Faculty/Presenter Disclosure
|
|
|
- Isabel Foster
- 5 years ago
- Views:
Transcription


 Speakers Bureau/Honoraria: None Consulting Fees: None Other: BC Centre on")
1 Provincial Guidelines for the Clinical Management of Opioid Use Disorder Leslie Lappalainen MD Family and Addiction Medicine Medical Lead for Addiction Medicine, Interior Health, Mental Health and Substance Use Clinical Instructor, UBC Provincial update: Officially Released Feb 7, 2017 Faculty/Presenter Disclosure Faculty: Leslie Lappalainen Relationships with commercial interests: Grants/Research Support: NIDA (previous) Speakers Bureau/Honoraria: None Consulting Fees: None Other: BC Centre on Substance Use (MoH), Interior Health 1
2 Disclosure of Commercial Support I have NOT received financial support or in kind support from any commercial interest. St Paul s Addiction Medicine Fellowship is funded in part by Goldcorp Corporation Potential for conflict(s) of interest: None Mitigating Potential Bias No sources of bias 2
3 Learning Objectives Opioid overdose emergency in the province and within the Interior Review new BC Centre on Substance Use and how this new centre plans to support IH Addition primer Review the role of detox as a standalone intervention for opioid use disorder Review the evidence for psychosocial treatments for opioid use disorder Learning Objectives Review evidence for pharmacotherapy options for opioid use disorder and potential advantages and disadvantages of each treatment option Review of specialist led treatments Review of harm reduction approaches (take home naloxone, supervised consumption sites) 3

4 Opioid Overdose Emergency 4


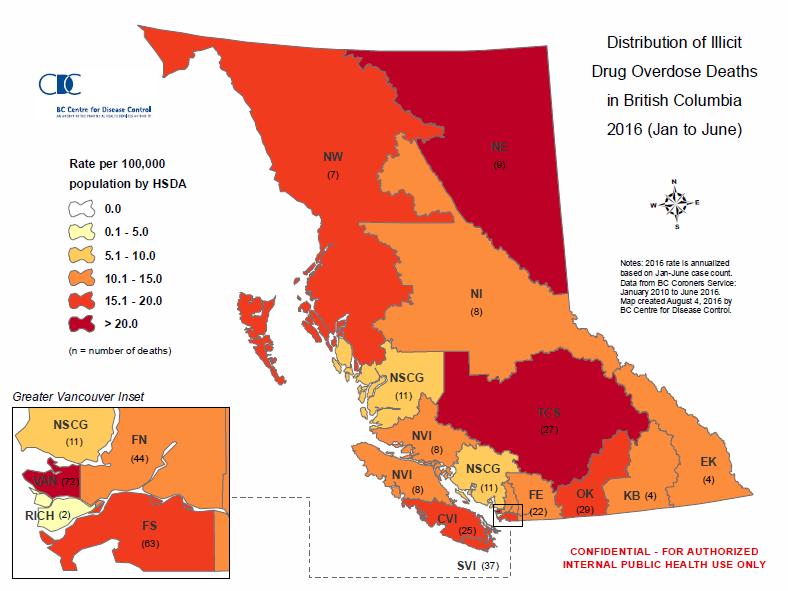
5 Number of deaths and mortality rate attributed to illicit drug use in B.C., Source: Illicit Drug Overdose Deaths in BC, January 1, 2007 to January 30, Office of the Chief Coroner of BC. Released Feb 17,
6 Source: Illicit Drug Overdose Deaths in BC, January 1, 2007 to November 30, Office of the Chief Coroner of BC.. Source: Illicit Drug Overdose Deaths in BC, January 1, 2007 to November 30, Office of the Chief Coroner of BC. 6

7

8


9 9
10 Public Health Emergency Comparisons SARS (2003) 44 deaths; 400 ill; quarantined (Canada) H1N1 (2009) 429 deaths, ill (Canada) 56 deaths, 1059 ill (BC) EBOLA (2014) 0 deaths, 0 ill, 1000 at risk (Canada) 0 deaths, 0 ill, 100 at risk (BC) Opioid Overdose (2016) 916 deaths, ill (BC) 154 deaths, 5000 ill (Interior Health) How do we stop this overdose trend? Requires a cultural shift to the way we treat opioid use and opioid addiction Application of evidence based practice Addressing gaps between evidence and practice More physicians trained to do addictions work within primary care settings 10


11 11

12 Core Functions Addiction Primer Addiction defined Review of reward pathways involved Opioid addiction why new guidelines? 12
13 What is addiction? Addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social and spiritual manifestations. Source: American Society of Addiction Medicine (ASAM) What is addiction? Addiction is characterized by: Inability to abstain Impairment in behavioral control Craving Diminished recognition of significant problems Dysfunctional emotional response Cycles of relapse and remission Without treatment or engagement in recovery process can result in disability and premature death Source: American Society of Addiction Medicine (ASAM) 13


14 Piore et al. Resetting the Addictive Brain May Discover Magazine. 14


15 15


16 16


17 Science Inpatient/Outpatient Detox Withdrawal/Taper Psychosocial Treatment OAT Methadone Buprenorphine/Naloxone Mandatory Counselling? Tapers vs. Maintenance 17

18 Background The province has a guideline for the treatment of opioid use disorder with methadone Updated July 2016 to include buprenorphine Evidence-based guidance for when to use methadone versus other treatments lacking Background Released in
19 Release date: Feb 7,
20 Disclosures No member of guideline committee reported direct financial or indirect conflicts of interest Overview of treatment options a WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. >> AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. HARM REDUCTION Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment Access to sterile syringes, needles, and other supplies Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits 20
21 Withdrawal management only Detox: Inpatient vs. Outpatient Intensive Psychosocial Treatment? Residential Treatment OAT Tapers, Clonidine? Outcomes? a r WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. >> AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment HARM Access to sterile syringes, needles, and other supplies REDUCTION Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits 21

22 22
23 Safety considerations - Withdrawal management alone Detox can potentially be an important first point of contact and a bridge to other treatment options However, detox as a stand alone intervention associated with: High rates of relapse (Strang et al., 2003) 90% relapse most within 7 days HIV-transmission (MacArthur et al., 2012) Morbidity and Mortality (Luty 2003, Simpson and Friend, 1988) THN Training Residential Treatment (without maintenance OAT) No systematic reviews or meta-analyses Signal to some clinical improvement, but much of the literature is outdated (Craddock 1997, Gossop 1999, Hubbard 1989, Simpson 1982) Relapse (Smyth et al., 2010) Without OAT 91% relapse, 59% within one week of D/C No OAT 2 times risk of death (Matthias Pierce 2016) 23
24 Withdrawal Options Buprenorphine/n aloxone taper Methadone taper Short-acting opioids Clonidine and ancillary meds Encourage: Long, slow taper Intensive psychosocial followup outpatient taper Ensure: take-home naloxone training Warn: risk of OD and death with inpatient taper Opioid Agonist (Maintenance) Therapy Methadone vs. buprenorphine First line? Safety profile of medications Mandatory counselling Take home dosing vs. methadone? How long; when and how to taper Other evidence-based options 24

25 a WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. >> AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. HARM REDUCTION Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment Access to sterile syringes, needles, and other supplies Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits What does work for opioid addiction: Opioid Agonist Therapy Methadone Buprenorphine/naloxone (4:1 ratio) (Suboxone ) Treatment duration: usually at least 12 months and then a slow taper 25
26 Threshold for Respiratory Depression 26
")
27 Partial Agonist (i.e. buprenorphine/naloxon e Suboxone) Partial activation 27
 Partial Agonist (i.e. buprenorphine) This relative difference between full activation of the receptor and partial activation of the receptor is called PRECIPITATED")
28 Full Agonist (i.e. heroin, methadone, morphine) Partial Agonist (i.e. buprenorphine) This relative difference between full activation of the receptor and partial activation of the receptor is called PRECIPITATED WITHDRAWAL Less Full activation Agonist Treatment Methadone MMT vs. no opioid replacement therapy (Mattick et al., Cochrane Review 2009) Methadone significantly more effective than nonpharmacological approaches in: o Treatment retention o Suppression of heroin use 28
29 Agonist treatment Buprenorphine/naloxone Buprenorphine vs. Methadone Maintenance Therapy (Mattick et al., Cochrane Review 2014) At medium/high doses bup/nlx ( mg) is not markedly different from methadone in terms of treatment retention No difference between bup/nlx and MMT in reducing illicit opioid use Agonist treatment Buprenorphine/naloxone Buprenorphine vs. Methadone Maintenance Therapy (Mattick et al., Cochrane Review 2014) At medium/high doses bup/nlx is not markedly different from methadone in terms of treatment retention Safety profile? No difference between bup/nlx and MMT in reducing illicit opioid use 29


30 98 unintentional OD b/w June Oct /98 cases tested positive for the bup metabolite Both tested + for 6-MAM, morphine (heroin OD) 30

31 31
32 mid 1990s MMT provided to only 20 30% of persons with OUD due to regulations and concerns re: safety 1995 all medical doctors allowed to prescribe buprenorphine without any special licensing Barriers minimized: physician compensation mechanisms in place, pharmacy services and insurance coverage Led to 65,000 patients per year getting on treatment (10 x more than with methadone) About 20% of all physicians in France use bup to treat OUD Reduction in overdose mortality with expanded access to buprenorphine (France) 2006 by the Infectious Diseases Society of America Carrieri et al.,
33 Advantages Potent opioid agonist Potentially better treatment retention, particularly for unstable opioiddependent individuals Disadvantages Higher risk of overdose, particularly during treatment initiation Generally requires daily witnessed ingestion (DWI) Methadone May be easier to initiate treatment Potentially better alternative if buprenorphine was unsuccessful at relieving withdrawal symptoms or associated with severe side effects Approved in Canada for primary purpose of pain control (split dose BID or TID dosing); Health Canada exemption required for prescribing More severe side effect profile More expensive if DWI required Longer time to achieve therapeutic dose (>35 days) Higher potential for adverse drug-drug interactions (e.g. Abx, ARVs) Increased risk of cardiac arrhythmias as a result of QTc prolongation Buprenorphine/Naloxone Advantages Risk of OD as partial agonist and ceiling effect for resp. depression Reduced risk of injection, diversion, and OD due to naloxone component Allows for safer take home schedules Milder side effect profile Easier to rotate from bup/nlx to methadone Flexible take home schedules many contribute to cost savings and patient autonomy Shorter time to achieve therapeutic dose (1-3 days) Disadvantages Potential risk of drop-out May cause precipitated withdrawal if induced inappropriately May block opioid analgesics used for concurrent pain treatment Not approved in Canada for the purposes of pain control 33

34 Opioid Use Disorder Bup/Nx 1 st line Primary Care = methadone 34




35 35





36 36


37 2011 review 35 studies, 4319 participants Psychosocial interventions + OAT vs. standard OAT No significant benefits retention or treatment outcomes Tapers? 37
38 Alternative Treatment Options a r WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. >> AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment HARM Access to sterile syringes, needles, and other supplies REDUCTION Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits 38
39 Emerging therapeutic options for severe OUD Slow release oral morphine (once daily witnessed ingestion) if failed 1 st line options off label use Prescribers must have methadone exemption and should consult with specialist experienced in prescribing SROM Injectable diacetylmorphine (heroin) and hydromorphone options in a supervised setting for treatment refractory opioid use disorder Included in Vancouver Coastal Health guidelines of OUD (but not in Provincial Guidelines), recommended injectable program expansion in Coroners Inquest (B. Jansen). Opioid Antagonist Naltrexone Full opioid blocker Reduced tolerance Low treatment retention rates Not superior to other forms of treatment Oral (Revia) vs. extended release (Vivitrol) (Naltrexone) 39
 40")
40 New Treatments (Not yet available in Canada) 40
41 Harm Reduction Approaches a r WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. > AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment HARM Access to sterile syringes, needles, and other supplies REDUCTION Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits 41


42 trained sites 42

43 Take Home Naloxone in BC Go to Find a harm reduction site in your area 43

44 Summary 44
45 Withdrawal Options Buprenorphine/n aloxone taper Methadone taper Short-acting opioids Clonidine and ancillary meds Encourage: Long, slow taper Intensive psychosocial followup outpatient taper Ensure: take-home naloxone training Warn: risk of OD and death with inpatient taper Treatment 1 st line: Buprenorphine/nalox one Relatively safer Take home doses Easier to transition from partial to full agonist Primary care settings Rural and remote settings Withdrawal Options Buprenorphine/nalox one taper Methadone taper Short-acting opioids Clonidine and ancillary meds 45
46 Treatment 1 st line: Buprenorphine/nalox one If contraindications: Methadone Withdrawal Options Buprenorphine/nalox one taper Methadone taper Short-acting opioids Clonidine and ancillary meds Treatment 1 st line: Buprenorphine/nalox one If contraindications: Methadone 2 nd line: Transition bup/nlx to methadone methadone to bup/nlx Withdrawal Options Buprenorphine/nalox one taper Methadone taper Short-acting opioids Clonidine and ancillary meds 46

47 a WITHDRAWAL MANAGEMENT 1 3 Tapered methadone, buprenorphine, or alpha 2 adrenergic agonists +/ psychosocial treatment 4 +/ residential treatment +/ oral naltrexone 5 LOW If opioid use continues, consider treatment intensifiction. >> AGONIST THERAPIES Buprenorphine/ naloxone 6 (preferred) Methadone 7,8 +/ psychosocial treatment +/ residential treatment TREATMENT INTENSITY SPECIALIST LED ALTERNATIVE APPROACHES* Slow release oral morphine 9,10 +/ psychosocial treatment +/ residential treatment HIGH Where possible, << simplify treatment. HARM REDUCTION Across the treatment intensity spectrum, evidence based harm reduction should be offeed to al l, includi ng: Education re: safer use of sterile syringes/needles and other applicable substance use equipment Access to sterile syringes, needles, and other supplies Access to Supervised Injection Sites (SIS) Take Home Naloxone (THN) kits 47
48 Intensive specialized Addiction care IM Psychiatry Primary Care Addiction Care Hospital Detox Health Care System Integrated with BCCSU Practical Tips: Continuing patients on Bup/Nx Collateral from initiating doctor Pharmanet! Improved retention: mg/d Know how medication is taken (SL) Course: suboxonecme.ca IH will cover 3.5 hours at sessional rate for doing this! Lower barriers: how long and who to DWI? Benzos, AUD, youth, working, school, psych, homeless Random pill counts Random UDS RACE line support 48
49 Practical tips billing T00039 fee code for methadone or buprenorphine/naloxone $22.98/week (payable once per patient per week, regardless of visits per week) P15039 fee code for point of care urine testing for individuals on methadone or bup/nal $12.42/per test (up to 26 per year) Revisions to fee codes are underway Coverage for bup/nlx recent update Income Assistance and PWD fully covered As of Feb 1, 2017 buprenorphine/naloxone is covered through Plan G (coverage for psychiatric medication) Available if family adjusted net income below $42,000 (plus $3000 per dependent) 49

 RACE Line: 604-696- 2131")
50 Additional Guideline Supports New guidelines Online on BCCSU website Point of care summary tools Patient information sheets Addiction teams and services (e.g. detox for challenging buprenorphine induction) RACE Line:
51 3 streams: Clinical, Nursing, and Social Work Timeline for Clinical Fellowship: August 28, 2017 Application process opens October 2, 2017 Application deadline Nov 6, 2016 Interview period to Dec 4, 2017 December 11, 2017 Acceptance notification December 18, 2017 Deadline for acceptance July 3, 2018 Fellowship begins Questions? Please Carmen Rock at 3 streams: Clinical, Nursing, and Social Work Timeline for Nursing Fellowship: September 30, 2016 Application process opens October 31, 2016 Application deadline Nov 15, 2016 to Interview period Jan 16, 2017 January 30, 2017 Acceptance notification February 10, 2017 Deadline for acceptance July 3, 2017 Fellowship begins Questions? Please Carmen Rock at 51
52 3 streams: Clinical, Nursing, and Social Work Timeline for Social Work Fellowship: December 5, 2016 Application process opens January 16, 2017 Application deadline Feb 6 to Mar 3, 2017 Interview period March 13, 2017 Acceptance notification March 20, 2017 Deadline for acceptance July 3, 2017 Fellowship begins Questions? Please Carmen Rock at crock@cfenet.ubc.ca Timeline for Research Fellowship: October 31, 2016 Application process opens December 5, 2016 Application deadline December 12, 2016 Interview period January 23, 2017 Acceptance notification January 30, 2017 Deadline for acceptance July 3, 2017 Fellowship begins Questions? Please Carmen Rock at crock@cfenet.ubc.ca 52







53 Training Opportunities UBC Enhanced Skills 3-6 months Questions? Please Carmen Rock at Treatment Guideline Committee 53


54 Acknowledgements Dr. Rolando Barrios Ms. Laura Case Ms. Anne McNabb Mr. Andrew McFarlane The BC Centre for Excellence in HIV AIDS Ms. Pauline Voon Ms. Deborah Graham Ms. Emily Wagner Mr. James Nakagawa Ms. Lianlian Ti Ms. Cheyenne Johnson Ms. Jessica Jun Ms. Maryam Babaei Ms. Josey Ross Mr. Peter Vann 54
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
PROVINCIAL OPIOID ADDICTION TREATMENT SUPPORT PROGRAM PRECEPTORSHIP WORKBOOK FOR HOSPITAL SETTINGS
 PROVINCIAL OPIOID ADDICTION TREATMENT SUPPORT PROGRAM PRECEPTORSHIP WORKBOOK FOR HOSPITAL SETTINGS 11 About the British Columbia Centre on Substance Use The BC Centre on Substance Use (BCCSU) is a new
PROVINCIAL OPIOID ADDICTION TREATMENT SUPPORT PROGRAM PRECEPTORSHIP WORKBOOK FOR HOSPITAL SETTINGS 11 About the British Columbia Centre on Substance Use The BC Centre on Substance Use (BCCSU) is a new
National Opioid Treatment Guideline Dr. Ronald Lim
 National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
The Opioid Overdose Crisis: Role of the TB Physician
 The Opioid Overdose Crisis: Role of the TB Physician February 22, 2019 Dr. Patricia Daly Chief Medical Health Officer Vancouver Coastal Health Source: Health Canada BC Overdose Deaths 1992 2018 BC Overdose
The Opioid Overdose Crisis: Role of the TB Physician February 22, 2019 Dr. Patricia Daly Chief Medical Health Officer Vancouver Coastal Health Source: Health Canada BC Overdose Deaths 1992 2018 BC Overdose
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine. March 10, 2016
 The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Provincial Health Services Authority. Correctional Health Services - Update. Dr. Nader Sharifi Andrew MacFarlane. April 11/2018
 Provincial Health Services Authority Correctional Health Services - Update Dr. Nader Sharifi Andrew MacFarlane April 11/2018 Similar to FNHA, PHSA covers the entire province of BC Correctional Health Services
Provincial Health Services Authority Correctional Health Services - Update Dr. Nader Sharifi Andrew MacFarlane April 11/2018 Similar to FNHA, PHSA covers the entire province of BC Correctional Health Services
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
a Guideline for the Clinical Management of Opioid Addiction
 a Guideline for the Clinical Management of Opioid Addiction Published 2015 This page left intentionally blank for double-sided printing. Vancouver Coastal Health & Providence Health Care Opioid Use Disorder
a Guideline for the Clinical Management of Opioid Addiction Published 2015 This page left intentionally blank for double-sided printing. Vancouver Coastal Health & Providence Health Care Opioid Use Disorder
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement
 Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
4/5/2018 MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS OBJECTIVES DEFINITION OF ADDICTION APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H.
 MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H. MEDICAL DIRECTOR, UNITYPOINT HEALTH MERITER/ NEWSTART ADJUNCT PROFESSOR, UNIVERSITY OF WISCONSIN MADISON
MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H. MEDICAL DIRECTOR, UNITYPOINT HEALTH MERITER/ NEWSTART ADJUNCT PROFESSOR, UNIVERSITY OF WISCONSIN MADISON
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE. Dr. David Williams Chief Medical Officer of Health
 ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE Dr. David Williams Chief Medical Officer of Health National opioid-related mortality data, 2016 (Health Canada) Provincial Overdose Coordinator
ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE Dr. David Williams Chief Medical Officer of Health National opioid-related mortality data, 2016 (Health Canada) Provincial Overdose Coordinator
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Public Health Association of British Columbia
 October 30 th, 2017 Open Letter to the Government of British Columbia: BC Needs an OPIOID ACTION PLAN Since April, 2016 when the epidemic of opioid overdose deaths was declared a Public Health Emergency
October 30 th, 2017 Open Letter to the Government of British Columbia: BC Needs an OPIOID ACTION PLAN Since April, 2016 when the epidemic of opioid overdose deaths was declared a Public Health Emergency
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
How Can Injectable Hydromorphone and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder?
 How Can Injectable Hydromorphone 0 and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder? Dr. Eugenia Oviedo-Joekes University of British Columbia Dr. Martin Schechter University of British
How Can Injectable Hydromorphone 0 and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder? Dr. Eugenia Oviedo-Joekes University of British Columbia Dr. Martin Schechter University of British
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Beyond Birth: A Comprehensive Recovery Center serving parenting women
 Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
Confronting the Opioid Epidemic: Suboxone in Primary Care
 Confronting the Opioid Epidemic: Suboxone in Primary Care Kami Harless, MD 1 The Opioid Epidemic 2 The Opioid Epidemic 3 Washington Epidemic 4 King County Epidemic 5 King County Epidemic 6 Outline Opioid
Confronting the Opioid Epidemic: Suboxone in Primary Care Kami Harless, MD 1 The Opioid Epidemic 2 The Opioid Epidemic 3 Washington Epidemic 4 King County Epidemic 5 King County Epidemic 6 Outline Opioid
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs
 It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE
 METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Treating Opioid Use Disorder with Buprenorphine/naloxone
 Treating Opioid Use Disorder with Buprenorphine/naloxone Faculty/Presenter Disclosure Faculty: Jessica Kirkwood Relationships with financial sponsors: Grants/Research Support: N/A Speakers Bureau/Honoraria:
Treating Opioid Use Disorder with Buprenorphine/naloxone Faculty/Presenter Disclosure Faculty: Jessica Kirkwood Relationships with financial sponsors: Grants/Research Support: N/A Speakers Bureau/Honoraria:
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
Disclosures. Objectives 2/5/2018. Women and opioid use disorder: Optimizing care during pregnancy and beyond
 Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
AGENDA U.S. SURGEON GENERAL, VIVEK MURTHY MD 2/5/2019
 FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
U.S. SURGEON GENERAL, VIVEK MURTHY MD
 FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction
 Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Harm Reduction in the Hospital: Preventing AMA Discharges and ED Bounce Backs
 Harm Reduction in the Hospital: Preventing AMA Discharges and ED Bounce Backs Kathryn Dong MD, MSc, FRCP, DABAM Director, Inner City Health and Wellness Program, Royal Alexandra Hospital Associate Clinical
Harm Reduction in the Hospital: Preventing AMA Discharges and ED Bounce Backs Kathryn Dong MD, MSc, FRCP, DABAM Director, Inner City Health and Wellness Program, Royal Alexandra Hospital Associate Clinical
POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Opioid Use Disorder Treatment Initiation in Diverse Settings
 Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Buprenorphine Order Set and Rapid Access Referral. Copyright 2017, CAMH
 2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
2 Buprenorphine Order Set and Rapid Access Referral 1 Agenda Problem Identification / Identification Importance / Importance Baseline Workflow Baseline Workflow Baseline Data Baseline Data Objectives Solution
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management Options for Opioid Dependence:
 Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Buprenorphine-naloxone for the treatment of opioid use disorder in primary care. June 11, 2018 Dr. Nikki Bozinoff
 Buprenorphine-naloxone for the treatment of opioid use disorder in primary care June 11, 2018 Dr. Nikki Bozinoff Disclosures I have no conflicts of interest to declare I am a family physician I completed
Buprenorphine-naloxone for the treatment of opioid use disorder in primary care June 11, 2018 Dr. Nikki Bozinoff Disclosures I have no conflicts of interest to declare I am a family physician I completed
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Acute General Medical and Surgical Admission:
 Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Medical Assisted Treatment of Opioid
 Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Medication-Assisted Treatment (MAT) for Opioid Use Disorders
 for Opioid Use Disorders") Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Vivitrol Drug Court and Medication Assisted Treatment
 Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Fentanyl, Opioid Overdose and Naloxone
 Fentanyl, Opioid Overdose and Naloxone Opioid Agonist Therapy Conference Saskatoon, SK April, 2016 Declaration No conflict of interest. Consultant in Addiction Medicine, SHR. Chair, College of Physicians
Fentanyl, Opioid Overdose and Naloxone Opioid Agonist Therapy Conference Saskatoon, SK April, 2016 Declaration No conflict of interest. Consultant in Addiction Medicine, SHR. Chair, College of Physicians
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Public Policy Statement on the Regulation of Office-Based Opioid Treatment
 Public Policy Statement on the Regulation of Office-Based Opioid Treatment Background Office-based opioid treatment (OBOT) commonly refers to outpatient treatment services provided outside of licensed
Public Policy Statement on the Regulation of Office-Based Opioid Treatment Background Office-based opioid treatment (OBOT) commonly refers to outpatient treatment services provided outside of licensed
Changing Course: statewide efforts to combat the opioid epidemic in California
 Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Treating Opioid Use Disorders: An Update for Counselors and Other Providers
 Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
OUD & MAR: Caring for Our Communities
 OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Access in California
 Buprenorphine Access in California James J. Gasper, PharmD, BCPP Pharmacy Benefits Division Department of Health Care Services james.gasper@dhcs.ca.gov Source: CDPH Vital Statisitics Death Statistical
Buprenorphine Access in California James J. Gasper, PharmD, BCPP Pharmacy Benefits Division Department of Health Care Services james.gasper@dhcs.ca.gov Source: CDPH Vital Statisitics Death Statistical
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film
 Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
Kelty Mental Health Resource Centre, Pinwheel Education Series: Youth and the Opioid Crisis
 Kelty Mental Health Resource Centre, Pinwheel Education Series: Youth and the Opioid Crisis March 21st, 2017, Jane Buxton Harm Reduction Lead BCCDC Overview Overdose deaths and fentanyl Declaration of
Kelty Mental Health Resource Centre, Pinwheel Education Series: Youth and the Opioid Crisis March 21st, 2017, Jane Buxton Harm Reduction Lead BCCDC Overview Overdose deaths and fentanyl Declaration of
Treating Opioid Addiction
 Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Safe Practices and Action Items
 Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
THE NALTREXONE CHALLENGE
 THE NALTREXONE CHALLENGE DISCLOSURE Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit Has no conflicts of interest Maureen Allen Has no conflicts of interest DONNA 68 years old Currently treated with
THE NALTREXONE CHALLENGE DISCLOSURE Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit Has no conflicts of interest Maureen Allen Has no conflicts of interest DONNA 68 years old Currently treated with
Treating Emergency Room Opioid Withdrawal with Buprenorphine
 Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Clinical Policy: Naltrexone (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.96 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: 03.01.12 Last Review Date: 02.19 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Clinical Policy: (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: 03.01.12 Last Review Date: 02.19 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Triage, Assessment and Treatment Planning
 Triage, Assessment and Treatment Planning Prepared by Todd Sakakibara MD, CCFP, FCFP Clinical Assistant Professor, Dept. Family Practice UBC Diplomate of the American Board of Addiction Medicine Triage
Triage, Assessment and Treatment Planning Prepared by Todd Sakakibara MD, CCFP, FCFP Clinical Assistant Professor, Dept. Family Practice UBC Diplomate of the American Board of Addiction Medicine Triage
Opioid use disorder is one of the most challenging forms
 VULNERABLE POPULATIONS CPD Management of opioid use disorders: a national clinical practice guideline Julie Bruneau MD MSc, Keith Ahamad MD, Marie-Ève Goyer MD MSc, Ginette Poulin MD, Peter Selby MBBS
VULNERABLE POPULATIONS CPD Management of opioid use disorders: a national clinical practice guideline Julie Bruneau MD MSc, Keith Ahamad MD, Marie-Ève Goyer MD MSc, Ginette Poulin MD, Peter Selby MBBS
ADDICTIONS NURSING IN Holland and Europe. Education now and in the future
 ADDICTIONS NURSING IN Holland and Europe Education now and in the future Disclosure IntNSA Holland: August 2018 2 ASAM American Society of Addiction Medicine: Definition of Addiction Addiction is a primary,
ADDICTIONS NURSING IN Holland and Europe Education now and in the future Disclosure IntNSA Holland: August 2018 2 ASAM American Society of Addiction Medicine: Definition of Addiction Addiction is a primary,
Clinical Policy: Naltrexone (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.96 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: 03.01.12 Last Review Date: 02.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Clinical Policy: (Vivitrol) Reference Number: CP.PHAR.96 Effective Date: 03.01.12 Last Review Date: 02.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Responding to BC s Opioid Overdose Epidemic
 Responding to BC s Opioid Overdose Epidemic Progress Update September 2017 BACKGROUND Since BC s Public Health Emergency was declared in 2016, people across the province have mobilized to immediately respond
Responding to BC s Opioid Overdose Epidemic Progress Update September 2017 BACKGROUND Since BC s Public Health Emergency was declared in 2016, people across the province have mobilized to immediately respond