sickle cells 2
27 Case 245 Scoring: for full marks, answers require alcohol, steatohepatitis and at least marked fibrosis to be included in response; half marks if part is missing Discussion around one use of alcohol in diagnosis most diagnose alcoholic liver disease when there is a history of excessive alcohol consumption supplied, and suggest alcoholic aetiology if no history of alcohol is given. Anecotally, this has caused problems where a given history of alcohol on the request form was subsequently found to be erroneous. However, pragmatically a case can be reported as consistent with alcohol if the alcohol history is supplied.
28 Case 245 The criteria for steatohepatitis Ballooned hepatocytes, Mallory bodies, and sinusoidal fibrosis in this case indicate that steatohepatitis is appropriate terminology even though there is no inflammatory cell component either in portal tracts or parenchyma. It was commented that as steatohepatitis resolves, the order of disappearance of features is polymorphs then fat then ballooning then Mallory s then fibrosis. As the lesion evolves over time, it is accepted to diagnose steatohepatitis without requiring the presence of inflammatory cells.
29 Case 244 Discussion contd: Fibrosis As long as vascular relationships appear preserved, as in this case, a diagnosis of established cirrhosis was probably not appropriate. Developing cirrhosis or severe fibrosis is more accurate here. Clearly there can be portal hypertension as a result of sinusoidal fibrosis without implying that cirrhosis has developed. Sclerosing central hyaline necrosis, as answered by 2, is the most appropriate terminology in this case. Follow-up information Clinical history was of high alcohol (4 bottles of wine per night for the last 18 months), admitted with jaundice and liver failure and bleeding varicies. Varicies banded difficult to manage and eventually died from variceal haemorrhage.
30 Case male History of SLE and sarcoidosis abnormal LFTs alk phos 164, gamma GT 326, IgG 17.4, ANA 1:640, dsdna >300, smooth muscle b ++ Needle core 28mm long

31 Case 245

32 Case 245

33 Case 245

34 Case 245

35 Case 245
36 Case 245
37 Case granulomas/granulomatous inflammation 3 granulomas not mentioned 2 slide missing 50 most likely sarcoidosis 3 sarcoidosis and/or SLE 1 sarcoidosis and AIH 1 sarcoidosis and AIH/SLE/PBC 1 sarcoidosis and veno-occlusive disease exclude TB/request ZN 27 needs AMA 3 need copper-protein 4 comment that granulomas are a feature of SLE several
38 Case 245 Scoring: Accept all diagnoses mentioning granulomas and sarcoidosis Discussion: The auto-antibodies may be associated with the separate clinical diagnosis of SLE, but there is thought to be insufficient histological evidence to suggest a component of autoimmune hepatitis.
39 Case 245 Follow up Diagnosis: granulomatous hepatitis, most likely sarcoidosis Evidence for diagnosis of sarcoidosis: Clinical diagnosis sarcoidosis and SLE 1 year after this biopsy,developed granulomatous skin lesion, diagnosed as sarcoid AMA ve LFTs currently normal apart from mildly raised GGT
40 Case M Hep C RNA positive genotype 1? For treatment

41 Case 246

42 Case 246

43 Case 246

44 Case 246
45 Case HCV 2 hepatitis C not mentioned 3 steatohepatitis, lacking usual features of hepatitis C 33 Also steatosis 3 Also steatohepatitis Additional clinical cause for steatosis: 12 Histology would indicate treatment if clinically appropriate 13
46 Case 246 contd. Severity: No comment on grade or stage 2 Mild chronic hepatitis 2 Moderate chronic hepatitis 1 inflammation Rest not possible to assess fibrosis without connective tissue stain Text:inflammation Ishak score - grade mild Mild-moderate Moderate marked Text - fibrosis Ishak stage Mild Mild-moderate Bridging Not marked 2 3 3
47 Case 246 Scoring: Reject answers that do not mention hepatitis C, or suggest the liver disease is other than due to hepatitis C; half marks if there in no comment on severity Discussion: The table of degrees of severity included so that individual can place themselves amongst their peers. Some of the spread in severity may be due to the widely variable amount of tissue in the slides.
48 Case 246 Follow up Dr Finlayson Ex-IVDU, was also drinking 2 bottles wine per day 4 months before biopsy, macrocytosis ALT 238 USS coarse texture, HCV combination therapy started.
49 Case M 6cm tumour in segment 8. probable focal nodular hyperplasia on imaging. Incidental finding. Laparoscopic tumour resection Several pieces of granular brown tissue up to 1.5cm

50 Case 247

51 Case 247

52 Case 247

53 Case 247
54 Case Focal nodular hyperplasia 2? telangiectatic FNH 1?cholangiocarcinoma? state of background liver 7
55 Case 247 Scoring: Accept all except cholangiocarcinoma.
56 Case M Jaundice. Special stains are negative for HBsAg, alpha 12 antitrypsin, copper, copper associated protein an haemosiderin. Core of brown tissue, 17x1mm
57 Case 248

58 Case 248

59 Case 248

60 Case 248

61 Case 248

62 Case 248
63 Case 248 Morphology/only diagnosis: 33 Cholestasis + inflammation/ cholestatic hepatitis 4 cholestasis and cholangiolitis 11 PSC 4 large duct obstruction 1 PSC or large duct obstruction 1 chronic hepatitis with biliary features 2 no mention of cholestasis or biliary disease anywhere in answer As main/most likely/only cause: 20?Drug reaction 10?PSC 4?large duct obstruction 1?ascending cholangitis differential diagnosis including: 13 drugs 12 PSC 1 PBC 4 large duct obstruction comments: autoantibodies 6 ERCP 16 Several mentioned periductal fibrosis No copper associated protein therefore not PSC/PBC 2
64 Case 248 Scoring: Insufficient concensus for scoring. Discussion: This was a cholestatic liver biopsy in which the changes appeared recent, and suggested of drugs. Because of periductal fibrosis in one portal tract, several responses were PSC with no qualification. In practice, in view of the absence of any fibrosis, ductopaenia, or copper associated protein, this case lacks sufficient histological features to allow an unqualified diagnosis of PSC. Canalicular cholestasis would also be unusual in early stage PSC.
65 Case 248 Follow up Diabetic, treated for foot ulcer with penicillin, then admitted with painless jaundice. US and CT negative. Fibrosis surrounding duct, so booked for MRCP. Autoantibodies and viral serology negative responded to prednisolone but developed perforated DU, surgically treated but died. No PM. Conclusion: painless jaundice most likely drug related.
66 Case F Liver bio9psy presented with non=specific illness/malaise. US multiple lesions in liver,?hydatid cysts,?mets. Also has lesions in spleen Wedge biopsy piece of tissue measuring 2.5x1x1cm. The cut surface shows irregular white foci.

67 Cased 249

68 Case 249

69 Case 249

70 Case 249
71 Case abscess with actinomycosis 2 abscess with aspergillus 1 hydatid (saw hooklets) 4 abscess with no organisms mentioned 1 abscess with possible bacterial colonies Comments:? primary source of infection 7?immunocompromised 8? IUCD 7
72 Case 249 Scoring: reject responses that do not include actinomycosis Discussion: Sufficiently characteristic for diagnosis of actinomycosis, although in real life would require confirmation by Gram and Grocott stains. The importance of mentioning actinomycosis was underlined by experience of a different case where this had been overlooked in original biopsy, resulting in multiple resections for unrecognized disseminated disease.
73 Case M Patient with ulcerative colitis on mesalazine (long term). Recent history of jaundice, AAT 1212; alk phos 230; total bilirubin 29; anti-smooth muscle antibody +++; antinuclear antibody 1:640; ferritin>2000; viral screen negative, no alcohol, no increase in collagen on connective tissue stains.

74 Case 250

75 Case 250

76 Case 250

77 Case 250

78 Case 250

79 Case 250

80 Case 250

81 Case 250
82 Case hepatitis, of which: 16 Hepatitis NOS 6 cholestatic hepatitis 14 acute hepatitis 4 subacute hepatitis 18 chronic hepatitis 7 no evidence of PSC 7 PSC a possibility 2 PSC/AIH overlap 2 alpha 1 antitrypsin deficiency (both also diagnosed autoimmune hepatitis) needs ERCP: 6 needs orcein 8 needs Perls 4 Aetiology: 31 autoimmune most likely or only diagnosis 16 drugs most likely or only diagnosis 5 drugs/aih equal 2 viral/drugs/autoimmune equal 1 viral or drug 8 autoimmune included in differential 13 drugs included in differential 9 autoimmune not mentioned 21 drugs not mentioned 8 answer implies awareness of association of autoimmune hepatitis in long term users of mesalazine (ref: Gut 99;44;886-8)
83 Case 250 Scoring: Responses that included hepatitis, aetiology of rautoimmune and/or drug related accepted Discussion: Terminology for Hepatitis as acute versus chronic in this case there is no fibrosis and the inflammation is predominantly lobular, and the history is acute therefore acute hepatitis would seem more appropriate. However, current terminology for autoimmune hepatitis is not to designate either acute or chronic, since these cannot be reliably be determined from histology, and acute presentations of autoimmune hepatitis are becoming well recognized.
84 Case 250 Discussion contd. Aetiology The presence of appropriate autoantibodies associated with hepatitic histology is sufficient for diagnosis of autoimmune hepatitis. In this case portal tracts eosinophils are readily identified, whereas interface hepatitis with plasma cells is more difficult to find. Mesalazine is reported as causing chronic hepatitis with autoantibodies; whether Mesalazine had caused the hepatitis, could not be known, as steroids were given and mesalazine withdrawn at the same time. (Ref: Deltenre et al. Mesalazine (5-ASA) induced chronic hepatitis. Gut 99;44;886-8).
85 Case 250 Follow up Patient had been taking mesalazine for several years prior to presentation The mesalazine was stopped after presentation. No other hepatotoxic drugs ERCP not done Perls stain negative Good response to steroids, LFTs normal and have remained so.
86 Case M Previous Dukes B carcinoma of transverse colon, 1 year earlier. Now has recurrence at ileo-sigmoid anastomosis. Site resected and solitary nodule? metastasis seen in gallbladder bed and resected. Segment 5 liver: 62g wedge of liver measuring 7x4.5x3.5cm. WShite nodular lesion on cutting this measuring 2cm diameter. Firm white appearance.

87 Case 251

88 Case 251

89 Case 251


90 Case 251

91 Case 251

92 Case 251
93 Case solitary necrotic nodule 6 infarcted nodular lesion? metastasis 1 chemotherapy induced necrosis of metastasis 1 consistent with metastatic adenocarcinoma 1 fibrous nodule 1 infarcted pseudotumour 1 inflammatory pseudotumour 1 nodule with pigmented ghost cells?? melanoma?? adenoma 2 infarction, no malignancy and steatosis 18 and steatohepatitis 2 differential includes post treatment metastasis 10 no evidence that this was a metastasis 19? previous surgery (gall bladder) 4? previous chemotherapy 13 lymphoma possible 2 needs ZN 2 needs reticulin 4 needs cytokeratin IHC 6
94 Case 251 Scoring: insufficient concensus for scoring Discussion; Solitary necrotic nodule as originally described was a small hyalinised nodule with some surrounding pallisading histiocytes, believed to be attributed to parasitic infection. Thus different from the histology in this case, which is larger with clearly central necrosis that was originally cellular. Participants have seen examples of post-chemotherapy metastases with this histology, although in the absence of any identifiable tumour morphology, an origin as metastatic carcinoma could not be confirmed. The history of previous chemotherapy was not available when slides were circulated. Although the correct answer was tumour regression following chemotherapy, there was not sufficient consensus to allow scoring.
95 Case 251 Follow up Diagnosis: solitary necrotic nodule Dukes B adenocarcinoma resected 1 year previously, liver mets seen at that time. Oxaliplatin chemotherapy prior to liver resection; (the cholecystectomy was at the time of this liver resection, not previously) All of the nodule was blocked no viable adenocarcinoma, subsequently immunohistochemistry shows no positivity for epithelial markers.
96 Case F Abnormal liver function tests, alp phos 253, GGT 395. Autoantibodies negative apart from smooth muscle antibodies +++ History of rheumatoid arthritis and thyroid disease.?autoimmune hepatitis. -ve ZN on biopsy 3 fragments of liver, combined length 14mm

97 Case 252

98 Case 252

99 Case 252

100 Case 252

101 Case 252

102 Case 252
103 Case granulomas/granulomatous hepatitis, with further comment about aetiology 4 granulomatous hepatitis, no further comment 4 granulomas and ductopaenia 3 PBC as main diagnosis, with differential 1 PBC as only diagnosis without qualification Aetiology: 32 sarcoidosis 21 TB must be excluded (stated in diagnosis box) 12 TB not mentioned anywhere or implied in comments 8 sarcoid/tb/pbc/drug with no preference 6 AMA ve PBC a possibility 11 differential diagnosis includes drugs 4 granulomas associated with rheumatoid arthritis Further information required: ZN lots AMA 4 Orcein 4 CXR 3 Drug history 3
104 Case 252 Scoring; Reject PBC as only diagnosis without qualification Discussion: Correct answer required recognition of granulomas, with some discussion of differential. The biopsy was not considered diagnostic of PBC without qualification. There are no mitochondrial antibodies. Definitive clinical diagnosis not yet available.
105 Case 252 Follow up: Diagnosis: Granulomatous hepatitis Multiple levels through the biopsy showed no evidence of bile duct damage associated with the granulomas Anti mitochomdrial antibodies were negative
106 Case M Hepatomegaly, GGT 450, alcoholic history 3 tan cores of tissue, from 7-20 mm

107 Case 253

108 Case 253

109 Case 253

110 Case 253

111 Case 253
112 Case amyloid 1 no answer (number of words in answer varies from 0 to 81!) differential of light chain deposition disease, if Congo red negative 4 some comment on clinical differential diagnosis 25
113 Case 253 Scoring: accept all responses Follow up: Further investigation showed normal renal and cardiac function, no paraprotein or Bence Jones but there was immunoparesis and 10% plasma cells in marrow. Referral to national amyloid centre for SAP scan confirmed uptake in Liver and Spleen and a high level of free AL light chain in blood. He has been started on high dose chemo.
Chronic Biliary Disease. Dr Susan Davies & Dr Bill Griffiths
 Chronic Biliary Disease Dr Susan Davies & Dr Bill Griffiths Chronic Biliary Disease Terminology is confusing with pathologists and hepatologists using the same language BUT with different meanings. Chronic
Chronic Biliary Disease Dr Susan Davies & Dr Bill Griffiths Chronic Biliary Disease Terminology is confusing with pathologists and hepatologists using the same language BUT with different meanings. Chronic
Slide 7 demonstrates acute pericholangitisis with neutrophils around proliferating bile ducts.
 Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
Many of the histologic images and the tables are from MacSween s Pathology of the Liver (5 th Edition). Other images were used from an online source called PathPedia.com. A few images from other sources
Biliary tract diseases of the liver
 Biliary tract diseases of the liver Digestive Diseases Course Bucharest 2016 Rob Goldin r.goldin@imperial.ac.uk How important are biliary tract diseases? Hepatology 2011 53(5):1608-17 Approximately 16%
Biliary tract diseases of the liver Digestive Diseases Course Bucharest 2016 Rob Goldin r.goldin@imperial.ac.uk How important are biliary tract diseases? Hepatology 2011 53(5):1608-17 Approximately 16%
Autoimmune Liver Diseases
 2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
2nd Pannonia Congress of pathology Hepato-biliary pathology Autoimmune Liver Diseases Vera Ferlan Marolt Institute of pathology, Medical faculty, University of Ljubljana Slovenia Siofok, Hungary, May 2012
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk Fatty liver disease Is there fatty
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need?
 Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
Basic patterns of liver damage what information can a liver biopsy provide and what clinical information does the pathologist need? Rob Goldin r.goldin@imperial.ac.uk @robdgol FATTY LIVER DISEASE Brunt
PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES I HAVE NOTHING TO DISCLOSE CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017
 CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
CURRENT ISSUES IN ANATOMIC PATHOLOGY 2017 I HAVE NOTHING TO DISCLOSE Linda Ferrell PITFALLS IN THE DIAGNOSIS OF MEDICAL LIVER DISEASE WITH TWO CONCURRENT ETIOLOGIES Linda Ferrell, MD, UCSF THE PROBLEM
Liver National EQA Scheme. Circulation Q Birmingham, March 15 th 2005
 Liver National EQA Scheme Circulation Q Birmingham, March 15 th 2005 Images from circulations Virtualpathology@leeds.ac.uk/uvw View slides from current circulation, Aperio see and navigate whole slide
Liver National EQA Scheme Circulation Q Birmingham, March 15 th 2005 Images from circulations Virtualpathology@leeds.ac.uk/uvw View slides from current circulation, Aperio see and navigate whole slide
National Liver EQA Scheme. Open meeting, Glasgow March 24th 2004
 National Liver EQA Scheme Open meeting, Glasgow March 24th 2004 Participants meeting SOP8 Case discussion Are we quorate All please sign attendance sheet There were 20 EQA participants and 7 non-members
National Liver EQA Scheme Open meeting, Glasgow March 24th 2004 Participants meeting SOP8 Case discussion Are we quorate All please sign attendance sheet There were 20 EQA participants and 7 non-members
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
British Liver Transplant Group Pathology meeting September Leeds cases
 British Liver Transplant Group Pathology meeting September 2014 Leeds cases Leeds Case 1 Male 61 years Liver transplant for HCV cirrhosis with HCC in January 2014. Now raised ALT and bilirubin,? acute
British Liver Transplant Group Pathology meeting September 2014 Leeds cases Leeds Case 1 Male 61 years Liver transplant for HCV cirrhosis with HCC in January 2014. Now raised ALT and bilirubin,? acute
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
How to Approach a Medical Liver Biopsy. 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology. Sarajevo, 6 th -7 th November 2015
 1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
1 A Brief Introduction to the Liver Sessions 9 th Bryan Warren School of Pathology Pancreatic and Liver Pathology Sarajevo, 6 th -7 th November 2015 Stefan Hübscher, Institute of Immunology & Immunotherapy,
ACP-BSG meeting The liver in systemic inflammatory disorders. Dr Adrian C Bateman Southampton University Hospitals NHS Trust
 ACP-BSG meeting 10.12.09 The liver in systemic inflammatory disorders Dr Adrian C Bateman Southampton University Hospitals NHS Trust Wide range of diseases General inflammatory disorders Connective tissue
ACP-BSG meeting 10.12.09 The liver in systemic inflammatory disorders Dr Adrian C Bateman Southampton University Hospitals NHS Trust Wide range of diseases General inflammatory disorders Connective tissue
Histology. The pathology of the. bile ducts. pancreas. liver. The lecture in summary. Vt-2006
 Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Vt-2006 The pathology of the liver, bile ducts and pancreas Richard Palmqvist Docent, ST-läkare, Klin Pat Lab, Labcentrum The lecture in summary Introduction, histology & physiology in brief General phenomenon
Liver Pathology Symposium - medical livers
 Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy
 Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
LIVER SPECIALTY CONFERENCE USCAP Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA
 LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
Disorders of the Liver and Pancreas
 Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
Disorders of the Liver and Pancreas Liver Lobule Hexagonal plates Sinusoids Triads Bile duct branch Arteriole Venuole Blood flows from periphery to Central vein Space of Dissé Lobular Microanatomy Hepatocytes
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Autoimmune hepatitis
 Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
Autoimmune hepatitis: Autoimmune hepatitis a spectrum within a spectrum Alastair Burt Professor of Pathology and Dean of Clinical Medicine Newcastle University Spectrum of autoimmune liver disease Autoimmune
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
DILI PATHOLOGY. PHILIP KAYE November 2017 BSG Pathology Winter Meeting
 DILI PATHOLOGY PHILIP KAYE November 2017 BSG Pathology Winter Meeting General Mechanisms Role of Liver Biopsy Outline Kleiner Categories Pathology! Differentials Severity Finally Drugs/Toxins may cause
DILI PATHOLOGY PHILIP KAYE November 2017 BSG Pathology Winter Meeting General Mechanisms Role of Liver Biopsy Outline Kleiner Categories Pathology! Differentials Severity Finally Drugs/Toxins may cause
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Resident, PGY1 David Geffen School of Medicine at UCLA. Los Angeles Society of Pathology Resident and Fellow Symposium 2013
 Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features?
 22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
ABNORMAL LIVER FUNCTION TESTS. Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust
 ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
Steatosis/Steatohepatitis
 Prepared by Kurt Schaberg Introduction to Medical Liver Steatosis/Steatohepatitis Alcoholic Hepatitis Hepatocyte injury and inflammation resulting from chronic alcohol consumption AST/ALT ratio typically
Prepared by Kurt Schaberg Introduction to Medical Liver Steatosis/Steatohepatitis Alcoholic Hepatitis Hepatocyte injury and inflammation resulting from chronic alcohol consumption AST/ALT ratio typically
Current Concepts in the Management and Treatment of PBC & PSC
 Current Concepts in the Management and Treatment of PBC & PSC Michael A Heneghan, MD, MMedSc, FRCPI. Institute of Liver Studies, King s College Hospital, London A family affair? Central vein Hepatocytes
Current Concepts in the Management and Treatment of PBC & PSC Michael A Heneghan, MD, MMedSc, FRCPI. Institute of Liver Studies, King s College Hospital, London A family affair? Central vein Hepatocytes
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Chapter 18 LIVER BILIARY TRACT
 Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
Chapter 18 LIVER & BILIARY TRACT DUCT SYSTEM N O FIBROUS TISSUE PORTAL TRIAD CENTRAL VEIN PATTERNS OF HEPATIC INJURY Degeneration: Balooning, feathery degeneration, fat, pigment Inflammation:
CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease
 CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease Maria Isabel Fiel, M.D. The Mount Sinai Medical Center New York, New York Case A 57 yo man, 7 months
CASE 1 Plasma Cell Infiltrates: Significance in post liver transplantation and in chronic liver disease Maria Isabel Fiel, M.D. The Mount Sinai Medical Center New York, New York Case A 57 yo man, 7 months
Pediatric Primary Sclerosing Cholangitis and Potential Therapies
 Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial
Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial
Nottingham Patterns of liver fibrosis and their clinical significance
 Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
Nottingham 2006 Patterns of liver fibrosis and their clinical significance Alastair D Burt Professor of Pathology and Dean of Clinical Medicine University of Newcastle upon Tyne Collapse of reticulin
PBC and PSC: Back to Basics
 Disclosure No financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in this presentation. PBC and PSC: Back to Basics
Disclosure No financial interest or other relationship with the manufacturer(s) of the product(s) or provider(s) of the service(s) that will be discussed in this presentation. PBC and PSC: Back to Basics
I have no disclosures relevant to this presentation LIVER TESTS: WHAT IS INCLUDED? LIVER TESTS: HOW TO UTILIZE THEM OBJECTIVES
 LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract. Shannon Martinson, March 2017
 Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Pathology of the Liver and Biliary Tract 5 Diseases of the Biliary Tract Shannon Martinson, March 2017 http://people.upei.ca/smartinson/ OUTLINE Normal anatomy & function Hepatobiliary injury and responses
Special stains in liver pathology
 Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
Current Issues in Surgical Pathology 2014 Special stains in liver pathology Which, why, how Really? Sanjay Kakar, MD University of California, San Francisco Outline Which stains Why the stain is done How
Case n 1 ( B 92 / 4208 ) Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )
 Case n 2 ( B 00 / 8249 ) Case n 3 ( B 98 / 8352 )") Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
Slide Seminar Case n 1 ( B 92 / 4208 ) 16 month-old girl. HBV serology +. Clinic in favour of chronic hepatitis. 4 portal triads! classification limited Viral B chronic hepatitis Mild activity (Fig. 1
ACCME/Disclosures. The Overlap Syndromes: Do They Exist? Key Points and Questions 4/6/2016. Hans Popper Hepatopathology Society
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
CASE 01 LA Path Slide Seminar 13 March, 08. Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center
 CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
Interesting Cases from Liver Tumor Board. Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine
 Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
Interesting Cases from Liver Tumor Board Jeffrey C. Weinreb, M.D.,FACR Yale University School of Medicine jeffrey.weinreb@yale.edu Common Liver Diseases Hemangioma Cyst FNH Focal Fat/Sparing THID Non-Cirrhotic
ACG Clinical Guideline: Primary Sclerosing Cholangitis
 ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Update on Autoimmune Liver Disease. Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC
 Update on Autoimmune Liver Disease Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth
Update on Autoimmune Liver Disease Role of Liver Biopsy in Autoimmune Hepatitis, PBC and PSC Stefan Hübscher, School of Cancer Sciences, University of Birmingham Dept of Cellular Pathology, Queen Elizabeth
AASLD: Boston Rob Goldin
 AASLD: Boston 2014 Rob Goldin r.goldin@imperial.ac.uk Autoimmune hepatitis 31 Does genuine acute autoimmune hepatitis have a better prognosis? 32 Patients with Autoimmune Hepatitis and Advanced Disease
AASLD: Boston 2014 Rob Goldin r.goldin@imperial.ac.uk Autoimmune hepatitis 31 Does genuine acute autoimmune hepatitis have a better prognosis? 32 Patients with Autoimmune Hepatitis and Advanced Disease
Liver Transplant Pathology a general view
 Liver Transplant Pathology a general view Dr S E Davies Addenbrooke s Hospital Cambridge University Hospitals NHS Trust ACP/BSG Meeting Leeds 2012 Liver transplantation When and where? Who and why? How?
Liver Transplant Pathology a general view Dr S E Davies Addenbrooke s Hospital Cambridge University Hospitals NHS Trust ACP/BSG Meeting Leeds 2012 Liver transplantation When and where? Who and why? How?
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Cell injury, adaptation and death. Unite one Second Lab.
 Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Cell injury, adaptation and death Unite one Second Lab. The two lung abscesses seen here are examples of liquefactive necrosis in which there is a liquid center in an area of tissue injury. One abscess
Extrahepatic Biliary Obstruction. Ductal Diseases: Stones Tumors. Acute Injury: Viral Hepatitis Toxin (APAP/Etoh) Reye s Shock.
 Reye s Shock.") Extrahepatic Biliary Obstruction Stones Tumors Ductal Diseases: Ductal Diseases: Primary Biliary Primary Biliary Cirrhosis Cirrhosis Sclerosing Cholangitis Sclerosing Cholangitis Acute Injury: Viral Hepatitis
Extrahepatic Biliary Obstruction Stones Tumors Ductal Diseases: Ductal Diseases: Primary Biliary Primary Biliary Cirrhosis Cirrhosis Sclerosing Cholangitis Sclerosing Cholangitis Acute Injury: Viral Hepatitis
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
2014 CURRENT ISSUES IN PATHOLOGY
 2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
2014 CURRENT ISSUES IN PATHOLOGY SPECIAL STAINS IN LIVER BIOPSY PATHOLOGY Sanjay Kakar, MD University of California, San Francisco Trichrome stain : (1) Assess degree of fibrosis. H&E stain is not reliable
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Key Points: Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective. Jenny Heathcote, MD. University of Toronto
 Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
New insights into fatty liver disease. Rob Goldin Centre for Pathology, Imperial College
 New insights into fatty liver disease Rob Goldin Centre for Pathology, Imperial College r.goldin@imperial.ac.uk Prevalence of NASH Global prevalence of NAFLD is 25% with highest prevalence in the Middle
New insights into fatty liver disease Rob Goldin Centre for Pathology, Imperial College r.goldin@imperial.ac.uk Prevalence of NASH Global prevalence of NAFLD is 25% with highest prevalence in the Middle
Dhanpat Jain Yale University School of Medicine, New Haven, CT
 Dhanpat Jain Yale University School of Medicine, New Haven, CT Case history 15 years old female presented with fatigue. Found to have features suggestive of cirrhosis with esophageal varices, splenomegaly
Dhanpat Jain Yale University School of Medicine, New Haven, CT Case history 15 years old female presented with fatigue. Found to have features suggestive of cirrhosis with esophageal varices, splenomegaly
AAIM: GI Workshop Follow Up to Case Studies. Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease
 AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
Management of autoimmune hepatitis. Pierre-Emmanuel RAUTOU Inserm U970, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France
 Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France Case 1 52 year-old woman, referred for liver blood tests
Management of autoimmune hepatitis Pierre-Emmanuel RAUTOU Inserm U970, PARCC@HEGP, Paris Service d hépatologie, Hôpital Beaujon, Clichy, France Case 1 52 year-old woman, referred for liver blood tests
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN
 Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
Overview of PSC Jayant A. Talwalkar, MD, MPH Associate Professor of Medicine Mayo Clinic Rochester, MN 2012 Annual Conference PSC Partners Seeking a Cure May 5, 2012 Primary Sclerosing Cholangitis Multifocal
Drug Induced Liver Disease Role of the Pathologist. Disclosure. DILI can never be excluded. Romil Saxena, MD. Dr. Saxena has nothing to Disclose
 Drug Induced Liver Disease Role of the Pathologist Romil Saxena, MD Disclosure Dr. Saxena has nothing to Disclose DILI can never be excluded #1 DILI has no specific pattern of injury it can mimic any and
Drug Induced Liver Disease Role of the Pathologist Romil Saxena, MD Disclosure Dr. Saxena has nothing to Disclose DILI can never be excluded #1 DILI has no specific pattern of injury it can mimic any and
Pitfalls in the diagnosis of well-differentiated hepatocellular lesions
 2013 Colorado Society of Pathology Pitfalls in the diagnosis of well-differentiated hepatocellular lesions Sanjay Kakar, MD University of California, San Francisco Outline Hepatocellular adenoma: new WHO
2013 Colorado Society of Pathology Pitfalls in the diagnosis of well-differentiated hepatocellular lesions Sanjay Kakar, MD University of California, San Francisco Outline Hepatocellular adenoma: new WHO
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Autoimmune liver diseases Harrison s Principles of Internal Medicine 18-19 Ed. 2012 e seguenti Chronic hepatitis classification by cause
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center
 Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
Case #1. Digital Slides 11/6/ year old woman presented with abnormal liver function tests. Liver Biopsy to r/o autoimmune hepatitis
 45 year old woman presented with abnormal liver function tests Liver Biopsy to r/o autoimmune hepatitis Further down. ANA 1: 160; ASMA 1:80 ANA 1: 160; ASMA 1:80 IgG = 14.5 g/l (upper normal range: 16)
45 year old woman presented with abnormal liver function tests Liver Biopsy to r/o autoimmune hepatitis Further down. ANA 1: 160; ASMA 1:80 ANA 1: 160; ASMA 1:80 IgG = 14.5 g/l (upper normal range: 16)
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology
 Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology Nonalcoholic steatohepatitis and Fatty Liver Disease Liver manifestations of the obesity epidemic Changes
Linda Ferrell, MD Distinguished Professor Vice Chair Director of Surgical Pathology Dept of Pathology Nonalcoholic steatohepatitis and Fatty Liver Disease Liver manifestations of the obesity epidemic Changes
4/27/2018. Disclosures LIVER FUNCTION TESTS LIVER FUNCTION TESTS LIVER FUNCTION TESTS APPROACH TO THE PATIENT WITH ABNORMAL LIVER TESTS
 APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM
 EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Liver and Pancreatic Case discussion
 The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
The Royal Marsden Liver and Pancreatic Case discussion Dr Ian Chau Consultant Medical Oncologist The Royal Marsden 77 year old gentleman with 2 months history of vague abdominal ache and clinically finding
Investigating and Referring Incidental Findings of Abnormal Liver Tests
 Investigating and Referring Incidental Findings of Abnormal Liver Tests Note on Referral Guidelines: these revised guidelines are presented as a tool to aid appropriate referral and management of common
Investigating and Referring Incidental Findings of Abnormal Liver Tests Note on Referral Guidelines: these revised guidelines are presented as a tool to aid appropriate referral and management of common
Autoimmune Pancreatitis: A Great Imitator
 Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS
 in ADULTS") CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
Liver and gall bladder curriculum for ST1, presented at Northern block teaching, January 2017.
 Liver and gall bladder curriculum for ST1, presented at Northern block teaching, January 2017. 1 The 2015 RCPath Stage A curriculum for hepatobiliary pathology and gall bladder. 2 The stage A curriculum
Liver and gall bladder curriculum for ST1, presented at Northern block teaching, January 2017. 1 The 2015 RCPath Stage A curriculum for hepatobiliary pathology and gall bladder. 2 The stage A curriculum
AMR in Liver Transplantation: Incidence
 AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
Supplemental Tables. Parasitic Schistosomiasis increase < 1. Genetic Hemochromatosis increase < 1. autoimmune Autoimmune hepatitis (AIH) increase < 1
 increase < 1") Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
Supplemental Tables Supplemental Table 1 Various etiologies of liver cirrhosis and their association with liver stiffness and AST/ALT ratio Disease category Cause Example LS AST/ALT Inflammatory liver
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Tratamiento endoscópico de la CEP. En quien como y cuando?
 Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems
 SHORT COURSE Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems Linda Ferrell, M.D. Department of Anatomic Pathology, University of California San Francisco,
SHORT COURSE Liver Pathology: Cirrhosis, Hepatitis, and Primary Liver Tumors. Update and Diagnostic Problems Linda Ferrell, M.D. Department of Anatomic Pathology, University of California San Francisco,
LIVER DISEASES. Pathology Department, Zhejiang University School of Medicine,
 LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
LIVER DISEASES Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn Viral Hepatitis Cirrhosis of liver Liver cancer Viral Hepatitis DEFINITION Primary hepatic infections
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Autoimmune Hepatitis: Histopathology
 REVIEW Autoimmune Hepatitis: Histopathology Stephen A. Geller M.D.*, Autoimmune hepatitis (AIH), a chronic hepatic necroinflammatory disorder, occurs mostly in women. AIH is characterized by prominent
REVIEW Autoimmune Hepatitis: Histopathology Stephen A. Geller M.D.*, Autoimmune hepatitis (AIH), a chronic hepatic necroinflammatory disorder, occurs mostly in women. AIH is characterized by prominent
Liver Ultrasound - Beyond the Basics. Pamela Parker Lead Sonographer
 Liver Ultrasound - Beyond the Basics Pamela Parker Lead Sonographer Aims Review what we know about the liver Reasons for imaging Focal lesions Diffuse disease Can we do more? The Liver The Liver The Liver
Liver Ultrasound - Beyond the Basics Pamela Parker Lead Sonographer Aims Review what we know about the liver Reasons for imaging Focal lesions Diffuse disease Can we do more? The Liver The Liver The Liver
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver, Pancreas and Gall Bladder Pathology
 Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Liver, Pancreas and Gall Bladder Pathology SCBM342 Systemic Pathology Witchuda Payuhakrit, Ph.D. (Pathobiology) Email: witchuda.pay@mahidol.ac.th Objectives 1. Understand etiology and pathogenesis of common
Liver Specialty Evening Conference. Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle
 Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Financial Disclosure
 Benign Liver Masses Adil Abdalla, MBBS Creighton University-CHI Health August 25, 2018 Financial Disclosure Nothing to disclose Financial Disclosure 1 Objectives To assess patients with benign liver tumors
Benign Liver Masses Adil Abdalla, MBBS Creighton University-CHI Health August 25, 2018 Financial Disclosure Nothing to disclose Financial Disclosure 1 Objectives To assess patients with benign liver tumors
Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center
 Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center Acute Hepatitis Clinical Features Classically acute hepatitis is defined clinically as a significant (at least 2X elevation
Acute and Chronic Hepatitis John Hart, M.D. University of Chicago Medical Center Acute Hepatitis Clinical Features Classically acute hepatitis is defined clinically as a significant (at least 2X elevation
Role of Liver Biopsy. Role of Liver Biopsy 9/3/2009. Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging
 Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology
Liver Biopsies in Viral Hepatitis: Beyond Grading and Staging for further reference: Liver biopsy assessment in chronic viral hepatitis: a personal, practical approach Neil Theise, MD. Depts of Pathology