Serrated Colorectal Polyps and the Serrated Neoplasia Pathway
|
|
|
- Violet Welch
- 5 years ago
- Views:
Transcription

1 Serrated Colorectal Polyps and the Serrated Neoplasia Pathway An update on the pathology and clinical significance Mark Be(ngton Envoi Specialist Pathologists
2 Overview 1. A framework of what is included in the serrated neoplasia pathway and how this fits into colorectal carcinoma as a whole 2. Briefly separadng the serrated neoplasia pathway from Lynch syndrome, separadng serrated morphology from the serrated neoplasia pathway and discussing serrated polyposis syndrome 3. A more detailed discussion of the polyp precursors of the serrated neoplasia pathway with a focus on: a) their pathological features b) their molecular biology c) the subtypes of colorectal carcinoma that they give rise to
3 Part I The Serrated Neoplasia Pathway in the Context of Colorectal Carcinoma
4 Proposed Major Molecular Subtypes of Colorectal Carcinoma Sinicrope et al, Gastroenterology 2015;148:88-99 Phipps et al, Gastroenterology 2015;148:77-87
5 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
6 TradiDonal Pathway of Tumour Progression Normal Colonic Epithelium DysplasDc ACF Early Adenoma Late Adenoma Carcinoma Metastasis 5qLOH and/ or APC mutadon KRAS mutadon 18qLOH 17pLOH (p53) Further Changes Adapted from Kinzler and Vogelstein, Cell, 1996
7 Serrated Pathway of Tumour Progression Normal Colonic Epithelium Non-dysplastic serrated polyp Dysplastic serrated polyp Carcinoma Metastasis BRAF mutadon CIMP MLH1 methyladon TP53 mutadon P16 methyladon Other events
8 The Serrated Neoplasia Pathway The major molecular alteradons underpinning the serrated neoplasia pathway are: 1. MAP kinase pathway acdvadon 2. The CpG island methylator phenotye



9 MAPK pathway acdvadon
10 The CpG island methylator phenotype (CIMP) This refers to the propensity to methylate CpG islands Cytosine followed by Guanine (CpG) is quite uncommon in the genome (far less than expected by chance alone) In general CpGs aggregate in the promoter regions of some genes These sites are typically hypomethylated In cancers with CIMP these sites become increasingly methylated undl transcripdon factors can no longer bind to the promoter This change is effecdvely irreversible and results in gene silencing When a tumour suppressor gene (such as MLH1) is methylated, it is oncogenic


11 CpG Island MethylaDon CpG rich promoter region TranscripDon start site
12 MAP kinase pathways acdvadon in serrated polyps Nearly all serrated polyps have an acdvadng mutadon of either BRAF or KRAS Both result in MAP kinase pathway acdvadon SSA TSA Combined 100% 100% 100% 80% 80% 80% 60% 60% 60% 40% 40% 40% 20% 20% 20% 0% BRAF KRAS WT 0% BRAF KRAS WT 0% BRAF KRAS WT
13 CpG island methylator phenotype high in serrated polyps 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% SSA TSA Combined
14 So what makes a serrated molecular signature? MAP kinase pathway acdvadon? MAP kinase and CIMP? BRAF mutadon? BRAF and CIMP? CIMP? BRAF, CIMP and MSI?
15 What do I think should be included in the serrated neoplasia pathway? Origin in an SSA or TSA is the best definidon to me Any cancer with a BRAF mutadon A small subset of cancers with a KRAS mutadon - if they have TSA at the edge - if they are CIMP- H A Dny fracdon of BRAF/KRAS wild- type cancers probably are of the serrated neoplasia pathway (having arisen from null type SSAs or TSAs) I do not consider mismatch repair status (and therefore microsatellite instability) to be relevant
16 Treatment ImplicaDons of the Serrated Neoplasia Pathway Surgical resecdon is the primary treatment Chemotherapy for stage III / IV (and possibly some stage II) Although the studies are conflicted, standard chemotherapy (e.g. folfox) does not appear to be as effecdve for MSI cancers as for MSS cancers 1 Targeted therapies Monoclonal andbodies to the EGFR (cetuximab, panitumumab) can be used A BRAF mutadon is not a contraindicadon Small molecule BRAF inhibitors do not appear to be effecdve as monotherapy 2 Small molecule MEK inhibitors alone or in combinadon with other targeted therapies are being trialed Immunotherapy CTLA- 4 antagonists and PD- 1 antagonsits have been udlised with great success in melanoma A brisk immune response to the tumour appears to be cridcal to success of these agents A recent small study has shown efficacy of pembrolizumab in MSI colorectal carcinoma 3 1. Sargent et al; JCO Prahallad et al; Nature Le et al; NEJM 2015
17 Summary Part I Cancers of the serrated neoplasia pathway have their origins in SSAs or TSAs A BRAF mutadon is the best molecular evidence of a serrated pathway carcinoma If a cancer is KRAS mutated or null- type it must have either an unequivocal serrated polyp at the edge, or be CIMP- H to consider it a serrated pathway carcinoma Overall about 20-25% of colorectal carcinoma fits this definidon Amounts to approximately 3000 cancer deaths per year in Australia Most (the MSI subset) are associated with a good prognosis Approximately 30% have a very poor prognosis Targeted therapies may be pardcularly relevant to the serrated neoplasia pathway, especially the MSI group
18 Part II SeparaDng the Serrated Neoplasia Pathway from Lynch Syndrome Serrated Morphology versus the Serrated Neoplasia Pathway And Serrated Polyposis Syndrome
19 DifferenDaDng serrated neoplasia pathway from Lynch syndrome
20 The role of the pathologist in separadng the serrated neoplasia pathway from Lynch syndrome 1. Polyp type - > SSA or TSA then it is not Lynch 2. Mismatch repair enzyme tesdng - we use reflex tesdng for all new colorectal carcinoma diagnoses - PMS2, MSH2, MSH6 loss - > suggest referral to a clinical genedcist - MLH1 (and PMS2) loss we have standard comments
21 Our standard comments 1. For padents less than 70 years of age Immunoperoxidase stains for the mismatch repair enzymes MLH1, PMS2 and MSH6 show loss of staining of carcinoma nuclei for MLH1 and its binding partner PMS2. MLH1- deficient colorectal carcinoma can be caused by Lynch syndrome or by sporadic MLH1 methylason. BRAF gene tessng can be performed upon request to dissnguish between these two ensses. 2. For padents over 70 years of age Immunoperoxidase stains for the mismatch repair enzymes MLH1, PMS2 and MSH6 show loss of staining of carcinoma nuclei for MLH1 and its binding partner PMS2. MLH1- deficient colorectal carcinoma can be caused by Lynch syndrome or by sporadic MLH1 methylason. In pasents over 70 years of age, sporadic MSI cancer is usual.
22
23 MLH1


24 CRC in PMS2 mutadon carrier MLH1 PMS2
25 Serrated Morphology versus the Serrated Neoplasia Pathway This is a confusing issue Serrated adenocarcinoma is now a specific subtype in the WHO, but the significance of the diagnosis is unclear and (in my opinion) the diagnosis lacks reproducibility Clinicians usually either don t understand what it means (nor do I), misinterpret what it means or ignore it Serrated morphology does not equal serrated neoplasia pathway
26 Examples of Serrated Carcinomas
27
28
29
30
31
32
33 Serrated Polyposis Syndrome DefiniDon - Remains clinical and arbitrary 1) At least 5 serrated polyps proximal to the sigmoid colon, at least two of which are >10mm 2) Any serrated polyp in a first degree reladve of a padent with serrated polyposis syndrome 3) >20 serrated polyps of any size distributed throughout the colorectum

34

35
36 Serrated Polyposis Syndrome Clinicopathological features - Most of the cancers are proximal - The mean age of onset is 50 years - Most padents will also have convendonal adenomas Surprising facts - 18% of padents meedng the criteria for SPS had MUTYH syndrome in one paper 1, actual figure is likely to be much less, but sdll requires consideradon - The cancers in SPS padents are not uniform, less than half have a BRAF mutadon and only 38% are MMRD 2 1. Boparai et al; Gastroenterology Rosty et al; AJSP 2013
37 Serrated Polyposis Syndrome Cancer risk and surveillance - The cancer risk is not clear and probably reflects a heterogeneous populadon - Probably <50% lifedme risk overall - No apparent risk of cancer outside the large bowel - Surveillance colonoscopy every 1-3 years depending on polyp burden - If adequate colonoscopic control is not possible, prophylacdc colectomy is reasonable - Risk to reladves is unclear, but there does appear to be an increased risk (up to 5 fold) - Start screening at age of CRC diagnosis or by 40
38 Summary Part II The serrated neoplasia pathway and Lynch syndrome are very different Pathologists should emphasise the disdncdon in reports, pardcularly when repordng mismatch repair enzymes Serrated morphology does not equal the serrated neoplasia pathway Serrated polyposis syndrome remains a clinicopathological endty The pathologist has a role in suggesdng SPS in reports (and considering MUTYH when appropriate)
39 Part III Serrated Colorectal Polyps
40 WHO classificadon WHO ClassificaSon of Tumours of the DigesSve System (4 th edison; 2010): HyperplasDc polyps microvesicular goblet cell mucin poor Sessile serrated adenoma Sessile serrated adenoma with dysplasia TradiDonal serrated adenoma
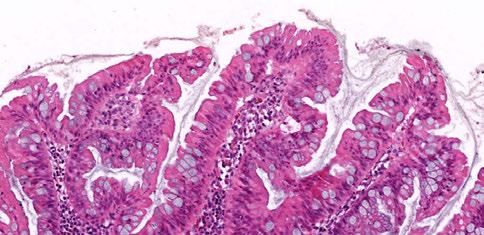
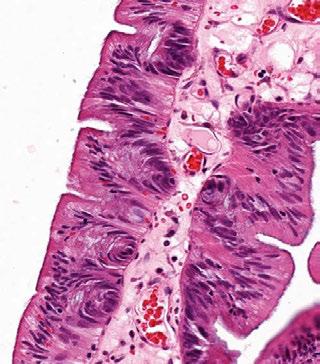
41 The Sessile Serrated Adenoma
42 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
43 The sessile serrated adenoma First recognised in 2003 Mostly proximal More common in women Variable size Definite risk of malignancy Require surveillance colonoscopy

44 Courtesy of David Hewet

45 Courtesy of David Hewet

46 Courtesy of David Hewet

47 Courtesy of David Hewet

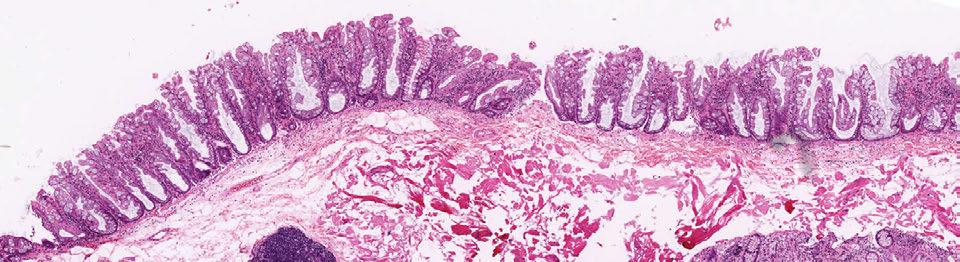
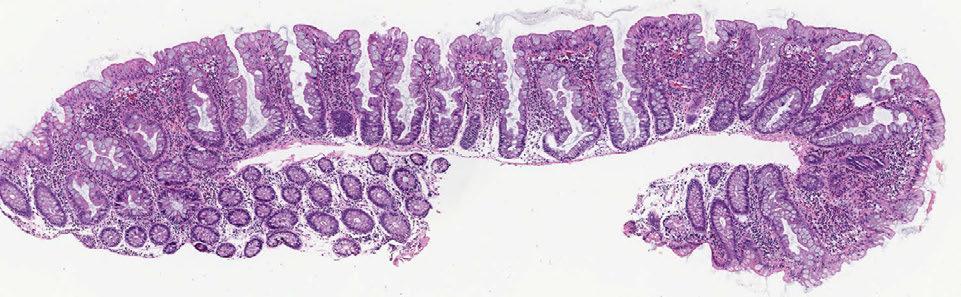
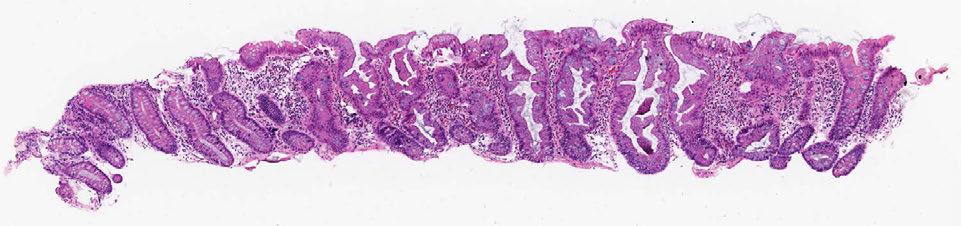
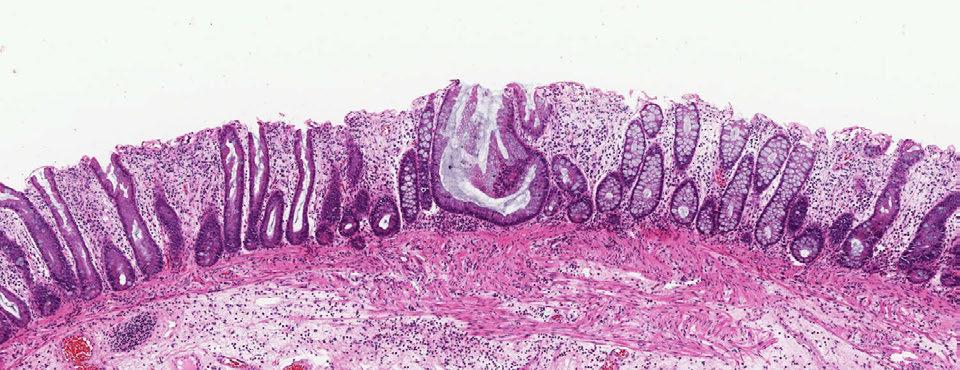
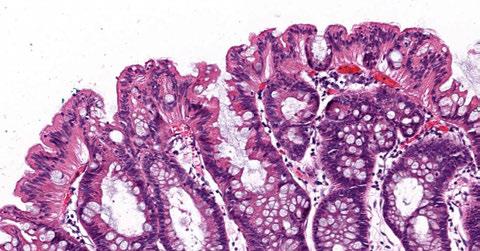
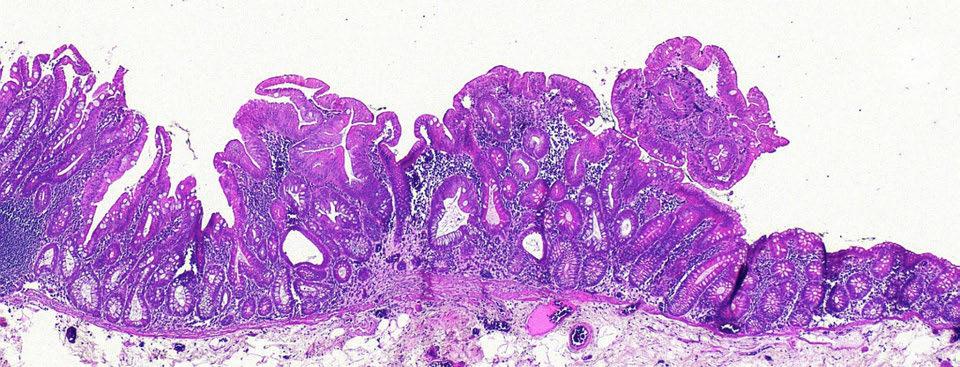
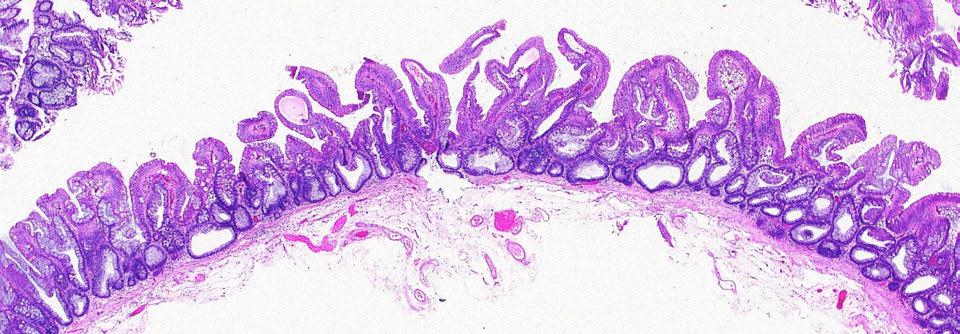
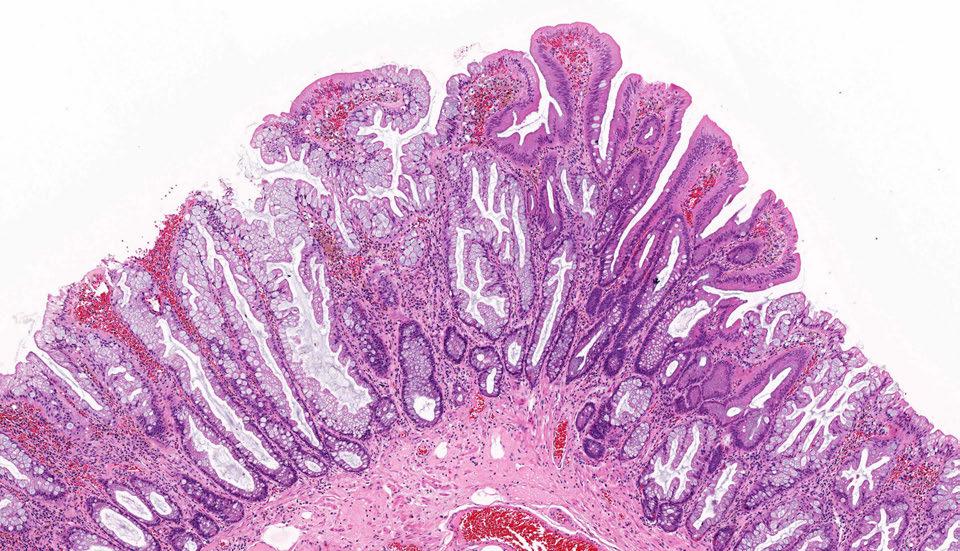
48 Sessile Serrated Adenoma

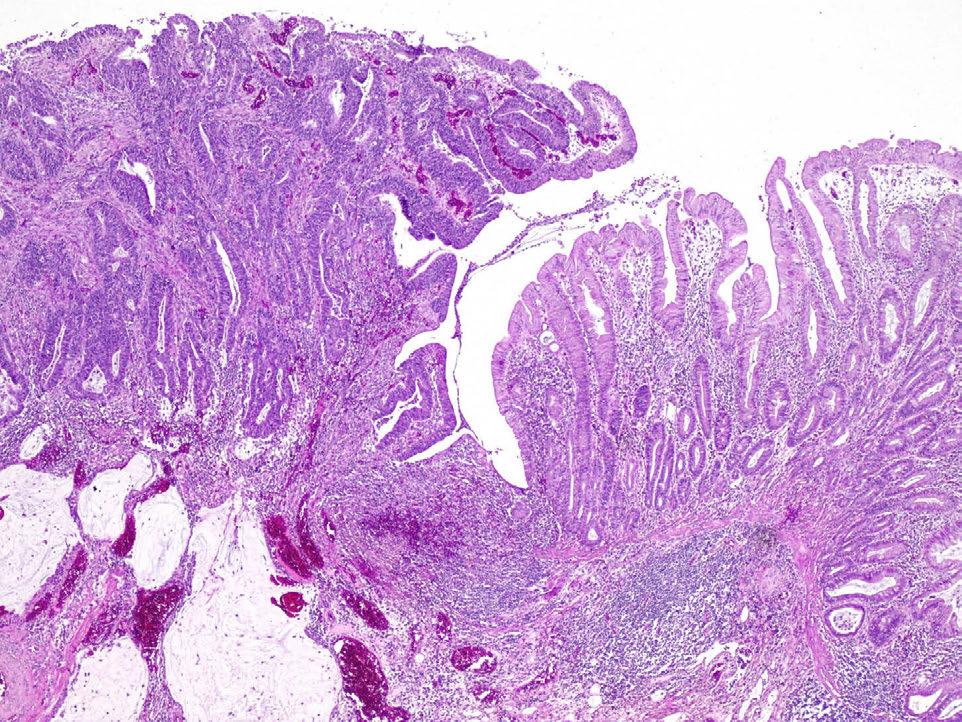
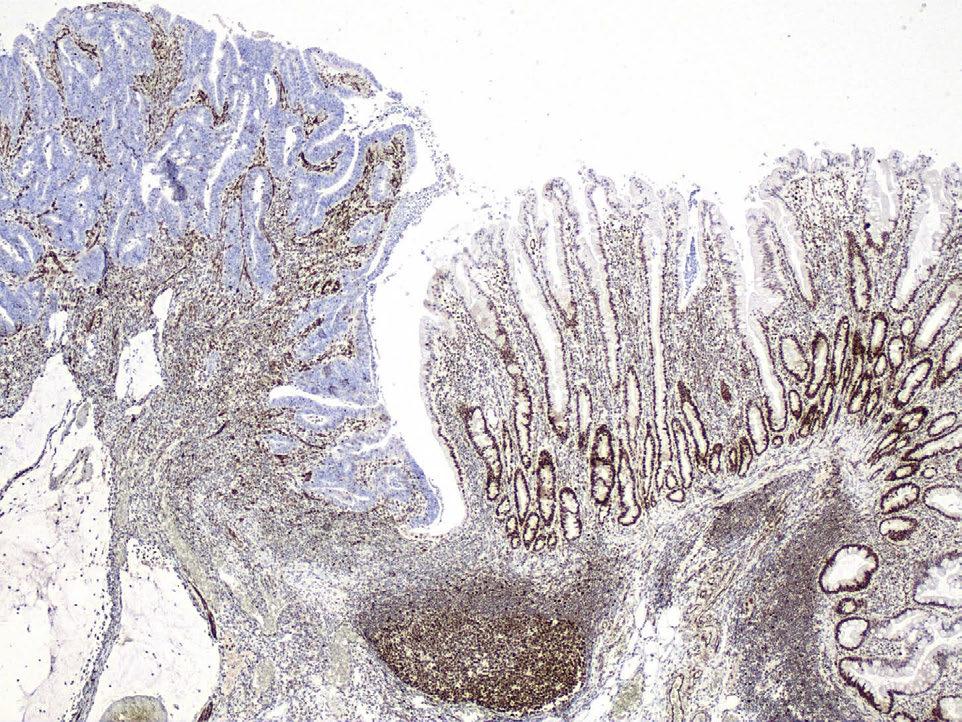
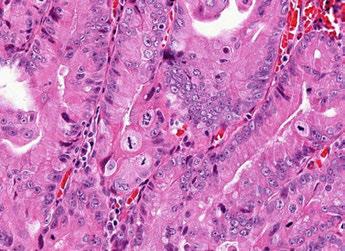
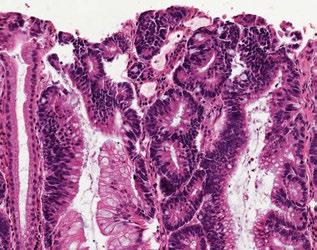
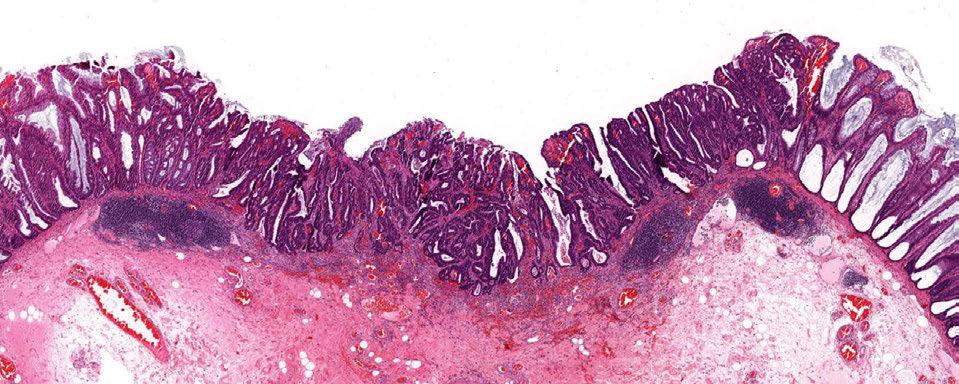
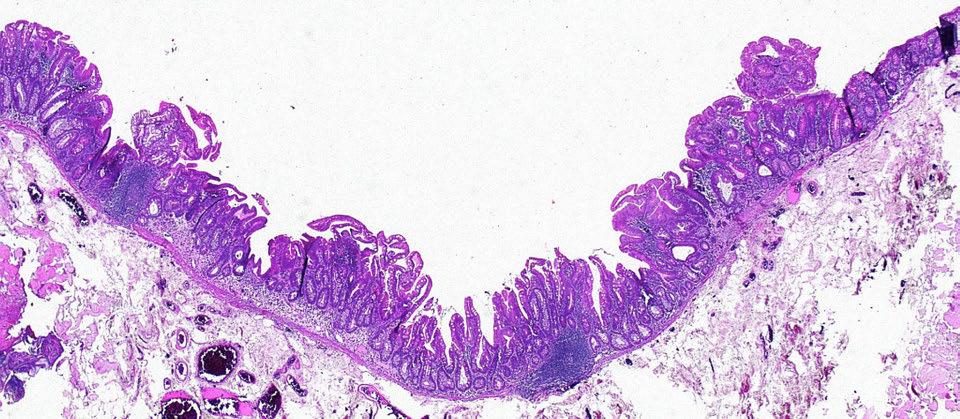
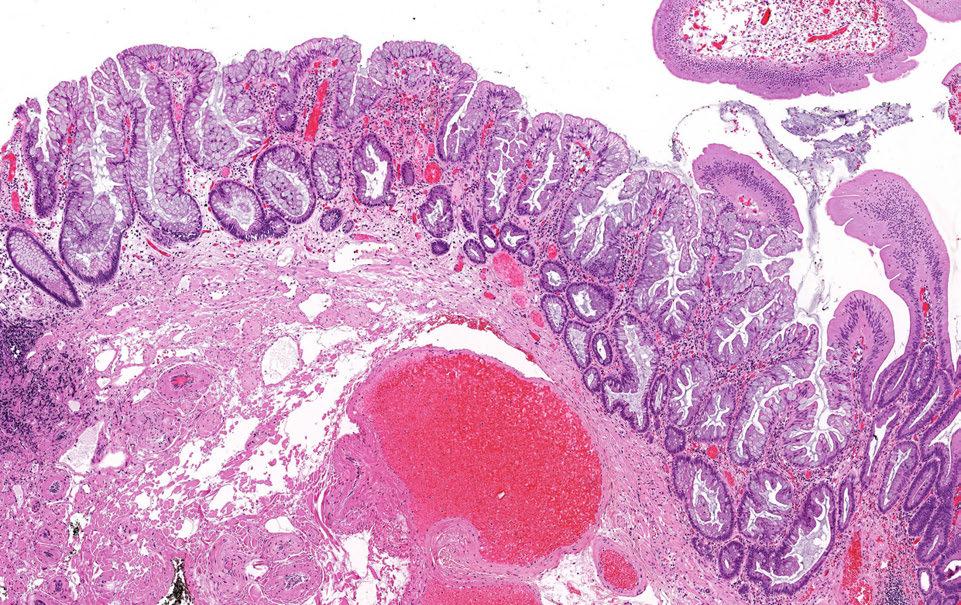
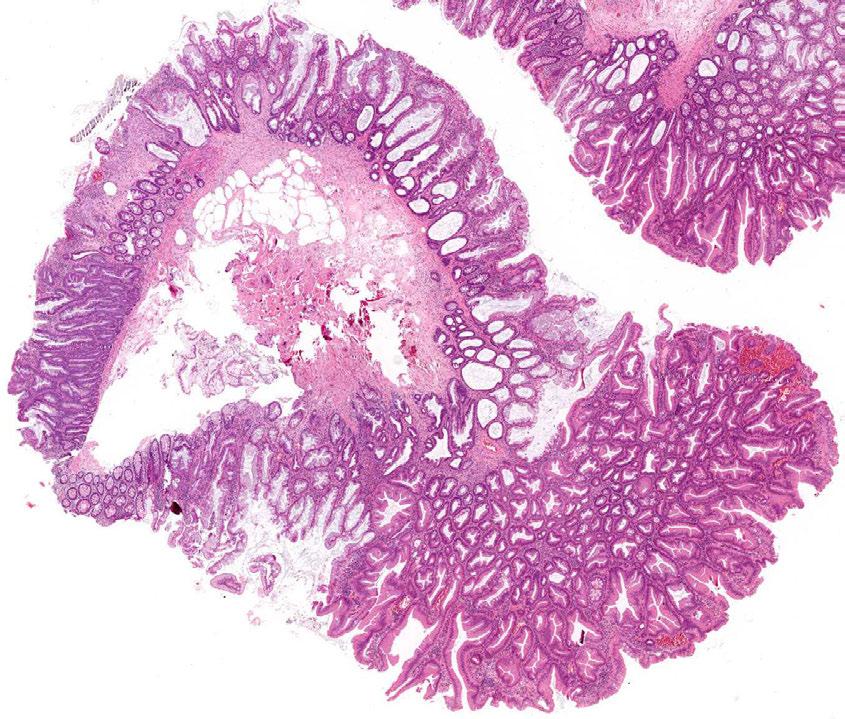
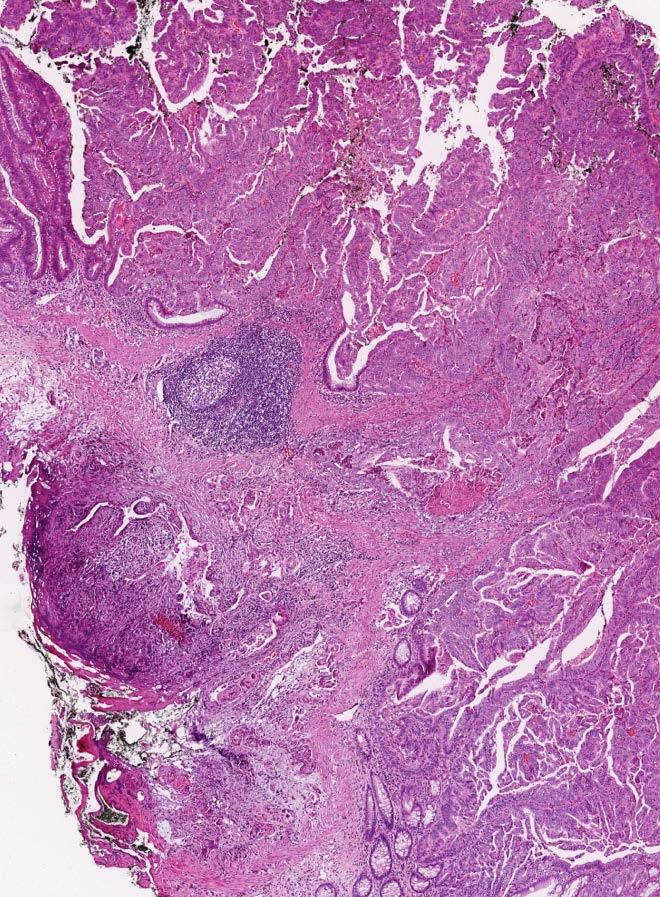
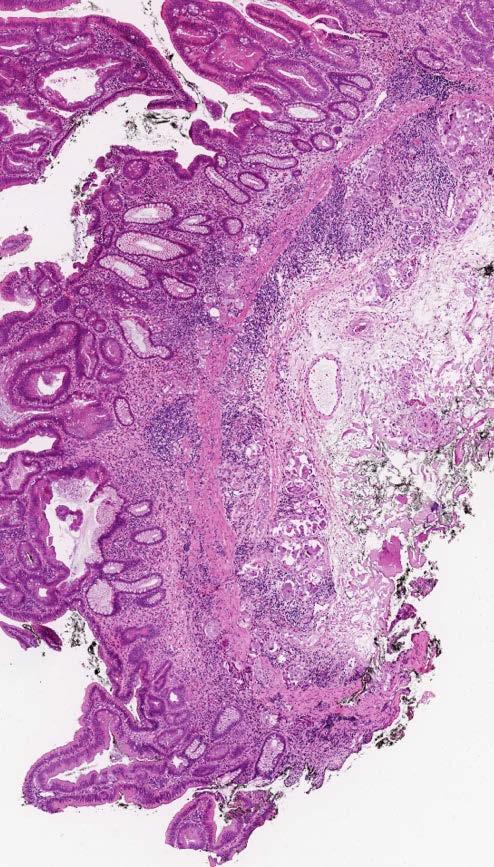
49 Sessile Serrated Adenoma with Dysplasia and Early Carcinoma
50 DiagnosDc criteria The diagnosdc criteria are variable Older criteria were fairly restricdve 2010 WHO relaxed the criteria substandally, requiring only 2-3 SSA type crypts More recently Rex et al, have proposed even one SSA- type crypt as sufficient for the diagnosis

51 DiagnosDc criteria We gathered a consecudve series of colorectal polyps received at our pracdce over a three month period (n=6340) and undertook a central review of all of the cases. For all of the MVHPs and SSAs we further divided them according to the number of SSA type crypts per polyp

52
53 Results The locadon and gender distribudon of the serrated polyps was most logical using the expert panel criteria to separate MVHP from SSA

54 Results locadon divided by number of SSA type crypts
55 Results gender divided by number of SSA type crypts
56 MVHP versus SSA using the single crypt criteria

57
58
59
60
61
62 Results - frequency We found that SSAs are common Using the WHO criteria 12.1% of all colorectal polyps are SSAs Using the criteria of the expert panel 14.7% of colorectal polyps are SSAs
63 SSA prevalence We are conducdng a study of SSA prevalence based on data from 707 consecudve colonscopies by an experienced gastroenterologist in a public hospital outpadent se(ng Central pathological review of all polyps SSAs diagnosed using the single crypt criteria SSA prevalence is 20.1%
64
65 Risk of malignancy in an SSA This is a very difficult quesdon to answer, especially because the goalposts for a diagnosis of an SSA keep changing Consider that about 75% of colorectal carcinoma arise from convendonal polyps and convendonal polyps have a prevalence of approximately 50% About 25% of colorectal carcinoma arise from serrated polyps and serrated polyps have a prevalence of approximately 20% This would suggest the risk of malignancy in a serrated polyp is slightly less than a convendonal adenoma
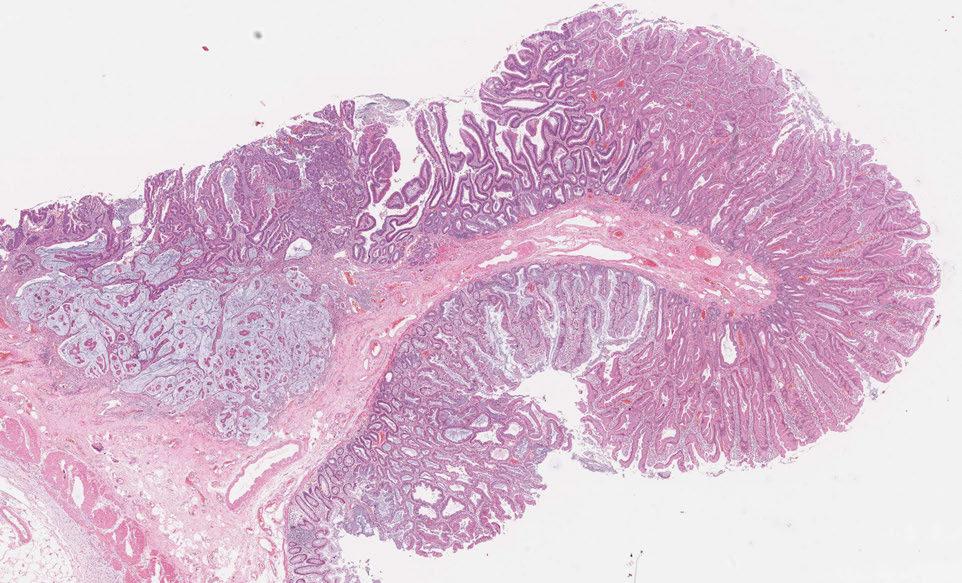
66 The sessile serrated adenoma with dysplasia
67 Much less is known about the SSAD Mostly because they are rare (0.4% of colorectal polyps) Much comes from small series and indirectly from what we know about ordinary SSAs and BRAF mutated colorectal carcinomas We have recently undertaken a study of advanced SSAs (SSAs with dysplasia and or carcinoma) to atempt to address some of the knowledge gaps
68 A series of 137 advanced SSAs We performed a detailed clinicopathological and molecular analysis of all cases Rigorous inclusion criteria: 1. Required an abrupt transidon from SSA to dysplasia in the one Dssue fragment 2. Excluded TSA arising in SSA 3. Sufficient Dssue for molecular analysis (BRAF, KRAS, CIMP, IHC)
69

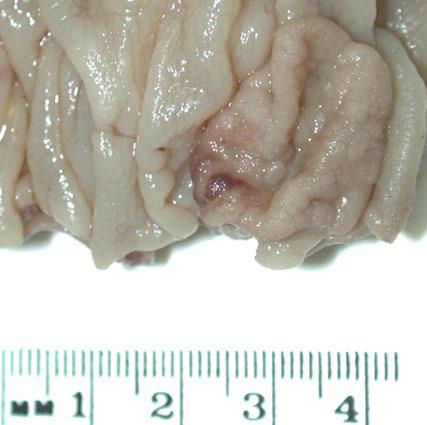
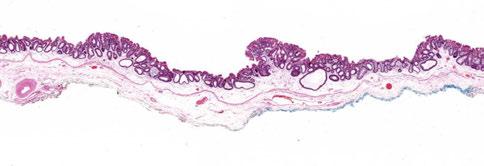
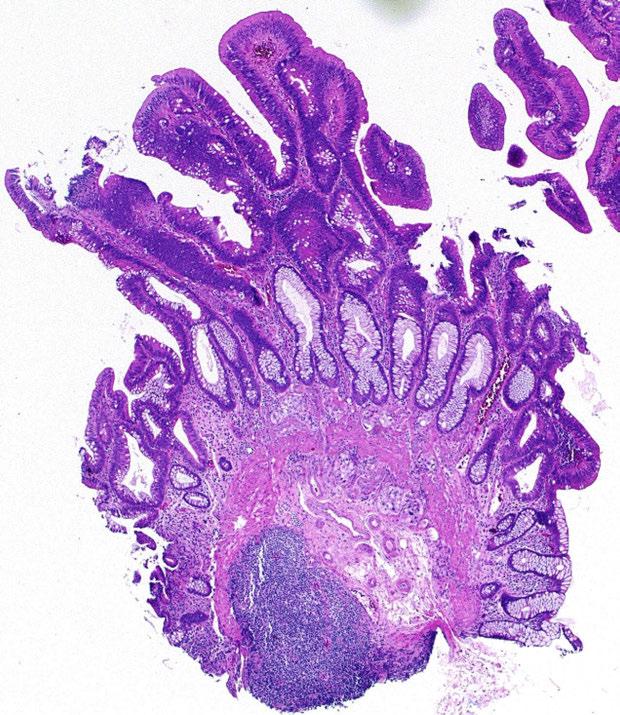
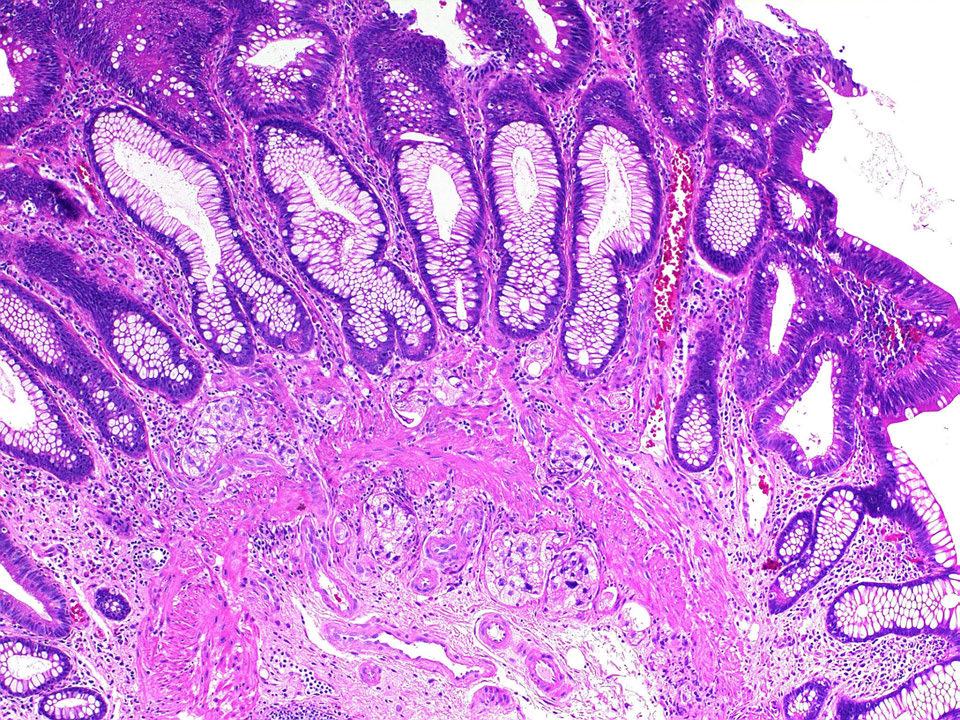
70 Clinicopathological features Advanced SSAs are predominantly small and flat polyps The median size of the cohort was 9mm 86% were flat

71 2.3mm SSADC Bar = 2mm
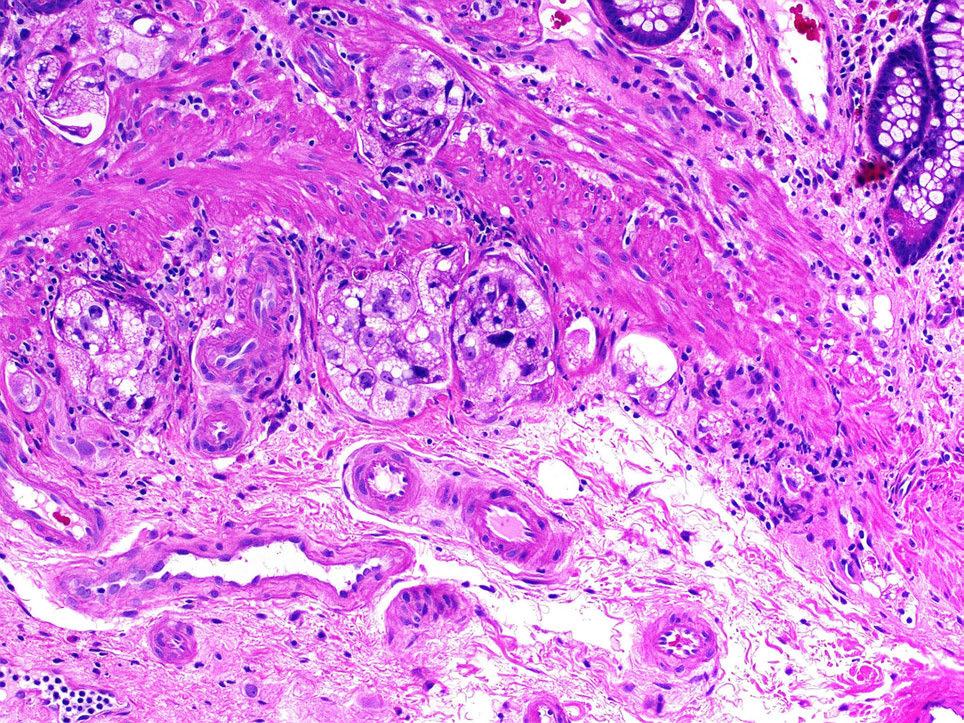
72 Clinicopathological features The transi>on from SSA to SSAD appears to be slow The transi>on from SSAD to carcinoma appears to be rapid Mean age of padents with ordinary SSAs 58.6 Mean age of padents with SSADs 75.3 Mean age of padents with SSAs with component of carcinoma 75.1 SSA versus SSAD (p- value <0.0001) SSAD versus SSA with carcinoma (p- value )
73
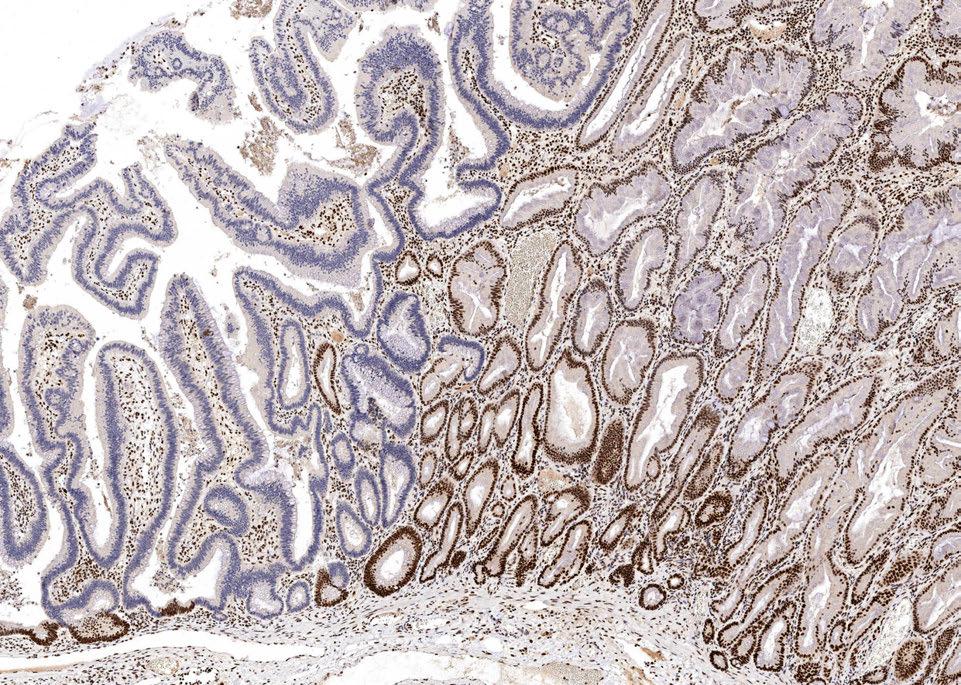
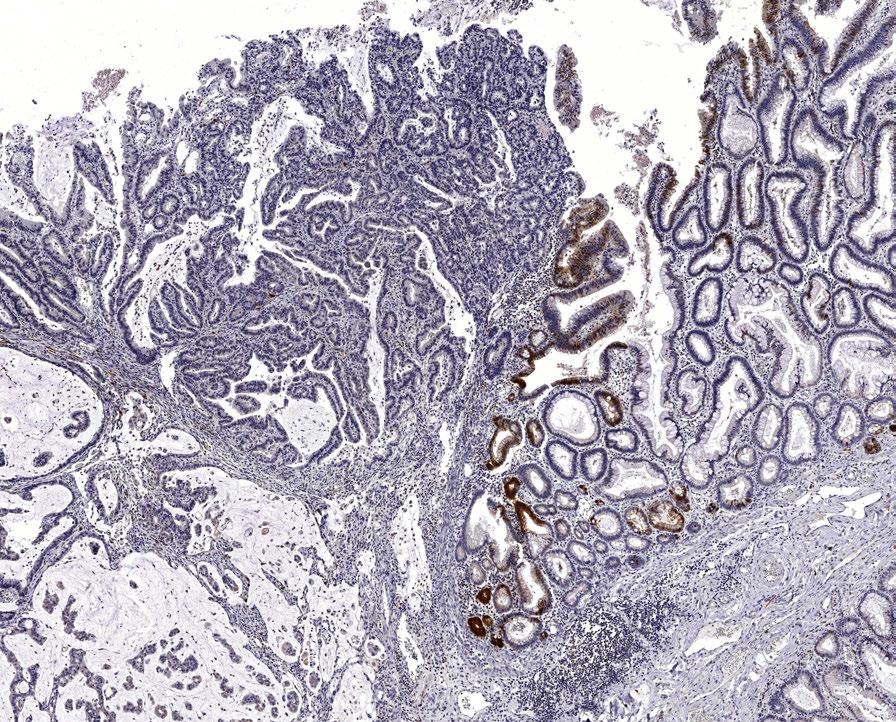
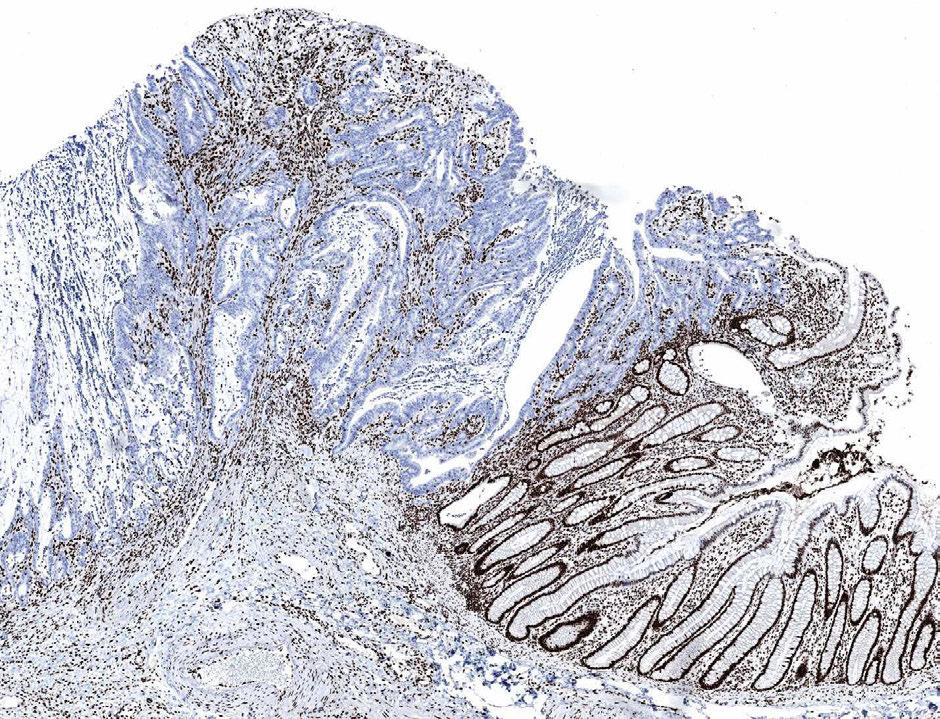
74 Molecular features 75% of the cohort was mismatch repair deficient Mismatch repair status divides SSAD/Cs into dis>nct clinical and molecular en>>es


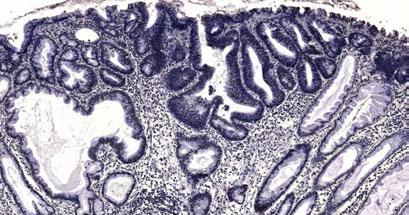
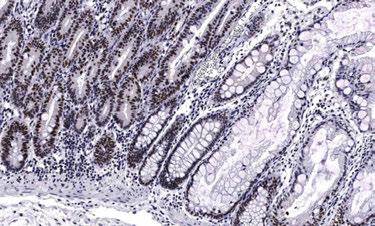
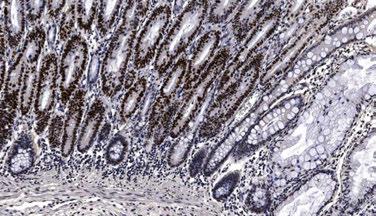
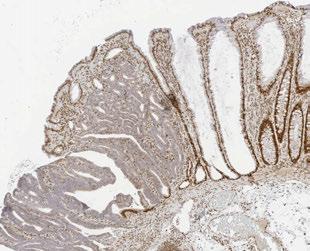
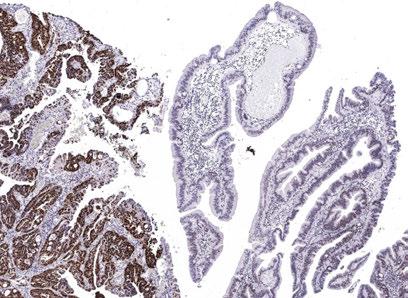
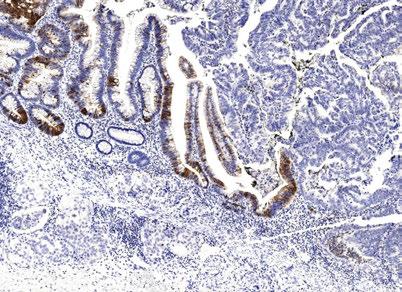
75 MMRD SSAD MMRP SSAD MLH1 MLH1 p53 p53
76
77 MMRD SSADCa
78 MLH1
79
80 p16
81

82 β- catenin
83 Key findings and clinical implications 1) Most of the study polyps were proximal, small (<10mm) and flat making them difficult to detect at colonoscopy 2) Progress to cancer by a combinadon of MLH1 and p16 silencing, WNT pathway acdvadon and TP53 mutadon (and almost certainly other methyladon / mutadon events) 3) There appears to be a rapid progression from SSAD to cancer meaning if they are missed, cancer can develop in the surveillance interval 4) The mismatch repair status separates these polyps into disdnct clinical and molecular subtypes. This is important because the MMRP subtype is the precursor of the most aggressive molecular subtype of colorectal carcinoma

84 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
85 Proposed pathways to carcinoma for sessile serrated adenomas Normal mucosa BRAF / CIMP MethylaDon of MLH1 MVHP / SSA MMRD SSAD MMRP SSAD BRAF mutant MSI CRC 75% MethylaDon of CDKN2A Wnt pathway acdvadon BRAF mutant MSS CRC 25% TP53 mutadon
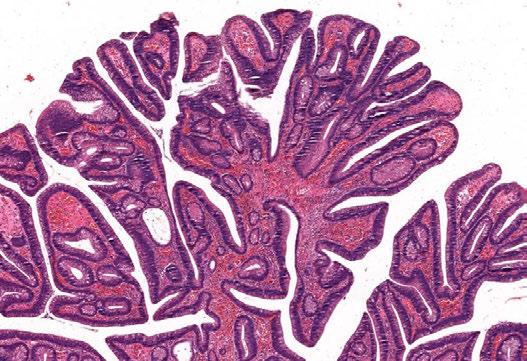
86 The TradiDonal Serrated Adenoma
87 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
88 A controversial endty For a lesion that is seemingly straighvorward to diagnose, the TSA is quite controversial The diagnosdc criteria are not all that clear The molecular features are quite variable The malignant risk is not known The pathways and types of cancer that arise from them are also not endrely clear

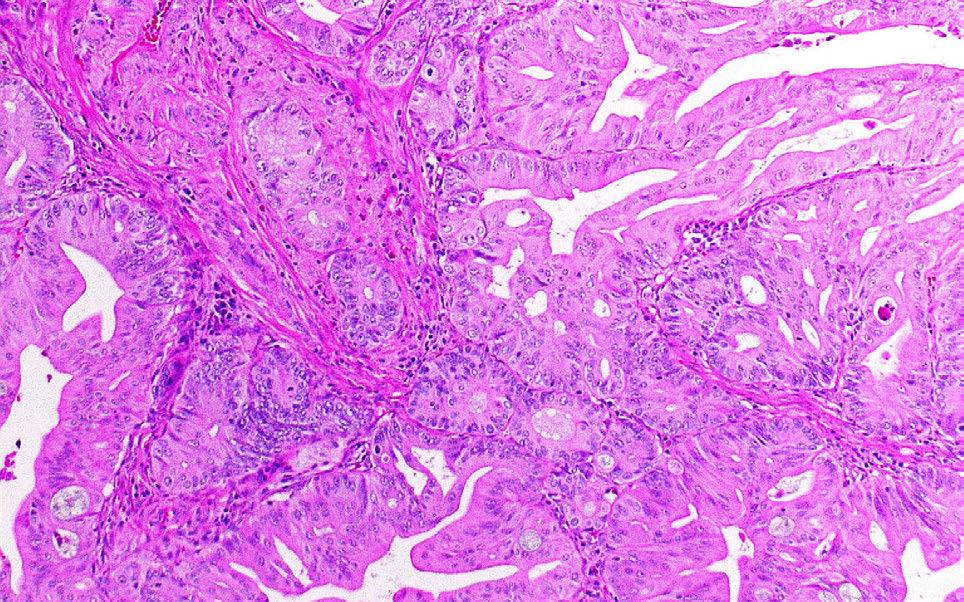
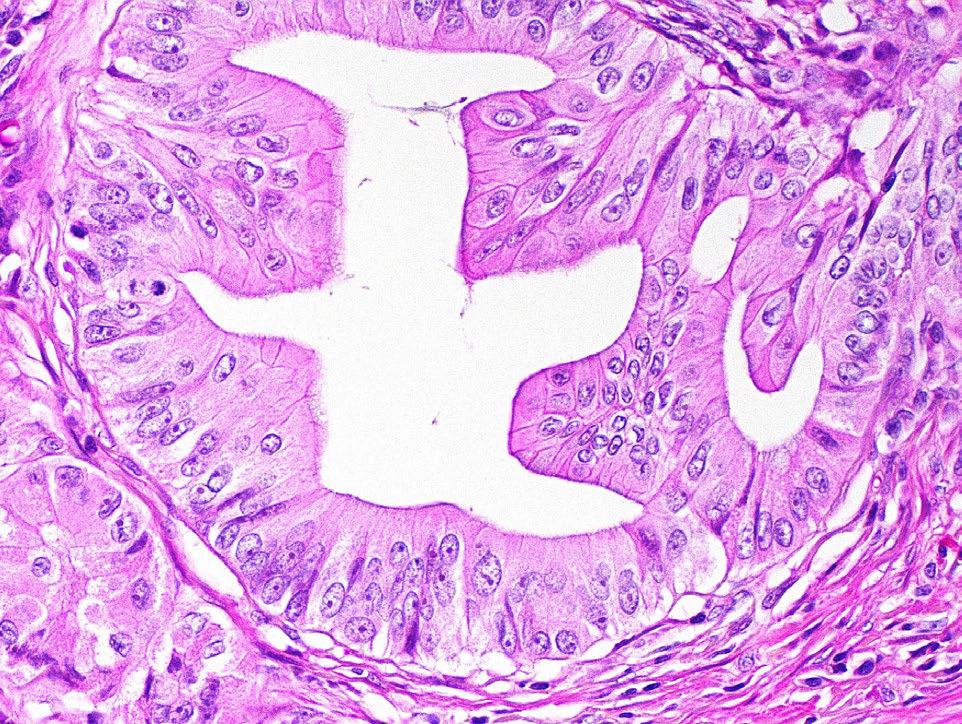
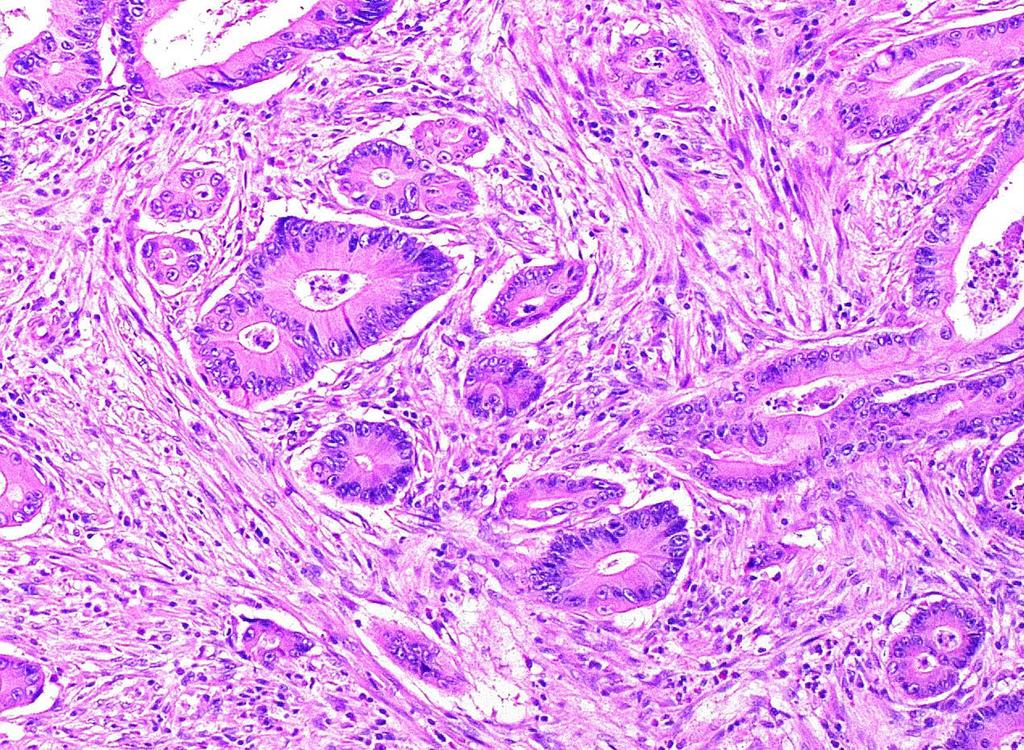
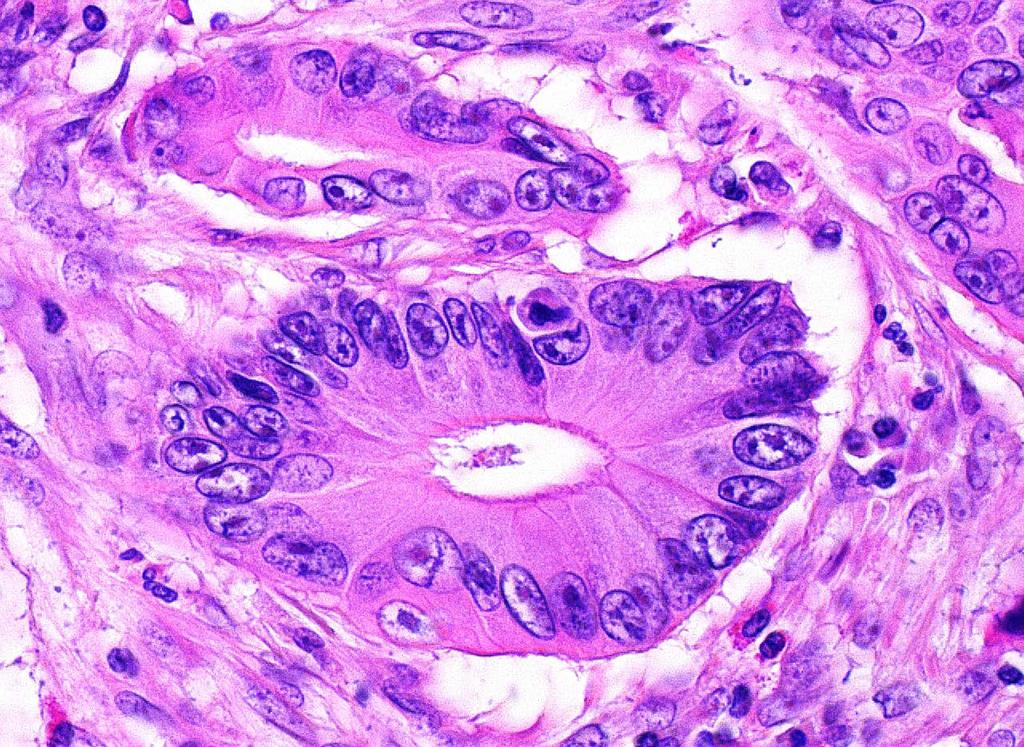
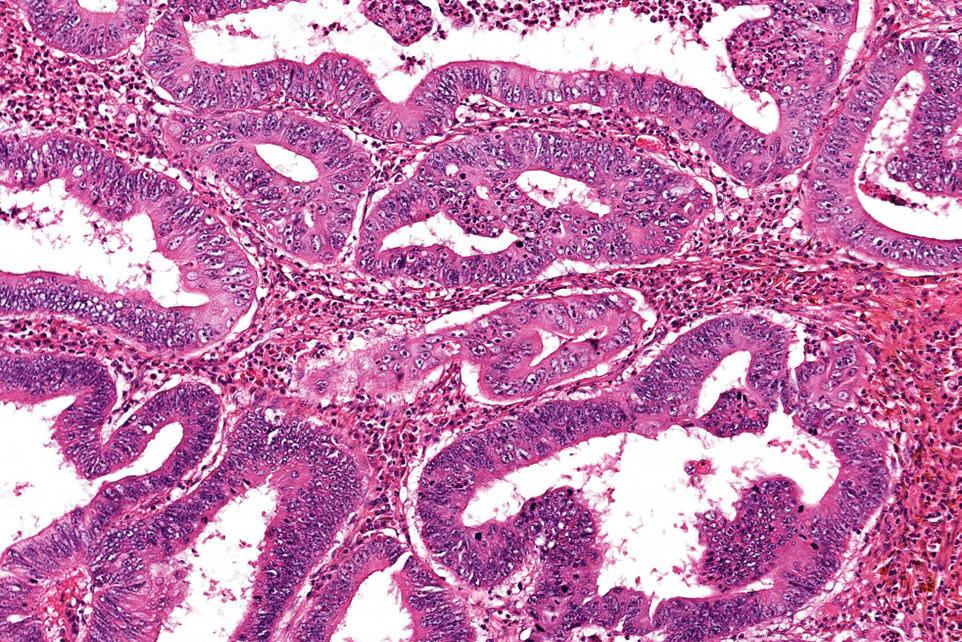
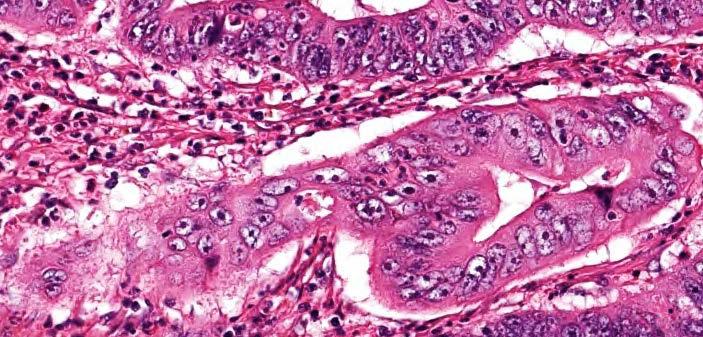
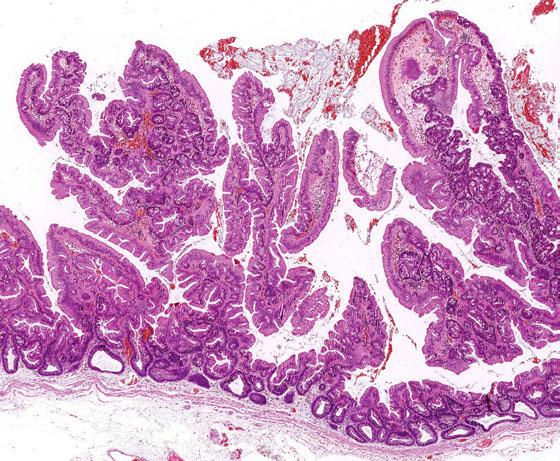
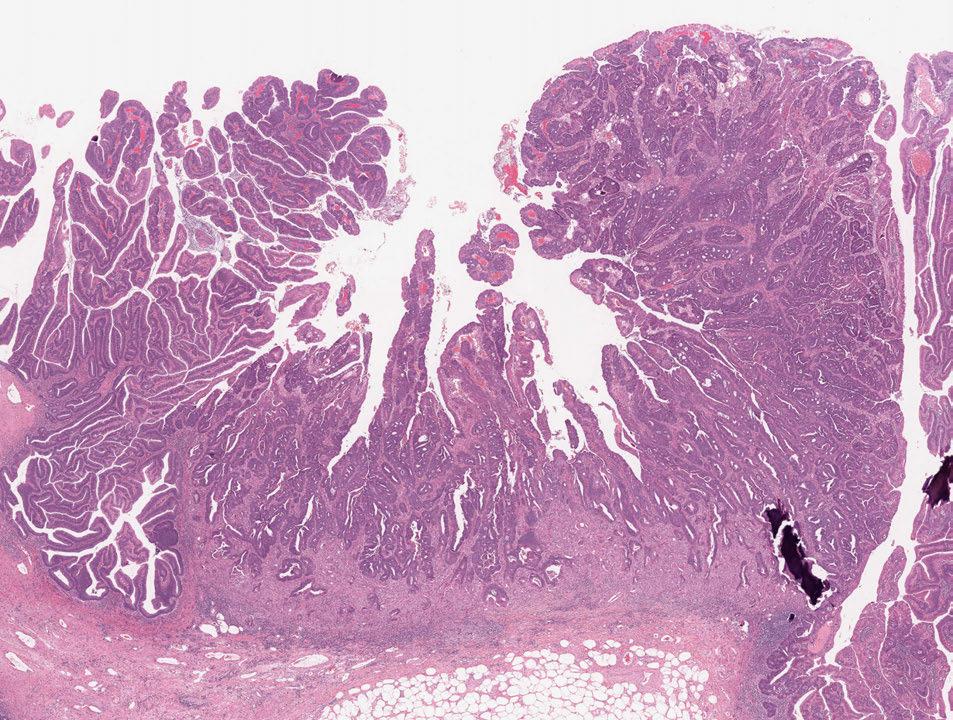
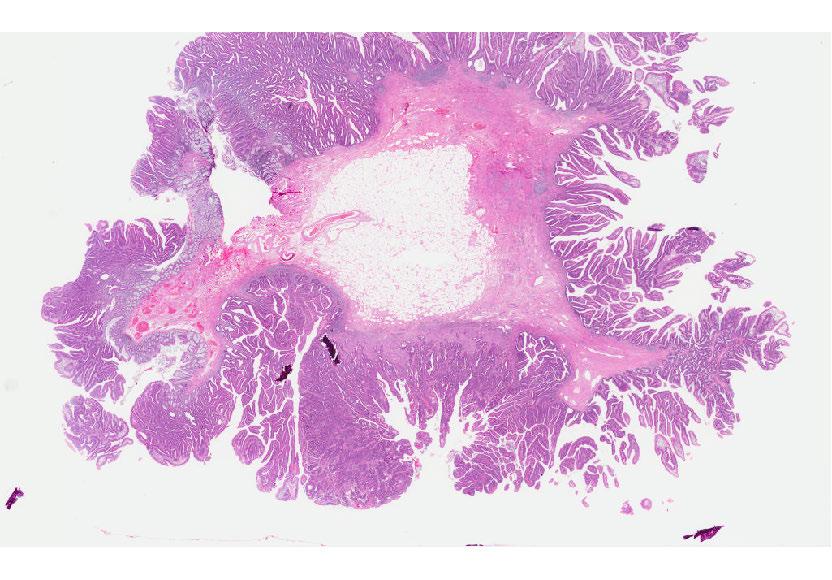
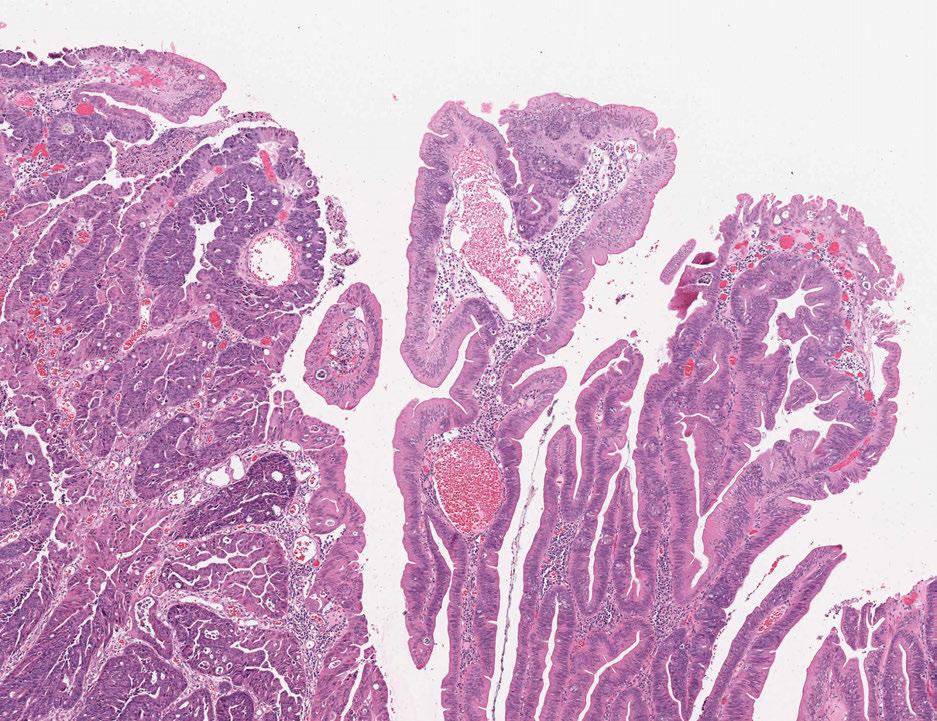
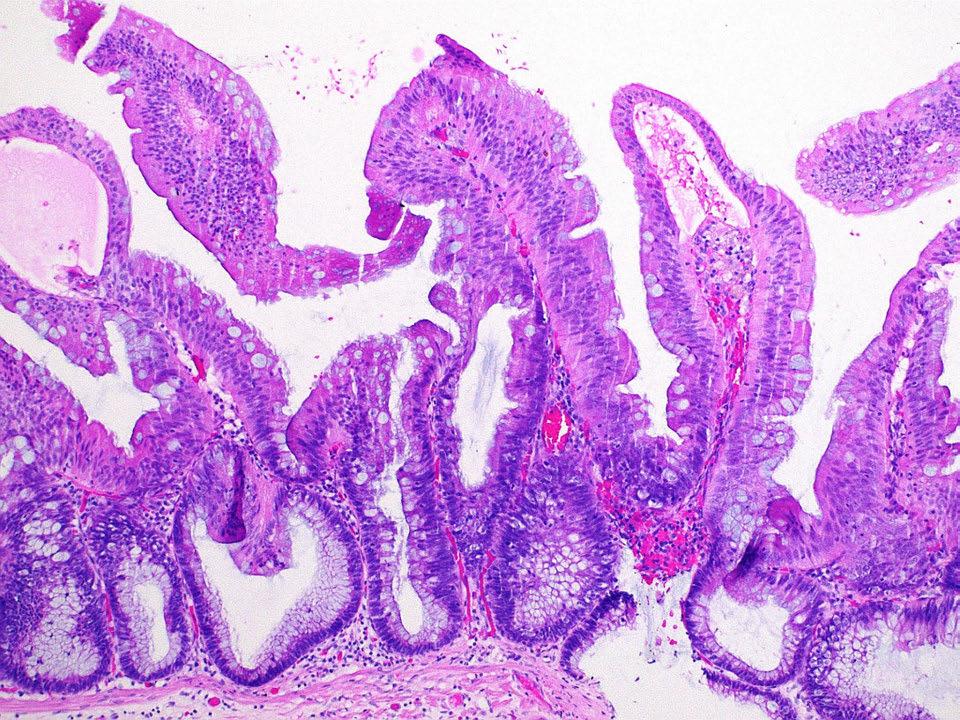
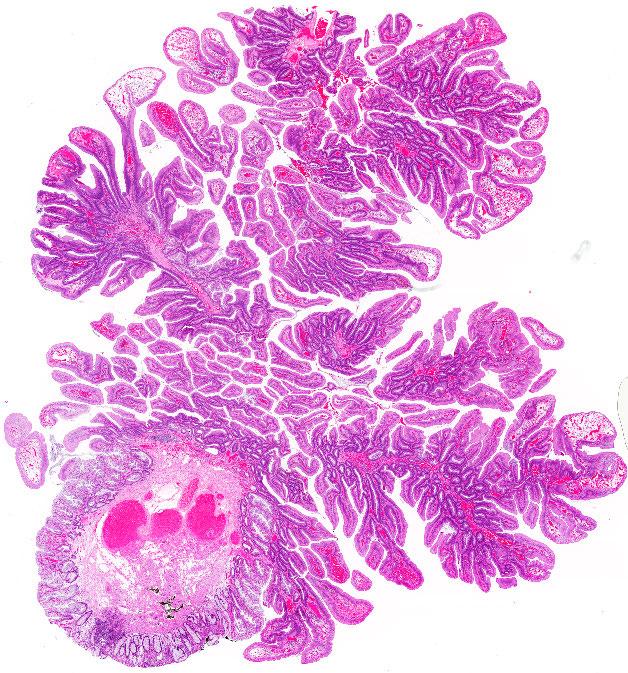
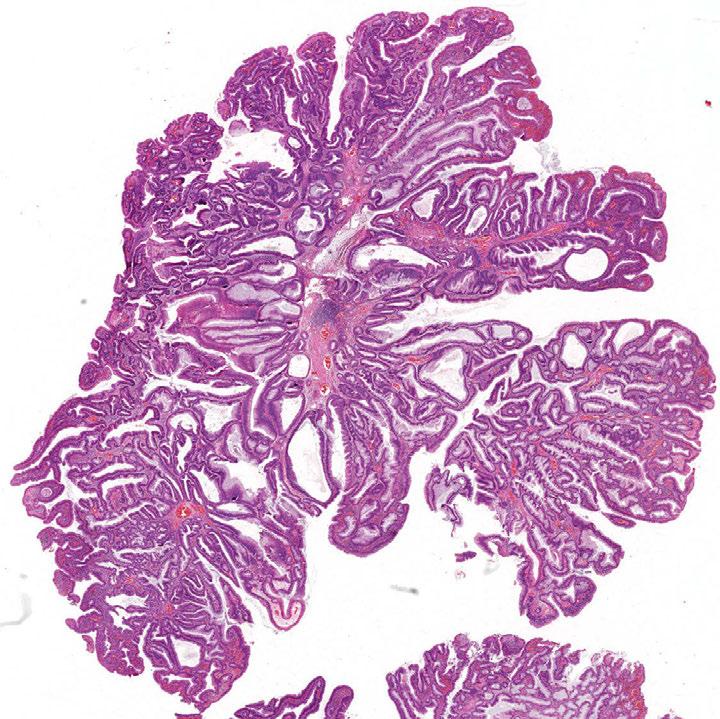
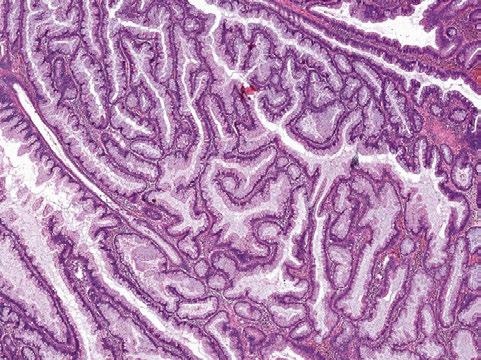
89 TradiDonal Serrated Adenoma

90 Kim MJ, Lee EJ, et al. Am J Clin Pathol 2013; 140:
91 Morphological features We like to see at least two of; 1. Eosinophilic cells 2. Ectopic crypt formadons 3. Slit- like serradons To call overt dysplasia we have similar criteria to an SSA i.e. an abrupt transidon from ordinary TSA to overt cytological dysplasia
92
93
94
95
96
97 TSAs can be broadly divided by either their BRAF and KRAS mutadon status or by the presence of advanced histology
98 TSAs can be flat In our study 38% of the TSAs were flat This has also been demonstrated by others More likely in the proximal colon and may be a reflecdon of intraluminal factors

99 Sigmoid Sigmoid Rectum Rectum
100
101
102
103
104 TSAs have frequent origin in an SSA or MVHP In our study 38% of the TSAs were had origin in an SSA or MVHP But it was restricted to BRAF mutated cases (57%) This has also been demonstrated by others
105
106

107 QIMR Berghofer Medical Research InsDtute 107
108
109
 - CIMP+ 46.3% MutaDon and CIMP status - BRAF mutadon in 22 (57.9%) - KRAS mutadon in 10 (26.3%) - Wild type in 6 (15.8%) - CIMP+ 44.")
110 Molecular features of TSAs BRAF/KRAS mutadon status and CIMP Ordinary TSAs Advanced TSAs MutaDon and CIMP status - BRAF mutadon in 112 (69.1%) - KRAS mutadon in 33 (20.4%) - Wild type in 17 (10.5%) - CIMP+ 46.3% MutaDon and CIMP status - BRAF mutadon in 22 (57.9%) - KRAS mutadon in 10 (26.3%) - Wild type in 6 (15.8%) - CIMP+ 44.7% CIMP high by muta>on status 100% 80% 60% 40% 20% 0% BRAF KRAS Wild
111 Molecular features of TSAs MMR funcdon MLH1 expression is retained in 99.5% of TSAs indica>ng a MICROSATELLITE STABLE PHENOTYPE
112 Molecular features of TSAs WNT signaling Nuclear β- catenin (ordinary TSAs) 100% 80% 60% 40% 20% Nuclear β- catenin (advanced TSAs) 100% 80% 60% 40% 20% 0% BRAF KRAS Wild type 0% p=< (ordinary vs advanced) BRAF KRAS Wild type
113 Molecular features of TSAs p53 Nuclear p53 (ordinary TSAs) Nuclear p53 (advanced TSAs) 100% 80% 60% 40% 20% 0% BRAF KRAS Wild 100% 80% 60% 40% 20% 0% p=< (ordinary vs advanced) BRAF KRAS Wild


114 Molecular features of TSAs p16 P16 staining in TSAs with dysplasia 100% 80% 60% 40% 20% P16 staining in TSAs with CRC 100% 80% 60% 40% 20% 0% BRAF KRAS/Wt 0% BRAF KRAS/Wt

115 β- catenin β- catenin p53 p16
116 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
117 Proposed pathways to carcinoma for tradi>onal serrated adenomas BRAF pathway Normal mucosa BRAF / CIMP KRAS pathway Normal mucosa MVHP / SSA KRAS TSA arising in MVHP/SSA TSAD P16 silencing P53 mutadon, Wnt pathway acdvadon TSA TSAD BRAF mutant MSS CRC KRAS mutant MSS CRC
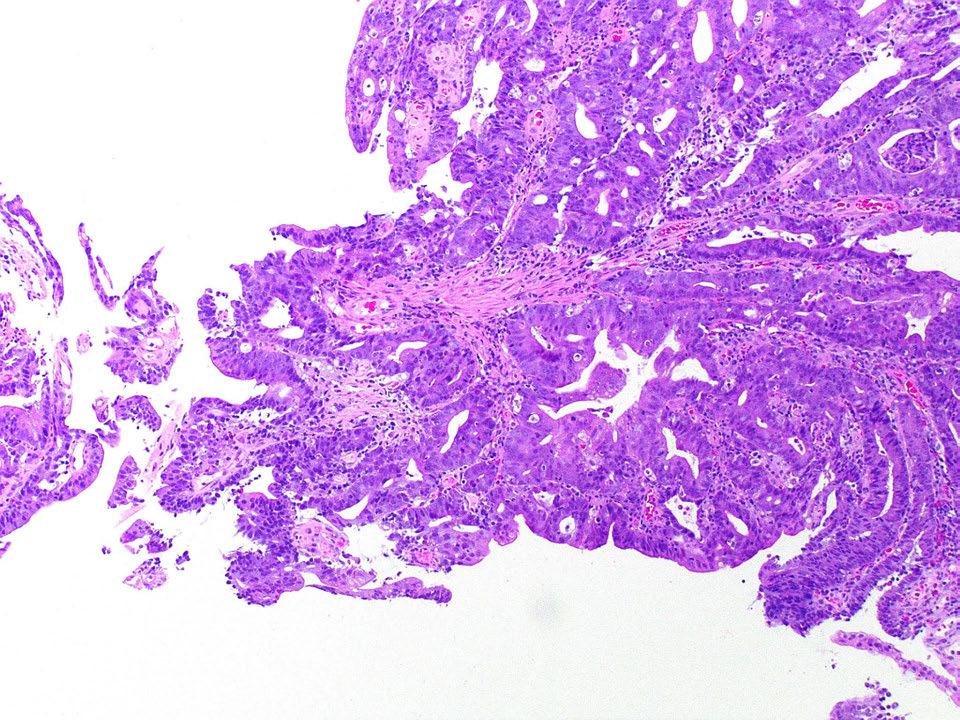
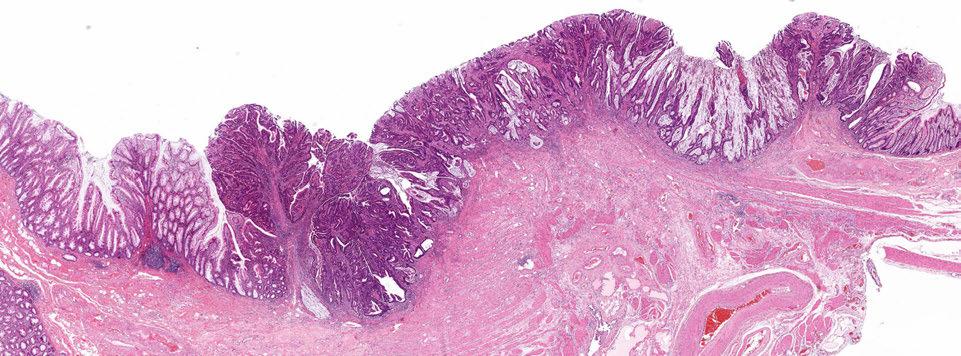
118 Serrated tubulovillous adenoma

119 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
120 Serrated Tubulovillous Adenoma (stva) a variant of convendonal tubulovillous adenoma (ctva) confused morphologically with tradidonal serrated adenoma postulated to be a precursor of KRAS mutated colon cancer no detailed studies available

 TradiDonal")
121 A subset of colorectal polyps are difficult to classify Tubulovillous adenoma Intermediate polyp (serrated tubulovillous adenoma) TradiDonal serrated adenoma
122 Serrated tubulovillous adenoma We collected a series of these difficult to classify polyps for clinicopathological and molecular analysis DiagnosDc criteria 1. Villous architecture in >25% of the polyp 2. SerraDon in >50% of the polyp 3. Lack of cytology and slit- like serradons seen in tradidonal serrated adenomas
123 DiagnosDc criteria 1. Villous architecture in >25% of the polyp 2. SerraDon in >50% of the polyp 3. Lack of cytology and slit- like serradons seen in tradidonal serrated adenomas
124

125
126 Serrated TVAs are rare When using our criteria: - 27 of 412 tubulovillous adenomas met the inclusion criteria - This represents 0.3% of all colorectal polyps We achieved a high level of diagnosdc reproducibility - Light s kappa value of 0.85 ( ) - This indicates excellent concordance - But this was opdmal condidons

127 Clinicopathological comparison
128 Molecular comparison
129 Summary of the serrated TVA The serrated tubulovillous adenomas is a rare polyp that can be reliably diagnosed It has disdnct clinicopathological and molecular features Compared to the convendonal tubulovillous adenoma the serrated tubulovillous adenoma is - larger - more o`en proximal - more o`en displays advanced histology - shows more frequent CIMP and - much more likely to harbour a KRAS muta>on Compared to the tradidonal serrated adenoma, the serrated tubulovillous adenoma is - more o`en proximal - has less CIMP and - has far more frequent Wnt pathway ac>va>on
130 Serrated ConvenDonal BRAF / CpG island methylator phenotype- high Normal Mucosa Normal Mucosa Sessile serrated adenoma Wnt pathway acdvadon MLH1 silencing TradiDonal serrated adenoma arising in sessile serrated adenoma KRAS / CpG island methylator phenotype low TradiDonal serrated adenoma Tubulovillous adenoma APC +/- MGMT methyladon KRAS / CpG island methylator phenotype low/negadve Tubular adenoma/ convendonal tubulovillous adenoma Sessile serrated adenoma with dysplasia TP53 mutadon, Wnt pathway acdvadon Serrated tubulovillous adenoma HypomethylaDon TP53 mutadon TradiDonal serrated adenoma with dysplasia TradiDonal serrated adenoma with dysplasia Serrated tubulovillous adenoma with high grade dysplasia Tubular adenoma/ convendonal tubulovillous adenoma with high grade dysplasia CDKN2A silencing SMAD4 APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite unstable carcinoma APC wild- type BRAF mutant CpG island methylator phenotype high Microsatellite stable carcinoma APC wild- type KRAS mutant CpG island methylator phenotype low Microsatellite stable carcinoma APC mutant KRAS mutant CpG island methylator phenotype low/nega>ve Microsatellite stable carcinoma APC mutant KRAS/BRAF wild- type CpG island methylator phenotype nega>ve Microsatellite stable carcinoma 10-15% 5% 5% 20-25% 50-60%
131 Some illustradve cases

132 Female 76 Biopsy of caecal polyp ( )

133 Female now 77 Biopsy of caecal lesion ( )
134

135

136 3 days later
137
138

139 Female 27 Biopsy of transverse colon polyp
140
141
142
143 QIMR Berghofer Medical Research InsDtute 143

144 QIMR Berghofer Medical Research InsDtute 144
145 QIMR Berghofer Medical Research InsDtute 145
146

147 QIMR Berghofer Medical Research InsDtute 147
148
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
Beyond the APC era Alternative pathways to CRC. Jeremy R Jass McGill University
 Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Colon Cancer and Hereditary Cancer Syndromes
 Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Serrated Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO
 Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO In the prelude to this article ( Polyps Part I: Their Confusing History) we discussed the evolution of colorectal serrated polyp classification,
Polyps, Part 2: Their Mechanisms and Management Ryan C. Romano, DO In the prelude to this article ( Polyps Part I: Their Confusing History) we discussed the evolution of colorectal serrated polyp classification,
Serrated Colorectal Polyps New Challenges to Old Dogma. Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN
 Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Serrated Colorectal Polyps New Challenges to Old Dogma Kenneth Batts, M.D. Abbott Northwestern Hospital Minneapolis, MN A Sneak Preview.... This was in the good old days: Adenomas HPPs Mixed Polyps A Sneak
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on the serrated pathway to colorectal carcinoma
 Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Human Pathology (2010) xx, xxx xxx www.elsevier.com/locate/humpath Progress in pathology Update on the serrated pathway to colorectal carcinoma Dale C. Snover MD Department of Pathology, Fairview Southdale
Pathology of serrated colorectal lesions
 Correspondence to Dr Adrian C Bateman, Department of Cellular Pathology, University Hospital Southampton NHS Foundation Trust, MP002, Level E, South Block, Southampton General Hospital, Tremona Road, Southampton
Correspondence to Dr Adrian C Bateman, Department of Cellular Pathology, University Hospital Southampton NHS Foundation Trust, MP002, Level E, South Block, Southampton General Hospital, Tremona Road, Southampton
A WHO update on Serrated Polyps
 A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
A WHO update on Serrated Polyps Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Am J Gastroenterol. 2010 Nov 2. [Epub ahead of The Clinical Significance of Serrated Polyps.
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
La genetica del carcinoma colo-rettale
 La genetica del carcinoma colo-rettale Ivana Cataldo Ospedale Ca Foncello, Treviso ARC-NET Centro di Ricerca Applicata sul Cancro AOUI, Verona OUTLINE What s new in colorectal cancer? Pathological Markers
La genetica del carcinoma colo-rettale Ivana Cataldo Ospedale Ca Foncello, Treviso ARC-NET Centro di Ricerca Applicata sul Cancro AOUI, Verona OUTLINE What s new in colorectal cancer? Pathological Markers
Genetic testing all you need to know
 Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
The Natural History of Right-Sided Lesions
 The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The molecular genetics of colorectal cancer
 1 Department of Gastroenterology, North Middlesex University Hospital, London, UK 2 Institute of Molecular Genetics, Cardiff University 3 Department of Gastroenterology, Queen s Hospital Romford, London,
1 Department of Gastroenterology, North Middlesex University Hospital, London, UK 2 Institute of Molecular Genetics, Cardiff University 3 Department of Gastroenterology, Queen s Hospital Romford, London,
The Clinical Significance of Serrated Polyps
 CLINICAL AND SYSTEMATIC S nature publishing group 229 CME The Clinical Significance of Serrated Polyps Christopher S. Huang, MD 1, Fr anc is A. Far raye, M D, M S c 1, Sh i Yang, M D 2 and Michael J. O
CLINICAL AND SYSTEMATIC S nature publishing group 229 CME The Clinical Significance of Serrated Polyps Christopher S. Huang, MD 1, Fr anc is A. Far raye, M D, M S c 1, Sh i Yang, M D 2 and Michael J. O
Colorectal cancer molecular biology moves into clinical practice
 1 Department of Laboratory Medicine, University of Washington, Washington, USA 2 Clinical Research Division, Fred Hutchison Cancer Research Center, Washington, USA 3 Department of Medicine, University
1 Department of Laboratory Medicine, University of Washington, Washington, USA 2 Clinical Research Division, Fred Hutchison Cancer Research Center, Washington, USA 3 Department of Medicine, University
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Gastroenterology, Hepatology & Digestive Disorders
 Research Article Gastroenterology, Hepatology & Digestive Disorders Investigating the Prevalence and Progression of Serrated Polyps Tampa VA Experience Shreya Narayanan MD 1*, Brijesh B. Patel MD 2, David
Research Article Gastroenterology, Hepatology & Digestive Disorders Investigating the Prevalence and Progression of Serrated Polyps Tampa VA Experience Shreya Narayanan MD 1*, Brijesh B. Patel MD 2, David
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Colon cancer: practical molecular diagnostics. Wade S. Samowitz, M.D. University of Utah and ARUP
 Colon cancer: practical molecular diagnostics Wade S. Samowitz, M.D. University of Utah and ARUP Disclosure Dr. Samowitz may receive royalties in the future related to the Ventana BRAF V600E antibody.
Colon cancer: practical molecular diagnostics Wade S. Samowitz, M.D. University of Utah and ARUP Disclosure Dr. Samowitz may receive royalties in the future related to the Ventana BRAF V600E antibody.
Universal Screening for Lynch Syndrome
 Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Inflammatory bowel disease (IBD) patients have a higher risk of
 patients have a higher risk of") Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease Alyssa M. Parian, MD, and Mark G. Lazarev, MD Dr Parian and Dr Lazarev are assistant professors of medicine at Johns Hopkins University
Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease Alyssa M. Parian, MD, and Mark G. Lazarev, MD Dr Parian and Dr Lazarev are assistant professors of medicine at Johns Hopkins University
Disclosure slide I Member of advisory board for AMGEN, ROCHE, BOEHRINGER I Speaker honoraria from FALK Pharma, Pfizer, Lilly and ROCHE I Third party f
 Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view
 colorectal cancer: The pathologist s point of view") Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Precision Genetic Testing in Cancer Treatment and Prognosis
 Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
Colorectal Cancer - Working in Partnership. David Baty Genetics, Ninewells Hospital
 Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis?
 E171 Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis? Authors Kensuke Shinmura 1, Kazuo Konishi 1, Toshiko
E171 Molecular features of colorectal polyps presenting Kudo s type II mucosal crypt pattern: are they based on the same mechanism of tumorigenesis? Authors Kensuke Shinmura 1, Kazuo Konishi 1, Toshiko
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
M. Azzam Kayasseh,Dubai,UAE
 Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
6 semanas de embarazo. Tubulovillous adenoma with dysplasia icd 10. Inicio / Embarazo / 6 semanas de embarazo
 Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer Predisposition
 SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 157073, 13 pages doi:10.4061/2011/157073 Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer
SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 157073, 13 pages doi:10.4061/2011/157073 Review Article Serrated Polyposis: An Enigmatic Model of Colorectal Cancer
Molecular subtyping: how useful is it?
 Molecular subtyping: how useful is it? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics at the NCT-Partner Site Dresden CMTD Disclosure
Molecular subtyping: how useful is it? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics at the NCT-Partner Site Dresden CMTD Disclosure
Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy Patient Cohort
 Gastroenterology Research and Practice, Article ID 374926, 1 pages http://dx.doi.org/1.1155/214/374926 Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy
Gastroenterology Research and Practice, Article ID 374926, 1 pages http://dx.doi.org/1.1155/214/374926 Research Article The CIMP Phenotype in BRAF Mutant Serrated Polyps from a Prospective Colonoscopy
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Histo-prognostic factors what histopathology has to offer for clinical decision making
 Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Colorectal Cancer Screening and Surveillance
 1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
FAMILIAL COLORECTAL CANCER. Lyn Schofield Manager Familial Cancer Registry
 FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Molecular Diagnosis for Colorectal Cancer Patients
 Molecular Diagnosis for Colorectal Cancer Patients Antonia R. Sepulveda MD, PhD, FCAP October, 20, 2010 www.cap.org Welcome to the PHC Webinar Series This talk on The Molecular Diagnosis for Colorectal
Molecular Diagnosis for Colorectal Cancer Patients Antonia R. Sepulveda MD, PhD, FCAP October, 20, 2010 www.cap.org Welcome to the PHC Webinar Series This talk on The Molecular Diagnosis for Colorectal
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Sessile serrated adenomas: prevalence of dysplasia and carcinoma in 2139 patients
 Caris Research Institute, Irving, Texas, USA Correspondence to Richard H Lash, MD, Caris Research Institute, 6655 MacArthur Blvd, Irving, TX 75039, USA; rlash@carisdx.com Accepted 11 March 2010 Published
Caris Research Institute, Irving, Texas, USA Correspondence to Richard H Lash, MD, Caris Research Institute, 6655 MacArthur Blvd, Irving, TX 75039, USA; rlash@carisdx.com Accepted 11 March 2010 Published
SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON.
 SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON. Dr Castleman Harvard In 1951 Dr. Benjamin Castleman succeeded Dr. Mallory as Chief of Pathology and Editor of the Case Records
SOME OBSERVATIONS ON COLORECTAL POLYPS; ONLY CONCERNS THOSE WHO HAVE A COLON. Dr Castleman Harvard In 1951 Dr. Benjamin Castleman succeeded Dr. Mallory as Chief of Pathology and Editor of the Case Records
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease
 Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Sessile Serrated Polyps: An Important Route to Colorectal Cancer
 Focused Review 1585 Sessile Serrated Polyps: An Important Route to Colorectal Cancer Matthew F. Kalady, MD Abstract The serrated neoplastic pathway accounts for approximately 30% of colorectal cancers.
Focused Review 1585 Sessile Serrated Polyps: An Important Route to Colorectal Cancer Matthew F. Kalady, MD Abstract The serrated neoplastic pathway accounts for approximately 30% of colorectal cancers.
The MYH Gene Status in Patients with Sporadic Colorectal Polyps
 Juan, I-Cheng PhD Thesis The MYH Gene Status in Patients with Sporadic Colorectal Polyps Wielkopolskie Centrum Onkologii w Poznaniu Poznan University of Medical Sciences Poland. ZaKład Immunologii Nowotworow.
Juan, I-Cheng PhD Thesis The MYH Gene Status in Patients with Sporadic Colorectal Polyps Wielkopolskie Centrum Onkologii w Poznaniu Poznan University of Medical Sciences Poland. ZaKład Immunologii Nowotworow.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Biology of cancer development in the GI tract
 1 Genesis and progression of GI cancer a genetic disease Colorectal cancer Fearon and Vogelstein proposed a genetic model to explain the stepwise formation of colorectal cancer (CRC) from normal colonic
1 Genesis and progression of GI cancer a genetic disease Colorectal cancer Fearon and Vogelstein proposed a genetic model to explain the stepwise formation of colorectal cancer (CRC) from normal colonic
Sessile serrated polyps: Cancer risk and appropriate surveillance
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will understand the role of the recently recognized serrated neoplasia pathway in the development of colorectal cancer ROHIT MAKKAR, MD St. Michael s Hospital,
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will understand the role of the recently recognized serrated neoplasia pathway in the development of colorectal cancer ROHIT MAKKAR, MD St. Michael s Hospital,
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
TumorNext-Lynch. genetic testing for hereditary colorectal or uterine cancer
 TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari
 Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari Milo Frattini XII Congresso AIFEG Villa Cagnola - Gazzada Schianno (VA) 16/17.10.2014 APC β-catenina APC Met (p16) Models of
Marcatori biomolecolari dei carcinomi del colon-retto sporadici ed ereditari Milo Frattini XII Congresso AIFEG Villa Cagnola - Gazzada Schianno (VA) 16/17.10.2014 APC β-catenina APC Met (p16) Models of
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
The Importance of Complete Colonoscopy and Exploration of the Cecal Region
 The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma
 Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma Andrew C. Nelson, M.D., Ph.D. Divisions of Anatomic & Molecular Pathology Department of Laboratory Medicine & Pathology
Molecular Biomarkers in the Characterization & Treatment of Colorectal Carcinoma Andrew C. Nelson, M.D., Ph.D. Divisions of Anatomic & Molecular Pathology Department of Laboratory Medicine & Pathology
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Molecular biology of colorectal cancer
 Molecular biology of colorectal cancer Phil Quirke Yorkshire Cancer Research Centenary Professor of Pathology University of Leeds, UK Rapid pace of molecular change Sequencing changes 2012 1,000 genomes
Molecular biology of colorectal cancer Phil Quirke Yorkshire Cancer Research Centenary Professor of Pathology University of Leeds, UK Rapid pace of molecular change Sequencing changes 2012 1,000 genomes
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Carcinogenesis in IBD
 Oxford Inflammatory Bowel Disease MasterClass Carcinogenesis in IBD Dr Simon Leedham, Oxford, UK Oxford Inflammatory Bowel Disease MasterClass Carcinogenesis in Inflammatory Bowel Disease Dr Simon Leedham
Oxford Inflammatory Bowel Disease MasterClass Carcinogenesis in IBD Dr Simon Leedham, Oxford, UK Oxford Inflammatory Bowel Disease MasterClass Carcinogenesis in Inflammatory Bowel Disease Dr Simon Leedham
IHC And Special Stains In Daily Practice. Dr Ian Brown Envoi Pathology Brisbane, Australia
 IHC And Special Stains In Daily Practice Dr Ian Brown Envoi Pathology Brisbane, Australia Why do special stains? Tumour Classify disease Prognostication Predict response to therapy Identify an inherited
IHC And Special Stains In Daily Practice Dr Ian Brown Envoi Pathology Brisbane, Australia Why do special stains? Tumour Classify disease Prognostication Predict response to therapy Identify an inherited
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
The silence of the genes: clinical applications of (colorectal) cancer epigenetics
 cancer epigenetics") The silence of the genes: clinical applications of (colorectal) cancer epigenetics Manon van Engeland, PhD Dept. of Pathology GROW - School for Oncology & Developmental Biology Maastricht University Medical
The silence of the genes: clinical applications of (colorectal) cancer epigenetics Manon van Engeland, PhD Dept. of Pathology GROW - School for Oncology & Developmental Biology Maastricht University Medical
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Disclaimer: I belong to the speakers bureau of the American Serrated Society, often referred to as the ASS
 An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
An Exposé on Serrated Lesions of the Colorectum How do you know it is a hyperplastic polyp and not something else? How do you know it is something else and not a hyperplastic polyp? Disclaimer: I belong
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By. Magnitude of the Problem. Magnitude of the Problem. Cardinal Features of Lynch Syndrome
 GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual